Abstract
Foundation Medicine® testing is a next-generation sequence (NGS)-based platform that allows clinicians to obtain the comprehensive genomic profiling (CGP) of several cancers. By using NGS approaches, relevant genomic alterations can be identified in a short timeframe, providing guidance to diagnostic and therapeutic decisions. This study reports the implementation of three commercially available Foundation Medicine® tests in a Portuguese institution and explores the genomic alterations identified. Data obtained from 72 patients tested with Foundation Medicine® between July 2017 and December 2020 were analysed retrospectively. A total of 290 gene alterations were identified, and TP53 was the gene most frequently altered. Among the 67 successfully profiled samples, 37.3% presented a potentially actionable variation. Breast carcinoma represented the most frequent tumour-carrying variation that can be targeted using currently approved drugs. A limited number of potentially actionable variants using approved drugs was found in this study; however, the genomic information provided by Foundation Medicine® may help clinicians in directing cancer patients into clinical trials or to off-label treatments.
1. Introduction
The evolution of precision medicine to specifically target genomic alterations expressed in different cancers highlights the importance of the efficient detection of actionable driver variations in cancer patients. Next-generation sequencing (NGS) is nowadays the gold standard for the sequencing of multiple genes that entail cancer predisposition [1]. When considering performing comprehensive genomic profiling (CGP), NGS can identify relevant genomic alterations and signatures in a short timeframe, and different studies have shown that, in selected cases, both patient response and survival may benefit from this approach [2,3]. When using a CGP, single-nucleotide variation (SNV), insertions or deletions (indels), copy number variations (CNVs) and gene rearrangements can be identified [4]. CGP assays also have the advantage of providing information on tumour mutational burden (TMB) and microsatellite instability (MSI), which represent biomarkers that can help guide clinicians on treatment decisions [4]. Although tumour tissue is commonly used in this analysis, this type of sample is not always available [5,6], and therefore the implementation of CGP using liquid biopsies gains relevance in a clinical context.
Foundation Medicine® (Cambridge, Massachusetts) testing is a comprehensive NGS-based testing platform developed and used to aid in the research, development, and identification of potential targeted therapies [7,8]. There are currently three tests available that allow for the CGP of all solid tumours, hematologic malignancies, and sarcomas [9,10,11]. FoundationOne CDx and FoundationOne Liquid CDx are FDA-approved companion diagnostic tests allowing for the identification of alterations occurring in 324 genes that are known to contribute to cancer through DNA sequencing, whilst FoundationOne Heme is a laboratory-developed test (LDT) designed for the study of 406 genes through DNA sequencing and 265 genes via RNA sequencing [9,10,11]. Different reports have shown that Foundation Medicine® testing, through CGP, can identify additional information on genomic alterations, beyond the actionable ones and that possible treatments may apply. Moreover, these comprehensive panels also contribute to the increased availability of clinical trials [2,12,13,14,15]. However, more comprehensive data are needed to fully understand the impact of performing these CGP tests while seeking to select effective therapeutic options.
The present study reports the implementation of FoundationOne CDx, FoundationOne Liquid CDx, and FoundationOne Heme services in a selected sample of Portuguese patients in different hospitals, with data centralised in one reference laboratory, and explores the identified genomic alterations.
2. Materials and Methods
2.1. Patients
This study involves a retrospective analysis of samples collected from 72 patients at 20 Portuguese institutions, which were analysed in a reference laboratory in Portugal. The present analysis reports data collected by the investigators between July 2017 and December 2020. This period corresponds to the implementation of Foundation Medicine® tests in Portugal. All patients provided written informed consent for the research use of their formalin-fixed, paraffin-embedded (FFPE) tissue and peripheral whole blood samples. After receiving a request from the clinician at IPATIMUP, we filled out a Test Requisition Form (TRF) on the FMI site. The samples were gathered in the following manner after receiving the analysis number (TRF number): the pathologist chose the FFPE samples with representative tumour tissue and sent them to the FMI. In the event that an FFPE sample was inconclusive, liquid biopsies were obtained by a nurse, transferred to the pathological department, and forwarded to the FMI.
