Abstract
Introduction: Cryptococcal meningoencephalitis is a life-threatening disease affecting mainly immunocompromised hosts. Case report: We present a case of a 64-year-old immunocompetent patient, who initially developed a traumatic scalp skin infection due to Cryptococcus neoformans. The patient received oral fluconazole and subsequently liposomal amphotericin B due to the development of resistance with resolution of the infection. Two years later, during chemotherapy for newly diagnosed gastric and lung cancer, he developed fulminant cryptococcal meningoencephalitis, which did not respond to liposomal amphotericin B and flucytosine. Conclusions: To our knowledge, this is the first case of fulminant cryptococcal meningoencephalitis following long latency after adequately treated primary cutaneous infection.
Introduction
Among the 19 species of Cryptococcus identified so far, mainly two are known to cause disease in humans, Cryptococcus neoformans and Cryptococcus gattii [1]. Recently, other saprophytic species have been recognized as uncommon agents of cryptococcosis, such as Cryptococcus laurentii [2]. These encapsulated fungi and in particular Cryptococcus neoformans, usually affect immunocompromised hosts, especially HIV positive patients; however, infections are increasingly reported in immunocompetent individuals with undefined risk factors so far. Cryptococcus neoformans usually enters the human organism through inhalation, thus establishing an asymptomatic pulmonary infection. It ultimately targets the central nervous system; to achieve that, it has to defeat the host innate immune system and to cross the blood-brain barrier [3,4]. Cryptococcal skin lesions often represent the first signs of infection; however, these usually prove to be secondary deposits of disseminated disease [5,6]. Primary cutaneous cryptococcosis is rare [7,8]. We report a unique case of fatal cryptococcal meningoencephalitis that probably represented reactivation of a latent primary cutaneous infection upon initiation of chemotherapy.
Case report
A 64-year-old male patient was admitted to the hospital with 15-day fever and headache of one-month duration of increasing intensity.
The history of the patient was remarkable of a hospital admission two years ago due to a C. neoformans scalp skin infection in the parietal area of the head, which developed after an olive tree branch trauma. The patient was negative for HIV serology. An extensive investigation for other pathologies was negative, except for prostate gland hyperplasia. At that point, computed tomography scanning of thorax and abdomen for dissemination of cryptococcosis were unremarkable.
Before that admission the patient was initially treated on an outpatient basis with oral fluconazole 200 mg qd which was raised to 600 mg qd and subsequently switched to liposomal amphotericin B 3 mg/kg intravenously for one month, due to the development of resistance to fluconazole (MIC 32 μg/mL) with complete resolution of the skin lesion. Susceptibility of the strain to the other antifungals tested was as follows: amphotericin B MIC 0.25 μg/mL, 5-flucytosine MIC 4 μg/mL.
Two years later (six months prior to the current admission), the patient was diagnosed with gastric cancer that was surgically resected and one month later with primary lung adenocarcinoma, which was also excised and for which chemotherapy was initiated. The last chemotherapy session was administered about 15 days prior to admission. Upon admission, the patient was febrile (38.0 °C), and complained of marked tension headache. White blood cell count was normal (6,800 cells/μL) and inflammatory markers were mildly elevated (C-reactive protein 19.8 mg/L, nv<5 mg/L). Chest X-ray and urinalysis were normal. Computed tomography scanning and magnetic resonance imaging of the central nervous system revealed only periventricular leukoencephalopathy. Cerebrospinal fluid analysis yielded 5 cells/μL, glucose 6 mg/dL, protein 41 mg/dL and yeast-like cells that were evident on Gram stain. Cryptococcus neoformans grew from blood and CSF cultures.
Based on the patient’s history (cryptococcal skin infection by a fluconazole-resistant strain), treatment was initiated with intravenous liposomal amphotericin B (4 mg/kg) and IV flucytosine (25 mg/kg every 6h). HIV antibodies tested negative and T cell subset determination in peripheral blood revealed normal CD3+CD4+/CD3+CD8+ T cell ratio and an increased number of NK cells. The patient’s clinical condition deteriorated within 4 days with loss of vision and intense neck rigidity. Repeated magnetic resonance imaging of the brain revealed lesions compatible with infectious meningoencephalitis (abnormal leptomeningeal enhancement in the frontal, parietal and posterior cranial fossa and dilated perivascular spaces in the bilateral basal ganglia; Figure 1a,b). Despite continuous antifungal therapy the patient died one week after initiation of treatment. The relatives of the patient gave us written informed consent to publish this case.
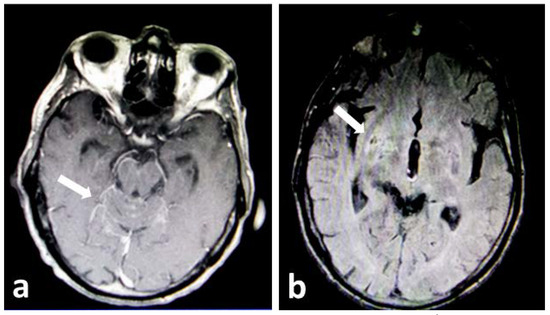
Figure 1.
Brain magnetic resonance images in the advanced stages of the disease showing a. abnormal leptomeningeal enhancement in the posterior cranial fossa (white arrow) and b. dilated perivascular spaces in the bilateral basal ganglia (white arrow pointing to the lesions on the right hemisphere). At the time when the scan was performed, the patient had severe neck rigidity and loss of vision.
