
Pre-Treatment C-Reactive Protein Predicts Survival in Small Cell Lung Cancer Patients

 , and
, and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
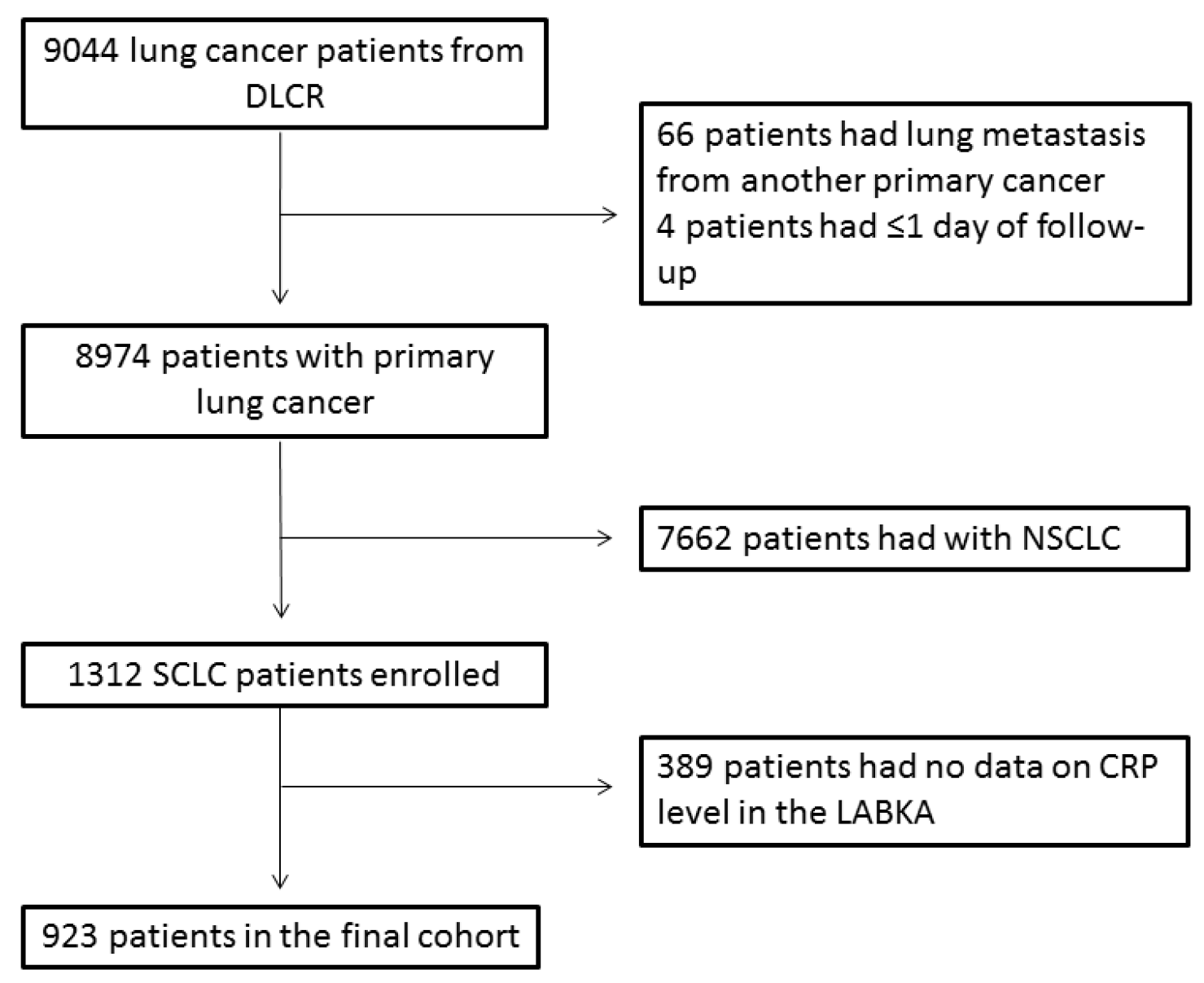
2.1. Patients
2.2. CRP Measurement
2.3. Ethics
2.4. Statistical Analysis
3. Results
3.1. Patients
3.2. Patient Characteristics
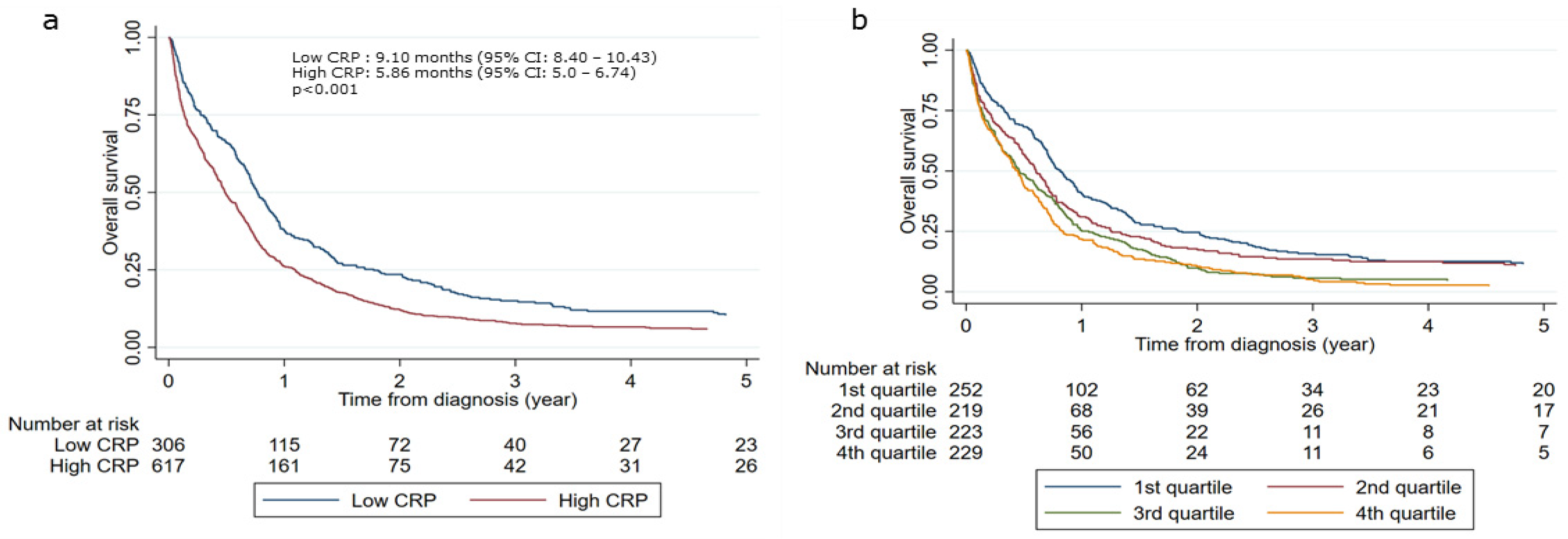
3.3. Survival Outcome and Level of CRP
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Aggarwal, B.B.; Shishodia, S.; Sandur, S.K.; Pandey, M.K.; Sethi, G. Inflammation and cancer: How hot is the link? Biochem. Pharmacol. 2006, 72, 1605–1621. [Google Scholar] [CrossRef]
- Coussens, L.M.; Werb, Z. Inflammation and cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef]
- Jing, X.; Huang, C.; Zhou, H.; Li, C.; Fan, L.; Chen, J.; Zhang, G.; Liu, Y.; Cui, Z.; Qi, D.; et al. Association between serum C-reactive protein value and prognosis of patients with non-small cell lung cancer: A meta-analysis. Int. J. Clin. Exp. Med. 2015, 8, 10633–10639. [Google Scholar] [PubMed]
- Sproston, N.R.; Ashworth, J.J. Role of C-Reactive Protein at Sites of Inflammation and Infection. Front. Immunol. 2018, 9, 754. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M.; Saito, H.; Hara, K.; Sugezawa, K.; Uejima, C.; Tanio, A.; Tada, Y.; Kihara, K.; Sakamoto, T.; Honjo, S.; et al. Combination of C-reactive protein and monocyte count is a useful prognostic indicator for patients with colorectal cancer. Vivo 2019, 34, 299–305. [Google Scholar] [CrossRef]
- Woo, H.D.; Kim, K.; Kim, J. Association between preoperative C-reactive protein level and colorectal cancer survival: A meta-analysis. Cancer Causes Control 2015, 26, 1661–1670. [Google Scholar] [CrossRef]