2.2. Foundation Medicine® Testing
Foundation Medicine® tests are NGS-based CGP platforms that allow for the detection of somatic genomic alterations: SNVs, indels, CNVs, and rearrangements. For this study, the estimation of tumour cells was obtained through the ratio between the nuclei quantification of neoplastic cells vs. non-neoplastic cells, as previously described by Gullo I et al. [16]. NGS assays were carried out following the manufacturer’s instructions [9,10,11]. This analysis also allows for the determination of the TMB and MSI status. TMB was classified as high TMB (≥10 mutations/Mb) and low TMB (<10 mutations/Mb), and MSI was classified as stable, unstable, and “could not be determined”. To determine a patient’s MSI status, in Foundation Medicine® testing, a fractional-based (FB) MSI algorithm is employed to categorise a tumour specimen as MSI high (MSI-H) or microsatellite stable (MSS). The FB-MSI algorithm calculates the fraction of microsatellite loci determined to be altered or unstable (i.e., the fraction with unstable loci score) based on a genome-wide analysis across >2000 microsatellite loci. For a given microsatellite locus, non-somatic alleles are discarded, and the microsatellite is categorised as unstable if the remaining alleles differ from the reference genome. The final fraction unstable loci score is calculated as the number of unstable microsatellite loci divided by the number of evaluable microsatellite loci. Two FB-MSI score thresholds are applied to classify a tumour specimen as having the MSI-H or MSS status. The MSI-H status is reported for patients with solid tumours whose samples have FB-MSI scores ≥ 0.0124, while the MSS status is reported for patients with solid tumours whose samples have FB-MSI scores ≤ 0.0041. For patients with solid tumours whose samples have FB-MSI scores > 0.0041 and <0.0124, the MSI result is reported as “cannot be determined”. Turnaround time (TAT) is defined as the time from receiving the material to sending out the report.
2.3. Statistical Analysis
Descriptive statistics of continuous variables are presented with median, minimum, and maximum. Descriptive statistics of discrete variables are presented as numbers and percentages.
Spearman’s rho was calculated to determine the correlation between the number of altered genes and the TMB value.
3. Results
3.1. Patient Characteristics
A total of 72 samples from 72 patients were collected between July 2017 and December 2020. Table 1 presents a summary of the characteristics of the patients included in this study. In this study, 31 (43.1%) patients were male, and 41 (56.9%) were female. The median age of patients at the time of sample collection was 60.5 years (range 27–82). Forty-four (61.1%) of the patients were classified as having a stage IV tumour at the time of testing.

Table 1.
Characteristics of the patients evaluated with Foundation Medicine® tests.
From the 72 samples collected, 63 (87.5%) were evaluated using the FoundationOne® CDX test, 6 (8.3%) with the FoundationOne Liquid CDX test, and 3 (4.2%) with the FoundationOne Heme test. Within the 63 samples examined using the FoundationOne CDX test, 38 (60.3%) were derived from a primary tumour site, and 25 (39.7%) were derived from a metastatic site. Five of these FoundationOne CDX samples were excluded from the initial genomic analysis: four due to DNA degradation and one because did not contain a sufficient percentage of tumour cells to allow analysis.
3.2. Tumour Histology
Table 2 summarises the main histological types of tumours identified in the studied population. The most common tumour types were breast carcinoma (n = 14, 19.4%), cancer of unknown primary (n = 8, 11.1%), prostate adenocarcinoma (n = 8, 11.1%), and gastric adenocarcinoma (n = 8, 11.1%).
Table 2.
Summary of the main tumour types identified (tumour frequency ≥3).
3.3. Characteristics of Foundation Medicine® Testing
The median (min–max) turnaround time evaluated for all the samples analysed with the three Foundation Medicine® tests was 16 calendar (5–48) days and the median (min–max) percentage of tumour cells obtained for 66 samples was 40 (10–90). Of those, 3 samples (4.5%) presented with ≤10% of tumour cells, whilst 63 (95.5%) of the samples contained ≥20% of tumour cells. Table 3 presents the median turnaround time and percentage of tumour cells obtained for each of the Foundation Medicine® tests performed. Among the samples evaluated with FoundationOne CDX, 3 (4.8%) contained ≤10% of tumour cells, and 60 (95.2%) contained ≥20% of tumour cells. All three samples tested with FoundationOne Heme contained ≥20% of tumour cells.
Table 3.
Turnaround times and percentage of tumour cells obtained for each Foundation Medicine® tests performed.
3.4. Frequency of Genomic Alterations
Within the 72 samples studied, a total of 290 genomic alterations in 114 genes were found. The median number (min–max) of altered genes found per patient was four (0–15). The most commonly affected genes identified in the tested samples using Foundation Medicine® testing are summarised in Table 4.
Table 4.
