
High Levels of Low-Density Lipoproteins Correlate with Improved Survival in Patients with Squamous Cell Carcinoma of the Head and Neck

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Cohort
2.2. Blood Collection and Lipoprotein Analysis
2.3. Statistical Analysis
3. Results
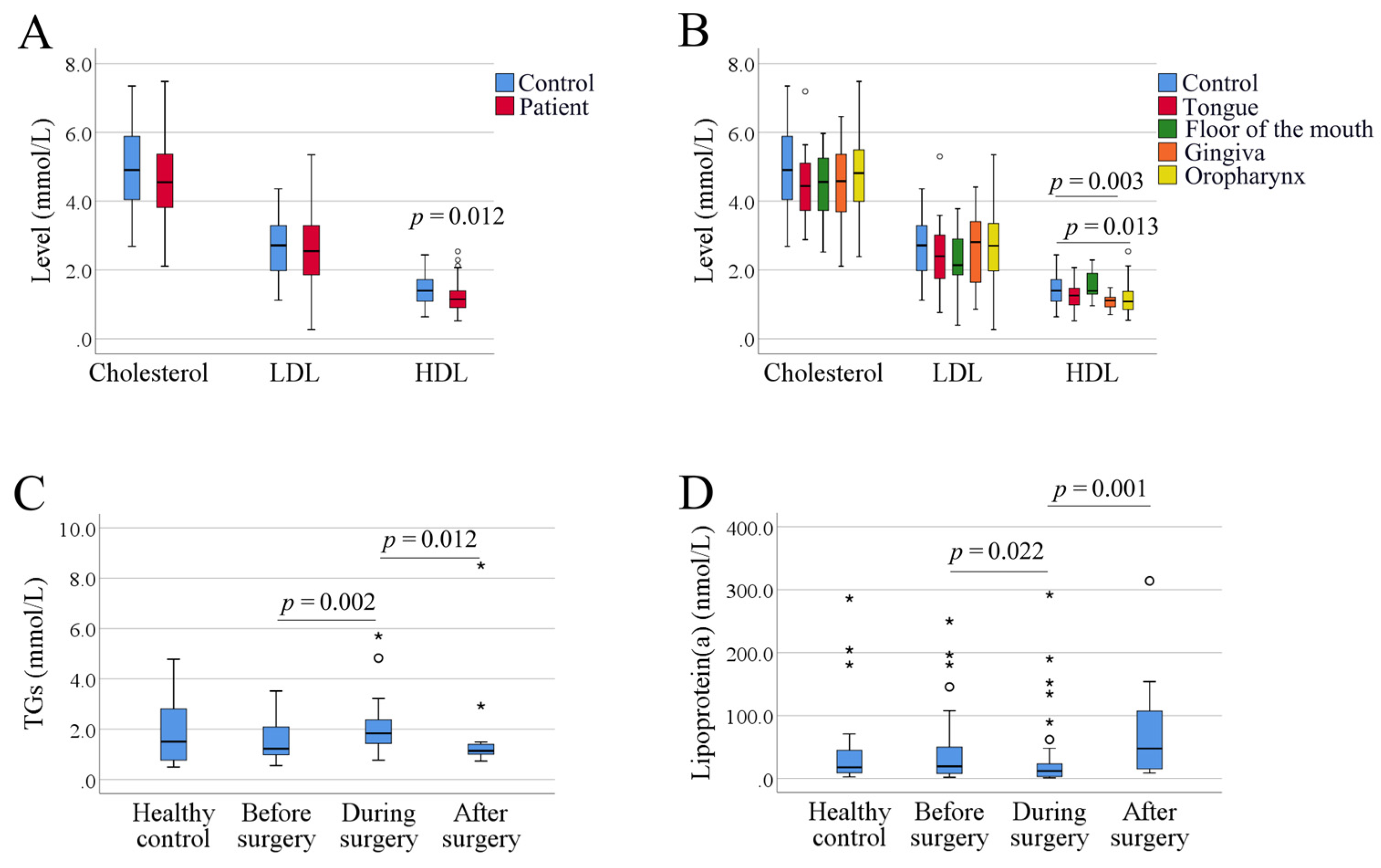
3.1. Serum Lipid Levels in SCCHN Patients Compared to Controls
3.2. Clinicopathological Data in Correlation to Levels of Lipoproteins
3.3. Levels of Lipoproteins in Correlation to Survival
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Henderson, B.E.; Lee, N.H.; Seewaldt, V.; Shen, H. The influence of race and ethnicity on the biology of cancer. Nat. Rev. Cancer 2012, 12, 648–653. [Google Scholar] [CrossRef]
- Cohen Goldemberg, D.; de Araujo, L.H.L.; Antunes, H.S.; de Melo, A.C.; Santos Thuler, L.C. Tongue cancer epidemiology in Brazil: Incidence, morbidity and mortality. Head Neck 2018, 40, 1834–1844. [Google Scholar] [CrossRef]
- Miranda-Filho, A.; Bray, F. Global patterns and trends in cancers of the lip, tongue and mouth. Oral Oncol. 2020, 102, 104551. [Google Scholar] [CrossRef] [PubMed]
- Lohe, V.K.; Degwekar, S.S.; Bhowate, R.R.; Kadu, R.P.; Dangore, S.B. Evaluation of correlation of serum lipid profile in patients with oral cancer and precancer and its association with tobacco abuse. J. Oral Pathol. Med. 2010, 39, 141–148. [Google Scholar] [CrossRef]
- Silvente-Poirot, S.; Poirot, M. Cholesterol and Cancer, in the Balance. Science 2014, 343, 1445–1446. [Google Scholar] [CrossRef] [PubMed]
- Boretti, A. Nutrition, lipidic parameters, and cancer risk and progress. Nutrition 2020, 69, 110538. [Google Scholar] [CrossRef]
- Lemieux, I.; Lamarche, B.; Couillard, C.; Pascot, A.; Cantin, B.; Bergeron, J.; Dagenais, G.R.; Despres, J.P. Total cholesterol/HDL cholesterol ratio vs LDL cholesterol/HDL cholesterol ratio as indices of ischemic heart disease risk in men: The Quebec Cardiovascular Study. Arch. Intern. Med. 2001, 161, 2685–2692. [Google Scholar] [CrossRef]
- Weiss, A.; Beloosesky, Y.; Schmilovitz-Weiss, H.; Grossman, E.; Boaz, M. Serum total cholesterol: A mortality predictor in elderly hospitalized patients. Clin. Nutr. 2013, 32, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Kawachi, K.; Kataoka, H.; Manabe, S.; Mochizuki, T.; Nitta, K. Low HDL cholesterol as a predictor of chronic kidney disease progression: A cross-classification approach and matched cohort analysis. Heart Vessel. 2019, 34, 1440–1455. [Google Scholar] [CrossRef]
