Simple Summary
Human epidermal growth factor receptors (HERs) are present in our body and are responsible for regulating cell growth. When there is an overexpression of HER2/neu receptors, it can lead to the development of certain cancers. Studies have shown that this overproduction of HER2/neu is found in 25–30% of breast cancers and 10–30% of stomach and food pipe cancers. HER2/neu has been identified as a useful marker for predicting and treating breast and stomach cancers. However, research suggests that HER2 also plays a role as a marker in other cancers. This article reviews the latest research on HER2 and its link to other cancers besides breast and gastric cancers.
Abstract
The human epidermal growth factor receptors (HERs) are expressed abundantly in the human body. The tumorigenic potential of HER2/neu is linked to its overexpression, amplification or somatic mutation. The HER2 gene amplification leading to protein overexpression has been reported in 25–30% of breast cancers and 10–30% of gastric/gastroesophageal cancers. While HER2 is a well-documented predictive, prognostic, and therapeutic marker in breast and gastric/gastroesophageal cancers, its relevance has also been demonstrated in multiple other malignancies. In this article, we will conduct an extensive review of current data pertaining to HER2 amplification, overexpression, or mutation in cancers other than breast and gastric cancers.
1. Introduction
1.1. Nomenclature, Structure and Function
HERs belong to a family of epidermal growth factor receptor (EGFR) and have four subtypes: HER1 (EGFR, erbB1), HER2 (erbB2, HER2/neu), HER3 (erbB3), and HER4 (erbB4). As far as nomenclature is concerned, erbB2 is used to represent the gene in both humans and rodents, whereas neu is used to refer to rodent gene and product in rodent species and HER2 in human species. HER2, also known as CD340 (cluster of differentiation) is a 185 kD transmembrane glycoprotein encoded by ERBB2 (erythroblastic oncogene 2) proto-oncogene present on the long arm of chromosome 17 (17q12) [1]. The neu oncogene was discovered by Shih et al. in 1981 in ethyl nitrosourea-induced rodent neuroblastoma [2]. It was described as a transforming oncogene with similarities to ErbB (avian erythroblastosis oncogene B) oncogene and the epidermal growth factor receptor (EGFR) gene [3,4]. King et al. found an EGFR-related gene amplification in human mammary cells in 1984 and named it as the human epidermal growth factor receptor 2 (HER2) [5].
The HER family is usually present as monomers on the surface of the cell. Their structure comprises three domains: transmembrane lipophilic, an intracellular tyrosine kinase, and an extracellular ligand-binding domain [6] (Figure 1). The extracellular domain (ECD) has 630 amino acids with four domains arranged in repetitive pairs of domain I-III (190 amino acids) followed by domain II-IV (120 amino acids). The extracellular domain pivots between active-inactive conformation and accelerate dimer formation only on the binding of the ligand. In HER1 and 3, domain II has finger-like projections which overlay on domain IV to occlude the dimerization surface [7]. When a ligand binds, there is domain rearrangement decreasing the proximity between domains I and III, making domain II projection free for dimer formation. HER2 differs from HER1 and 3 in that domains II and IV have no contact and HER2 has no known activating ligand, and its extracellular domain is constitutively in active configuration due to lack of internal autoinhibitory structure. Additionally, HER2 can form heterodimerization with other members, such as HER1 or HER3 or insulin-like growth factor receptor 1. On the contrary, other HERs have several known activating ligands [8].
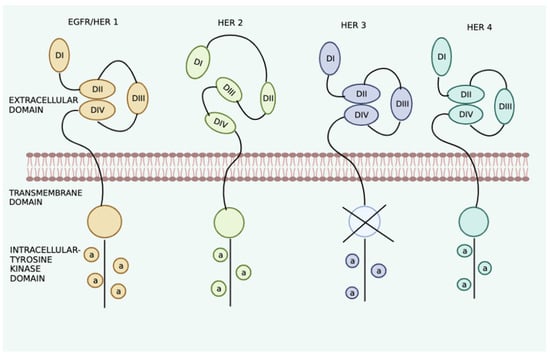
Figure 1.
Schematic diagram representing the structure of HERs. Extracellular domains include I and III and II and IV, and transmembrane domain and intracellular domain include juxtmembranous part, tyrosine kinase catalytic part and C-terminal tail (dotted line) which contains the tyrosine residues.
The HERs are expressed normally in neuronal tissues, epithelial cells, and mammary glands, playing an important role in cellular proliferation, survival, differentiation, and angiogenesis. Heterodimerization of HERs lead to autophosphorylation of cytoplasmic domain of tyrosine kinase initiating various downstream signaling pathways, important ones being mitogen-activated protein kinase (MAPK), signal transducer and activator of transcription (STAT), phospholipase C gamma, protein kinase C(PKC) and phosphoinositide 3-kinase (PI3K) (Figure 2). These signaling pathways which regulate the proliferation and survival of cells, angiogenesis and invasion are recognized as the targets of HER2/neu upon activation in different malignancies. HER3 lacks ATP (adenosine triphosphate) binding within its catalytic domain, making it dependent on its heterodimers for its kinase activity [9]. Studies have shown that HER2-HER3 are obligate partners, and this heterodimer is the most potent activating stimulus for PI3L/Akt pathway [10]. Aberrant HER2 signaling can lead to tumorigenesis through the above-mentioned pathways and other reported mechanisms including Src kinase activation; loss of cell polarity and adhesion; invasive phenotype promotion; and cell cycle dysregulation, particularly G1/S checkpoint control via two important downstream targets, cyclin D1 and p27 [11,12].

Figure 2.
Schematic diagram of the function of HER2 with downstream signaling pathways: mitogen-activated protein kinase (MAPK) and phosphoinositide 3-kinase (PI3K), activated on homo or heterodimerization.
1.2. Testing for HER2 Neu
Immunohistochemistry (IHC) is a technique that utilizes monoclonal as well as polyclonal antibodies to identify tissue distribution of antigen of interest. Scoring criteria is summarized in (Table 1). IHC is a faster technique utilizing conventional bright-field microscopes and there is no degradation of stained tissue over time [13]. Moreover, it allows for parallel viewing of morphological features of tumor cells under the microscope [13]. Despite conferring these advantages, test results can vary based on primary antibodies and the scoring criteria used. Furthermore, it is a semi-quantitative method based on subjective determination of color intensity with a host of pre-analytic, analytic, and post-analytic parameters affecting the results.

Table 1.
Summarizing the scoring criteria for IHC results in breast cancer.
Fluorescence in situ hybridization (FISH) is a technique utilizing single-stranded deoxyribonucleotide (DNA) or ribonucleotide (RNA) sequence (probe) to detect a specific DNA sequence on the chromosome by forming complementary base pairs with DNA or RNA of the tissue sample. Apart from being more precise, sensitive, and reproducible [14], results are more quantitative and less dependent on processing techniques. However, given the time-consuming nature and the requirement of fluorescent microscopy for integration, it is usually reserved for IHC equivocal samples (IHC score 2+) to confirm HER2 status. IHC scores 0 and 1+ are considered as HER2-negative and score 3+ is considered HER2-positive. If the IHC score is 2+, then it is reflex tested via FISH. If the HER2 gene is amplified in the FISH testing, it is considered as HER2-positive. Newer techniques using peroxidase enzyme-labeled probes, such as CISH (chromogenic in situ hybridization) and SISH (silver in situ hybridization), have emerged in recent years. Instead of using a fluorescent microscope, they employ a normal bright-field microscope for interpretation, thus conferring an advantage over FISH analysis [13].
Other techniques include serum detection of HER2 ECD using enzyme-linked immunosorbent assay or HER2 in circulating tumor cells [15,16]. RT-PCR is a technique utilizing reverse transcription of RNA (ribonucleic acid) into DNA (deoxyribonucleic acid) followed by polymerase chain reaction mediated amplification of DNA targets to measure the amount of specific RNA in the sample. It has no interobserver variability, can be used in small samples, and is automated [17]. However, there is a chance of false-negative results as during RNA extraction, non-tumor and tumor cells are mixed, thus diluting the influence of tumor cells [18].
2. Strategies for Review
We carried out an electronic systematic search in PubMed database using keywords “Receptor, ErbB-2 [MeSH]” OR “Genes, erbB-2 [MeSH]” OR “HER-2 protein [Supplementary concept]” OR “ERBB2 protein, human [Supplementary concept] and “Neoplasms [MeSH]”. All cancers, except for breast and gastro-esophageal malignancies with which association was reported, were noted.
Original articles with HER2/neu overexpression or amplification or mutation status reported in a malignancy were included. Articles other than original research (i.e., review articles, case reports, letter to editor, editorial or commentaries), duplicate publications or non-English publications were excluded. Titles and abstracts were independently screened by two authors (FA, and PM). Full texts of the included articles with extraction of data were independently conducted by three authors (FA, PS, and NG). Any discrepancy was resolved by a consensus of the authors. Additional articles were included by cross-referencing the reference list of the included articles. Descriptive analysis in the form of percentages has been used to describe HER2 amplification, expression, and mutation status with cumulative range to express the overall results.
We have also incorporated clinical trials utilizing HER2 agents in some malignancies (ovarian, endometrial, colorectal, salivary gland, pancreatic, bladder and prostate cancer) in the last two decades, between 1 January 2000 and 21 February 2022 (Figure 3).
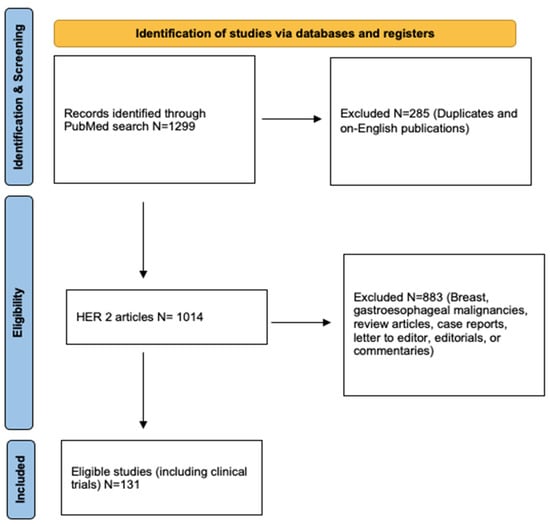
Figure 3.
PRISMA flow diagram of the literature search process.
3. Results
3.1. Ovarian Cancer
Ovarian cancer is the second leading cause of gynecologic cancer in the USA. Approximately 95% of ovarian cancers are epithelial and the other 5% include sex cord stromal and germ cell tumors. HER2/neu overexpression and amplification has been reported in 5–50% and 2–25% of ovarian cancer cases, respectively, especially in the mucinous histologic subtype (Table 2 and Table 3).
Table 2.
Summarizing studies on HER2 overexpression or amplification in epithelial ovarian carcinoma.
Table 3.
Summarizing clinical trials (only in the last 20 years) using anti-HER2 agents in epithelial ovarian cancer.
Some studies have reported somatic HER2 mutations—insertional mutation in exon 20 and missense mutations (R970W and E971G) [38,39]. Berchuck et al., reported that patients with high HER2 overexpression were significantly less likely to have complete response to primary therapy or negative second-look laparotomy when serum CA 125 levels were normal pre-operatively [40]. Danish 2003 MALOVA ovarian cancer study concluded HER2 overexpression to be a negative prognostic marker [22]. As mentioned in (Table 3), two phase II clinical trials showed variable response to anti-HER2 agents; one study reported lack of clinical response after using trastuzumab whereas another study using pertuzumab showed clinical benefit, especially in the presence of low HER3 mRNA expression.
3.2. Endometrial Cancer
Endometrial cancer is the leading cause of gynecologic malignancy in the USA. The most common histologic subtype is endometroid carcinoma and it has the most favorable prognosis as compared to the other subtypes. HER2 gene amplification and protein expression is postulated in 3–47% and 14–80% of endometrial cancers, respectively, most commonly in serous histologic subtype (Table 4). Rolitsky et al., reported that whereas amplification was detected in both clear cell and serous subtypes, overexpression was only associated with clear cell type [41]. For all histologic subtypes, including endometrioid type, both expression and amplification corroborate a high stage and grade, implying poor overall survival [41,42]. Satin et al., reported that African American women harbor a significantly higher proportion of amplified HER2/neu gene in serous papillary uterine carcinoma and have overall poorer prognosis [43]. As mentioned in (Table 5), two phase II clinical trials have been conducted, one using trastuzumab alone and another in combination with carboplatin/paclitaxel with no overall benefit, however, they had manageable toxicity profile although full accrual of HER2 expressing tumors was not achieved in one of them.
Table 4.
Summarizing studies on HER2 overexpression or amplification in uterine serous carcinoma.
Table 5.
Summarizing clinical trials (only in the last 20 years) using anti-HER2 agents in uterine serous carcinoma.