Summary of the most frequently altered genes identified with Foundation Medicine®.
Testing with Foundation Medicine® also allowed for the evaluation of the median (min–max) TMB, which was 4 (0–33) in the 62 samples evaluated. Four (6.5%) patients presented a TMB ≥ 10 mutations/Mb, and 58 (93.5%) patients presented a TMB < 10 mutations/Mb. A positive correlation was found between the number of altered genes and TMB for the samples tested with FoundationOne CDX (r = 0.400; p = 0.001). Among the 67 patients assessed for MSI, 60 (89.6%) patients were found to be stable, while for 7 (10.4%), their status could not be determined.
Among the 67 profiled samples, 25 (37.3%) presented with potentially actionable genomic alterations with either FDA- and EMA-approved drugs (n = 9, 36.0%) or by experimental drug(s) in clinical trials (n = 16, 64.0%). Breast carcinoma (six samples, 24.0%), cancers of unknown primary (four samples, 16.0%), and prostate adenocarcinoma (three samples, 12.0%) were the most prevalent tumours with potentially actionable alterations. The most prevalent tumour-carrying alterations that are currently actionable with approved drugs was breast carcinoma (four samples, 44.4%), followed by prostate adenocarcinoma (two samples, 22.2%) (Figure 1).
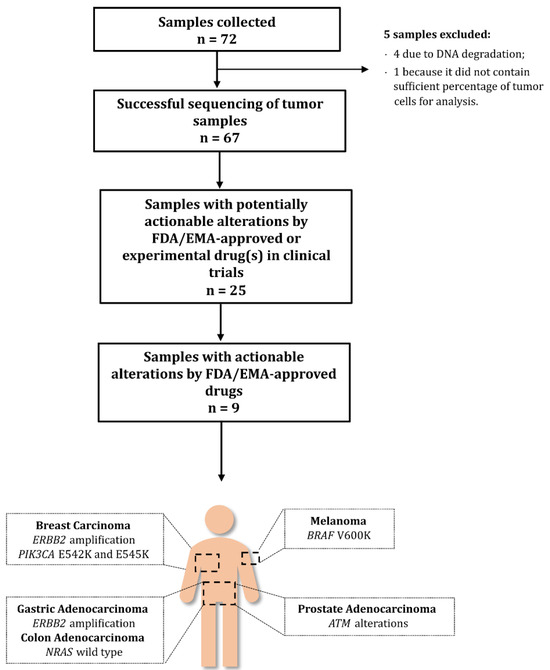
Figure 1.
Potential actionability of detected alterations. A total of 25 samples among the 67 successfully sequenced using Foundation Medicine® testing carried potentially actionable alterations with FDA-/EMA-approved or experimental drug(s). Samples that were derived from breast carcinoma, prostate adenocarcinoma, gastric adenocarcinoma, colon adenocarcinoma, and melanoma carried actionable alterations with currently approved drugs. Breast carcinoma was the most prevalent tumour in this group.
4. Discussion
The clinical approach to cancer patients is evolving, taking into account the identification of relevant genomic alterations that may help guide diagnostic and therapeutic decisions. NGS panels play a key role in this process, providing clinicians with the relevant information within an acceptable time/cost timeframe. The present study reports the first real-world evidence data on the Portuguese population with solid and non-solid malignancies that have undergone NGS study with Foundation Medicine®. Foundation Medicine® testing currently provides a comprehensive platform for the analysis of 324 to 406 genes using three different types of tests for the detection of solid tumours, hematologic malignancies, and sarcomas [9,10,11]. Additionally, this NGS approach delivers information on genomic signatures, including MSI and TMB and loss of heterozygosity (LOH)/homologous recombination deficiency (HDR) [9,10,11].