- Li, B.; McIntyre, M.; Gandhi, C.; Halabi, M.; Long, A.; Van Hoof, A.; Afridi, A.; Schmidt, M.; Cole, C.; Santarelli, J.; et al. Low total cholesterol and high density lipoprotein are independent predictors of poor outcomes following aneurysmal subarachnoid hemorrhage: A preliminary report. Clin. Neurol. Neurosurg. 2020, 197, 106062. [Google Scholar] [CrossRef]
- Kark, J.D.; Smith, A.H.; Hames, C.G. Serum retinol and the inverse relationship between serum cholesterol and cancer. Br. Med. J. (Clin. Res. Ed.) 1982, 284, 152–154. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.S.; Shah, M.H.; Jha, F.P.; Raval, G.N.; Rawal, R.M.; Patel, M.M.; Patel, J.B.; Patel, D.D. Alterations in plasma lipid profile patterns in head and neck cancer and oral precancerous conditions. Indian J. Cancer 2004, 41, 25–31. [Google Scholar]
- Yao, J.J.; He, X.J.; Lawrence, W.R.; Zhang, W.J.; Kou, J.; Zhang, F.; Zhou, G.Q.; Wang, S.Y.; Sun, Y. Prognostic Value of Circulating Lipoprotein in Patients with Locoregionally Advanced Nasopharyngeal Carcinoma. Cell. Physiol. Biochem. 2018, 48, 285–292. [Google Scholar] [CrossRef]
- Li, G.; Da, M.; Zhang, W.; Wu, H.; Ye, J.; Chen, J.; Ma, L.; Gu, N.; Wu, Y.; Song, X. Alteration of serum lipid profile and its prognostic value in head and neck squamous cell carcinoma. J. Oral Pathol. Med. 2016, 45, 167–172. [Google Scholar] [CrossRef]
- Kyrgiou, M.; Kalliala, I.; Markozannes, G.; Gunter, M.J.; Paraskevaidis, E.; Gabra, H.; Martin-Hirsch, P.; Tsilidis, K.K. Adiposity and cancer at major anatomical sites: Umbrella review of the literature. BMJ 2017, 356, j477. [Google Scholar] [CrossRef]
- Mika, A.; Sledzinski, T. Alterations of specific lipid groups in serum of obese humans: A review. Obes. Rev. 2017, 18, 247–272. [Google Scholar] [CrossRef] [PubMed]
- Hu, Q.; Peng, J.; Chen, X.; Li, H.; Song, M.; Cheng, B.; Wu, T. Obesity and genes related to lipid metabolism predict poor survival in oral squamous cell carcinoma. Oral Oncol. 2019, 89, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Varady, K.A.; Tussing, L.; Bhutani, S.; Braunschweig, C.L. Degree of weight loss required to improve adipokine concentrations and decrease fat cell size in severely obese women. Metabolism 2009, 58, 1096–1101. [Google Scholar] [CrossRef]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corra, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts)Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef]
- Nicholls, S.J.; Tang, W.H.; Scoffone, H.; Brennan, D.M.; Hartiala, J.; Allayee, H.; Hazen, S.L. Lipoprotein(a) levels and long-term cardiovascular risk in the contemporary era of statin therapy. J. Lipid Res. 2010, 51, 3055–3061. [Google Scholar] [CrossRef]
