
Xerostomia in Dialysis Patients—Oral Care to Reduce Hyposalivation, Dental Biofilms and Gingivitis in Patients with Terminal Renal Insufficiency: A Randomized Clinical Study


Abstract
1. Introduction
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| DHI | denture hygiene index |
| GPM/T | index assessing the number of gingivitis affected teeth (G), periodontitis affected teeth (P) and missing teeth (M) |
| HbA1c | glycated hemoglobin |
| MOA | mechanism of action |
| OHIP-G 14 | Oral Health Impact Profile, German version, 7 Items with 14 Questions |
| SLI | Silness–Löe dental plaque index |
References
- Ying Joanna, N.D.; Thomson, M.W. Dry mouth—An overview. Singap. Dent. J. 2015, 36, 12–17. [Google Scholar] [CrossRef]
- Gaengler, P.; Arnold, W.H.; Steinberg, D. Ätiologie und Pathogenese. In Konservierende Zahnheilkunde und Parodontologie; Gängler, P., Hoffmann, T., Willershausen, B., Schwenzer, N., Ehrenfeld, M., Eds.; Georg Thieme Verlag Stuttgart: New York, NY, USA, 2010; pp. 112–138. [Google Scholar]
- Neuhaus, K.W.; Strömberg, S. Zahn- und Mundpflege bei Mundtrockenheit. In Speichel; Filippi, A., Waltimo, T., Eds.; Quintessenz Verlag: Berlin, Germany, 2020; pp. 259–269. [Google Scholar]
- Billings, R.J.; Proskin, H.M.; Moss, M.E. Xerostomia and associated factors in a community-dwelling adult population. Commun. Dent. Oral Epidemiol. 1996, 24, 312–316. [Google Scholar] [CrossRef]
- Nederfors, T.; Isaksson, R.; Mörnstad, H.; Dahlöf, C. Prevalence of perceived symptoms od dry mouth in an adult Swedish population—relation to age, sex and pharmacotherapy. Commun. Dent. Oral Epidemiol. 1997, 25, 211–216. [Google Scholar] [CrossRef]
- Yeh, C.K.; Johnson, D.A.; Dodds, M.W.J. Impact of aging on human salivary gland function: A community-based study. Aging Clin. Exp. Res. 1998, 10, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Ship, J.A.; Pillemer, S.R.; Baum, B.J. Xerostomia and the geriatric patient. J. Am. Geriatr. Soc. 2002, 50, 535–543. [Google Scholar] [CrossRef]
- Diep, M.T.; Jensen, J.L.; Skudutyte-Rysstad, R.; Young, A.; Sødal, A.T.T.; Petrovski, B.É.; Hove, L.H. Xerostomia and hyposalivation among a 65-yr-old population living in Oslo, Norway. Eur. J. Oral Sci. 2021, 129, e12757. [Google Scholar] [CrossRef] [PubMed]
- Jover Cerveró, A.; Bagán, J.V.; Soriano, Y.J.; Roda, R.P. Dental management in renal failure: Patients on dialysis. Med. Oral Patol. Oral Cir. Bucal. 2008, 13, 419–426. [Google Scholar]
