
Determinants of Pulmonary Emphysema Severity in Taiwanese Patients with Chronic Obstructive Pulmonary Disease: An Integrated Epigenomic and Air Pollutant Analysis

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Patients
2.2. Inclusion and Exclusion Criteria
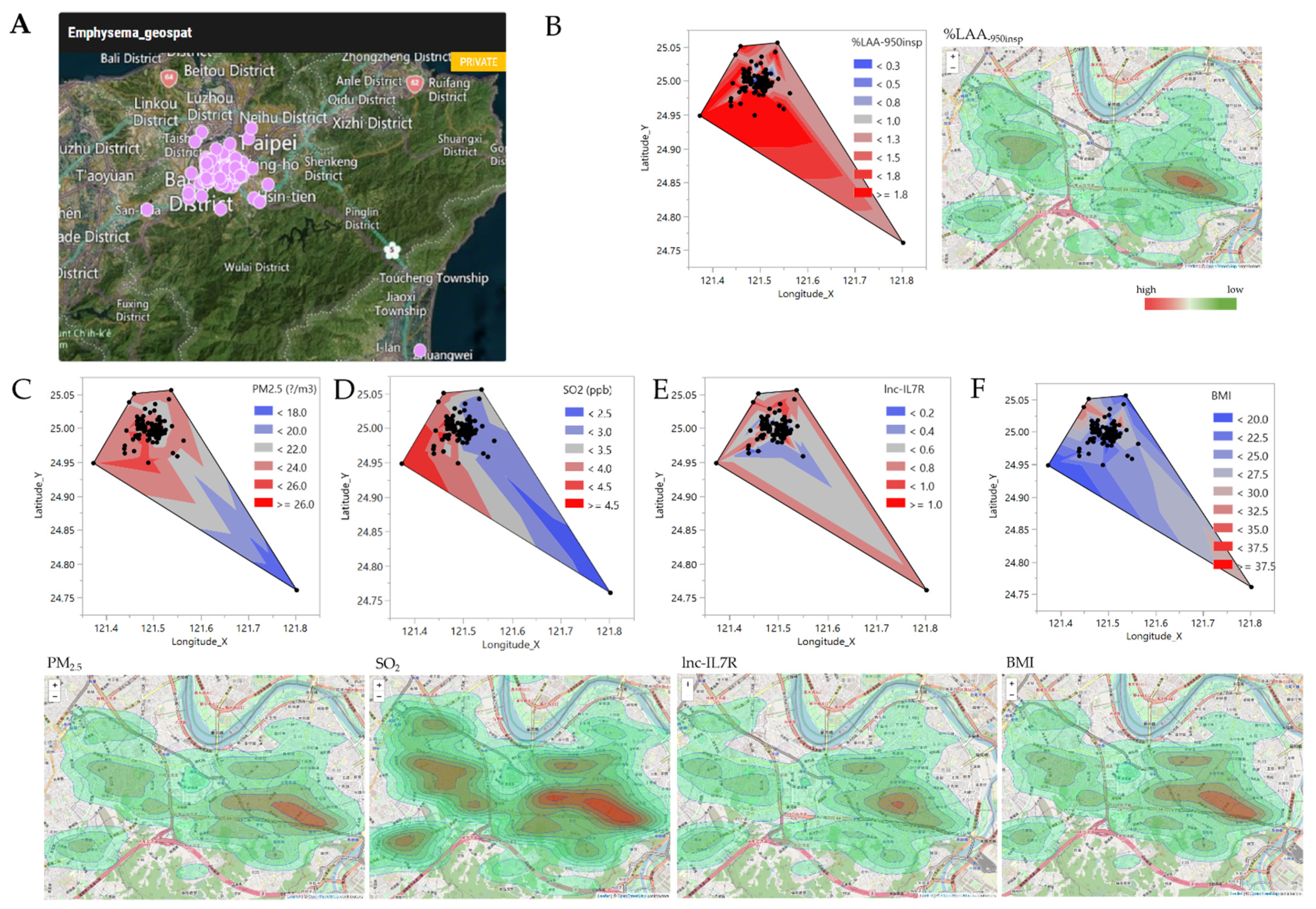