The median age of the patients included in our study was 60.5 (range 27–82) years, which is similar to the median age of the population reported in different studies that analysed solid tumour samples with the Foundation Medicine® platform [17,18,19,20]. A total of 72 samples were processed for the identification of genomic alterations, and data were obtained for 67 samples, corresponding to a success rate of 93.1%. The obtained success rate is similar to that observed in some studies [20] and higher than the success rates of other reports [21]. The high success rate observed in our series could be attributed to the fact that, prior to shipping, the tissue was always examined by a pathologist with experience in morphological assessment of cases using molecular studies. Despite the logistic factors associated with sending cases to a reference laboratory and conducting a previous assessment by a pathologist before sending the case, the median turnaround time for all samples was 16 days calendar days (range 5–48 days), which is in line with the typical turnaround times expected for Foundation Medicine® testing [9,10,11]. The median percentage of tumour cells collected for the analysis is an additional factor positively contributing to this success rate since the overall median of 40% of tumour cells obtained is above the 20% threshold estimated as adequate for performing genomic profiling [1,20,21,22]. Of the five cases initially excluded from the study, four were due to degradation at the DNA level, and just one was due to insufficient material. All these five cases were reassessed over the course of the study. Four of them were reassessed using FoundationOne Liquid CDx, and one was reassessed using FoundationOne CDx in a repeated tissue biopsy. The results showed significant genomic alterations in three cases, emphasising the need to repeat the genomic analysis whenever possible. The need to repeat the test has a direct impact on the TAT. If we consider the final TAT of these five cases, the median time was 29 days (ranging from 20 to 40 days) because another sample was necessary, and even for blood sample collection, the logistics can be challenging. Although not in the scope of the present study, more recently, another strategy was applied in our laboratory in some of these cases, which is repeating the comprehensive genomic testing in-house using other platforms. We obtained results for around 40% of the cases This is likely related to the strict criteria of acceptability used by the FoundationOne test.
The most commonly altered gene found in the studied samples was TP53. This result is in line with previous studies that report TP53 as the most frequent gene mutated in cancer [23,24]. Previous studies with Foundation Medicine® testing have also reported TP53 as a frequently altered gene [8,20]. Following TP53, KRAS and CDKN2A/B genes were also found frequently altered, which is also in line with previous studies reporting the frequent identification of genomic alterations of KRAS and CDKN2A genes using the FoundationOne CDX panel [8,20,21,24,25].
TMB data were available from 62 of the 72 total samples. TMB is defined as the total number of somatic mutations occurring per coding area of a tumour genome, and previous studies have reported this signature as a potential biomarker that could allow for the identification of patients that are likely to benefit from a treatment approach, including immune checkpoint blockers [26]. In our study, samples were classified as high TMB (≥10 mutations/Mb) and low TMB (<10 mutations/Mb) [20,27,28]. Four samples were identified as high TMB through FoundationOne CDX testing. These samples corresponded to patients with melanoma, breast carcinoma, head and neck squamous cell carcinoma (SCC), and metastatic ovarian tumours. Also, in our study, within the samples analysed with FoundationOne CDX, a positive correlation was found between the number of altered genes and the TMB classification. A high TMB has been associated with patients whose response to immune checkpoint blockade is improved [29,30]. Previous reports have associated high TMB values with clinical responses after using antibodies against PD-1 or PD-L1 [31,32]. TMB has also shown variability among different cancers [33], although a high value can be expected in cancers such as melanoma or head and neck SCC, which is in line with our observations [28]. Additionally, all the high-TMB samples identified in this study corresponded to an MSI-stable status, and MSI-stable tumours linked to a high-TMB status have been reported as potentially benefiting from immunotherapy [34]. However, in this previous study, a different cutoff for the TMB status definition was used [34]. This fact reinforces the need for a consensus on the definition of TMB thresholds that may allow for robust comparisons between different studies.
A total of 25 (37.3%) of the sequenced samples presented at least one alteration that was potentially actionable with either FDA-/EMA-approved drug(s) (9 samples, 36.0%) or experimental drug(s) (16 samples, 64.0%) if there was no approved drug available. Breast carcinoma represented the most prevalent tumour harbouring directly actionable alterations using alpelisib and trastuzumab, with PIK3CA E542K and E545K genomic alterations and ERBB2 amplification.
The samples corresponding to prostate adenocarcinomas were shown to carry ATM alterations. Olaparib has been approved by the FDA and the EMA for addressing homologous recombination repair (HRR) gene-mutated metastatic castration-resistant prostate cancer in 2020 [35], after the date of testing reported for these samples. Additionally, a gastric adenocarcinoma presenting ERBB2 amplification may currently potentially benefit from the recently FDA-approved trastuzumab deruxtecan for adult patients with locally advanced or metastatic HER2-positive gastric adenocarcinoma [36]. Other biomarkers detected in this study were the presence of BRAF V600K alteration and wild-type NRAS derived from melanoma and colon adenocarcinoma samples. Information regarding the follow-up of these patients and specifically concerning their enrolment in clinical trials or potentially performed targeted therapy was not made available for this study.