3.3. Lung Cancer
Lung cancer is the most prevalent cause of cancer-related death in both males and females worldwide. Majority of the lung cancers (85%) are non-small cell lung cancer (NSCLC). HER2 overexpression and amplification has been reported in 10–30% and 10–20% of the analyzed surgical specimens of non-small cell lung cancers, respectively, in retrospective studies. Somatic mutations have been frequently reported in 1–4% cases, most commonly in exon 20 and C-helix region of the kinase domain (Table 6). Two large studies by Sasaki et al., (in Japanese population) and Arcila et al., (in Caucasian population) have reported insertion mutations (YVMA) in exon 20 at codon 775 [55,56]. In different meta-analysis, Nakamura H et al. (2579 patients) and Liu L et al., (6135 patients) found that there is a significant negative prognostic effect of HER2 overexpression [57,58]. In lung adenocarcinomas, HER2 mutations have been reported, especially in Asian patient population, female sex and light/non-smokers [59,60]. As mentioned in (Table 7), initial phase II clinical trials conducted in the early 2000s with trastuzumab alone or in combination with either cisplatin-gemcitabine, paclitaxel and carboplatin or docetaxel did not improve the overall survival in HER2-positive NSCLC although it was suggested that HER2 3+/FISH-positive patient might benefit from these therapies [61,62,63]. IHC is not the most optimal test for detecting HER2 status and it was used in these trials. Later, studies using antibody drug conjugates, such as Ado-trastuzumab emastine or trastuzumab deruxtecan, in HER2 mutated NSCLC patients demonstrated a durable response irrespective of the absence or presence of HER2 protein expression or amplification [64,65,66]. Gefitinib or afatinib when used in EGFR TKI naïve HER2 mutated advanced NSLC showed no benefit but dacomitinib showed clinical activity [67,68,69]. More recently, trials using other TKIs in HER2-mutated NSCLC, such as Pyrotinib (PRIDE TRIAL), are ongoing [55].
Table 6.
Summarizing studies reporting HER2 somatic mutations in lung cancer.
Table 7.
Summarizing clinical trials (only in the last 20 years) using anti-HER2 agents in lung cancer.
3.4. Colorectal Cancer (CRC)
HER2/neu overexpression and amplification has been noted in 2.5–80% and 1.5–60% of the CRC’s, respectively (Table 8). While a significant amount of research has been undertaken to elucidate the role of membranous HER2/neu in CRC, the clinical significance of cytoplasmic expression remains yet to be deciphered. Somatic HER2 mutations have been reported on the kinase domain in 3 out of 104 patients in a study by Lee et al. [82]. HER2/neu positivity is linked with high UICC (Union for International Cancer Control) stage and nodal positive metastases, as well as T-category and nodal status in sigmoidal and rectal subgroups [83,84]. Conradi et al. found that in advanced rectal carcinomas, HER2-positive tumors have better 5-year cancer-specific survival than HER2/neu-negative tumors post neoadjuvant radio chemotherapy [85]. As mentioned in (Table 9), initial trials using trastuzumab with irinotecan or cetuximab and pertuzumab showed some activity but studies were limited due to low overexpression rate or drug toxicity [86,87]. More recently, dual anti-HER2 therapies, such as trastuzumab with pertuzumab and trastuzumab with lapatinib, have been tried with significant clinical responses [87,88,89]. Furthermore, trastuzumab deruxtecan alone has shown a promising activity against metastatic HER2 expressing CRC refractory to standard treatment, thereby offering newer insights into treatment of this subset of tumor [90].
Table 8.
Summarizing studies on HER2 overexpression or amplification in colorectal carcinoma.
Table 9.
Summarizing clinical trials (only in the last 20 years) using anti-HER2 agents in colorectal carcinoma.
3.5. Salivary Gland Cancer
Salivary gland cancer is a subset of head and neck cancers constituting various histologic subtypes, such as mucoepidermoid carcinoma, salivary ductal carcinoma (SDC), adenoid cystic carcinoma mammary analogue secretory carcinoma and carcinoma ex pleomorphica (CEPA). Adenocarcinoma, not otherwise specified, is the most common malignant subtype followed by salivary ductal carcinoma. HER2 gene amplification and protein expression has been reported in 20–100% and 2–100% of the samples, respectively, most commonly being reported in salivary ductal carcinoma (Table 10). HER2 overexpression has been reported as the marker of pleomorphic adenoma to CEPA malignant transformation [108]. In both CEPA and salivary ductal carcinoma, HER2 gene expression and amplification are suggested to have poor prognosis. As mentioned in (Table 11), initial phase II clinical trials on HER2 positive salivary gland cancer using trastuzumab or lapatinib have shown limited clinical response [109,110]. These trials did not have patients with salivary ductal carcinoma and there have been many retrospective studies and case reports demonstrating the effect of trastuzumab on salivary ductal carcinoma [111,112]. A most recent single center trial in Japan on HER2 expression in SDC patients showed a 70.2% response to the trastuzumab + docetaxel combination therapy [113].
Table 10.
Summarizing studies on HER2 overexpression or amplification in salivary gland cancers with histologic subtype.
Table 11.
Summarizing clinical trials (only in the last 20 years) using anti-HER2 agents in salivary gland cancers.
3.6. Pancreatic Cancer
Despite recent advances, treatment for pancreatic cancer remains an enigma, portraying a dismal prognosis with surgical resection being the only potential curative option. The prevalence of HER2 overexpression and amplification is approximately 10–70% and 2–20%, respectively (Table 12). HER2/neu protein expression has been significantly associated with grade and not stage [126]. As mentioned in (Table 13), studies have been conflicting, as trial comparing combined trastuzumab with capecitabine or gemcitabine did not show any improvement in overall survival but recently published GATE 1 trial using it with gemcitabine and erlotinib as first line agent showed clinical activity [127,128,129].
Table 12.
Summarizing studies on HER2/neu overexpression or amplification in pancreatic carcinoma.
Table 13.
Summarizing clinical trials (only in the last 20 years) using anti-HER2 agents in pancreatic carcinoma.
3.7. Bladder Cancer
Bladder cancer is the most common malignancy of urinary system with urothelial (transitional cell) carcinoma being the most prevalent histologic subtype in the USA. The exact numbers are uncertain, but HER2 overexpression and gene amplifications have been reported in 10–70% and 5–10%, respectively. A metanalysis in 2021 showed that HER2 expression was associated with CIS, large tumor size, high tumor grade and stage, multifocal tumor, lymph node metastasis, progression, recurrence papillary tumor and poor prognosis [143]. As mentioned in (Table 14), trials using trastuzumab in combination with gemcitabine, carboplatin and paclitaxel have observed higher cardiotoxicity rates, although most were grade 2 or lower with 70% clinical response rates but promising response has been obtained with use of HER2 targeting the antibody-drug conjugate RC48-ADC.
Table 14.
Summarizing studies clinical trials (only in the last 20 years) using anti-HER2 agents in bladder cancer.
3.8. Prostate Cancer
Prostate cancer is the second leading cause of cancer-related mortality in men in the USA after lung cancer. Initially being hormone-dependent, androgen receptor overexpression and mutations are the most implicated pathophysiological reasons that lead to the eventual progression to androgen-independent prostate cancer. HER2/neu overexpression has been demonstrated in androgen-independent prostate cancer and is associated with advanced disease, high recurrence and poor prognosis [147,148,149]. As mentioned in (Table 15), multiple phase II trials using trastuzumab or pertuzumab as single agent or in combination with docetaxel or single agent TKIs, such as lapatinib or gefitinib, in hormone refractory prostate cancer have shown no clinical response.
Table 15.
Summarizing studies clinical trials (only in the last 20 years) using anti-HER2 agents in prostate cancer.
3.9. Biliary Tract Cancer (BTC)
Gall bladder cancer is a rare and an aggressive cancer with heterogenous genetic makeup, with so far published data showing 0–25% HER2/neu protein expression with most studies being from India, Japan or South America [157,158,159]. HER2 gene amplification have been reported in 5–8% cases [160]. Sampling 186 patients with gall bladder cancer, of which 74 had high grade biliary intra-epithelial neoplasia, Albrecht et al. found that 5.9% of patients had a 2+ IHC score and 5.4% of the patients had an IHC score of 3+ with clear-cut gene amplification. [161]. A single-center study on HER2 expressing BTC showed that none of the cholangiocarcinoma patients (five) but eight out of nine patients with gall bladder cancer (three disease stability, four partial response and one complete response) responded to HER2/neu-directed therapy [162]. There have been demonstrated antiproliferative activity of lapatinib in in vitro models of BTCs [163]
3.10. Other Malignancies
3.10.1. Osteosarcoma (OS)
OS is the most prevalent and aggressive primary pediatric bone cancer, with HER2/neu overexpression been postulated to be a poor prognostic marker [164,165]. Akastsuka et al. found that HER2 overexpression decreases in osteosarcoma as they metastasized to the lungs [166]. However, a retrospective study conducted in Michigan in 2002 and in Netherlands in 2004 [167,168] demonstrated the absence of HER2 mRNA or protein overexpression in OS. Two clinical trials to study the use of trastuzumab in recurrent osteosarcoma (Clinicaltrials.gov Identifier: NCT00005033) and metastatic osteosarcoma (Clinicaltrials.gov Identifier: NCT00023998) have been undertaken but the results have not yet been published.
3.10.2. Thyroid Cancer
Thyroid cancers can originate from either epithelial-derived follicular cells or from parafollicular C-cells, called medullary thyroid cancer, or appear as primary thyroid lymphoma. Epithelial-derived cancers can be subgrouped into differentiated thyroid cancers (follicular 12% and papillary cancer 85%) or undifferentiated cancers (anaplastic < 3%). HER2/neu overexpression was associated to a predictive factor in differentiated thyroids carcinomas (both papillary and follicular) with a tendency towards distant metastasis [169,170,171]. Another study showed decreased HER2 expression in anaplastic and poorly differentiated thyroid cancer correlating with aggressive behavior [172]. High HER2/neu oncoprotein levels have been associated with extrathyroidal growth in medullary thyroid cancer and C-cell hyperplasia [173].
3.10.3. Glioblastoma Multiforme (GBM)
Glioblastoma multiforme is the most common primary malignant tumor of the central nervous system (CNS), and is regarded as one of the most chemo-resistant malignancies. Although HER2 is not expressed in adult CNS but its expression increases with increase in glioma cell anaplasia. HER2/neu overexpression has been reported in 20–90% patients with GBM and is a poor prognostic marker [174,175]. Mineo et al. demonstrated that use of trastuzumab in GBM cell lines (A172 and U251MG) expressing HER2/neu leads to apoptosis and cellular-dependent cytotoxicity of the cell lines [176].
3.10.4. Acute Lymphoblastic Leukemia (ALL)
In B-ALL or T-ALL, HER2/neu is known to be expressed in 30% of patients, with no expression in blasts [177,178]. Some studies have suggested HER2/neu overexpression to be related with chemoresistance and worse clinical outcomes in ALL patients [178,179]. Haen et al. reported no prognostic significance of HER2/neu in ALL patients on long-term follow-up of 15 years in accordance with the overall survival, disease-free survival or response to chemotherapy [180]. Using trastuzumab alone or in combination with other monoclonal antibodies, such as rituximab, for relapsed or refractory HER2/neu-positive ALL is a promising strategy [180,181].
3.10.5. Soft Tissue Sarcoma
Synovial sarcoma (SS) is a high-grade tumor which has t(X;18) (p11:q11) translocation and contributes to 10% of the sarcomas. Nuciforo et al. studied 13 patients with SS and found that increased HER2/neu expression correlated with statistically significant favorable clinical outcome [182] Another study conducted in Germany on patients with soft tissue sarcoma found no significant effect of HER2/neu expression on prognosis [183].
3.10.6. Wilms Tumor
Wilms tumor is an embryonal tumor arising from the remnants of renal tissue and is the most common solid malignancy in children. A study conducted by Babashahi et al. in 2013 found that epithelial differentiation (68.5% in 38 patients), especially in the early stages of tumor (81.5%), had higher HER2 expression [184]. Another study from Egypt on 28 patients suggested HER2/neu expression as a favorable indicator of overall survival and longer recurrence-free survival [185].
3.10.7. Melanoma
Melanoma is a primary skin cancer and the fifth leading cause of cancer-related death in men and women in the USA. In a large cohort of 600 patients, HER2/neu overexpression was found in 5.2% cases, many of them being primary cutaneous lesions with Breslow depth < 2 mm rather than metastatic or recurrence cancer [186].