2.3. Geographic Information System (GIS) and Ambient Air Pollutant Exposure
2.4. Sample Preparation and Quantitative Reverse Transcription PCR (RT-qPCR)
2.5. Statistical Analysis
3. Results
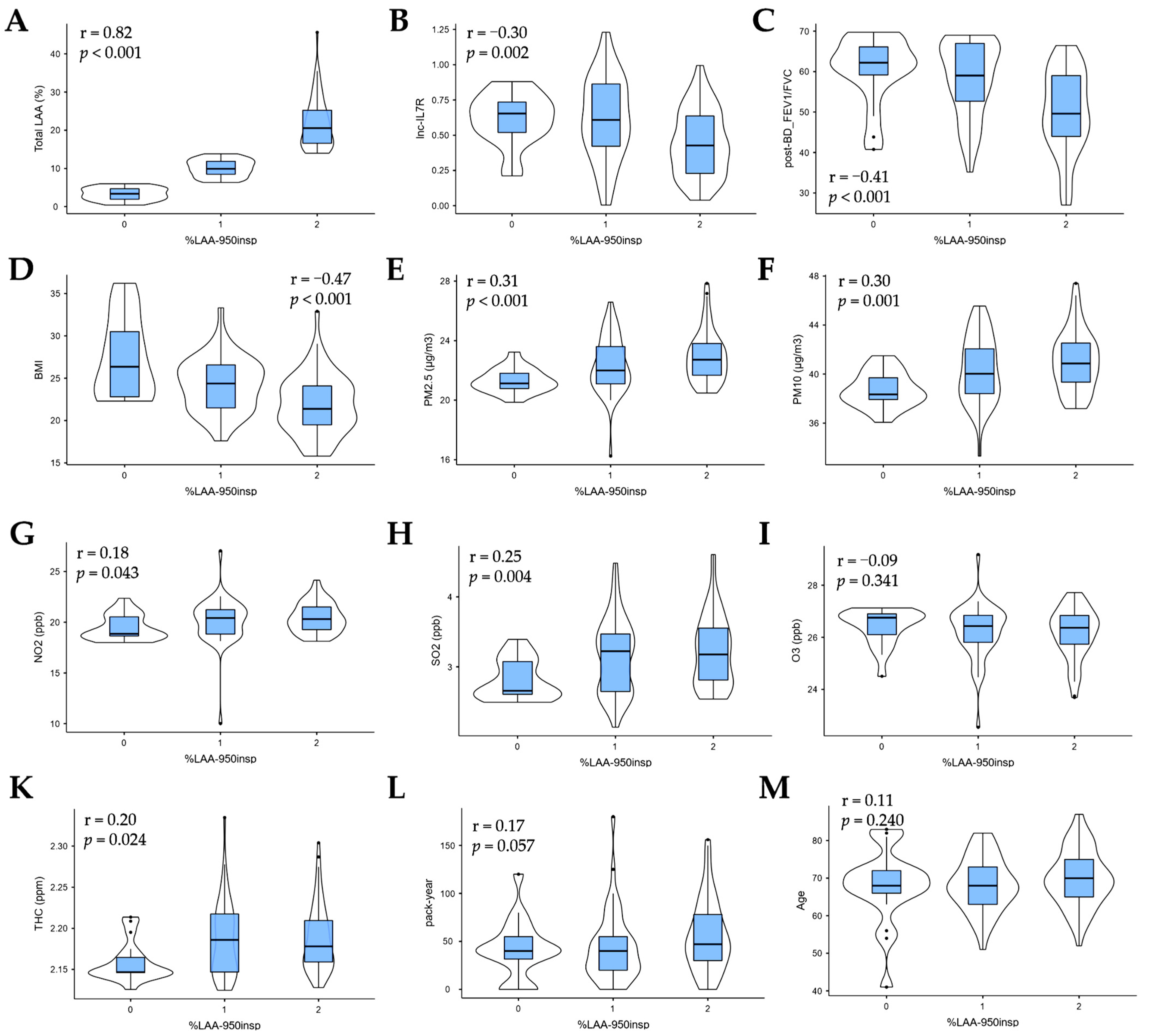
3.1. Emphysema Risk Modulators in Taiwanese Patients with COPD
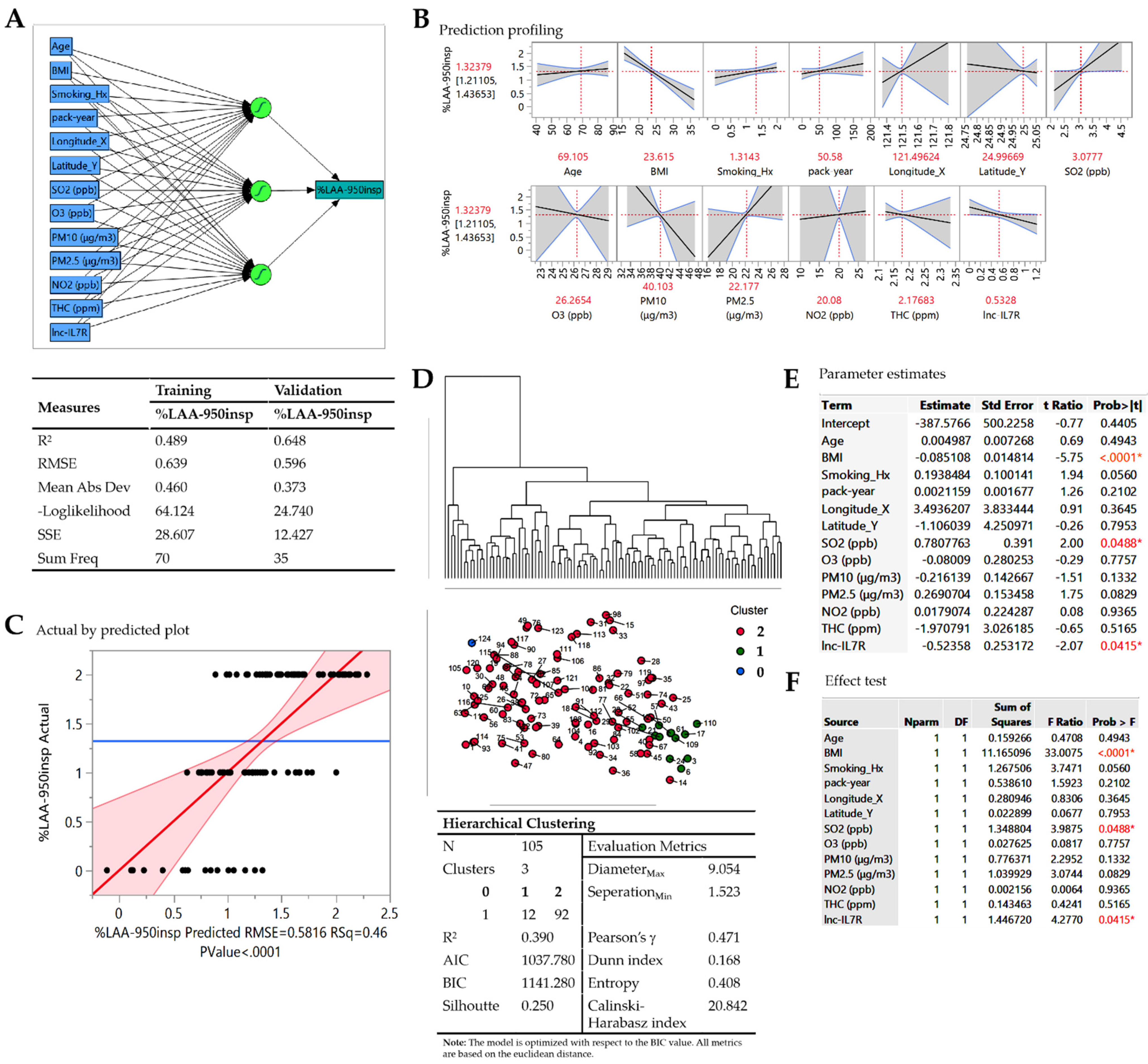