Despite the presented data and the potential benefits that patients can gain following the development of precision oncology, most of the genomic alterations identified in this study have no direct match with currently approved drugs, as reported in other large series using the same test [17,18,19]. One such example in this study is the cancers of unknown primary, which presented KRAS alterations. Recently, sotorasib has been approved for the treatment of patients with non-small cell lung cancer harbouring KRAS G12C alterations [37]. For patients carrying other KRAS alterations such as G12V, further drug development is needed for achieving selective targeting. These patients may, however, be candidates to enrol in therapeutic clinical trials or recommended for the off-label use of approved therapy based on the potentially actionable alterations reported through the NGS study.
It is also important to note that samples from lung cancer, namely non-small cell lung cancer (NSCLC), were tested in a specific panel and not by Foundation Medicine. Nevertheless, it is important to highlight that, for patients with newly diagnosed non-squamous advanced NSCLC, the use of NGS testing may help to avoid potentially missed targeted therapy options and improve the uptake of testing for recently approved biomarkers and access to clinical trials of molecularly guided therapies [38].
There are some limitations associated with this study, including a small sample size, despite the reduced number of samples excluded from testing due to insufficient material for testing or degradation, and the heterogeneity of the population studied, with most of the patients in an advanced state of the disease. Another limitation is that it was conducted in a single centre; however, the aim was to evaluate local practices and highlight the impact of the tests in routine practice. Moreover, the real-world design of the present study provides data with a real clinical impact without the selective criteria of clinical trials. Patients who underwent testing were selected by physicians, which may lead to selection bias; for example, our study does not include patients with known actionable driver alterations such as those with EGFR mutation-positive lung cancer or HER2-positive breast cancer.
There are also important strengths in this study that should be highlighted. This is the first real-world study reporting the use of Foundation Medicine® testing in Portugal, relying on the use of all three commercially available tests. Additionally, this study included samples from different cancers and 20 centres. Despite the expected preanalytical variability, a high success rate was observed, supporting the robustness of Foundation Medicine® tests.
5. Conclusions
This real-world study demonstrates the successful application of Foundation Medicine® testing in the Portuguese population. Even though a reduced number of potentially actionable genomic alterations with FDA-/EMA-approved drug(s) were identified in this study, the overall genomic information derived from the performed analysis can help physicians to guide patients in clinical trials or direct patients to off-label treatments. These data also highlight the need of developing novel targeted agents that can tackle the identified genomic alterations, either in single or combination therapy. This process may not only provide additional support to the comprehensive use of NGS platforms such as Foundation Medicine® for diagnostic and therapeutic decisions but also for improving patients’ outcomes.
Author Contributions
Conceptualisation, R.P. and F.S.; methodology, R.P. and F.S.; investigation, R.P.; resources, R.P.; data curation, R.P. and F.S.; writing—original draft preparation, R.P. and F.S.; writing—review and editing, F.S.; supervision, F.S.; project administration. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Roche Farmacêutica Quimica Lda.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki. Ethical review and approval were waived as the study is in accordance with Article 19 (‘DNA Banks and Other Biological Products’) of Portuguese Law No. 12/2005 of 26 January (‘Personal genetic information and health information’), which states that in the case of using retrospective samples from human origin or in special situations where the consent of the people involved cannot be obtained because of the amount of data or subjects, of their age, or another reason comparable, material and data can be processed but only for purposes of scientific research or epidemiological and statistical data collection.
Informed Consent Statement
All patients provided written informed consent for the research use of their formalin-fixed, paraffin-embedded (FFPE) tissue and peripheral whole blood samples.
Data Availability Statement
Not applicable.
Acknowledgments
The authors wish to acknowledge all the IPATIMUP Diagnostics team for their support. The authors thank X2—Science Solutions for providing medical writing support, in accordance with Good Publication Practice (GPP3) guidelines.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Correction Statement
This article has been republished with a minor correction of the information included in the Institutional Review Board Statement. This change does not affect the scientific content of the article.