- Boldrup, L.; Coates, P.J.; Laurell, G.; Nylander, K. Differences in p63 expression in SCCHN tumours of different sub-sites within the oral cavity. Oral Oncol. 2011, 47, 861–865. [Google Scholar] [CrossRef] [PubMed]
- Boldrup, L.; Coates, P.J.; Wahlgren, M.; Laurell, G.; Nylander, K. Subsite-based alterations in miR-21, miR-125b, and miR-203 in squamous cell carcinoma of the oral cavity and correlation to important target proteins. J. Carcinog. 2012, 11, 18. [Google Scholar] [CrossRef] [PubMed]
- Bailwad, S.A.; Singh, N.; Jani, D.R.; Patil, P.; Singh, M.; Deep, G.; Singh, S. Alterations in serum lipid profile patterns in oral cancer: Correlation with histological grading and tobacco abuse. Oral Health Dent. Manag. 2014, 13, 573–579. [Google Scholar] [PubMed]
- Ganjali, S.; Ricciuti, B.; Pirro, M.; Butler, A.E.; Atkin, S.L.; Banach, M.; Sahebkar, A. High-Density Lipoprotein Components and Functionality in Cancer: State-of-the-Art. Trends Endocrinol. Metab. 2019, 30, 12–24. [Google Scholar] [CrossRef]
- Allampallam, K.; Dutt, D.; Nair, C.; Shetty, V.; Mundle, S.; Lisak, L.; Andrews, C.; Ahmed, B.; Mazzone, L.; Zorat, F.; et al. The clinical and biologic significance of abnormal lipid profiles in patients with myelodysplastic syndromes. J. Hematother. Stem Cell Res. 2000, 9, 247–255. [Google Scholar] [CrossRef]
- Guan, X.; Liu, Z.; Zhao, Z.; Zhang, X.; Tao, S.; Yuan, B.; Zhang, J.; Wang, D.; Liu, Q.; Ding, Y. Emerging roles of low-density lipoprotein in the development and treatment of breast cancer. Lipids Health Dis. 2019, 18, 137. [Google Scholar] [CrossRef]
- Kreger, B.E.; Anderson, K.M.; Schatzkin, A.; Splansky, G.L. Serum cholesterol level, body mass index, and the risk of colon cancer. The Framingham Study. Cancer 1992, 70, 1038–1043. [Google Scholar] [CrossRef]
- Li, T.; Qian, Y.; Li, H.; Deng, J. Combination of serum lipids and cancer antigens as a novel marker for colon cancer diagnosis. Lipids Health Dis. 2018, 17, 261. [Google Scholar] [CrossRef]
- Hao, B.; Yu, M.; Sang, C.; Bi, B.; Chen, J. Dyslipidemia and non-small cell lung cancer risk in Chinese population: A case-control study. Lipids Health Dis. 2018, 17, 278. [Google Scholar] [CrossRef]
- Zhou, T.; Zhan, J.; Fang, W.; Zhao, Y.; Yang, Y.; Hou, X.; Zhang, Z.; He, X.; Zhang, Y.; Huang, Y.; et al. Serum low-density lipoprotein and low-density lipoprotein expression level at diagnosis are favorable prognostic factors in patients with small-cell lung cancer (SCLC). BMC Cancer 2017, 17, 269. [Google Scholar] [CrossRef]