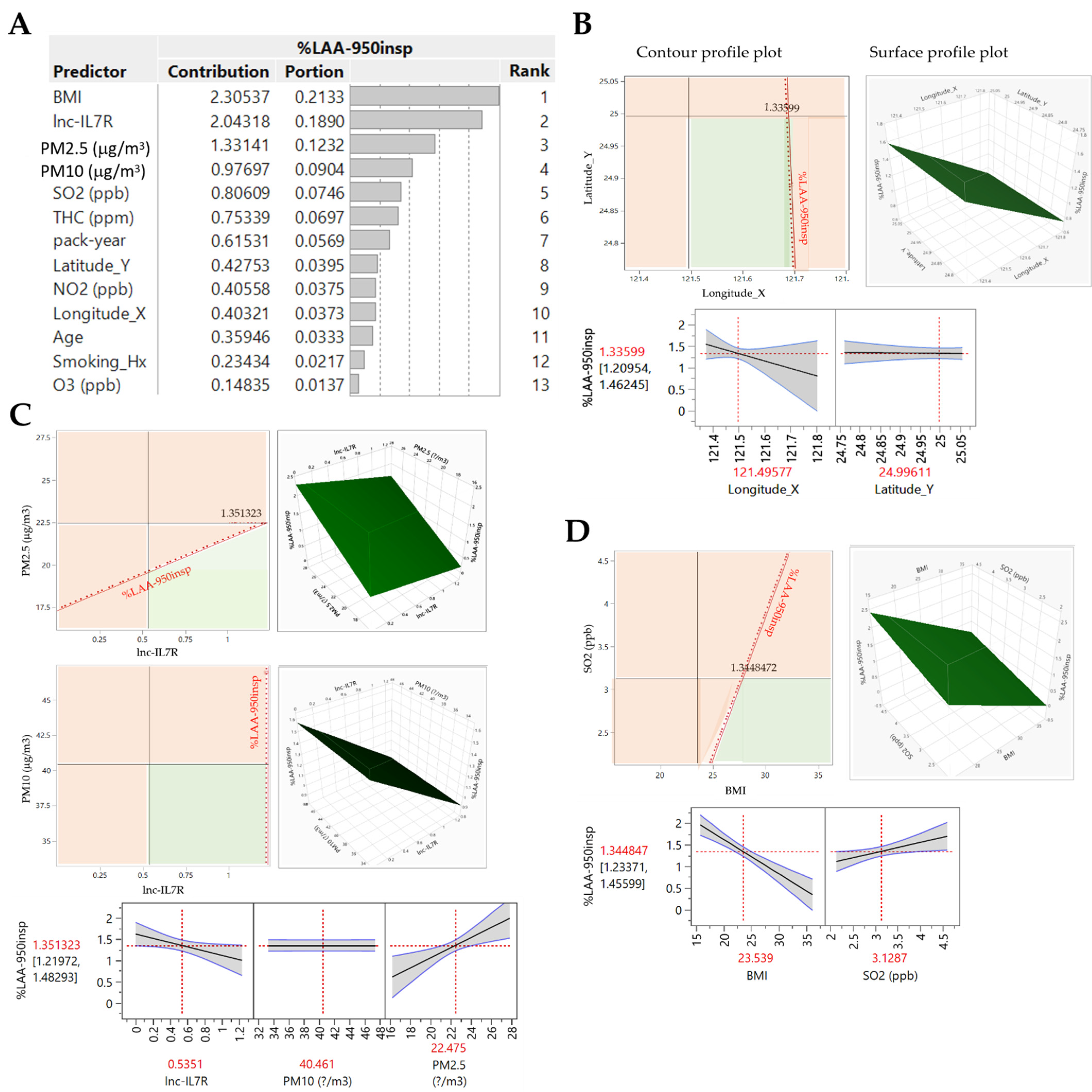
3.2. Delineating Predictors of Disease Severity in Taiwanese Patients with COPD-E
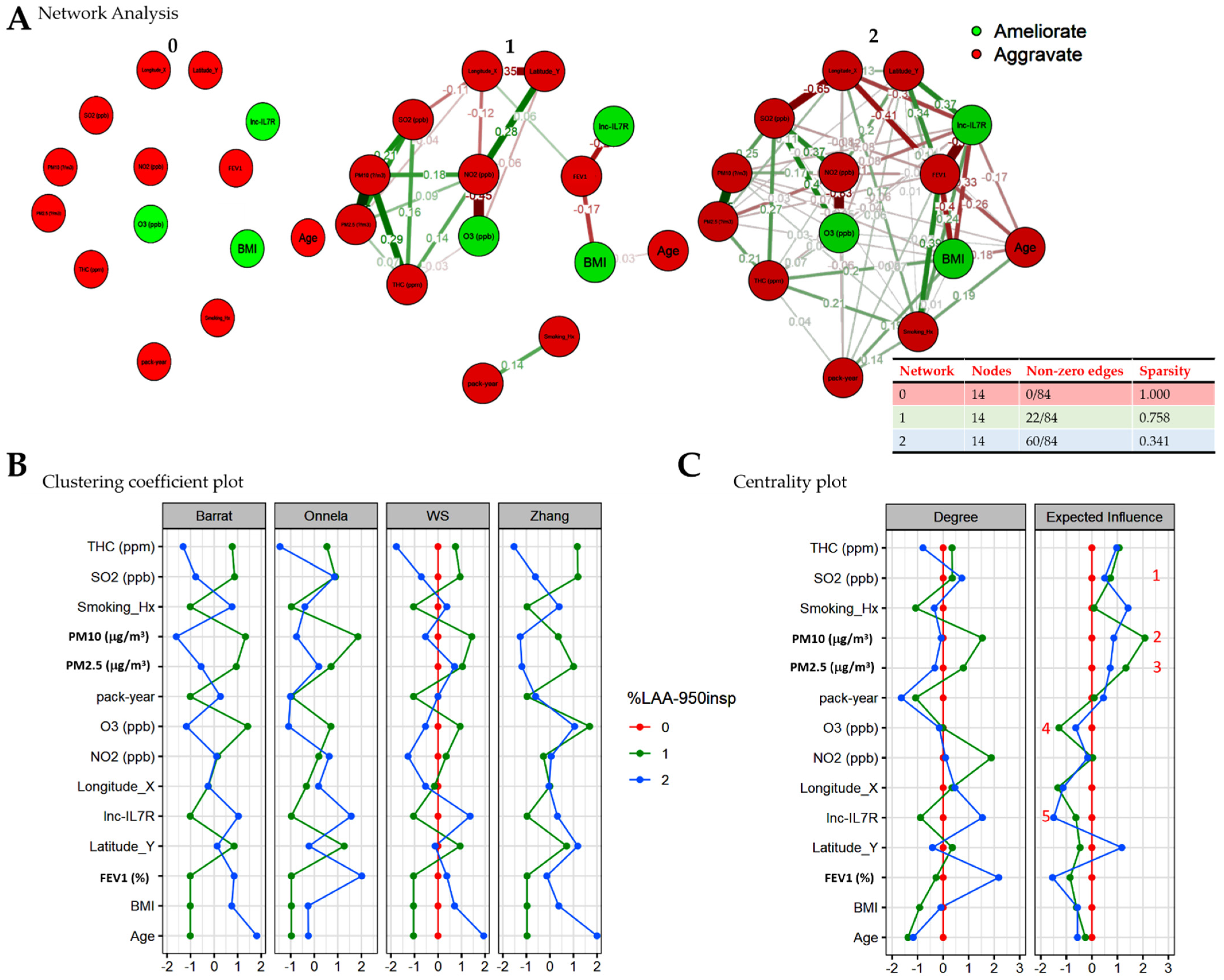