References
- Avila, M.; Meric-Bernstam, F. Next-generation sequencing for the general cancer patient. Clin. Adv. Hematol. Oncol. 2019, 17, 447–454. [Google Scholar]
- Mockus, S.M.; Patterson, S.E.; Statz, C.; Bult, C.J.; Tsongalis, G.J. Clinical Trials in Precision Oncology. Clin. Chem. 2016, 62, 442–448. [Google Scholar] [CrossRef]
- Radovich, M.; Kiel, P.J.; Nance, S.M.; Niland, E.E.; Parsley, M.E.; Ferguson, M.E.; Jiang, G.; Ammakkanavar, N.R.; Einhorn, L.H.; Cheng, L.; et al. Clinical benefit of a precision medicine based approach for guiding treatment of refractory cancers. Oncotarget 2016, 7, 56491–56500. [Google Scholar] [CrossRef] [PubMed]
- Woodhouse, R.; Li, M.; Hughes, J.; Delfosse, D.; Skoletsky, J.; Ma, P.; Meng, W.; Dewal, N.; Milbury, C.; Clark, T.; et al. Clinical and analytical validation of FoundationOne Liquid CDx, a novel 324-Gene cfDNA-based comprehensive genomic profiling assay for cancers of solid tumor origin. PLoS ONE 2020, 15, e0237802. [Google Scholar] [CrossRef]
- Chouaid, C.; Dujon, C.; Do, P.; Monnet, I.; Madroszyk, A.; Le Caer, H.; Auliac, J.B.; Berard, H.; Thomas, P.; Lena, H.; et al. Feasibility and clinical impact of re-biopsy in advanced non small-cell lung cancer: A prospective multicenter study in a real-world setting (GFPC study 12-01). Lung Cancer 2014, 86, 170–173. [Google Scholar] [CrossRef] [PubMed]
- Schwaederle, M.C.; Patel, S.P.; Husain, H.; Ikeda, M.; Lanman, R.B.; Banks, K.C.; Talasaz, A.; Bazhenova, L.; Kurzrock, R. Utility of Genomic Assessment of Blood-Derived Circulating Tumor DNA (ctDNA) in Patients with Advanced Lung Adenocarcinoma. Clin. Cancer Res. 2017, 23, 5101–5111. [Google Scholar] [CrossRef]
- Frampton, G.M.; Fichtenholtz, A.; Otto, G.A.; Wang, K.; Downing, S.R.; He, J.; Schnall-Levin, M.; White, J.; Sanford, E.M.; An, P.; et al. Development and validation of a clinical cancer genomic profiling test based on massively parallel DNA sequencing. Nat. Biotechnol. 2013, 31, 1023–1031. [Google Scholar] [CrossRef]
- Karol, D.; McKinnon, M.; Mukhtar, L.; Awan, A.; Lo, B.; Wheatley-Price, P. The Impact of Foundation Medicine Testing on Cancer Patients: A Single Academic Centre Experience. Front. Oncol. 2021, 11, 687730. [Google Scholar] [CrossRef] [PubMed]
- Foundation Medicine. FoundationOne® CDx Technical Information. Available online: https://www.rochefoundationmedicine.com/f1cdxtech (accessed on 7 February 2022).
- Foundation Medicine. FoundationOne® Liquid CDx Technical Information. Available online: https://info.foundationmedicine.com/hubfs/FMI%20Labels/FoundationOne_Liquid_CDx_Label_Technical_Info.pdf (accessed on 7 February 2022).
- Foundation Medicine. FoundationOne® Heme Technical Specifications. Available online: https://assets.ctfassets.net/w98cd481qyp0/42r1cTE8VR4137CaHrsaen/a7e4b78c5ee67503ede12ef0c3507de3/FoundationOne_Heme_Technical_Specifications.pdf (accessed on 7 February 2022).