4. Discussion
HER2/neu plays a significant role in the pathogenesis of various cancers and has garnered attention in the field of oncology due to its therapeutic potential. The overexpression, mutations, and gene amplification of HER2/neu in different malignancies have been the subject of extensive research over the years [17]. Given that HER2/neu is a targetable entity, it is evaluated in clinical settings, particularly for advanced malignancies. In clinical practice, HER2/neu testing may be performed for extra-mammary and extra-gastric tumors based on the clinician’s judgment and the availability of anti-HER2 agents for that specific malignancy of interest and based on the availability of clinical trials enrolling patients with HER2/neu biomarker positivity. In several malignancies, HER2/neu testing is performed in the metastatic setting for further lines of treatment. In non-small cell lung cancer, anti-HER2 agents are approved for use in previously treated patients with HER2/neu mutations [66]. Similarly, anti-HER2 agents are approved for use in HER2-positive advanced/metastatic CRC and endometrial carcinoma [54,88,90]. However, most of the anti-HER2 agents are currently utilized in clinical trial settings for specific extra-mammary and extra-gastric malignancies as they are not FDA-approved for use in all HER2/neu-positive cancers.
The prognostic and therapeutic significance of HER2 differs between breast, gastric/gastroesophageal, and other malignancies. Several anti-HER2 agents have been approved for use in breast, gastric, and gastroesophageal malignancies, and have been utilized for therapeutic purposes for several years [187,188,189]. Anti-HER2 agents are also approved for use in certain other malignancies, such as colorectal cancer, lung cancer, and uterine cancer [54,88,90,190]. However, the utilization of anti-HER2 agents is limited in extra-mammary and extra-gastric/gastroesophageal tumors, as studies have shown conflicting results. Additionally, several trials are still ongoing, as mentioned in our article.
Considering the prevalence of HER2/neu protein overexpression, gene amplification, and somatic mutation in several malignancies beyond breast, gastric, and gastroesophageal tumors, it is advisable to test for the HER2/neu biomarker, especially in metastatic cases where patients often require multiple lines of treatment. Testing for HER2/neu is beneficial in malignancies, such as lung cancer, endometrial cancer, and colorectal cancer, as anti-HER2 agents have been approved for use in the metastatic setting for these malignancies. HER2/neu testing can also be considered in other malignancies, particularly for patients who are candidates for clinical trials. However, there are challenges associated with HER2/neu testing in extra-mammary and extra-gastric/gastroesophageal settings. These challenges include the lack of testing algorithms, the absence of standardized laboratory testing, and the difficulties in obtaining insurance approval. It should be noted that HER2/neu testing is not approved in some of these malignancies, as mentioned in our article.
There are several knowledge gaps in our understanding regarding the prevalence of HER2/neu protein overexpression, gene amplification, and somatic mutation in extra-mammary and extra-gastric malignancies. The expansion of the HER2 spectrum to include HER2-low disease status (IHC 1+, 2+ and FISH negative) has sparked novel research in the field of HER2/neu disease. By gaining a better understanding of HER2-low disease status and its therapeutic potential, HER2-low can be utilized as a therapeutic target in extra-mammary and extra-gastric malignancies.
5. Conclusions
HER2/neu is one of the most well-characterized molecular markers in breast and gastric/gastroesophageal junction cancers, with several HER2-targeted agents currently being used alone or in combination with other agents for their treatment. As underscored in this review, HER2 protein overexpression, gene amplification, and somatic mutations have been reported and studied in many other different types of malignancies. With wide variation in HER2 protein expression and response rates to HER2 targeted therapy, there is a pressing need to establish a defined HER2 testing algorithm and reporting system for other solid and hematologic malignancies, as they currently exist only for breast and gastric cancers. This will allow to refine the HER2-targeted therapies for these malignancies.
Author Contributions
Conceptualization, F.A. and S.J.M.; methodology, F.A. and P.M.; data curation, F.A. and P.M.; writing—original draft preparation, F.A.; writing—review and editing, F.A., P.M., P.S., N.G., T.H.P., A.M.R., S.R.K.S. and S.J.M.; supervision, S.J.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable as this is a review article.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
We do not have any conflict of interest.
References
- Brandt-Rauf, P.W.; Pincus, M.R.; Carney, W.P. The c-erbB-2 protein in oncogenesis: Molecular structure to molecular epidemiology. Crit. Rev. Oncog. 1994, 5, 313–329. [Google Scholar] [CrossRef] [PubMed]
- Shih, C.; Padhy, L.C.; Murray, M.; Weinberg, R.A. Transforming genes of carcinomas and neuroblastomas introduced into mouse fibroblasts. Nature 1981, 290, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Schechter, A.L.; Hung, M.C.; Vaidyanathan, L.; Weinberg, R.A.; Yang-Feng, T.L.; Francke, U.; Ullrich, A.; Coussens, L. The neu gene: An erbB-homologous gene distinct from and unlinked to the gene encoding the EGF receptor. Science 1985, 229, 976–978. [Google Scholar] [CrossRef] [PubMed]
- Schechter, A.L.; Stern, D.F.; Vaidyanathan, L.; Decker, S.J.; Drebin, J.A.; Greene, M.I.; Weinberg, R.A. The neu oncogene: An erb-B-related gene encoding a 185,000-Mr tumour antigen. Nature 1984, 312, 513–516. [Google Scholar] [CrossRef] [PubMed]
- King, C.R.; Kraus, M.H.; Aaronson, S.A. Amplification of a novel v-erbB-related gene in a human mammary carcinoma. Science 1985, 229, 974–976. [Google Scholar] [CrossRef]
- Cho, H.S.; Mason, K.; Ramyar, K.X.; Stanley, A.M.; Gabelli, S.B.; Denney, D.W.; Leahy, D.J. Structure of the extracellular region of HER2 alone and in complex with the Herceptin Fab. Nature 2003, 421, 756–760. [Google Scholar] [CrossRef]
- Cho, H.S.; Leahy, D.J. Structure of the extracellular region of HER3 reveals an interdomain tether. Science 2002, 297, 1330–1333. [Google Scholar] [CrossRef]
- Nahta, R.; Yuan, L.X.H.; Zhang, B.; Kobayashi, R.; Esteva, F.J. Insulin-like growth factor-I receptor/human epidermal growth factor receptor 2 heterodimerization contributes to trastuzumab resistance of breast cancer cells. Cancer Res. 2005, 65, 11118–11128. [Google Scholar] [CrossRef]
- Sierke, S.L.; Cheng, K.; Kim, H.H.; Koland, J.G. Biochemical characterization of the protein tyrosine kinase homology domain of the ErbB3 (HER3) receptor protein. Biochem. J. 1997, 322, 757–763. [Google Scholar] [CrossRef]
- Sliwkowski, M.X.; Schaefer, G.; Akita, R.W.; Lofgren, J.A.; Fitzpatrick, V.D.; Nuijens, A.; Fendly, B.M.; Cerione, R.A.; Vandlen, R.L.; Carraway, K.L., 3rd. Coexpression of erbB2 and erbB3 proteins reconstitutes a high affinity receptor for heregulin. J. Biol. Chem. 1994, 269, 14661–14665. [Google Scholar] [CrossRef]
- Wilson, G.R.; Cramer, A.; Welman, A.; Knox, F.; Swindell, R.; Kawakatsu, H.; Clarke, R.B.; Dive, C.; Bundred, N.J. Activated c-SRC in ductal carcinoma in situ correlates with high tumour grade, high proliferation and HER2 positivity. Br. J. Cancer 2006, 95, 1410–1414. [Google Scholar] [CrossRef]
- Timms, J.F.; White, S.L.; O’Hare, M.J.; Waterfield, M.D. Effects of ErbB-2 overexpression on mitogenic signalling and cell cycle progression in human breast luminal epithelial cells. Oncogene 2002, 21, 6573–6586. [Google Scholar] [CrossRef]
- Penault-Llorca, F.; Bilous, M.; Dowsett, M.; Hanna, W.; Osamura, R.Y.; Rüschoff, J.; van de Vijver, M. Emerging technologies for assessing HER2 amplification. Am. J. Clin. Pathol. 2009, 132, 539–548. [Google Scholar] [CrossRef]
- Press, M.F.; Slamon, D.J.; Flom, K.J.; Park, J.; Zhou, J.Y.; Bernstein, L. Evaluation of HER-2/neu gene amplification and overexpression: Comparison of frequently used assay methods in a molecularly characterized cohort of breast cancer specimens. J. Clin. Oncol. 2002, 20, 3095–3105. [Google Scholar] [CrossRef]
- Graves, H.; Czerniecki, B.J. Circulating tumor cells in breast cancer patients: An evolving role in patient prognosis and disease progression. Pathol. Res. Int. 2011, 2011, 621090. [Google Scholar] [CrossRef]
- Cao, S.; Li, Y.; Li, J.; Li, C.F.; Zhang, W.; Yang, Z.Q.; Meng, S.D. Quantitative determination of HER2 expression by confocal microscopy assay in CTCs of breast cancer. Oncol. Rep. 2010, 23, 423–428. [Google Scholar]
- De, P.; Smith, B.R.; Leyland-Jones, B. Human epidermal growth factor receptor 2 testing: Where are we? J. Clin. Oncol. 2010, 28, 4289–4292. [Google Scholar] [CrossRef]
- Lehmann-Che, J.; Amira-Bouhidel, F.; Turpin, E.; Antoine, M.; Soliman, H.; Legres, L.; Bocquet, C.; Bernoud, R.; Flandre, E.; Varna, M.; et al. Immunohistochemical anmolecular analyses of HER2 status in breast cancers are highly concordant and complementary approaches. Br. J. Cancer 2011, 104, 1739–1746. [Google Scholar] [CrossRef]
- Rubin, S.C.; Finstad, C.L.; Federici, M.G.; Scheiner, L.; Lloyd, K.O.; Hoskins, W.J. Prevalence and significance of HER-2/neu expression in early epithelial ovarian cancer. Cancer 1994, 73, 1456–1459. [Google Scholar] [CrossRef]
- Seki, A.; Yoshinouchi, M.; Seki, N.; Kodama, J.; Miyagi, Y.; Kudo, T. Detection of c-erbB-2 and FGF-3 (INT-2) gene amplification in epithelial ovarian cancer. Int. J. Oncol. 2000, 17, 103–106. [Google Scholar] [CrossRef]
- Gao, D.; Lu, Y.; Lu, Y.; Wang, Y.; Zhang, B.; Wu, B. Significance of HER-2/neu expression in ovarian epithelial tumours. Zhonghua Bing Li Xue Za Zhi 2002, 31, 268–270. [Google Scholar] [PubMed]