- Chen, P.; Han, L.; Wang, C.; Jia, Y.; Song, Q.; Wang, J.; Guan, S.; Tan, B.; Liu, B.; Jia, W.; et al. Preoperative serum lipids as prognostic predictors in esophageal squamous cell carcinoma patients with esophagectomy. Oncotarget 2017, 8, 41605–41619. [Google Scholar] [CrossRef]
- Li, A.J.; Elmore, R.G.; Chen, I.Y.; Karlan, B.Y. Serum low-density lipoprotein levels correlate with survival in advanced stage epithelial ovarian cancers. Gynecol. Oncol. 2010, 116, 78–81. [Google Scholar] [CrossRef] [PubMed]
- Hollander, D.; Kampman, E.; van Herpen, C.M. Pretreatment body mass index and head and neck cancer outcome: A review of the literature. Crit. Rev. Oncol. Hematol. 2015, 96, 328–338. [Google Scholar] [CrossRef] [PubMed]
- Karnell, L.H.; Sperry, S.M.; Anderson, C.M.; Pagedar, N.A. Influence of body composition on survival in patients with head and neck cancer. Head Neck 2016, 38 (Suppl. 1), E261–E267. [Google Scholar] [CrossRef]
- Iyengar, N.M.; Kochhar, A.; Morris, P.G.; Morris, L.G.; Zhou, X.K.; Ghossein, R.A.; Pino, A.; Fury, M.G.; Pfister, D.G.; Patel, S.G.; et al. Impact of obesity on the survival of patients with early-stage squamous cell carcinoma of the oral tongue. Cancer 2014, 120, 983–991. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Clinical Features | Number of Patients | |
|---|---|---|
| Tumor Localization | Tongue | 28 |
| Floor of the mouth | 9 | |
| Gingivae | 21 | |
| Oropharynx (tonsils and/or base of the tongue) | 48 | |
| Age at Diagnosis | ≤40 years | 8 |
| 41 to 65 years | 50 | |
| >65 years | 48 | |
| Gender | Female | 36 |
| Male | 70 | |
| Smoking | Non-smoker | 38 |
| Previous smoker | 31 | |
| Smoker | 37 | |
| Alcohol | No | 24 |
| Yes | 82 | |
| HPV Status | Negative | 67 |
| Positive | 39 | |
| BMI | Underweight (<18.5) | 4 |
| Normal (18.5 to 24) | 46 | |
| Overweight (25 to 30) | 40 | |
| Obese (>30) | 16 | |
| Weight change | No change | 64 |
| Increase of 1 to 5 kg | 4 | |
| Decrease of 1 to 5 kg | 20 | |
| Decrease > 5 kg | 18 | |
| Cholesterol-lowering Medication | No | 89 |
| Yes | 17 | |
| T Stage | T1 | 22 |
| T2 | 35 | |
| T3 | 5 | |
| T4 | 44 | |
| Lymph Node Metastasis | No | 50 |
| Yes | 56 | |
| Distant Metastasis | No | 104 |
| Yes | 2 | |
| Clinical TNM Stage (8th edition) | I | 35 |
| II | 16 | |
| III | 19 | |
| IV | 1 | |
| IVa | 30 | |
| IVb | 4 | |
| IVc | 1 | |
| Treatment | Surgery alone | 12 |
| Surgery with postoperative radiotherapy | 27 | |
| Surgery with postoperative radiotherapy and chemotherapy | 2 | |
| Radiotherapy alone | 38 | |
| Preoperative radiotherapy and surgery | 15 | |
| Radiotherapy in combination with chemotherapy or pharmacotherapy | 12 | |
| Status | Alive | 76 |
| Dead | 30 | |