- Szkandera, J.; Stotz, M.; Absenger, G.; Stojakovic, T.; Samonigg, H.; Kornprat, P.; Schaberl-Moser, R.; Alzoughbi, W.; Lackner, C.; Ress, A.L.; et al. Validation of C-reactive protein levels as a prognostic indicator for survival in a large cohort of pancreatic cancer patients. Br. J. Cancer 2014, 110, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Nurmi, A.M.; Mustonen, H.K.; Stenman, U.-H.; Seppänen, H.E.; Haglund, C.H. Combining CRP and CA19-9 in a novel prognostic score in pancreatic ductal adenocarcinoma. Sci. Rep. 2021, 11, 1–11. [Google Scholar] [CrossRef]
- Mitsunaga, S.; Ikeda, M.; Shimizu, S.; Ohno, I.; Takahashi, H.; Okuyama, H.; Ueno, H.; Morizane, C.; Kondo, S.; Sakamoto, Y.; et al. C-Reactive Protein Level Is an Indicator of the Aggressiveness of Advanced Pancreatic Cancer. Pancreas 2016, 45, 110–116. [Google Scholar] [CrossRef]
- Yu, X.; Zhao, J.; Shi, L.; Jin, Y.; Sun, Y.; Shi, X. Prognostic value of circulating C-reactive protein levels in patients with non-small cell lung cancer: A systematic review with meta-analysis. J. Cancer Res. Ther. 2014, 10, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Leuzzi, G.; Galeone, C.; Gisabella, M.; Duranti, L.; Taverna, F.; Suatoni, P.; Morelli, D.; Pastorino, U. Baseline C-Reactive Protein Level Predicts Survival of Early-Stage Lung Cancer: Evidence from a Systematic Review and Meta-Analysis. Tumori J. 2016, 102, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.; Yu, Z.; Guo, W.; Liu, Q.; Wu, Y.; Li, Y.; Bai, L. Prognostic value of circulating inflammatory factors in non-small cell lung cancer: A systematic review and meta-analysis. Cancer Biomark. 2014, 14, 469–481. [Google Scholar] [CrossRef]