- Ali, S.M.; Palma, N.A.; Wang, K.; Ross, J.S.; Stephens, P.J.; Yelensky, R.; Palmer, G.A.; Lipson, D.; Miller, V.A. Clinical next generation sequencing (NGS) to reveal high frequency of alterations to guide targeted therapy in lung cancer patients. J. Clin. Oncol. 2013, 31, 8020. [Google Scholar] [CrossRef]
- Boland, P.M.; Skarbnik, A.P.; Cristofanilli, M.; Alpaugh, R.K.; Olszanski, A.J. Application of next-generation sequencing (NGS) for evaluation of advanced epithelial cancers: A single institution experience. J. Clin. Oncol. 2013, 31, 11092. [Google Scholar] [CrossRef]
- He, J.; Patel, M.; Phillip, I.; Bailey, M.; Berman, E.; Park, J.H.; Shukla, N.N.; Chung, S.S.; Castro-Malaspina, H.; Douer, D.; et al. Clinical Relevant Alterations Identified By Comprehensive Genomic Profiling Can Potentially Improve Therapeutic Option and Change Prognosis in Hematologic Malignancies. Blood 2016, 128, 5109. [Google Scholar] [CrossRef]
- Parrondo, R.D.; Mariotti, V.; Gonzalez Velez, M.; Leslie, L.A. Clinical implications of genomic-directed therapies by comprehensive genomic profiling in breast cancer patients at a large academic cancer center. J. Clin. Oncol. 2017, 35, e12037. [Google Scholar] [CrossRef]
- Gullo, I.; Marques, A.; Pinto, R.; Cirnes, L.; Schmitt, F. Morphological control for molecular testing: A practical approach. J. Clin. Pathol. 2021, 74, 331–333. [Google Scholar] [CrossRef]
- Aoyagi, Y.; Kano, Y.; Tohyama, K.; Matsudera, S.; Kumaki, Y.; Takahashi, K.; Mitsumura, T.; Harada, Y.; Sato, A.; Nakamura, H.; et al. Clinical utility of comprehensive genomic profiling in Japan: Result of PROFILE-F study. PLoS ONE 2022, 17, e0266112. [Google Scholar] [CrossRef] [PubMed]
- Pinet, S.; Durand, S.; Perani, A.; Darnaud, L.; Amadjikpe, F.; Yon, M.; Darbas, T.; Vergnenegre, A.; Egenod, T.; Simonneau, Y.; et al. Clinical management of molecular alterations identified by high throughput sequencing in patients with advanced solid tumors in treatment failure: Real-world data from a French hospital. Front. Oncol. 2023, 13, 1104659. [Google Scholar] [CrossRef]
- Teuwen, L.A.; Roets, E.; D’Hoore, P.; Pauwels, P.; Prenen, H. Comprehensive Genomic Profiling and Therapeutic Implications for Patients with Advanced Cancers: The Experience of an Academic Hospital. Diagnostics 2023, 13, 1619. [Google Scholar] [CrossRef]
- Takeda, M.; Takahama, T.; Sakai, K.; Shimizu, S.; Watanabe, S.; Kawakami, H.; Tanaka, K.; Sato, C.; Hayashi, H.; Nonagase, Y.; et al. Clinical Application of the FoundationOne CDx Assay to Therapeutic Decision-Making for Patients with Advanced Solid Tumors. Oncologist 2021, 26, e588–e596. [Google Scholar] [CrossRef]
- De Falco, V.A.-O.; Poliero, L.; Vitello, P.P.; Ciardiello, D.; Vitale, P.; Zanaletti, N.; Giunta, E.F.; Terminiello, M.; Caputo, V.; Carlino, F.; et al. Feasibility of next-generation sequencing in clinical practice: Results of a pilot study in the Department of Precision Medicine at the University of Campania ‘Luigi Vanvitelli’. ESMO Open 2020, 5, e000675. [Google Scholar] [CrossRef] [PubMed]
- Su, D.; Zhang, D.; Chen, K.; Lu, J.; Wu, J.; Cao, X.; Ying, L.; Jin, Q.; Ye, Y.; Xie, Z.; et al. High performance of targeted next generation sequencing on variance detection in clinical tumor specimens in comparison with current conventional methods. J. Exp. Clin. Cancer Res. 2017, 36, 121. [Google Scholar] [CrossRef]
- Baugh, E.H.; Ke, H.; Levine, A.J.; Bonneau, R.A.; Chan, C.S. Why are there hotspot mutations in the TP53 gene in human cancers? Cell Death Differ. 2018, 25, 154–160. [Google Scholar] [CrossRef]
- Hirshfield, K.M.; Tolkunov, D.; Zhong, H.; Ali, S.M.; Stein, M.N.; Murphy, S.; Vig, H.; Vazquez, A.; Glod, J.; Moss, R.A.; et al. Clinical Actionability of Comprehensive Genomic Profiling for Management of Rare or Refractory Cancers. Oncologist 2016, 21, 1315–1325. [Google Scholar] [CrossRef]