| Total | 106 | |
| Clinical Variables | Total Cholesterol | LDL | HDL | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Normal | High | p-Value | Normal | High | p-Value | Normal | Low | p-Value | ||
| Age at diagnosis (years) | 20–40 | 5 | 3 | 0.066 | 6 | 2 | 0.092 | 3 | 5 | 0.302 |
| 41–65 | 25 | 25 | 25 | 21 | 33 | 17 | ||||
| > 65 | 35 | 13 | 36 | 12 | 29 | 19 | ||||
| Gender | Female | 23 | 13 | 0.834 | 26 | 10 | 0.384 | 24 | 12 | 0.528 |
| Male | 42 | 28 | 41 | 25 | 41 | 29 | ||||
| Alcohol | Yes | 49 | 33 | 0.637 | 52 | 26 | 0.807 | 51 | 31 | 0.813 |
| No | 16 | 8 | 15 | 9 | 14 | 10 | ||||
| Smoking | Smoker | 19 | 18 | 0.244 | 23 | 12 | 0.233 | 25 | 12 | 0.558 |
| Previous smoker | 22 | 9 | 23 | 7 | 17 | 14 | ||||
| Non-smoker | 24 | 14 | 21 | 16 | 23 | 15 | ||||
| BMI | Underweight | 3 | 1 | 0.374 | 4 | 0 | 0.351 | 3 | 1 | 0.093 |
| Normal | 32 | 14 | 32 | 14 | 34 | 12 | ||||
| Overweight | 21 | 19 | 23 | 16 | 20 | 20 | ||||
| Obese | 9 | 7 | 8 | 5 | 8 | 8 | ||||
| Cholesterol-lowering medication | No | 50 | 39 | 0.014 | 51 | 34 | 0.005 | 54 | 35 | 1.000 |
| Yes | 15 | 2 | 16 | 1 | 11 | 6 | ||||
| T stage | T1, T2 | 36 | 21 | 0.694 | 39 | 16 | 0.296 | 38 | 19 | 0.237 |
| T3, T4 | 29 | 20 | 28 | 19 | 27 | 22 | ||||
| Lymph node metastasis | Negative | 28 | 22 | 0.322 | 29 | 19 | 0.305 | 32 | 18 | 0.690 |
| Positive | 37 | 19 | 38 | 16 | 33 | 23 | ||||
| Clinical TNM stage | I, II | 33 | 18 | 0.552 | 34 | 16 | 0.680 | 34 | 17 | 0.321 |
| III, IV | 32 | 23 | 33 | 19 | 31 | 24 | ||||
| HPV status | Negative | 42 | 25 | 0.836 | 44 | 20 | 0.518 | 46 | 21 | 0.062 |
| Positive | 23 | 16 | 23 | 15 | 19 | 20 | ||||
| Weight change (kg) | No change | 37 | 27 | 0.454 | 40 | 23 | 0.144 | 41 | 23 | 0.121 |
| Increase of 1–5 | 2 | 2 | 2 | 1 | 2 | 2 | ||||
| Decrease of 1–5 | 12 | 8 | 10 | 9 | 15 | 5 | ||||
| Decrease > 5 | 14 | 4 | 15 | 2 | 7 | 11 | ||||
| Overall survival status | Alive | 42 | 34 | 0.048 | 44 | 31 | 0.017 | 46 | 30 | 0.828 |
| Dead | 23 | 7 | 23 | 4 | 19 | 11 | ||||
| Disease-free status | Disease-free | 44 | 34 | 0.113 | 46 | 31 | 0.030 | 50 | 28 | 0.370 |
| With disease | 21 | 7 | 21 | 4 | 15 | 13 | ||||
| Group | Overall Survival | Disease-Free Survival | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| p-Value | Hazard Ratio | 95% CI for Hazard Ratio | p-Value | Hazard Ratio | 95% CI for Hazard Ratio | |||||
| Lower | Upper | Lower | Upper | |||||||
| Univariate Cox regression analysis | Cholesterol | 0.021 | 0.599 | 0.387 | 0.926 | 0.068 | 0.676 | 0.444 | 1.029 | |
| LDL | 0.006 | 0.514 | 0.319 | 0.827 | 0.015 | 0.551 | 0.341 | 0.890 | ||