- Zeng, Q.; Xue, N.; Dai, D.; Xing, S.; He, X.; Li, S.; Du, Y.; Huang, C.; Li, L.; Liu, W. A nomogram based on inflammatory factors c-reactive protein and fibrinogen to predict the prognostic value in patients with resected non-small cell lung cancer. J. Cancer 2017, 8, 744–753. [Google Scholar] [CrossRef]
- Dirican, N.; Dirican, A.; Anar, C.; Atalay, S.; Ozturk, O.; Bircan, A.; Akkaya, A.; Cakir, M. A New inflammatory prognostic index, based on C-reactive protein, the neutrophil to lymphocyte ratio and serum albumin is useful for predicting prognosis in non-small cell lung cancer cases. Asian Pac. J. Cancer Prev. 2016, 17, 5101–5106. [Google Scholar] [CrossRef] [PubMed]
- Baek, A.R.; Seo, H.J.; Lee, J.H.; Park, S.W.; Jang, A.S.; Paik, S.H.; Koh, E.S.; Shin, H.K.; Kim, D.J. Prognostic value of baseline carcinoembryonic antigen and cytokeratin 19 fragment levels in advanced non-small cell lung cancer. Cancer Biomark. 2018, 22, 55–62. [Google Scholar] [CrossRef]
- Koch, A.; Fohlin, H.; Sörenson, S. Prognostic Significance of C-reactive protein and smoking in patients with advanced non-small cell lung cancer treated with first-line palliative chemotherapy. J. Thorac. Oncol. 2009, 4, 326–332. [Google Scholar] [CrossRef]
- Bernhardt, D.; Aufderstrasse, S.; König, L.; Adeberg, S.; Bozorgmehr, F.; Christopoulos, P.; El Shafie, R.A.; Hörner-Rieber, J.; Kappes, J.; Thomas, M.; et al. Impact of inflammatory markers on survival in patients with limited disease small-cell lung cancer undergoing chemoradiotherapy. Cancer Manag. Res. 2018, 10, 6563–6569. [Google Scholar] [CrossRef]