- Kaushik, A.; Reddy, S.; Umesh, L.; Devi, B.K.Y.; Santana, N.; Rakesh, N. Oral and salivary changes among renal patients undergoing hemodialysis: A cross-sectional study. Indian J. Nephrol. 2013, 23, 125–129. [Google Scholar] [CrossRef]
- Swapna, L.A.; Reddy, R.S.; Ramesh, T.; Reddy, R.L.; Vijayalaxmi, N.; Karmakar, P.; Pradeep, K. Oral health status in haemodialysis patients. J. Clin. Diagnos. Res. 2013, 7, 2047–2050. [Google Scholar] [CrossRef] [PubMed]
- Lohaus, J. Auswirkungen Professioneller Pflege auf die Mundgesundheit und Lebensqualität von Bewohnern eines Städtischen Pflegeheims. Ph.D. Dissertation, University of Witten/Herdecke, Witten, Germany, 2020. [Google Scholar]
- Silness, J.; Löe, H. Periodontal disease in Pregnancy. II. Correlation between oral hygiene and periodontal condition. Acta Odontol. Scand. 1964, 22, 121–135. [Google Scholar] [CrossRef]
- Gaengler, P. Prevalence and distribution of gingivitis, periodontitis and missing teeth in adolescents and adults according to GPM/T index. Commun. Dent. Oral Epidemiol. 1984, 12, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Klein, H.; Palmer, C. Studies on dental caries. Public Health Rep. 1938, 53, 1353–1364. [Google Scholar] [CrossRef]
- Wefers, K.P. Der “Denture Hygiene Index” (DHI). Dent. Forum 1999, 1, 13–15. [Google Scholar]
- John, M.T.; Patrick, D.L.; Slade, G.D. The German version of the Oral Health Impact Profile—Translation and psychometric properties. Eur. J. Oral. Sci. 2002, 110, 425–433. [Google Scholar] [CrossRef]
- Ariyamuthu, V.K.; Nolph, K.D.; Ringdahl, B.E. Periodontal disease in chronic kidney disease and end-stage renal disease patients: A review. Cardiorenal Med. 2013, 3, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Bayraktar, G.; Kurtulus, I.; Duraduryan, A.; Cintan, S.; Kazancıoğlu, R.T.; Yildiz, A.; Bural, C.; Bozfakioglu, S.; Besler, M.; Trablus, S.; et al. Dental and periodontal findings in hemodialysis patients. Oral Dis. 2007, 13, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Bhatsange, A.; Patil, S.R. Assessment of periotontal health status in patients undergoing renal dialysis: A descriptive, cross-sectional study. J. Indian Soc. Periodontol. 2012, 16, 37–42. [Google Scholar] [CrossRef]
- Rodrigues, R.P.C.B.; Vidigal, M.T.C.; Vieira, W.A.; Nascimento, G.G.; Sabino-Silva, R.; Blumenberg, C.; Siqueira, M.F.; Siqueira, W.L.; Paranhos, L.R. Salivary changes in chronic kidney disease and in patients undergoing hemodialysis: A systematic review and meta-analysis. J. Nephrol. 2022, 35, 1339–1367. [Google Scholar] [CrossRef]