Discussion
To our knowledge, this is the first case reported of a fatal cryptococcal meningoencephalitis case developing two years after a cured primary cutaneous cryptococcal infection.
Cryptococcus is usually acquired through inhalation, leading to an initial symptomatic or latent pulmonary infection [9]. In the case of our patient initial infection appeared to have been caused by cutaneous inoculation caused by skin injury on his head and leading to the initial development of primary cutaneous cryptococcosis without any obvious involvement of the underlying bone. Both at the time of diagnosis of the skin infection, as well as at the time of lung adenocarcinoma diagnosis, the patient did not have any evidence of cryptococcal lung infection. Primary cutaneous cryptococcosis, a diagnosis that is based on the absence of invasive manifestations in other sites, is by itself a rare clinical entity [7]. If left untreated, it may cause disseminated disease [10]. Following initial clinical improvement after treatment with fluconazole our patient developed a persistent infection due to the development of resistance and needed to receive liposomal amphotericin B with complete regression of the lesion.
Fluconazole is the mainstay of cryptococcal treatment. Its prolonged use can, however, induce selection pressure for resistant Cryptococcus strains [11]. Two years later, he developed a fulminant central nervous system infection with dismal outcome despite antifungal therapy, which further indicates the urgent need to establish antifungal breakpoints for Cryptococcus spp. In the absence of evidence of a re-infection or other site involvement, cryptococci may have persisted in a latent state throughout and reactivated during antineoplastic chemotherapy, although reactivation remains a hypothesis in this case that unfortunately cannot be supported by molecular evidence.
Conclusions
Our patient’s case appears to be the first case reported as a disseminated cryptococcal infection after a long latent period following a complete cure of a primary cutaneous cryptococcosis episode.
Author Contributions
I.R. participated in the care of the patient, wrote the first draft and approved the final version. Z.D.P., D.I. and A.K. reviewed the manuscript and approved the final version. A.P. and ER participated in the care of the patient, reviewed the manuscript and approved the final version. I.L., E.A., M.S. and E.C. participated in the care of the patient and approved the final version. All authors read and approved the final version of manuscript.
Funding
None to declare.
Informed Consent Statement
Written informed consent was obtained from the patient’s family for publication of this case report and images.
Conflicts of Interest
All authors—none to declare.
References
- Kwon-Chung, K.J.; Fraser, J.A.; Doering, T.L.; et al. Cryptococcus neoformans and Cryptococcus gattii, the etiologic agents of cryptococcosis. Spring Harb Perspect Med. 2014, 4, a019760. [Google Scholar] [CrossRef] [PubMed]
- Castro-Lainez, M.T.; Deliz-Aguirre, R.; Antunez, D.; et al. Cryptococcus laurentii meningitis in a non-HIV patient. IDCases. 2019, 18, e00612. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.L.; Wang, J.; Zou, L.L. Innate immune evasion strategies against Cryptococcal meningitis caused by Cryptococcus neoformans. Exp Ther Med. 2017, 14, 5243–5250. [Google Scholar] [CrossRef] [PubMed]
- Coelho, C.; Bocca, A.L.; Casadevall, A. The tools for virulence of Cryptococcus neoformans. Adv Appl Microbiol. 2014, 87, 1–41. [Google Scholar] [CrossRef] [PubMed]
- Henderson, G.P.; Dreyer, S. Ulcerative cellulitis of the arm: A case of primary cutaneous cryptococcosis. Dermatol Online J. 2018, 24, 9. [Google Scholar] [CrossRef]
- Srivastava, G.N.; Tilak, R.; Yadav, J.; Bansal, M. Cutaneous Cryptococcus: Marker for disseminated infection. BMJ Case Rep. 2015, 2015, bcr2015210898. [Google Scholar] [CrossRef] [PubMed]
- Du, L.; Yang, Y.; Gu, J.; Chen, J.; Liao, W.; Zhu, Y. Systemic review of published reports on primary cutaneous cryptococcosis in immunocompetent patients. Mycopathologia. 2015, 180, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Arjona-Aguilera, C.; Jiménez-Gallo, D.; Collantes-Rodríguez, C.; Linares-Barrios, M. Primary cutaneous cryptococcosis: A new case of this rare entity. Open Forum Infect Dis. 2017, 4, ofw276. [Google Scholar] [CrossRef] [PubMed]
- Amaral, D.M.; Rocha, R.C.; Carneiro, L.E.; Vasconcelos, D.M.; Abreu, M.A. Disseminated cryptococcosis manifested as a single tumor in an immunocompetent patient, similar to the cutaneous primary forms. An Bras Dermatol. 2016, 91 (Suppl. S1), 29–31. [Google Scholar] [CrossRef] [PubMed]
- Tilak, R.; Prakash, P.; Nigam, C.; Tilak, V.; Gambhir, I.S.; Gulati, A.K. Cryptococcal meningitis with an antecedent cutaneous cryptococcal lesion. Dermatol Online J. 2009, 15, 12. [Google Scholar] [CrossRef] [PubMed]
- Bongomin, F.; Oladele, R.O.; Gago, S.; Moore, C.B.; Richardson, M.D. A systematic review of fluconazole resistance in clinical isolates of Cryptococcus species. Mycoses. 2018, 61, 290–297. [Google Scholar] [CrossRef] [PubMed]

© GERMS 2020.