- Hong, S.; Kang, Y.A.; Cho, B.C.; Kim, D.J. Elevated Serum C-reactive protein as a prognostic marker in small cell lung cancer. Yonsei Med. J. 2012, 53, 111–117. [Google Scholar] [CrossRef]
- Minami, S.; Ogata, Y.; Ihara, S.; Yamamoto, S.; Komuta, K. Pretreatment Glasgow prognostic score and prognostic nutritional index predict overall survival of patients with advanced small cell lung cancer. Lung Cancer Targets Ther. 2017, 8, 249–257. [Google Scholar] [CrossRef]
- Park, M.-R.; Park, Y.-H.; Choi, J.-W.; Park, D.-I.; Chung, C.-U.; Moon, J.-Y.; Park, H.-S.; Jung, S.-S.; Kim, J.-O.; Kim, S.-Y.; et al. Progression-free survival: An important prognostic marker for long-term survival of small cell lung cancer. Tuberc. Respir. Dis. 2014, 76, 218–225. [Google Scholar] [CrossRef][Green Version]
- Shao, N.; Cai, Q. High pretreatment serum C-reactive protein level predicts a poor prognosis for combined small-cell lung cancer. Tumor Biol. 2015, 36, 8465–8470. [Google Scholar] [CrossRef]
- Zhou, T.; Hong, S.; Wenhua, L.; Hou, X.; Huang, Y.; Zhao, H.; Liang, W.; Zhao, Y.; Fang, W.; Wu, X.; et al. A systemic inflammation-based prognostic scores (mGPS) predicts overall survival of patients with small-cell lung cancer. Tumor Biol. 2014, 36, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Sandfeld-Paulsen, B.; Aggerholm-Pedersen, N.; Winther-Larsen, A. Hyponatremia in lung cancer: Incidence and prognostic value in a Danish population-based cohort study. Lung Cancer 2021, 153, 42–48. [Google Scholar] [CrossRef]
- Jakobsen, E.; Rasmussen, T.R. The Danish Lung Cancer Registry. Clin. Epidemiol. 2016, 8, 537–541. [Google Scholar] [CrossRef]
- Patobank. 2021. Available online: https://www.patobank.dk/ (accessed on 1 July 2020).