3.3. Severity-Stratified Spatiofunctional Interaction between Individual Predictors of COPD-E
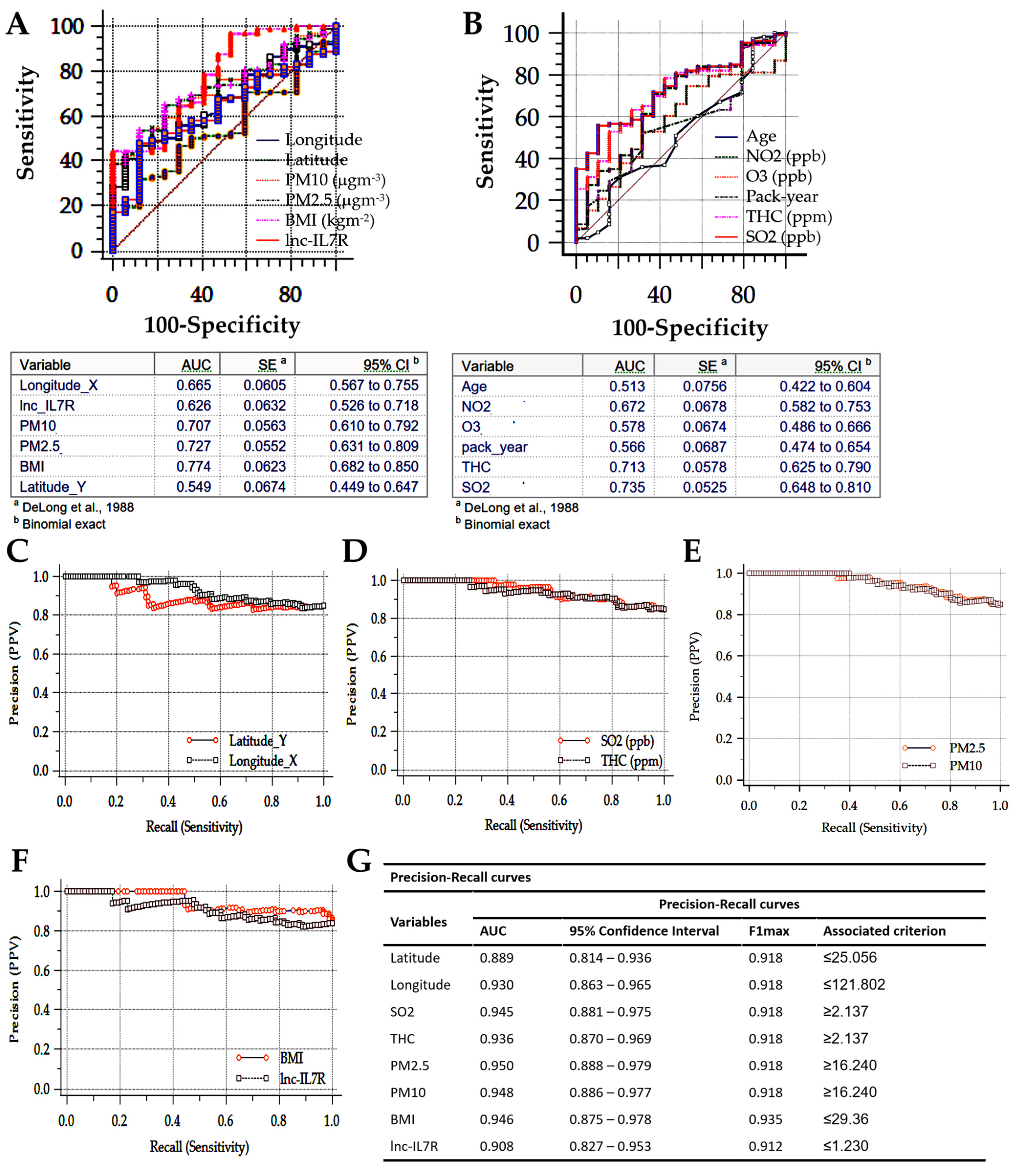
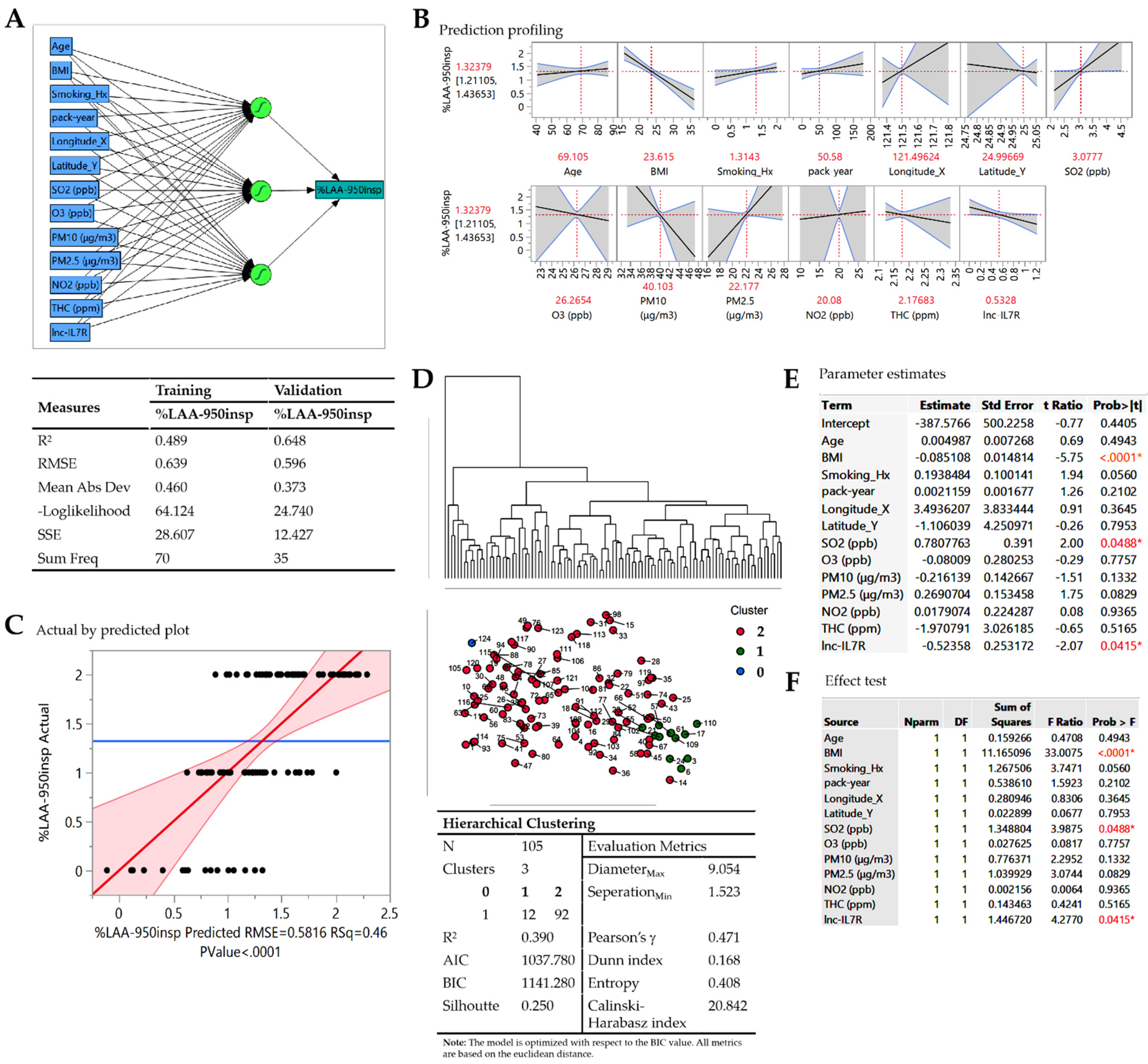