- Hogdall, E.V.; Christensen, L.; Kjaer, S.K.; Blaakaer, J.; Bock, J.E.; Glud, E.; Nørgaard-Pedersen, B.; Høgdall, C.K. Distribution of HER-2 overexpression in ovarian carcinoma tissue and its prognostic value in patients with ovarian carcinoma: From the Danish MALOVA Ovarian Cancer Study. Cancer 2003, 98, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Bookman, M.A.; Darcy, K.M.; Clarke-Pearson, D.; Boothby, R.A.; Horowitz, I.R. Evaluation of monoclonal humanized anti-HER2 antibody, trastuzumab in patients with recurrent or refractory ovarian or primary peritoneal carcinoma with overexpression of HER2: A phase II trial of the Gynaecologic Oncology Group. J. Clin. Oncol. 2003, 21, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Camilleri-Broet, S.; Hardy-Bessard, A.C.; Le Tourneau, A.; Paraiso, D.; Levrel, O.; Leduc, B.; Bain, S.; Orfeuvre, H.; Audouin, J.; Pujade-Lauraine, E. HER-2 overexpression is an independent marker of poor prognosis of advanced primary ovarian carcinoma: A multicentre study of the GINECO group. Ann. Oncol. 2004, 15, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Mano, M.; Awada, A.; Di Leo, A.; Durbecq, V.; Paesmans, M.; Cardoso, F.; Larsimont, D.; Piccart, M. Rates of topoisomerase II-alpha and HER-2 gene amplification and expression in epithelial ovarian carcinoma. Gynecol. Oncol. 2004, 92, 887–889. [Google Scholar] [CrossRef]
- Lee, C.H.; Huntsman, D.G.; Cheang, M.C.; Parker, R.L.; Brown, L.; Hoskins, P.; Miller, D.; Gilks, C.B. Assessment of Her-1, Her-2 and Her-3 expression and Her-2 amplification in advanced stage ovarian carcinoma. Int. J. Gynecol. Pathol. 2005, 24, 147–152. [Google Scholar] [CrossRef]
- Tuefferd, M.; Coutier, J.; Penault-Llorca, F.; Vincent-Salomon, A.; Broet, P.; Guastalla, J.P.; Allouache, D.; Combe, M.; Weber, B.; Pujade-Lauraine, E.; et al. HER2 status in ovarian carcinomas: A multicentre GINECO study of 320 patients. PLoS ONE 2007, 2, e1138. [Google Scholar] [CrossRef]
- Sasaki, N.; Kudoh, K.; Kita, T.; Tsuda, H.; Furuya, K.; Kikuchi, Y. Effect of HER-2/neu overexpression on chemoresistance and prognosis in ovarian carcinoma. J. Obstet. Gynaecol. Res. 2007, 33, 17–23. [Google Scholar] [CrossRef]
- Sueblinvong, T.; Manchana, T.; Khemapech, N.; Triratanachat, S.; Termrungruanglert, W.; Tresukosol, D. Lack of prognostic significance of HER-2/neu in early epithelial ovarian cancer. Asian Pac. J. Cancer Prev. 2007, 8, 502–506. [Google Scholar]
- Steffensen, K.D.; Waldstrom, M.; Jeppesen, U.; Jakobsen, E.; Brandslund, I.; Jakobsen, A. The prognostic importance of cyclooxygenase 2 and HER2 expression in epithelial ovarian cancer. Int. J. Gynecol. Cancer 2007, 17, 798–807. [Google Scholar] [CrossRef]
- Steffensen, K.D.; Waldstrom, M.; Andersen, R.F.; Olsen, D.A.; Jeppesen, U.; Knudsen, H.J.; Brandslund, I.; Jakobsen, A. Protein levels and gene expressions of the epidermal growth factor receptors, HER1, HER2, HER3 and HER4 in benign and malignant ovarian tumors. Int. J. Oncol. 2008, 33, 195–204. [Google Scholar] [CrossRef]
- Vermeij, J.; Teugels, E.; Bourgain, C.; Xiangming, J.; Ghislain, V.; Neyns, B.; De Greve, J. Genomic activation of the EGFR and HER2-neu genes in a significant proportion of invasive epithelial ovarian cancers. BMC 2008, 8, 3. [Google Scholar] [CrossRef]
- Chekerov, R.; Koensgen, D.; Klaman, I.; Rosenthal, A.; Oskay-Oezcelik, G.; Mustea, A.; Lightenegger, W.; Dahl, E.; Sehouli, J. Tumor- and stromal cell-specific expression of topoisomerase IIα and HER-2/neu in primary and recurrent ovarian cancer: Results of a prospective study. Mol. Med. Rep. 2009, 2, 1011–1016. [Google Scholar] [CrossRef]
- Sylvia, M.T.; Kumar, S.; Dasari, P. The expression of immunohistochemical markers estrogen receptor, progesterone receptor, Her-2-neu, p53 and Ki-67 in epithelial ovarian tumors and its correlation with clinicopathologic variables. Indian J. Pathol. Microbiol. 2012, 55, 33–37. [Google Scholar] [CrossRef]
- Jafri, A.; Rizvi, S. Frequency of Her2/Neu Protein Expression in Ovarian Epithelial Cancers. J. Coll. Physic. Surg. Pak. 2017, 27, 544–546. [Google Scholar]
- Pankaj, S.; Kumari, J.; Choudhary, V.; Kumari, A.; Kumari, S.; Kumari, A.; Nazneen, S.; Madhawi, R.; Kumar, S. Prognostic Value of HER-2/neu Gene Amplification in Epithelial Ovarian Carcinoma. J. Obstet. Gynaecol. India. 2019, 69 (Suppl. S2), 177–181. [Google Scholar] [CrossRef]
- Makhija, S.; Amler, L.C.; Glenn, D.; Ueland, F.R.; Gold, M.A.; Dizon, D.S.; Paton, V.; Lin, C.Y.; Januario, T.; Ng, K.; et al. Clinical activity of gemcitabine plus pertuzumab in platinum-resistant ovarian cancer, fallopian tube cancer, or primary peritoneal cancer. J. Clin. Oncol. 2010, 28, 1215–1223. [Google Scholar] [CrossRef]
- Lin, W.-L.; Kuo, W.-H.; Chen, F.-L.; Lee, M.-Y.; Ruan, A.; Tyan, Y.-S.; Hsu, J.-D.; Chiang, H.; Han, C.-P. Identification of the coexisting HER2 gene amplification and novel mutations in the HER2 protein-overexpressed mucinous epithelial ovarian cancer. Ann. Surg. Oncol. 2011, 18, 2388–2394. [Google Scholar] [CrossRef]
- Lassus, H.; Sihto, H.; Leminen, A.; Joensuu, H.; Isola, J.; Nupponen, N.N.; Butzow, R. Gene amplification, mutation and protein expression of EGFR and mutations of ERBB2 in serousovarian carcinoma. J. Mol. Med. 2006, 84, 671–681. [Google Scholar] [CrossRef]
- Berchuck, A.; Kamel, A.; Whitaker, R.; Kerns, B.; Olt, G.; Kinney, R.; Soper, J.T.; Dodge, R.; Clarke-Pearson, D.L.; Marks, P.; et al. Overexpression of HER-2/neu is associated with poor survival in advanced epithelial ovarian cancer. Cancer Res. 1990, 50, 4087–4091. [Google Scholar]
- Rolitsky, C.D.; Theil, K.S.; McGaughy, V.R.; Copeland, L.J.; Niemann, T.H. HER-2/neu amplification and overexpression in endometrial carcinoma. Int. J. Gynecol. Pathol. 1999, 18, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Grushko, T.A.; Filiaci, V.L.; Mundt, A.J.; Ridderstråle, K.; Olopade, O.I.; Fleming, G.F.; Gynecologic Oncology Group. An exploratory analysis of HER-2 amplification and overexpression in advanced endometrial carcinoma: A Gynecologic Oncology Group study. Gynecol. Oncol. 2008, 108, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Santin, A.D.; Bellone, S.; Van Stedum, S.; Bushen, W.; Palmieri, M.; Siegel, E.R.; De Las Casas, L.E.; Roman, J.J.; Burnett, A.; Pecorelli, S. Amplification of c-erbB2 oncogene: A major prognostic indicator in uterine serous papillary carcinoma. Cancer 2005, 104, 1391–1397. [Google Scholar] [CrossRef] [PubMed]
- Santin, A.D.; Bellone, S.; Gokden, M.; Palmieri, M.; Dunn, D.; Agha, J.; Roman, J.J.; Hutchins, L.; Pecorelli, S.; O’Brien, T.; et al. Overexpression of HER-2/neu in uterine serous papillary cancer. Clin. Cancer Res. 2002, 8, 1271–1279. [Google Scholar] [PubMed]
- Slomovitz, B.M.; Broaddus, R.R.; Burke, T.W.; Sneige, N.; Soliman, P.T.; Wu, W.; Sun, C.C.; Munsell, M.F.; Gershenson, D.M.; Lu, K.H. Her-2/neu overexpression and amplification in uterine papillary carcinoma. J. Clin. Oncol. 2004, 22, 3126–3132. [Google Scholar] [CrossRef] [PubMed]
- Santin, A.D.; Bellone, S.; Siegel, E.R.; Palmieri, M.; Thomas, M.; Cannon, M.J.; Kay, H.H.; Roman, J.J.; Burnett, A.; Pecorelli, S. Racial differences in the overexpression of epidermal growth factor type II receptor (HER2/neu): A major prognostic indicator in uterine serous papillary cancer. Am. J. Obstet. Gynecol. 2005, 192, 813–818. [Google Scholar] [CrossRef]
- Diaz-Montes, T.P.; Ji, H.; Smith Sehdev, A.E.; Zahurak, M.L.; Kurman, J.; Armstrong, D.K.; Bristow, R.E. Clinical significance of Her-2/neu overexpression in uterine serous carcinoma. Gynecol. Oncol. 2006, 100, 139–144. [Google Scholar] [CrossRef]
- Villella, J.A.; Cohen, S.; Smith, D.H.; Hibshoosh, H.; Hershman, D. HER-2/neu overexpression in uterine papillary serous cancers and its possible therapeutic implications. Int. J. Gynecol. Cancer 2006, 16, 1897–1902. [Google Scholar] [CrossRef]
- Odicino, F.E.; Bignotti, E.; Rossi, E.; Pasinneti, E.; Tassi, R.A.; Donzelli, C.; Falchetti, M.; Fontana, P.; Grigolato, P.G.; Pecorelli, S. HER-2/neu overexpression and amplification in uterine serous papillary carcinoma: Comparative analysis of immunohistochemistry, real-time reverse transcription-polymerase chain reaction, and fluorescence in situ hybridization. Int. J. Gynecol. Cancer 2008, 18, 14–21. [Google Scholar] [CrossRef]
- Ren, Y.; Wang, H.; Zhou, X.; Yang, W.; Huang, X.; Lu, Y.; Shi, D. Clinicopathological characteristics and her-2/neu status in chinese patients with uterine papillary serous carcinoma. ISRN Obstet. Gynecol. 2011, 2011, 575327. [Google Scholar] [CrossRef]
- Togami, S.; Sasajima, Y.; Oi, T.; Ishikawa, M.; Onda, T.; Ikeda, S.-I.; Kato, T.; Tsuda, H.; Kasamatsu, T. Clinicopathological and prognostic impact of human epidermal growth factor receptor type 2 (HER2) and hormone receptor expression in uterine papillary serous carcinoma. Cancer Sci. 2012, 103, 926–932. [Google Scholar] [CrossRef]
- Banet, N.; Shahi, M.; Batista, D.; Yonescu, R.; Tanner, E.J.; Fader, A.N.; Cimino-Mathews, A. HER-2 Amplification in Uterine Serous Carcinoma and Serous Endometrial Intraepithelial Carcinoma. Am. J. Surg. Pathol. 2021, 45, 708–715. [Google Scholar] [CrossRef]
- Fleming, G.F.; Sill, M.W.; Darcy, K.M.; McMeekin, D.S.; Thigpen, J.T.; Adler, L.M.; Berek, J.S.; Chapman, J.A.; DiSilvestro, P.A.; Horowitz, I.R.; et al. Phase II trial of trastuzumab in women with advanced or recurrent, HER2-positive endometrial carcinoma: A Gynecologic Oncology Group study. Gynecol Oncol. 2010, 116, 15–20. [Google Scholar] [CrossRef]
- Tymon-Rosario, J.; Siegel, E.R.; Bellone, S.; Harold, J.; Adjei, N.; Zeybek, B.; Mauricio, D.; Altwerger, G.; Menderes, G.; Ratner, E.; et al. Trastuzumab tolerability in the treatment of advanced (stage III-IV) or recurrent uterine serous carcinomas that overexpress HER2/neu. Gynecol. Oncol. 2021, 163, 93–99. [Google Scholar] [CrossRef]
- Ai, X.; Song, Z.; Jian, H.; Zhou, Z.; Chen, Z.; Yu, Y.; Li, Z.; Lu, S. Pyrotinib combined with thalidomide in advanced non-small-cell lung cancer patients harboring HER2 exon 20 insertions (PRIDE): Protocol of an open-label, single-arm phase II trial. BMC Cancer 2021, 21, 1033. [Google Scholar] [CrossRef]