- Cunha, F.L.; Tagliaferro, E.P.S.; Pereira, A.C.; Meneghim, M.C.; Hebling, E. Oral health of a Brazilian population on renal dialysis. Spec. Care Dent. 2007, 27, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Klassen, J.T.; Krasko, B.M. The dental health status of dialysis patients. J. Canad. Dent. Assoc. 2002, 68, 34–38. [Google Scholar]
- Altamimi, A.; AlBakr, S.; Alanazi, T.; Alshahrani, F.; Chalisserry, E.; Anil, S. Prevalence of periodontitis in patients undergoing hemodialysis: A case control study. Mater. Sociomed. 2018, 30, 58–61. [Google Scholar] [CrossRef]
- Bayraktar, G.; Kurtulus, I.; Kazancıoğlu, R.T.; Bayramgurler, I.; Cintan, S.; Bural, C.; Bozfakıoğlu, S.; Besler, M.; Trablus, S.; Issever, H.; et al. Evaluation of periodontal parameters in patients undergoing peritoneal dialysis or hemodialysis. Oral Dis. 2008, 14, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Atassi, F. Oral home care and the reasons for seeking dental care by individuals on renal dialysis. J. Contemp. Dent. Pract. 2002, 3, 31–41. [Google Scholar] [CrossRef]
- Kho, H.-S.; Lee, S.-W.; Chung, S.-C.; Kim, Y.-K. Oral manifestations and salivary flow rate, pH, and buffer capacity in patients with end-stage renal disease undergoing hemodialysis. Oral Surg. Oral Med. Oral Radiol. Endodont. 1999, 88, 316–319. [Google Scholar] [CrossRef]
- Almeida, S.; Figueredo, C.M.; Lemos, C.; Bregman, R.; Fischer, R.G. Periodontal treatment in patients with chronic kidney disease: A pilot study. J. Periodont. Res. 2017, 52, 262–267. [Google Scholar] [CrossRef]
- de Souza, C.M.; Braosi, A.P.; Luczyszyn, S.M.; Olandoski, M.; Kotanko, P.; Craig, R.G.; Trevilatto, P.C.; Pecoits-Filho, R. Association among oral health parameters, periodontitis, and its treatment and mortality in patients undergoing hemodialysis. J. Periodontol. 2014, 85, 169–178. [Google Scholar] [CrossRef]
- Palmer, S.C.; Ruospo, M.; Wong, G.; Craig, J.; Petruzzi, M.; De Benedittis, M.; Ford, P.; Johnson, D.W.; Tonelli, M.; Natale, P.; et al. Dental health and mortality in people with end-stage kidney disease treated with hemodialysis: A multinational cohort study. Am. J. Kidney Dis. 2015, 66, 666–676. [Google Scholar] [CrossRef]