- Grann, A.F.; Erichsen, R.; Nielsen, A.G.; Frøslev, T.; Thomsen, R.W. Existing data sources for clinical epidemiology: The clinical laboratory information system (LABKA) research database at Aarhus University, Denmark. Clin. Epidemiol. 2011, 3, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Pedersen, L.; Sørensen, H.T. The Danish civil registration system as a tool in epidemiology. Eur. J. Epidemiol. 2014, 29, 541–549. [Google Scholar] [CrossRef]
- Greenland, S.; Pearl, J.; Robins, J.M. Causal diagrams for epidemiologic research. Epidemiology 1999, 10, 37–48. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| CRP Normal * | CRP Elevated * | p-Value a | |
|---|---|---|---|
| Total | 306 (33%) | 617 (67%) | |
| Age, median years (95% percentiles) | 68 (52–82) | 70 (53–84) | 0.033 |
| Sex | |||
| Female | 177 → (57%) | 288 → (47%) | 0.002 |
| Male | 129 → (43%) | 329 → (53%) | |
| Stage | |||
| I | 26 → (8%) | 21 → (3%) | 0.001 |
| II | 12 → (4%) | 8 → (1%) | |
| III | 73 → (24%) | 152 → (25%) | |
| IV | 173 → (57%) | 375 → (61%) | |
| Unknown | 22 → (7%) | 61 → (10%) | |
| Performance status, ECOG | |||
| 0 | 85 → (28%) | 128 → (21%) | 0.003 |
| 1 | 103 → (34%) | 188 → (30%) | |
| 2 | 46 → (15%) | 103 → (17%) | |
| 3 | 39 → (13%) | 132 → (21%) | |
| Unknown | 33 → (11%) | 66 → (11%) | |
| Smoking | |||
| Never | 1 → (0%) | 6 → (1%) | 0.287 |
| Former or current | 272 → (89%) | 545 → (88%) | |
| Unknown | 33 → (11%) | 66 → (11%) | |
| Median CRP (95% percentiles) | 3 mg/L (1–7) or 23 nmol/L (7–75) | 40 mg/L (9–254) or 391 (88–2375) nmol/L |
| HR (95% CI) | Adjusted HR b (95% CI) | |
|---|---|---|
| CRP level | ||
| Normal | 1.00 | 1.00 |
| Elevated | 1.42 (1.23–1.64) | 1.25 (1.08–1.46) |
| CRP level a | ||
| 1st quartile | 1.00 | 1.00 |
| 2nd quartile | 1.22 (1.01–1.48) | 1.06 (0.86–1.31) |
| 3rd quartile | 1.58 (1.31–1.90) | 1.26 (1.03–1.55) |
| 4th quartile | 1.75 (1.45–2.11) | 1.44 (1.17–1.77) |
| Stage | ||
| I | 1.00 | |
| II | 1.16 (0.57–2.34) | |
| III | 3.52 (2.28–5.21) | |
| IV | 7.15 (4.69–10.58) | |
| Age, continuous variable | 1.03 (1.03–1.04) | |
| Sex | ||
| Female | 1.00 | |
| Male | 1.17 (1.02–1.34) | |
| Performance status, ECOG | ||
| 0 | 1.00 | |
| 1 | 1.47 (1.22–1.77) | |
| 2 | 2.86 (2.13–3.57) | |
| 3 + 4 | 4.54 (3.67–5.63) |
| Model | AIC | C-Index |
|---|---|---|
| (1) Stage + age + sex + PS | 8219 | 0.7322 |
| (2) CRP + stage + age + sex + PS | 8210 | 0.7355 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stensvold, A.M.; Aggerholm-Pedersen, N.; Winther-Larsen, A.; Sandfeld-Paulsen, B. Pre-Treatment C-Reactive Protein Predicts Survival in Small Cell Lung Cancer Patients. Onco 2021, 1, 114-122. https://doi.org/10.3390/onco1020010
Stensvold AM, Aggerholm-Pedersen N, Winther-Larsen A, Sandfeld-Paulsen B. Pre-Treatment C-Reactive Protein Predicts Survival in Small Cell Lung Cancer Patients. Onco. 2021; 1(2):114-122. https://doi.org/10.3390/onco1020010
Chicago/Turabian StyleStensvold, Anne Marie, Ninna Aggerholm-Pedersen, Anne Winther-Larsen, and Birgitte Sandfeld-Paulsen. 2021. "Pre-Treatment C-Reactive Protein Predicts Survival in Small Cell Lung Cancer Patients" Onco 1, no. 2: 114-122. https://doi.org/10.3390/onco1020010
APA StyleStensvold, A. M., Aggerholm-Pedersen, N., Winther-Larsen, A., & Sandfeld-Paulsen, B. (2021). Pre-Treatment C-Reactive Protein Predicts Survival in Small Cell Lung Cancer Patients. Onco, 1(2), 114-122. https://doi.org/10.3390/onco1020010