- Park, D.I.; Oh, S.J.; Park, S.H.; Yun, J.W.; Kim, H.J.; Cho, Y.K.; Sung, I.K.; Sohn, C.I.; Jeon, W.K.; Kim, B.I.; et al. Clinical significance of HER-2/neu expression in colon cancer. Korean J. Gastroenterol. 2004, 44, 147–152. [Google Scholar]
- Nakamura, H.; Kawasaki, N.; Taguchi, M.; Kabasawa, K. Association of HER2 overexpression with prognosis in non-small cell lung carcinoma: A metaanalysis. Cancer 2005, 103, 1865–1873. [Google Scholar] [CrossRef]
- Liu, L.; Shao, X.; Gao, W.; Bai, J.; Wang, R.; Huang, P.; Yin, Y.; Liu, P.; Shu, Y. The role of human epidermal growth factor receptor 2 as a prognostic factor in lung cancer: A meta-analysis of published data. J. Thorac. Oncol. 2010, 5, 1922–1932. [Google Scholar] [CrossRef]
- Shigematsu, H.; Takahashi, T.; Nomura, M.; Majmudar, K.; Suzuki, M.; Lee, H.; Wistuba, I.I.; Fong, K.M.; Toyooka, S.; Shimizu, N.; et al. Somatic mutations of the HER2 kinase domain in lung adenocarcinomas. Cancer Res. 2005, 65, 1642–1646. [Google Scholar] [CrossRef]
- Stephens, P.; Hunter, C.; Bignell, G.; Edkins, S.; Davies, H.; Teague, J.; Stevens, C.; O’Meara, S.; Smith, R.; Parker, A.; et al. Lung cancer: Intragenic ERBB2 kinase mutations in tumours. Nature 2004, 431, 525–526. [Google Scholar] [CrossRef]
- Langer, C.J.; Stephenson, P.; Thor, A.; Vangel, M.; Johnson, D.H.; Eastern Cooperative Oncology Group Study 2598. Trastuzumab in the treatment of advanced non-small-cell lung cancer: Is there a role? Focus on Eastern Cooperative Oncology Group study 2598. J. Clin. Oncol. 2004, 22, 1180–1187. [Google Scholar] [CrossRef] [PubMed]
- Zinner, R.G.; Glisson, B.S.; Fossella, F.V.; Pisters, K.M.; Kies, M.S.; Lee, P.M.; Massarelli, E.; Sabloff, B.; Fritsche, H.A., Jr.; Ro, J.Y.; et al. Trastuzumab in combination with cisplatin and gemcitabine in patients with Her2-overexpressing, untreated, advanced non-small cell lung cancer: Report of a phase II trial and findings regarding optimal identification of patients with Her2-overexpressing disease. Lung Cancer 2004, 44, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Lara, P.N., Jr.; Laptalo, L.; Longmate, J.; Lau, D.H.; Gandour-Edwards, R.; Gumerlock, P.H.; Doroshow, J.H.; Gandara, D.R.; California Cancer Consortium. Trastuzumab plus docetaxel in HER2/neu-positive non-small-cell lung cancer: A California Cancer Consortium screening and phase II trial. Clin. Lung Cancer 2004, 5, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Li, B.T.; Shen, R.; Buonocore, D.; Olah, Z.T.; Ni, A.; Ginsberg, M.S.; Ulaner, G.A.; Offin, M.; Feldman, D.; Hembrough, T.; et al. Ado-Trastuzumab Emtansine for Patients with HER2-Mutant Lung Cancers: Results from a Phase II Basket Trial. J. Clin. Oncol. 2018, 36, 2532–2537. [Google Scholar] [CrossRef]
- Peters, S.; Stahel, R.; Bubendorf, L.; Bonomi, P.; Villegas, A.; Kowalski, D.M.; Baik, C.S.; Isla, D.; Carpeno, J.C.; Garrido, P.; et al. Trastuzumab Emtansine (T-DM1) in Patients with Previously Treated HER2-Overexpressing Metastatic Non-Small Cell Lung Cancer: Efficacy, Safety, and Biomarkers. Clin. Cancer Res. 2019, 25, 64–72. [Google Scholar] [CrossRef]
- Li, B.T.; Smit, E.F.; Goto, Y.; Nakagawa, K.; Udagawa, H.; Mazières, J.; Nagasaka, M.; Bazhenova, L.; Saltos, A.N.; Felip, E.; et al. Trastuzumab Deruxtecan in HER2-Mutant Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2022, 386, 241–251. [Google Scholar] [CrossRef]
- Kris, M.G.; Camidge, D.R.; Giaccone, G.; Hida, T.; Li, B.T.; O’Connell, J.; Taylor, I.; Zhang, H.; Arcila, M.E.; Goldberg, Z.; et al. Targeting HER2 aberrations as actionable drivers in lung cancers: Phase II trial of the pan-HER tyrosine kinase inhibitor dacomitinib in patients with HER2-mutant or amplified tumors. Ann. Oncol. 2015, 26, 1421–1427. [Google Scholar] [CrossRef]
- Dziadziuszko, R.; Smit, E.F.; Dafni, U.; Wolf, J.; Wasąg, B.; Biernat, W.; Finn, S.P.; Kammler, R.; Tsourti, Z.; Rabaglio, M.; et al. Afatinib in NSCLC with HER2 Mutations: Results of the Prospective, Open-Label Phase II NICHE Trial of European Thoracic Oncology Platform (ETOP). J. Thorac Oncol. 2019, 14, 1086–1094. [Google Scholar] [CrossRef]
- Fan, Y.; Chen, J.; Zhou, C.; Wang, H.; Shu, Y.; Zhang, J.; Hua, H.; Huang, D.C.-L.; Zhou, C. Afatinib in patients with advanced non-small cell lung cancer harboring HER2 mutations, previously treated with chemotherapy: A phase II trial. Lung Cancer 2020, 147, 209–213. [Google Scholar] [CrossRef]
- Buttitta, F.; Barassi, F.; Fresu, G.; Felicioni, L.; Chella, A.; Paolizzi, D.; Lattanzio, G.; Salvatore, S.; Camplese, P.P.; Rosini, S.; et al. Mutational analysis of the HER2 gene in lung tumors from Caucasian patients: Mutations are mainly present in adenocarcinomas with bronchoalveolar features. Int. J. Cancer 2006, 119, 2586–2591. [Google Scholar] [CrossRef]
- Sasaki, H.; Shimizu, S.; Endo, K.; Takada, M.; Kawahara, M.; Tanaka, H.; Matsumura, A.; Iuchi, K.; Haneda, H.; Suzuki, E.; et al. EGFR and erbB2 mutation status in Japanese lung cancer patients. Int. J. Cancer 2006, 118, 180–184. [Google Scholar] [CrossRef]
- Sun, Y.; Ren, Y.; Fang, Z.; Li, C.; Fang, R.; Gao, B.; Han, X.; Tian, W.; Pao, W.; Bin Chen, G.; et al. Lung adenocarcinoma from East Asian never-smokers is a disease largely defined by targetable oncogenic mutant kinases. J. Clin. Oncol. 2010, 28, 4616–4620. [Google Scholar] [CrossRef]
- Tomizawa, K.; Suda, K.; Onozato, R.; Kosaka, T.; Endoh, H.; Sekido, Y.; Shigematsu, H.; Kuwano, H.; Yatabe, Y.; Mitsudomi, T. Prognostic and predictive implications of HER2/ERBB2/neu gene mutations in lung cancers. Lung Cancer 2011, 74, 139–144. [Google Scholar] [CrossRef]
- Li, C.; Sun, Y.; Fang, R.; Han, X.; Luo, X.; Wang, R.; Pan, Y.; Hu, H.; Zhang, Y.; Pao, W.; et al. Lung adenocarcinomas with HER2-activating mutations are associated with distinct clinical features and EGFR/HER2 copy number gains. J. Thorac. Oncol. 2012, 7, 85–89. [Google Scholar] [CrossRef]
- Arcila, M.E.; Chaft, J.E.; Nafa, K.; Roy-Chowduri, S.; Lau, C.; Zaidinski, M.; Paik, P.K.; Zakowski, M.F.; Kris, M.G.; Ladanyi, M. Prevalence, clinicopathologic associations and molecular spectrum of ERBB2 (HER2) tyrosine kinase mutations in lung adenocarcinomas. Clin. Cancer Res. 2012, 18, 4910–4918. [Google Scholar] [CrossRef]
- Mazieres, J.; Peters, S.; Lepage, B.; Cortot, A.B.; Barlesi, F.; Beau-Faller, M.; Besse, B.; Blons, H.; Mansuet-Lupo, A.; Urban, T.; et al. Lung cancer that harbors an HER2 mutation: Epidemiologic characteristics and therapeutic perspectives. J. Clin. Oncol. 2013, 31, 1997–2003. [Google Scholar] [CrossRef]
- Cappuzzo, F.; Gregorc, V.; Rossi, E.; Cancellieri, A.; Magrini, E.; Paties, C.T.; Ceresoli, G.; Lombardo, L.; Bartolini, S.; Calandri, C.; et al. Gefitinib in pretreated non-small-cell lung cancer (NSCLC): Analysis of efficacy and correlation with HER2 and epidermal growth factor receptor expression in locally advanced or metastatic NSCLC. J. Clin. Oncol. 2003, 21, 2658–2663. [Google Scholar] [CrossRef]
- Gatzemeier, U.; Growth, G.; Hirsh, V.; Butts, C.; Van Zandwijk, N.; Shepherd, F.; Rosso, R.; Howell, J. A randomized phase II study of gemcitabine/cisplatin alone and with herceptin in patients with HER-2-positive non-small cell lung cancer. Proc. ECCO 2001, 37 (Suppl. S6), S50. [Google Scholar]
- Clamon, G.; Herndon, J.; Kern, J.; Govindan, R.; Garst, J.; Watson, D.; Green, M.; Cancer and Leukemia Group, B. Lack of trastuzumab activity in nonsmall cell lung carcinoma with overexpression of erb-B2: 39810: A phase II trial of Cancer and Leukemia Group B. Cancer 2005, 104, 1670–1675. [Google Scholar] [CrossRef]
- Krug, L.M.; Miller, V.A.; Patel, J.; Crapanzano, J.; Azzoli, C.G.; Gomez, J.; Kris, M.G.; Heelan, R.T.; Pizzo, B.; Tyson, L.; et al. Randomized phase II study of weekly docetaxel plus trastuzumab versus weekly paclitaxel plus trastuzumab in patients with previously untreated advanced nonsmall cell lung carcinoma. Cancer. 2005, 10, 2149–2155. [Google Scholar] [CrossRef]
- De Langen, A.J.; Jebbink, M.; Hashemi, S.M.S.; Kuiper, J.L.; de Bruin-Visser, J.; Monkhorst, K.; Thunnissen, E.; Smit, E.F. Trastuzumab and paclitaxel in patients with EGFR mutated NSCLC that express HER2 after progression on EGFR TKI treatment. Br. J. Cancer 2018, 119, 558–564. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Soung, Y.H.; Seo, S.H.; Kim, S.Y.; Park, C.H.; Wang, Y.P.; Park, K.; Nam, S.W.; Park, W.S.; Kim, S.H.; et al. Somatic mutations of ERBB2 kinase domain in gastric, colorectal and breast carcinomas. Clin. Cancer Res. 2006, 12, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Shabbir, A.; Mirza, T.; Khalid, A.B.; Qureshi, M.A.; Asim, S.A. Frequency of Her2/neu expression in colorectal adenocarcinoma: A study from developing South Asian Country. BMC Cancer 2016, 16, 855. [Google Scholar] [CrossRef] [PubMed]
- Ingold Heppner, B.; Behrens, H.M.; Balschun, K.; Haag, J.; Krüger, S.; Becker, T.; Röcken, C. HER2/neu testing in primary colorectal carcinoma. Br. J. Cancer 2014, 111, 1977–1984. [Google Scholar] [CrossRef] [PubMed]
- Conradi, L.C.; Styczen, H.; Sprenger, T.; Wolff, H.A.; Rödel, C.; Nietert, M.; Homayounfar, K.; Gaedcke, J.; Kitz, J.; Talaulicar, R.; et al. Frequency of HER-2 positivity in rectal cancer and prognosis. Am. J. Surg. Pathol. 2013, 37, 522–531. [Google Scholar] [CrossRef]
- Rubinson, D.A.; Hochster, H.S.; Ryan, D.P.; Wolpin, B.M.; McCleary, N.J.; Abrams, T.A.; Chan, J.A.; Iqbal, S.; Lenz, H.J.; Lim, D.; et al. Multi-drug inhibition of the HER pathway in metastatic colorectal cancer: Results of a phase I study of pertuzumab plus cetuximab in cetuximab-refractory patients. Investig. New Drugs. 2014, 32, 113–122. [Google Scholar] [CrossRef]