- Veisa, G.; Tasmoc, A.; Nistor, I.; Segall, L.; Siriopol, D.; Solomon, S.M.; Donciu, M.D.; Voroneanu, L.; Nastasa, A.; Covic, A. The impact of periodontal disease on physical and psychological domains in long-term hemodialysis patients: A cross-sectional study. Intern. Urol. Nephrol. 2017, 49, 1261–1266. [Google Scholar] [CrossRef] [PubMed]
- Veisa, G.; Tasmoc, A.; Nistor, I.; Segall, L.; Siriopol, D.; Solomon, S.M.; Donciu, M.D.; Voroneanu, L.; Nastasa, A.; Covic, A. Lack of correlation between periodontitis and renal dysfunction in systemically healthy patients. Eur. J. Dent. 2011, 5, 8–18. [Google Scholar]
- Xie, T.; Yang, Z.; Dai, G.; Yan, K.; Tian, Y.; Zhao, D.; Zou, H.; Deng, F.; Chen, X.; Yuan, Q. Evaluation of the oral health status in Chinese hemodialysis patients. Hemodial. Intern. 2014, 18, 668–673. [Google Scholar] [CrossRef] [PubMed]
- Ziebolz, D.; Fischer, P.; Hornecker, E.; Mausberg, R.F. Oral health of hemodialysis patients: A cross-sectional study at two German dialysis centers. Hemodial. Int. 2012, 16, 69–75. [Google Scholar] [CrossRef]
- Plemons, J.M.; Al-Hashimi, I.; Marek, C.L. Managing xerostomia and salivary gland hypofunction. J. Am. Dent. Assoc. 2014, 145, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Dalodom, S.; Lam-Ubol, A.; Jeanmaneechotechai, S.; Takamfoo, L.; Intachai, W.; Duangchada, K.; Hongsachum, B.; Kanjanatiwat, P.; Vacharotayangul, P.; Trachootham, D. Influence of oral moisturizing jelly as a saliva substitute for the relief of xerostomia in elderly patients with hypertension and diabetes mellitus. Geriatr. Nurs. 2016, 37, 101–109. [Google Scholar] [CrossRef]
- Yu, I.-C.; Tsai, Y.-F.; Fang, J.-T.; Yeh, M.-M.; Fang, J.-Y.; Liu, C.-Y. Effects of mouthwash interventions on xerostomia and unstimulated whole saliva flow rate among hemodialysis patients: A randomized controlled study. Int. J. Nurs. Stud. 2016, 63, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Bin Mohsin, A.H.; Reddy, S.V.; Kumar, M.P.; Samee, S. Aloe vera for dry mouth denture patients—Palliative therapy. J. Clin. Diagnos. Res. 2017, 11, 20–23. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, M.; Shirayama, Y.; Imoto, I.; Hinode, D.; Yanagisawa, S.; Takeuchi, Y. Current status of collaborative relationships between dialysis facilities and dental facilities in Japan: Results of a nationwide survey. BMC Nephrol. 2015, 16, 17. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Control Group | Verum Group | |||||
|---|---|---|---|---|---|---|
| Parameter | Baseline (x ± SD) | Final (x ± SD) | p< | Baseline (x ± SD) | Final (x ± SD) | p< |