- Kimura, R.; Ohtsuka, T.; Kubo, M.; Kajihara, A.; Fujii, A.; Watanabe, Y.; Mori, Y.; Ikenaga, N.; Nakata, K.; Shindo, K.; et al. FoundationOne(R) CDx gene profiling in Japanese pancreatic ductal adenocarcinoma patients: A single-institution experience. Surg. Today 2021, 51, 619–626. [Google Scholar] [CrossRef] [PubMed]
- Marabelle, A.; Fakih, M.; Lopez, J.; Shah, M.; Shapira-Frommer, R.; Nakagawa, K.; Chung, H.C.; Kindler, H.L.; Lopez-Martin, J.A.; Miller, W.H., Jr.; et al. Association of tumour mutational burden with outcomes in patients with advanced solid tumours treated with pembrolizumab: Prospective biomarker analysis of the multicohort, open-label, phase 2 KEYNOTE-158 study. Lancet Oncol. 2020, 21, 1353–1365. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.S.P.; Haberberger, J.; Severson, E.; Duncan, D.L.; Hemmerich, A.; Edgerly, C.; Ferguson, N.L.; Williams, E.; Elvin, J.; Vergilio, J.A.; et al. A pan-cancer analysis of PD-L1 immunohistochemistry and gene amplification, tumor mutation burden and microsatellite instability in 48,782 cases. Mod. Pathol. 2021, 34, 252–263. [Google Scholar] [CrossRef] [PubMed]
- Sha, D.; Jin, Z.; Budczies, J.; Kluck, K.; Stenzinger, A.; Sinicrope, F.A. Tumor Mutational Burden as a Predictive Biomarker in Solid Tumors. Cancer Discov. 2020, 10, 1808–1825. [Google Scholar] [CrossRef]
- Fancello, L.; Gandini, S.; Pelicci, P.G.; Mazzarella, L. Tumor mutational burden quantification from targeted gene panels: Major advancements and challenges. J. Immunother. Cancer 2019, 7, 183. [Google Scholar] [CrossRef]
- Stenzinger, A.; Allen, J.D.; Maas, J.; Stewart, M.D.; Merino, D.M.; Wempe, M.M.; Dietel, M. Tumor mutational burden standardization initiatives: Recommendations for consistent tumor mutational burden assessment in clinical samples to guide immunotherapy treatment decisions. Genes. Chromosomes Cancer 2019, 58, 578–588. [Google Scholar] [CrossRef]
- Ott, P.A.; Bang, Y.J.; Piha-Paul, S.A.; Razak, A.R.A.; Bennouna, J.; Soria, J.C.; Rugo, H.S.; Cohen, R.B.; O’Neil, B.H.; Mehnert, J.M.; et al. T-Cell-Inflamed Gene-Expression Profile, Programmed Death Ligand 1 Expression, and Tumor Mutational Burden Predict Efficacy in Patients Treated With Pembrolizumab Across 20 Cancers: KEYNOTE-028. J. Clin. Oncol. 2019, 37, 318–327. [Google Scholar] [CrossRef]
- Yarchoan, M.; Hopkins, A.; Jaffee, E.M. Tumor Mutational Burden and Response Rate to PD-1 Inhibition. N. Engl. J. Med. 2017, 377, 2500–2501. [Google Scholar] [CrossRef]
- Chalmers, Z.R.; Connelly, C.F.; Fabrizio, D.; Gay, L.; Ali, S.M.; Ennis, R.; Schrock, A.; Campbell, B.; Shlien, A.; Chmielecki, J.; et al. Analysis of 100,000 human cancer genomes reveals the landscape of tumor mutational burden. Genome Med. 2017, 9, 34. [Google Scholar] [CrossRef]
- Goodman, A.M.; Sokol, E.S.; Frampton, G.M.; Lippman, S.M.; Kurzrock, R. Microsatellite-Stable Tumors with High Mutational Burden Benefit from Immunotherapy. Cancer Immunol. Res. 2019, 7, 1570–1573. [Google Scholar] [CrossRef] [PubMed]
- Dror, C.M.; Wyatt, A.W.; Chi, K.N. Olaparib for the treatment of metastatic prostate cancer. Future Oncol. 2021, 17, 2413–2429. [Google Scholar] [CrossRef] [PubMed]
- Grieb, B.C.; Agarwal, R. HER2-Directed Therapy in Advanced Gastric and Gastroesophageal Adenocarcinoma: Triumphs and Troubles. Curr. Treat. Options Oncol. 2021, 22, 88. [Google Scholar] [CrossRef]
- Blair, H.A. Sotorasib: First Approval. Drugs 2021, 81, 1573–1579. [Google Scholar] [CrossRef] [PubMed]
- Paz-Ares, L.; Gondos, A.; Saldana, D.; Thomas, M.; Mascaux, C.; Bubendorf, L.; Barlesi, F. Genomic testing among patients with newly diagnosed advanced non-small cell lung cancer in the United States: A contemporary clinical practice patterns study. Lung Cancer 2022, 167, 41–48. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).