- Sartore-Bianchi, A.; Trusolino, L.; Martino, C.; Bencardino, K.; Lonardi, S.; Bergamo, F.; Zagonel, V.; Leone, F.; Depetris, I.; Martinelli, E.; et al. Dual-targeted therapy with trastuzumab and lapatinib in treatment-refractory, KRAS codon 12/13 wild-type, HER2-positive metastatic colorectal cancer (HERACLES): A proof-of-concept, multicentre, open-label, phase 2 trial. Lancet Oncol. 2016, 17, 738–746, Erratum in Lancet Oncol. 2016, 17, e420. [Google Scholar] [CrossRef]
- Meric-Bernstam, F.; Hurwitz, H.; Raghav, K.P.S.; McWilliams, R.R.; Fakih, M.; VanderWalde, A.; Swanton, C.; Kurzrock, R.; Burris, H.; Sweeney, C.; et al. Pertuzumab plus trastuzumab for HER2-amplified metastatic colorectal cancer (MyPathway): An updated report from a multicentre, open-label, phase 2a, multiple basket study. Lancet Oncol. 2019, 20, 518–530. [Google Scholar] [CrossRef]
- Sartore-Bianchi, A.; Lonardi, S.; Martino, C.; Fenocchio, E.; Tosi, F.; Ghezzi, S.; Leone, F.; Bergamo, F.; Zagonel, V.; Ciardiello, F.; et al. Pertuzumab and trastuzumab emtansine in patients with HER2-amplified metastatic colorectal cancer: The phase II HERACLES-B trial. ESMO Open 2020, 5, e000911. [Google Scholar] [CrossRef]
- Siena, S.; Di Bartolomeo, M.; Raghav, K.; Masuishi, T.; Loupakis, F.; Kawakami, H.; Yamaguchi, K.; Nishina, T.; Fakih, M.; Elez, E.; et al. Trastuzumab deruxtecan (DS-8201) in patients with HER2-expressing metastatic colorectal cancer (DESTINY-CRC01): A multicentre, open-label, phase 2 trial. Lancet Oncol. 2021, 22, 779–789. [Google Scholar] [CrossRef]
- Rossi, H.A.; Liu, Q.; Banner, B.; Hsieh, C.C.; Savas, L.; Savarese, D. The prognostic value of invariant chain (Ii) and Her-2/neu expression in curatively resected colorectal cancer. Cancer J. 2002, 8, 268–275. [Google Scholar] [CrossRef]
- Knösel, T.; Yu, Y.; Stein, U.; Schwabe, H.; Schlüns, K.; Schlag, P.M.; Dietel, M.; Petersen, I. Overexpression of c-erbB-2 protein correlates with chromosomal gain at the c-erbB-2 locus and patient survival in advanced colorectal carcinomas. Clin. Exp. Metastasis 2002, 19, 401–407. [Google Scholar] [CrossRef]
- Nathanson, D.R.; Culliford, A.T., IV; Shia, J.; Chen, B.; D’Alessio, M.; Zeng, Z.S.; Nash, G.M.; Gerald, W.; Barany, F.; Paty, P.B. HER 2/neu expression and gene amplification in colon cancer. Int. J. Cancer 2003, 105, 796–802. [Google Scholar] [CrossRef]
- Schuell, B.; Gruenberger, T.; Scheithauer, W.; Zielinski, C.; Wrba, F. HER 2/neu protein expression in colorectal cancer. BMC Cancer 2006, 6, 123. [Google Scholar] [CrossRef]
- Kountourakis, P.; Pavlakis, K.; Psyrri, A.; Rontogianni, D.; Xiros, N.; Patsouris, E.; Pectasides, D.; Economopoulos, T. Clinicopathologic significance of EGFR and Her-2/neu in colorectal adenocarcinomas. Cancer J. 2006, 12, 229–236. [Google Scholar] [CrossRef]
- Park, D.I.; Kang, M.S.; Oh, S.J.; Kim, H.J.; Cho, Y.K.; Sohn, C.I.; Jeon, W.K.; Kim, B.I.; Han, W.K.; Kim, H.; et al. HER-2/neu overexpression is an independent prognostic factor in colorectal cancer. Int. J. Colorectal. Dis. 2007, 22, 491–497. [Google Scholar] [CrossRef]
- Ismail, H.M.; El-Baradie, M.; Moneer, M.; Khorshid, O.; Touny, A. Clinico-Pathological and Prognostic Significance of p53, Bcl-2 and Her-2/neu Protein Markers in Colorectal Cancer Using Tissue Microarray. J. Egypt. Natl. Cancer Inst. 2007, 19, 3–14. [Google Scholar]
- Kavanagh, D.O.; Chambers, G.; O’Grady, L.; Barry, K.M.; Waldron, R.P.; Bennani, F.; Eustace, P.W.; Tobbia, I. Is overexpression of HER-2 a predictor of prognosis in colorectal cancer? BMC Cancer 2009, 9, 1. [Google Scholar] [CrossRef]
- Marx, A.H.; Burandt, E.C.; Choschzick, M.; Simon, R.; Yekebas, E.; Kaifi, J.T.; Mirlacher, M.; Atanackovic, D.; Bokemeyer, C.; Fiedler, W.; et al. Heterogenous high-level HER-2 amplification in a small subset of colorectal cancers. Hum. Pathol. 2010, 41, 1577–1585. [Google Scholar] [CrossRef]
- Li, Q.; Wang, D.; Li, J.; Chen, P. Clinicopathological and prognostic significance of HER-2/neu and VEGF expression in colon carcinomas. BMC Cancer 2011, 11, 277. [Google Scholar] [CrossRef]
- Herreros-Villanueva, M.; Rodrigo, M.; Claver, M.; Muñiz, P.; Lastra, E.; García-Girón, C.; Coma del Corral, M.J. KRAS, BRAF, EGFR and HER2 gene status in a Spanish population of colorectal cancer. Mol. Biol. Rep. 2011, 38, 1315–1320. [Google Scholar] [CrossRef] [PubMed]
- Pappas, A.; Lagoudianakis, E.; Seretis, C.; Tsiambas, E.; Koronakis, N.; Toutouzas, K.; Katergiannakis, V.; Manouras, A. Clinical role of HER-2/neu expression in colorectal cancer. J. BUON 2013, 18, 98–104. [Google Scholar] [PubMed]
- Kwak, Y.; Yun, S.; Nam, S.K.; Seo, A.N.; Lee, K.S.; Shin, E.; Oh, H.K.; Kim, D.W.; Kang, S.B.; Kim, W.H.; et al. Comparative analysis of the EGFR, HER2, c-MYC, and MET variations in colorectal cancer determined by three different measures: Gene copy number gain, amplification status and the 2013 ASCO/CAP guideline criterion for HER2 testing of breast cancer. J. Transl. Med. 2017, 15, 167. [Google Scholar] [CrossRef] [PubMed]
- Ross, J.S.; Fakih, M.; Ali, S.M.; Elvin, J.A.; Schrock, A.B.; Suh, J.; Vergilio, J.A.; Ramkissoon, S.; Severson, E.; Daniel, S.; et al. Targeting HER2 in colorectal cancer: The landscape of amplification and short variant mutations in ERBB2 and ERBB3. Cancer 2018, 124, 1358–1373. [Google Scholar] [CrossRef] [PubMed]
- Hasan, R.; Bhatt, D.; Khan, S.; Khan, V.; Verma, A.K.; Anees, A.; Dev, K. Association of Her-2 Expression and Clinicopathological Parameters in Colorectal Carcinoma in Indian Population. Open Access Maced. J. Med. Sci. 2018, 7, 6–11. [Google Scholar] [CrossRef]
- Richman, S.D.; Southward, K.; Chambers, P.; Cross, D.; Barrett, J.; Hemmings, G.; Taylor, M.; Wood, H.; Hutchins, G.; Foster, J.M.; et al. HER2 overexpression and amplification as a potential therapeutic target in colorectal cancer: Analysis of 3256 patients enrolled in the QUASAR, FOCUS and PICCOLO colorectal cancer trials. J. Pathol. 2016, 238, 562–570. [Google Scholar] [CrossRef]
- Ramanathan, R.K.; Hwang, J.J.; Zamboni, W.C.; Sinicrope, F.A.; Safran, H.; Wong, M.K.; Earle, M.; Brufsky, A.; Evans, T.; Troetschel, M.; et al. Low overexpression of HER-2/neu in advanced colorectal cancer limits the usefulness of trastuzumab (Herceptin) and irinotecan as therapy. A phase II trial. Cancer Investig. 2004, 22, 858–865. [Google Scholar] [CrossRef]
- Hashimoto, K.; Yamamoto, H.; Shiratsuchi, H.; Nakashima, T.; Tamiya, S.; Nishiyama, K.I.; Higaki, Y.; Komune, S.; Tsuneyoshi, M.; Oda, Y. HER-2/neu gene amplification in carcinoma ex pleomorphic adenoma in relation to progression and prognosis: A chromogenic in-situ hybridization study. Histopathology 2012, 60, E131–E142. [Google Scholar] [CrossRef]
- Haddad, R.; Colevas, A.; Krane, J.F.; Cooper, D.; Glisson, B.; Amrein, P.C.; Weeks, L.; Costello, R.; Posner, M. Herceptin in patients with advanced or metastatic salivary gland carcinomas. A phase II study. Oral Oncol. 2003, 39, 724–727. [Google Scholar] [CrossRef]
- Agulnik, M.; Cohen, E.W.; Cohen, R.B.; Chen, E.X.; Vokes, E.E.; Hotte, S.J.; Winquist, E.; Laurie, S.; Hayes, D.N.; Dancey, J.E.; et al. Phase II study of lapatinib in recurrent or metastatic epidermal growth factor receptor and/or erbB2 expressing adenoid cystic carcinoma and non adenoid cystic carcinoma malignant tumors of the salivary glands. J. Clin. Oncol. 2007, 25, 3978–3984. [Google Scholar] [CrossRef]
- Perissinotti, A.J.; Lee Pierce, M.; Pace, M.B.; El-Naggar, A.; Kies, M.S.; Kupferman, M. The role of trastuzumab in the management of salivary ductal carcinomas. Anticancer Res. 2013, 33, 2587–2591. [Google Scholar]
- Lee, J.S.; Kwon, O.J.; Park, J.J.; Seo, J.H. Salivary duct carcinoma of the parotid gland: Is adjuvant HER-2-targeted therapy required? J. Oral Maxillofac. Surg. 2014, 72, 1023–1031. [Google Scholar] [CrossRef]
- Takahashi, H.; Tada, Y.; Saotome, T.; Akazawa, K.; Ojiri, H.; Fushimi, C.; Masubuchi, T.; Matsuki, T.; Tani, K.; Osamura, R.Y.; et al. Phase II Trial of Trastuzumab and Docetaxel in Patients with Human Epidermal Growth Factor Receptor 2-Positive Salivary Duct Carcinoma. J. Clin. Oncol. 2019, 37, 125–134. [Google Scholar] [CrossRef]
- Press, M.F.; Pike, M.C.; Hung, G.; Zhou, J.Y.; Ma, Y.; George, J.; Dietz-Band, J.; James, W.; Slamon, D.J.; Batsakis, J.G.; et al. Amplification and overexpression of HER-2/neu in carcinomas of the salivary gland: Correlation with poor prognosis. Cancer Res. 1994, 54, 5675–5682. [Google Scholar]
- Skalova, A.; Starek, K.V.; Szepe, P.; Plank, L. Salivary duct carcinoma-a highly aggressive salivary gland tumour with HER-2/neuoncoprotein overexpression. Pathol. Res. Pract. 2001, 197, 621–626. [Google Scholar] [CrossRef]
- Skalova, A.; Starek, I.; Vanecek, T.; Kucerova, V.; Plank, L.; Szepe, P.; Di Palma, S.; Leivo, I. Expression of HER-2/neu gene and protein in salivary duct carcinomas of parotid gland as revealed by fluorescence in-situ hybridization and immunohistochemistry. Histopathology 2003, 42, 348–356. [Google Scholar] [CrossRef]
- Etges, A.; Pinto, D.S., Jr.; Kowalski, L.P.; Soares, F.A.; Araujo, V.C. Salivary duct carcinoma: Immunohistochemical profile of an aggressive salivary gland tumour. J. Clin. Pathol. 2003, 56, 914–918. [Google Scholar] [CrossRef]
- Jaehne, M.; Roeser, K.; Jaekel, T.; Schepers, J.D.; Albert, N.; Loning, T. Clinical and immunohistologic typing of salivary duct carcinoma: A report of 50 cases. Cancer 2005, 103, 2526–2533. [Google Scholar] [CrossRef]
- Cornolti, G.; Ungari, M.; Morassi, M.L.; Facchetti, F.; Rossi, E.; Lombardi, D.; Nicolai, P. Amplification and overexpression of HER2/neu gene and HER2/neu protein in salivary duct carcinoma of the parotid gland. Arch. Otolaryngol. Head Neck Surg. 2007, 133, 1031–1036. [Google Scholar] [CrossRef]
- Johnson, C.J.; Barry, M.B.; Vasef, M.A.; Deyoung, B.R. Her-2/neu expression in salivary duct carcinoma: An immunohistochemical and chromogenic in situ hybridization study. Appl. Immunohistochem. Mol. Morphol. 2008, 16, 54–58. [Google Scholar] [CrossRef]