| Age | 0.113 | 1.031 | 0.993 | 1.071 | 0.115 | 1.030 | 0.993 | 1.068 | ||
| Gender | 0.559 | 0.763 | 0.308 | 1.891 | 0.355 | 0.664 | 0.278 | 1.583 | ||
| Alcohol | 0.971 | 0.980 | 0.327 | 2.935 | 0.817 | 1.126 | 0.412 | 3.077 | ||
| Smoking | 0.730 | 1.087 | 0.677 | 1.744 | 0.964 | 1.011 | 0.628 | 1.627 | ||
| BMI | 0.080 | 0.901 | 0.801 | 1.013 | 0.073 | 0.907 | 0.816 | 1.009 | ||
| HPV status | 0.568 | 0.757 | 0.291 | 1.971 | 0.300 | 0.606 | 0.235 | 1.563 | ||
| T stage | 0.065 | 1.460 | 0.977 | 2.183 | 0.046 | 1.489 | 1.007 | 2.201 | ||
| Lymph node metastasis | 0.064 | 2.374 | 0.952 | 5.918 | 0.192 | 1.793 | 0.746 | 4.312 | ||
| TNM stage | 0.011 | 1.376 | 1.075 | 1.762 | 0.002 | 1.510 | 1.166 | 1.956 | ||
| Weight change | 0.011 | 0.903 | 0.834 | 0.977 | 0.024 | 0.915 | 0.846 | 0.988 | ||
| Multivariate Cox regression analysis | Independent predictors | Cholesterol | 0.033 | 0.599 | 0.374 | 0.959 | 0.105 | 0.691 | 0.442 | 1.080 |
| TNM stage | 0.021 | 1.355 | 1.047 | 1.755 | 0.004 | 1.488 | 1.138 | 1.944 | ||
| Weight change | 0.088 | 0.931 | 0.858 | 1.011 | 0.232 | 0.951 | 0.875 | 1.033 | ||
| Independent predictors | LDL | 0.005 | 0.451 | 0.259 | 0.787 | 0.013 | 0.501 | 0.290 | 0.867 | |
| TNM stage | 0.034 | 1.357 | 1.024 | 1.800 | 0.006 | 1.494 | 1.122 | 1.991 | ||
| Weight change | 0.046 | 0.916 | 0.841 | 0.998 | 0.154 | 0.941 | 0.865 | 1.023 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wilms, T.; Boldrup, L.; Gu, X.; Coates, P.J.; Sgaramella, N.; Nylander, K. High Levels of Low-Density Lipoproteins Correlate with Improved Survival in Patients with Squamous Cell Carcinoma of the Head and Neck. Biomedicines 2021, 9, 506. https://doi.org/10.3390/biomedicines9050506
Wilms T, Boldrup L, Gu X, Coates PJ, Sgaramella N, Nylander K. High Levels of Low-Density Lipoproteins Correlate with Improved Survival in Patients with Squamous Cell Carcinoma of the Head and Neck. Biomedicines. 2021; 9(5):506. https://doi.org/10.3390/biomedicines9050506
Chicago/Turabian StyleWilms, Torben, Linda Boldrup, Xiaolian Gu, Philip J. Coates, Nicola Sgaramella, and Karin Nylander. 2021. "High Levels of Low-Density Lipoproteins Correlate with Improved Survival in Patients with Squamous Cell Carcinoma of the Head and Neck" Biomedicines 9, no. 5: 506. https://doi.org/10.3390/biomedicines9050506
APA StyleWilms, T., Boldrup, L., Gu, X., Coates, P. J., Sgaramella, N., & Nylander, K. (2021). High Levels of Low-Density Lipoproteins Correlate with Improved Survival in Patients with Squamous Cell Carcinoma of the Head and Neck. Biomedicines, 9(5), 506. https://doi.org/10.3390/biomedicines9050506