| Dry mouth frequency 0–4 | 2.14 ± 0.99 | 2.24 ± 0.94 | n.s. | 2.82 ± 0.80 | 1.76 ± 0.70 | 0.001 |
| Dry mouth during dialysis y/n | 11 | 12 | n.s. | 13 | 5 | 0.01 |
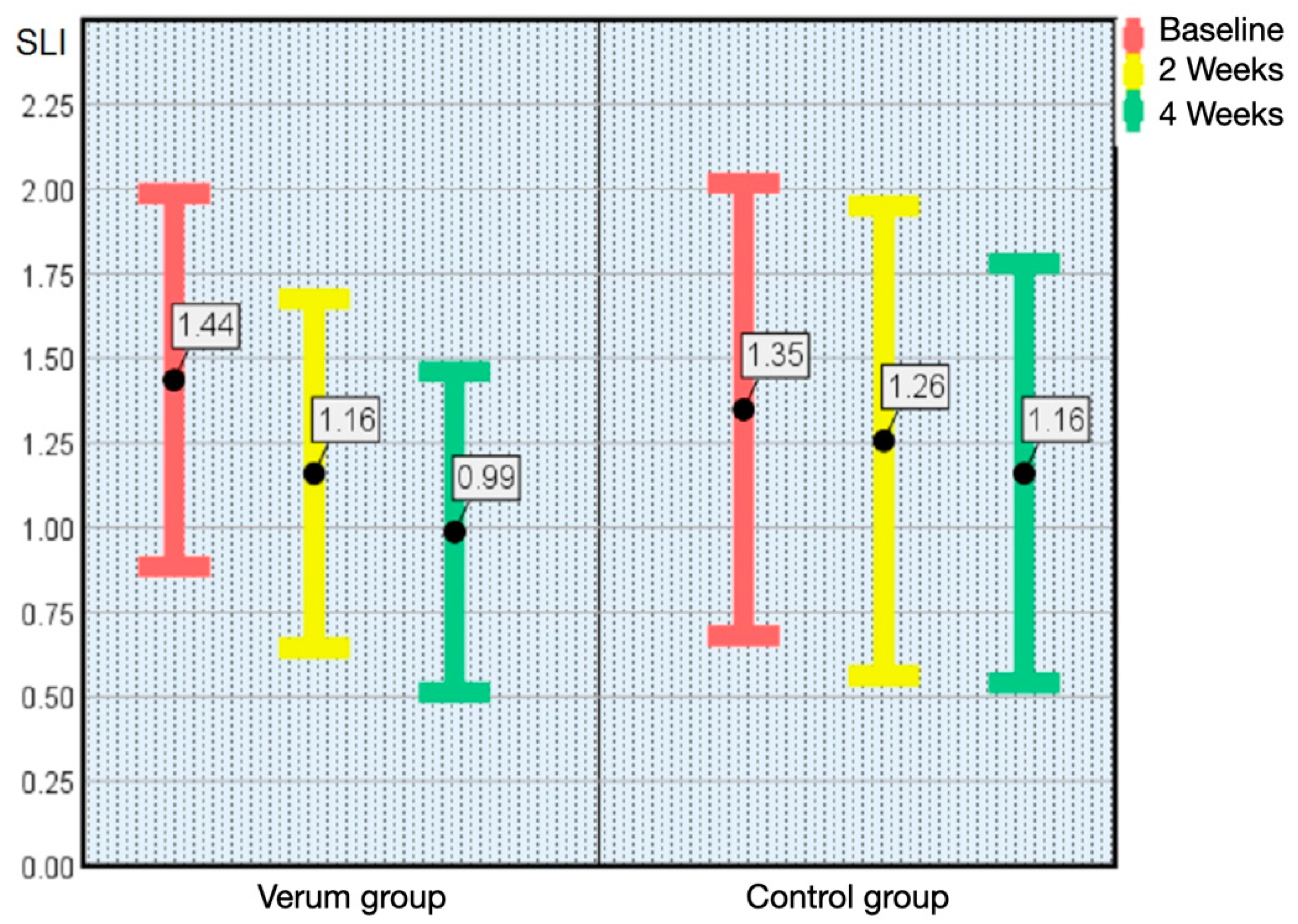
| Plaque index SLI codes 0–3 | 1.35 ± 0.67 | 1.16 ± 0.62 | n.s. | 1.44 ± 0.55 | 0.99 ± 0.47 | 0.001 |
| Tongue coating codes 0–2 | 1.73 ± 0.63 | 1.5 ± 0.60 | n.s. | 1.73 ± 0.07 | 1.14 ± 0.36 | 0.01 |
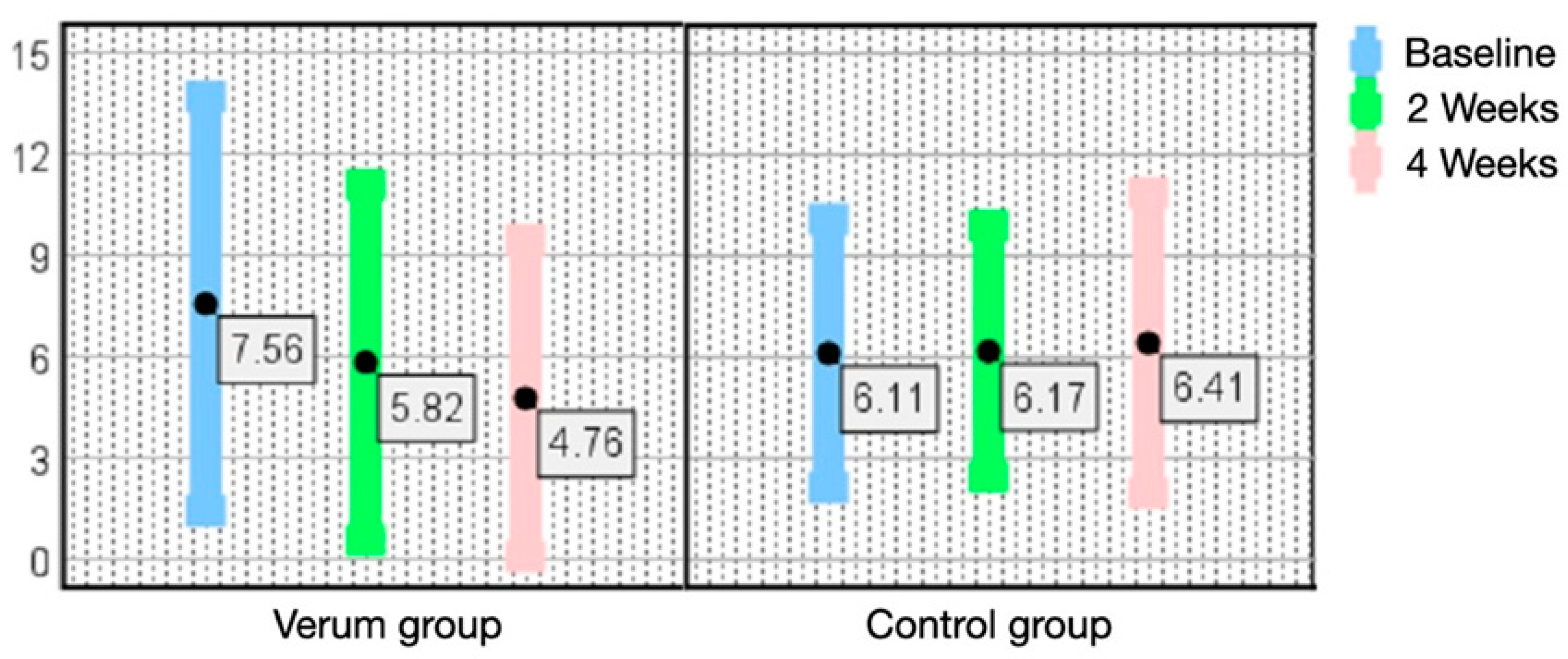
| Gingivitis affected teeth (n) | 6.12 ± 3.98 | 6.41 ± 4.46 | n.s. | 7.56 ± 6.14 | 4.76 ± 4.70 | 0.001 |
| Periodontitis affected teeth shallow (n) | 9.00 ± 4.63 | 9.88 ± 3.85 | n.s. | 9.00 ± 4.30 | 8.35 ± 4.39 | 0.05 |
| Denture hygiene index maxillary plaquefree % | 28.33 ± 18.37 | 34.50 ± 26.09 | n.s. | 33.89 ± 22.45 | 61.14 ± 29.48 | 0.05 |
| Denture hygiene index mandibulary plaquefree % | 36.67 ± 40.33 | 44.00 ± 40.37 | n.s. | 32.71 ± 27.78 | 51.14 ± 18.14 | 0.05 |
| OHIP-G14 7 items, 5 codes, total 0–56 | 6.25 ± 6.36 | 5.67 ± 5.7 | n.s. | 6.62 ± 5.74 | 4.75 ± 5.02 | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Egbring, L.C.; Lang, T.; Kreft, B.; Weich, K.W.; Gaengler, P. Xerostomia in Dialysis Patients—Oral Care to Reduce Hyposalivation, Dental Biofilms and Gingivitis in Patients with Terminal Renal Insufficiency: A Randomized Clinical Study. Kidney Dial. 2023, 3, 111-120. https://doi.org/10.3390/kidneydial3010010
Egbring LC, Lang T, Kreft B, Weich KW, Gaengler P. Xerostomia in Dialysis Patients—Oral Care to Reduce Hyposalivation, Dental Biofilms and Gingivitis in Patients with Terminal Renal Insufficiency: A Randomized Clinical Study. Kidney and Dialysis. 2023; 3(1):111-120. https://doi.org/10.3390/kidneydial3010010
Chicago/Turabian StyleEgbring, Leonie C., Tomas Lang, Burkhard Kreft, Karl W. Weich, and Peter Gaengler. 2023. "Xerostomia in Dialysis Patients—Oral Care to Reduce Hyposalivation, Dental Biofilms and Gingivitis in Patients with Terminal Renal Insufficiency: A Randomized Clinical Study" Kidney and Dialysis 3, no. 1: 111-120. https://doi.org/10.3390/kidneydial3010010
APA StyleEgbring, L. C., Lang, T., Kreft, B., Weich, K. W., & Gaengler, P. (2023). Xerostomia in Dialysis Patients—Oral Care to Reduce Hyposalivation, Dental Biofilms and Gingivitis in Patients with Terminal Renal Insufficiency: A Randomized Clinical Study. Kidney and Dialysis, 3(1), 111-120. https://doi.org/10.3390/kidneydial3010010