- Santana, T.; Pavel, A.; Martinek, P.; Steiner, P.; Grossmann, P.; Baněčková, M.; Skálová, A. Biomarker immunoprofile and molecular characteristics in salivary duct carcinoma: Clinicopathological and prognostic implications. Hum. Pathol. 2019, 93, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.D.; Roberts, D.B.; Kies, M.S.; Mao, L.; Weber, R.S.; El-Naggar, A.K. Genetic and expression analysis of HER-2 and EGFR genes in salivary duct carcinoma: Empirical and therapeutic significance. Clin. Cancer Res. 2010, 16, 2266–2274. [Google Scholar] [CrossRef] [PubMed]
- Clauditz, T.S.; Reiff, M.; Gravert, L.; Gnoss, A.; Tsourlakis, M.C.; Münscher, A.; Sauter, G.; Bokemeyer, C.; Knecht, R.; Wilczak, W. Human epidermal growth factor receptor 2 (HER2) in salivary gland carcinomas. Pathology 2011, 43, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Nardi, V.; Sadow, P.M.; Juric, D.; Zhao, D.; Cosper, A.K.; Bergethon, K.; Scialabba, V.L.; Batten, J.M.; Borger, D.R.; Iafrate, A.J.; et al. Detection of novel actionable genetic changes in salivary duct carcinoma helps direct patient treatment. Clin. Cancer Res. 2013, 19, 480–490. [Google Scholar] [CrossRef]
- Xia, L.; Hu, Y.; Li, J.; Gu, T.; Zhang, C.; Wang, L.; Tian, Z. A low percentage of HER-2 amplification whereas indicates poor prognosis in salivary carcinoma ex pleomorphic adenoma: A study of 140 cases. J. Oral Pathol. Med. 2017, 46, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Tsiambas, E.; Karameris, A.; Dervenis, C.; Lazaris, A.C.; Giannakou, N.; Gerontopoulos, K.; Patsouris, E. HER2/neu expression and gene alterations in pancreatic ductal adenocarcinoma: A comparative immunohistochemistry and chromogenic in situ hybridization study based on tissue microarrays and computerized image analysis. JOP 2006, 7, 283–294. [Google Scholar]
- Chou, A.; Waddell, N.; Cowley, M.J.; Gill, A.J.; Chang, D.K.; Patch, A.-M.; Nones, K.; Wu, J.; Pinese, M.; Johns, A.L.; et al. Clinical and molecular characterization of HER2 amplified-pancreatic cancer. Genome Med. 2013, 5, 78. [Google Scholar] [CrossRef]
- Safran, H.; Iannitti, D.; Ramanathan, R.; Schwartz, J.D.; Steinhoff, M.; Nauman, C.; Hesketh, P.; Rathore, R.; Wolff, R.; Tantravahi, U.; et al. Herceptin and gemcitabine for metastatic pancreatic cancers that overexpress HER-2/neu. Cancer Investig. 2004, 22, 706–712. [Google Scholar] [CrossRef]
- Assenat, E.; Azria, D.; Mollevi, C.; Guimbaud, R.; Tubiana-Mathieu, N.; Smith, D.; Delord, J.P.; Samalin, E.; Portales, F.; Larbouret, C.; et al. Dual targeting of HER1/EGFR and HER2 with cetuximab and trastuzumab in patients with metastatic pancreatic cancer after gemcitabine failure: Results of the “THERAPY”phase 1-2 trial. Oncotarget 2015, 6, 12796–12808. [Google Scholar] [CrossRef]
- Lei, S.; Appert, H.E.; Nakata, B.; Domenico, D.R.; Kim, K.; Howard, J.M. Overexpression of HER2/neu oncogene in pancreatic cancer correlates with shortened survival. Int. J. Pancreatol. 1995, 17, 15–21. [Google Scholar] [CrossRef]
- Day, J.D.; Digiuseppe, J.A.; Yeo, C.; Lai-Goldman, M.; Anderson, S.M.; Goodman, S.N.; Kern, S.E.; Hruban, R.H. Immunohistochemical evaluation of HER-2/neu expression in pancreatic adenocarcinoma and pancreatic intraepithelial neoplasms. Hum. Pathol. 1996, 27, 119–124. [Google Scholar] [CrossRef]
- Dugan, M.C.; Dergham, S.T.; Kucway, R.; Singh, K.; Biernat, L.; Du, W.; Vaitkevicius, V.K.; Crissman, J.D.; Sarkar, F.H. HER-2/neu expression in pancreatic adenocarcinoma: Relation to tumor differentiation and survival. Pancreas 1997, 14, 229–236. [Google Scholar] [CrossRef]
- Safran, H.; Steinhoff, M.; Mangray, S.; Rathore, R.; King, T.C.; Chai, L.; Berzein, K.; Moore, T.; Iannitti, D.; Reiss, P.; et al. Overexpression of the HER-2/neu oncogene in pancreatic adenocarcinoma. Am. J. Clin. Oncol. 2001, 24, 496–499, Erratum in Am. J. Clin. Oncol. 2002, 25, 181. [Google Scholar] [CrossRef]
- Novotný, J.; Petruzelka, L.; Vedralová, J.; Kleibl, Z.; Matous, B.; Juda, L. Prognostic significance of c-erbB-2 gene expression in pancreatic cancer patients. Neoplasma 2001, 48, 188–191. [Google Scholar]
- Potti, A.; Ganti, A.K.; Tendulkar, K.; Chitajallu, S.; Sholes, K.; Koch, M.; Kargas, S. HER-2/neu and CD117 (C-kit) overexpression in hepatocellular and pancreatic carcinoma. Anticancer Res. 2003, 23, 2671–2674. [Google Scholar]
- Hermanová, M.; Lukás, Z.; Nenutil, R.; Brázdil, J.; Kroupová, I.; Kren, L.; Pazourková, M.; Růzicka, M.; Díte, P. Amplification and overexpression of HER-2/neu in invasive ductal carcinomas of the pancreas and pancreatic intraepithelial neoplasms and the relationship to the expression of p21(WAF1/CIP1). Neoplasma 2004, 51, 77–83. [Google Scholar]
- Tamiolakis, D.; Venizelos, I.; Simopoulos, C.; Kotini, A.; Jivannakis, T.; Papadopoulos, N. Correlation of immunohistochemically detected HER-2/neu (c-erbB-2) with histological stage and perineural invasion in pancreatic cancer. Hepatogastroenterology 2004, 51, 334–337. [Google Scholar]
- Stoecklein, N.H.; Luebke, A.M.; Erbersdobler, A.; Knoefel, W.T.; Schraut, W.; Verde, P.E.; Stern, F.; Scheunemann, P.; Peiper, M.; Eisenberger, C.F.; et al. Copy number of chromosome 17 but not HER2 amplification predicts clinical outcome of patients with pancreatic ductal adenocarcinoma. J. Clin. Oncol. 2004, 22, 4737–4745. [Google Scholar] [CrossRef]
- Sharif, S.; Ramanathan, R.K.; Potter, D.; Cieply, K.; Krasinskas, A.M. HER2 gene amplification and chromosome 17 copy number do not predict survival of patients with resected pancreatic adenocarcinoma. Dig. Dis. Sci. 2008, 53, 3026–3032. [Google Scholar] [CrossRef]
- Komoto, M.; Nakata, B.; Amano, R.; Yamada, N.; Yashiro, M.; Ohira, M.; Wakasa, K.; Hirakawa, K. HER2 overexpression correlates with survival after curative resection of pancreatic cancer. Cancer Sci. 2009, 100, 1243–1247. [Google Scholar] [CrossRef]
- Harder, J.; Ihorst, G.; Heinemann, V.; Hofheinz, R.; Moehler, M.; Buechler, P.; Kloeppel, G.; Röcken, C.; Bitzer, M.; Boeck, S.; et al. Multicentre phase II trial of trastuzumab and capecitabine in patients with HER2 overexpressing metastatic pancreatic cancer. Br. J. Cancer 2012, 106, 1033–1038. [Google Scholar] [CrossRef] [PubMed]
- Assenat, E.; Mineur, L.; Mollevi, C.; Lopez-Crapez, E.; Lombard-Bohas, C.; Samalin, E.; Portales, F.; Walter, T.; Forges, H.; Dupuy, M.; et al. Phase II study evaluating the association of gemcitabine, trastuzumab and erlotinib as first-line treatment in patients with metastatic pancreatic adenocarcinoma (GATE 1). Int. J. Cancer 2021, 148, 682–691. [Google Scholar] [CrossRef] [PubMed]
- Gan, K.; Gao, Y.; Liu, K.; Xu, B.; Qin, W. The Clinical Significance and Prognostic Value of HER2 Expression in Bladder Cancer: A Meta-Analysis and a Bioinformatic Analysis. Front. Oncol. 2021, 11, 653491. [Google Scholar] [CrossRef]
- Hussain, M.H.; MacVicar, G.R.; Petrylak, D.P.; Dunn, R.L.; Vaishampayan, U.; Lara, P.N., Jr.; Chatta, G.S.; Nanus, D.M.; Glode, L.M.; Trump, D.L.; et al. Trastuzumab, paclitaxel, carboplatin, and gemcitabine in advanced human epidermal growth factor receptor-2/neu-positive urothelial carcinoma: Results of a multicenter phase II National Cancer Institute trial. J. Clin. Oncol. 2007, 25, 2218–2224, Erratum in J. Clin. Oncol. 2008, 26, 3295. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Huddart, R.A.; Elliott, T.; Sarker, S.J.; Ackerman, C.; Jones, R.; Hussain, S.; Crabb, S.; Jagdev, S.; Chester, J.; et al. Phase III, Double-Blind, Randomized Trial that Compared Maintenance Lapatinib Versus Placebo after First-Line Chemotherapy in Patients with Human Epidermal Growth Factor Receptor 1/2-Positive Metastatic Bladder Cancer. J. Clin. Oncol. 2017, 35, 48–55. [Google Scholar] [CrossRef]
- Sheng, X.; Yan, X.; Wang, L.; Shi, Y.; Yao, X.; Luo, H.; Shi, B.; Liu, J.; He, Z.; Yu, G.; et al. Open-label, Multicenter, Phase II Study of RC48-ADC, a HER2-Targeting Antibody-Drug Conjugate, in Patients with Locally Advanced or Metastatic Urothelial Carcinoma. Clin. Cancer Res. 2021, 27, 43–51. [Google Scholar] [CrossRef]
- Nishio, Y.; Yamada, Y.; Kokubo, H.; Nakamura, K.; Aoki, S.; Taki, T.; Honda, N.; Nakagawa, A.; Saga, S.; Hara, K. Prognostic significance of immunohistochemical expression of the Her-2/neu oncoprotein in bone metastatic prostate cancer. Urology 2006, 68, 110–115. [Google Scholar] [CrossRef]
- Morote, J.; de Torres, I.; Caceres, C.; Vallejo, C.; Schwartz, S., Jr.; Reventos, J. Prognostic value of immunohistochemical expression of the c-erbB-2 oncoprotein in metastatic prostate cancer. Int. J. Cancer 1999, 84, 421–425. [Google Scholar] [CrossRef]
- Neto, A.S.; Tobias-Machado, M.; Wroclawski, M.L.; Fonseca, F.L.; Teixeira, G.K.; Amarante, R.D.; Wroclawski, E.R.; Del Giglio, A. Her-2/neu expression in prostate adenocarcinoma: A systematic review and meta-analysis. J. Urol. 2010, 184, 842–850. [Google Scholar] [CrossRef]
- Ziada, A.; Barqawi, A.; Glode, L.M.; Varella-Garcia, M.; Crighton, F.; Majeski, S.; Rosenblum, M.; Kane, M.; Chen, L.; Crawford, E.D. The use of trastuzumab in the treatment of hormone refractory prostate cancer; phase II trial. Prostate 2004, 60, 332–337. [Google Scholar] [CrossRef]
- Lara, P.N., Jr.; Chee, K.G.; Longmate, J.; Ruel, C.; Meyers, F.J.; Gray, C.R.; Edwards, R.G.; Gumerlock, P.H.; Twardowski, P.; Doroshow, J.H.; et al. Trastuzumab plus docetaxel in HER-2/neu-positive prostate carcinoma: Final results from the California Cancer Consortium Screening and Phase II Trial. Cancer 2004, 100, 2125–2131. [Google Scholar] [CrossRef]
- Curigliano, G.; De Braud, F.; Teresa Sandri, M.; Renne, G.; Zorzino, L.; Scardino, E.; Rocco, B.; Spitaleri, G.; De Pas, T.; Noberasco, C.; et al. Gefitinib combined with endocrine manipulation in patients with hormone-refractory prostate cancer: Quality of life and surrogate markers of activity. Anticancer Drugs 2007, 18, 949–954. [Google Scholar] [CrossRef]
- de Bono, J.S.; Bellmunt, J.; Attard, G.; Droz, J.P.; Miller, K.; Flechon, A.; Sternberg, C.; Parker, C.; Zugmaier, G.; Hersberger-Gimenez, V.; et al. Open-label phase II study evaluating the efficacy and safety of two doses of pertuzumab in castrate chemotherapy-naive patients with hormone-refractory prostate cancer. J. Clin. Oncol. 2007, 25, 257–262. [Google Scholar] [CrossRef]
- Agus, D.B.; Sweeney, C.J.; Morris, M.J.; Mendelson, D.S.; McNeel, D.G.; Ahmann, F.R.; Wang, J.; Derynck, M.K.; Ng, K.; Lyons, B.; et al. Efficacy and safety of single-agent pertuzumab (rhuMAb 2C4), a human epidermal growth factor receptor dimerization inhibitor, in castration-resistant prostate cancer after progression from taxane-based therapy. J. Clin. Oncol. 2007, 25, 675–681. [Google Scholar] [CrossRef]
- Vuky, J.; Porter, C.; Isacson, C.; Vaughan, M.; Kozlowski, P.; Picozzi, V.; Corman, J. Phase II trial of neoadjuvant docetaxel and gefitinib followed by radical prostatectomy in patients with high-risk, locally advanced prostate cancer. Cancer 2009, 115, 784–791. [Google Scholar] [CrossRef]
- Whang, Y.E.; Armstrong, A.J.; Rathmell, W.K.; Godley, P.A.; Kim, W.Y.; Pruthi, R.S.; Wallen, E.M.; Crane, J.M.; Moore, D.T.; Grigson, G.; et al. A phase II study of lapatinib, a dual EGFR and HER-2 tyrosine kinase inhibitor, in patients with castration-resistant prostate cancer. Urol. Oncol. 2013, 31, 82–86. [Google Scholar] [CrossRef]
- Roa, I.; de Toro, G.; Schalper, K.; de Aretxabala, X.; Churi, C.; Javle, M. Overexpression of the HER2/neu gene: A new therapeutic possibility for patients with advanced gallbladder cancer. Gastrointest. Cancer Res. 2014, 7, 42–48. [Google Scholar]
- Kawamoto, T.; Krishnamurthy, S.; Tarco, E.; Trivedi, S.; Wistuba, I.I.; Li, D.; Roa, I.; Roa, J.C.; Thomas, M.B. HER receptor family: Novel candidate for targeted therapy for gallbladder and extrahepatic bile duct cancer. Gastrointest. Cancer Res. 2007, 1, 221–227. [Google Scholar]
- Toledo, C.; Matus, C.E.; Barraza, X.; Arroyo, P.; Ehrenfeld, P.; Figueroa, C.D.; Bhoola, K.D.; Del Pozo, M.; Poblete, M.T. Expression of HER2 and bradykinin B(1) receptors in precursor lesions of gallbladder carcinoma. World J. Gastroenterol. 2012, 18, 1208–1215. [Google Scholar] [CrossRef]
- Harder, J.; Waiz, O.; Otto, F.; Geissler, M.; Olschewski, M.; Weinhold, B.; Blum, H.E.; Schmitt-Graeff, A.; Opitz, O.G. EGFR and HER2 expression in advanced biliary tract cancer. World J. Gastroenterol. 2009, 15, 4511–4517. [Google Scholar] [CrossRef]
- Albrecht, T.; Rausch, M.; Roessler, S.; Geissler, V.; Albrecht, M.; Halske, C.; Seifert, C.; Renner, M.; Singer, S.; Mehrabi, A.; et al. HER2 gene (ERBB2) amplification is a low-frequency driver with potential predictive value in gallbladder carcinoma. Virchows Arch. 2020, 476, 871–880. [Google Scholar] [CrossRef] [PubMed]
- Javle, M.; Churi, C.; Kang, H.C.; Shroff, R.; Janku, F.; Surapaneni, R.; Zuo, M.; Barrera, C.; Alshamsi, H.; Krishnan, S.; et al. HER2/neu-directed therapy for biliary tract cancer. J. Hematol. Oncol. 2015, 8, 58. [Google Scholar] [CrossRef] [PubMed]
- Pignochino, Y.; Sarotto, I.; Peraldo-Neia, C.; Penachioni, J.Y.; Cavalloni, G.; Migliardi, G.; Casorzo, L.; Chiorino, G.; Risio, M.; Bardelli, A.; et al. Targeting EGFR/HER2 pathways enhances the antiproliferative effect of gemcitabine in biliary tract and gallbladder carcinomas. BMC Cancer 2010, 10, 631. [Google Scholar] [CrossRef] [PubMed]
- Gorlick, R.; Huvos, A.G.; Heller, G.; Aledo, A.; Beardsley, G.P.; Healey, J.H.; Meyers, P.A. Expression of HER2/erbB-2 correlates with survival in osteosarcoma. J. Clin. Oncol. 1999, 17, 2781–2788. [Google Scholar] [CrossRef] [PubMed]
- Onda, M.; Matsuda, S.; Higaki, S.; Iijima, T.; Fukushima, J.; Yokokura, A.; Kojima, T.; Horiuchi, H.; Kurokawa, T.; Yamamoto, T. ErbB-2 expression is correlated with poor prognosis for patients with osteosarcoma. Cancer 1996, 77, 71–78. [Google Scholar] [CrossRef]
- Akatsuka, T.; Wada, T.; Kokai, Y.; Sawada, N.; Yamawaki, S.; Ishii, S. Loss of ErbB2 expression in pulmonary metastatic lesions in osteosarcoma. Oncology 2001, 60, 361–366. [Google Scholar] [CrossRef]
- Thomas, D.G.; Giordano, T.J.; Sanders, D.; Biermann, J.S.; Baker, L. Absence of HER2/neu gene expression in osteosarcoma and skeletal Ewing’s sarcoma. Clin. Cancer Res. 2002, 8, 788–793. [Google Scholar]
- Anninga, J.K.; van de Vijver, M.J.; Cleton-Jansen, A.M.; Kristel, P.M.; Taminiau, A.H.; Nooij, M.; Egeler, R.M.; Hogendoorn, P.C. Overexpression of the HER-2 oncogene does not play a role in high-grade osteosarcomas. Eur. J. Cancer 2004, 40, 963–970. [Google Scholar] [CrossRef]
- Kremser, R.; Obrist, P.; Spizzo, G.; Erler, H.; Kendler, D.; Kemmler, G.; Mikuz, G.; Ensinger, C. Her2/neu overexpression in differentiated thyroid carcinomas predicts metastatic disease. Virchows Arch. 2003, 442, 322–328. [Google Scholar] [CrossRef]
- Ruggeri, R.M.; Campennì, A.; Giuffrè, G.; Giovanella, L.; Siracusa, M.; Simone, A.; Branca, G.; Scarfì, R.; Trimarchi, F.; Ieni, A.; et al. HER2 Analysis in Sporadic Thyroid Cancer of Follicular Cell Origin. Int. J. Mol. Sci. 2016, 17, 2040. [Google Scholar] [CrossRef]
- Haugen, D.R.; Akslen, L.A.; Varhaug, J.E.; Lillehaug, J.R. Expression of c-erbB-2 protein in papillary thyroid carcinomas. Br. J. Cancer 1992, 65, 832–837. [Google Scholar] [CrossRef]
- Ensinger, C.; Prommegger, R.; Kendler, D.; Gabriel, M.; Spizzo, G.; Mikuz, G.; Kremser, R. Her2/neu expression in poorly-differentiated and anaplastic thyroid carcinomas. Anticancer Res. 2003, 23, 2349–2353. [Google Scholar]
- Ensinger, C.; Prommegger, R.; Kendler, D.; Gabriel, M.; Spizzo, G.; Mikuz, G.; Kremser, R. Her2/neu expression in C-cell hyperplasia and medullary thyroid carcinomas. Anticancer Res. 2003, 23, 2241–2243. [Google Scholar]
- Koka, V.; Potti, A.; Forseen, S.E.; Pervez, H.; Fraiman, G.N.; Koch, M.; Levitt, R. Role of Her-2/neu overexpression and clinical determinants of early mortality in glioblastoma multiforme. Am. J. Clin. Oncol. 2003, 26, 332–335. [Google Scholar] [CrossRef]
- Forseen, S.E.; Potti, A.; Koka, V.; Koch, M.; Fraiman, G.; Levitt, R. Identification and relationship of HER-2/neu overexpression to short-term mortality in primary malignant brain tumors. Anticancer Res. 2002, 22, 1599–1602. [Google Scholar]
- Mineo, J.F.; Bordron, A.; Quintin-Roué, I.; Loisel, S.; Ster, K.L.; Buhé, V.; Lagarde, N.; Berthou, C. Recombinant humanised anti-HER2/neu antibody (Herceptin) induces cellular death of glioblastomas. Br. J. Cancer 2004, 91, 1195–1199. [Google Scholar] [CrossRef]
- Buhring, H.J.; Sures, I.; Jallal, B.; Weiss, F.U.; Busch, F.W.; Ludwig, W.D.; Handgretinger, R.; Waller, H.D.; Ullrich, A. The receptor tyrosine kinase p185HER2 is expressed on a subset of B-lymphoid blasts from patients with acute lymphoblastic leukemia and chronic myelogenous leukemia. Blood 1995, 86, 1916–1923. [Google Scholar] [CrossRef]
- Chevallier, P.; Robillard, N.; Wuilleme-Toumi, S.; Mechinaud, F.; Harousseau, J.L.; Avet-Loiseau, H. Overexpression of Her2/neu is observed in one third of adult acute lymphoblastic leukemia patients and is associated with chemoresistance in these patients. Haematologica 2004, 89, 1399–1401. [Google Scholar]
- Muller, M.R.; Grunebach, F.; Kayser, K.; Vogel, W.; Nencioni, A.; Brugger, W.; Kanz, L.; Brossart, P. Expression of her-2/neu on acute lymphoblastic leukemias: Implications for the development of immunotherapeutic approaches. Clin. Cancer Res. 2003, 9, 3448–3453. [Google Scholar]
- Haen, S.P.; Schmiedel, B.J.; Rothfelder, K.; Schmied, B.J.; Dang, T.M.; Mirza, N.; Möhle, R.; Kanz, L.; Vogel, W.; Salih, H.R. Prognostic relevance of HER2/neu in acute lymphoblastic leukemia and induction of NK cell reactivity against primary ALL blasts by trastuzumab. Oncotarget 2016, 7, 13013–13030. [Google Scholar] [CrossRef]
- Chevallier, P.; Robillard, N.; Charbonnier, A.; Raffoux, E.; Maury, S.; Carras, S.; Chabrot, C.; Fohrer, C.; Bernard, M.; Blade, J.S.; et al. Trastuzumab for treatment of refractory/relapsed HER2-positive adult B-ALL: Results of a phase 2 GRAALL study. Blood 2012, 119, 2474–2477. [Google Scholar] [CrossRef] [PubMed]
- Nuciforo, P.G.; Pellegrini, C.; Fasani, R.; Maggioni, M.; Coggi, G.; Parafioriti, A.; Bosari, S. Molecular and immunohistochemical analysis of HER2/neu oncogene in synovial sarcoma. Hum. Pathol. 2003, 34, 639–645. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.; Peiper, M.; Heinecke, A.; Zurakowski, D.; Eisenberger, C.F.; Hosch, S.; Knoefel, W.T.; Izbicki, J.R. Expression of HER2/neu does not correlate with survival in soft tissue sarcoma. Onkologie 2003, 26, 268–271. [Google Scholar] [CrossRef] [PubMed]
- Babashahi, M.; Mehrazma, M.; Nasiri, S.J.; Azizi Jalilian, F.; Rezaei-Tavirani, M. Her2/neu Expression in Wilms’ Tumor and Correlation with Histopathologic Findings. Iran J. Cancer Prev. 2013, 6, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Ragab, S.M.; Samaka, R.M.; Shams, T.M. HER2/neu expression: A predictor for differentiation and survival in children with Wilms tumor. Pathol. Oncol. Res. 2010, 16, 61–67. [Google Scholar] [CrossRef]
- Kluger, H.M.; DiVito, K.; Berger, A.J.; Halaban, R.; Ariyan, S.; Camp, R.L.; Rimm, D.L. Her2/neu is not a commonly expressed therapeutic target in melanoma—A large cohort tissue microarray study. Melanoma Res. 2004, 14, 207–210. [Google Scholar] [CrossRef]
- Tarantino, P.; Morganti, S.; Curigliano, G. Targeting HER2 in breast cancer: New drugs and paradigms on the horizon. Explor. Target. Antitumor Ther. 2021, 2, 139–155. [Google Scholar] [CrossRef]
- Fong, C.; Chau, I. HER2 Inhibition in Gastric Cancer-Novel Therapeutic Approaches for an Established Target. Cancers 2022, 14, 3824. [Google Scholar] [CrossRef]
- Grieb, B.C.; Agarwal, R. HER2-Directed Therapy in Advanced Gastric and Gastroesophageal Adenocarcinoma: Triumphs and Troubles. Curr. Treat. Options Oncol. 2021, 22, 88. [Google Scholar] [CrossRef]
- Fader, A.N.; Roque, D.M.; Siegel, E.; Buza, N.; Hui, P.; Abdelghany, O.; Chambers, S.K.; Secord, A.A.; Havrilesky, L.; O’Malley, D.M.; et al. Randomized Phase II Trial of Carboplatin-Paclitaxel Versus Carboplatin-Paclitaxel-Trastuzumab in Uterine Serous Carcinomas That Overexpress Human Epidermal Growth Factor Receptor 2/neu. J. Clin. Oncol. 2018, 36, 2044–2051. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).