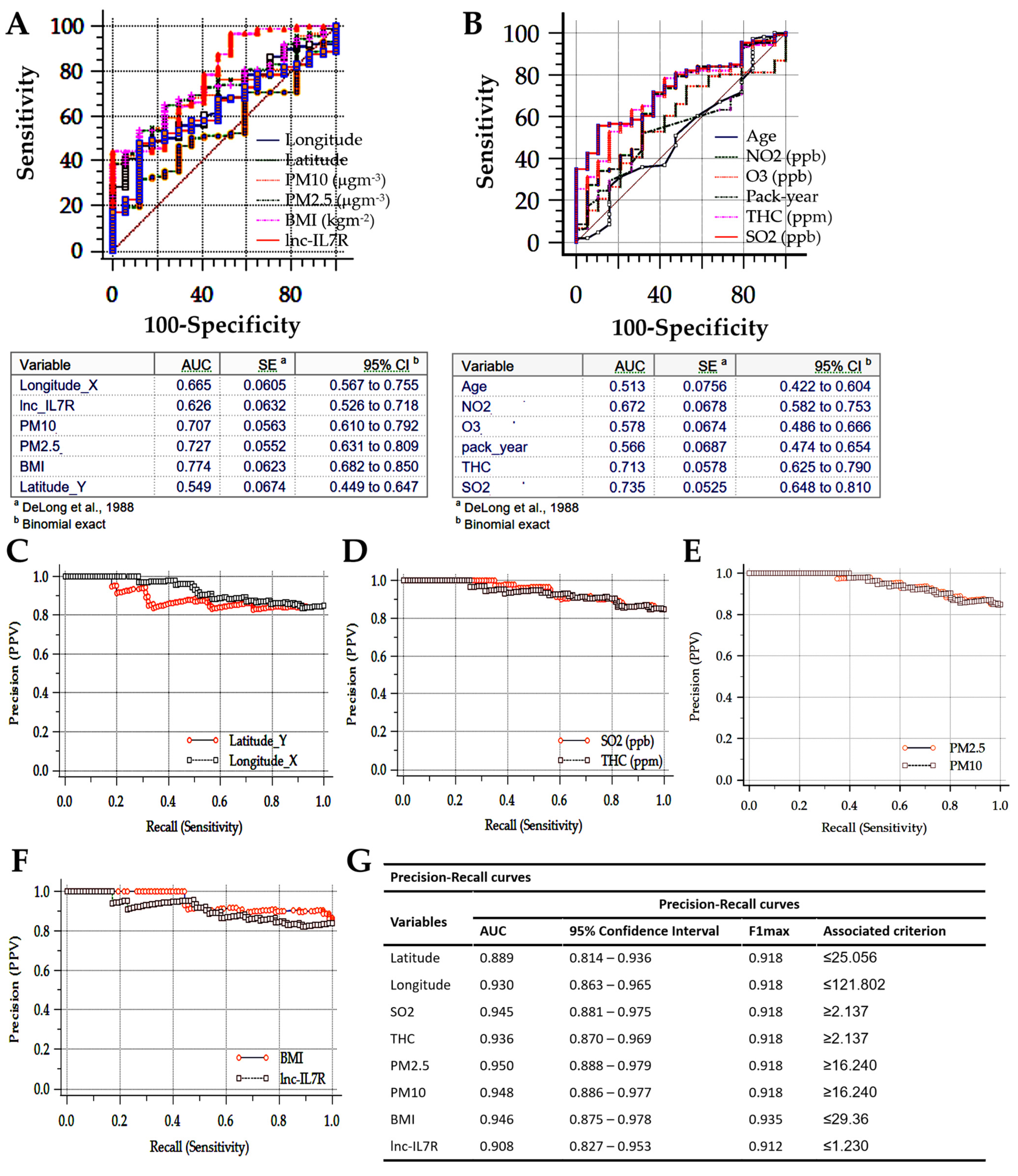
3.4. BMI, lnc-IL7R, PM2.5, PM10, and SO2 Levels Are Excellent Classifiers for Accurate Patient Stratification and COPD-E Management Triage in Taiwan
3.5. BMI, lnc-IL7R, PM2.5, PM10, and SO2 Are Highly Specific Predictors of COPD-E Severity and Disease Progression in New Taipei City
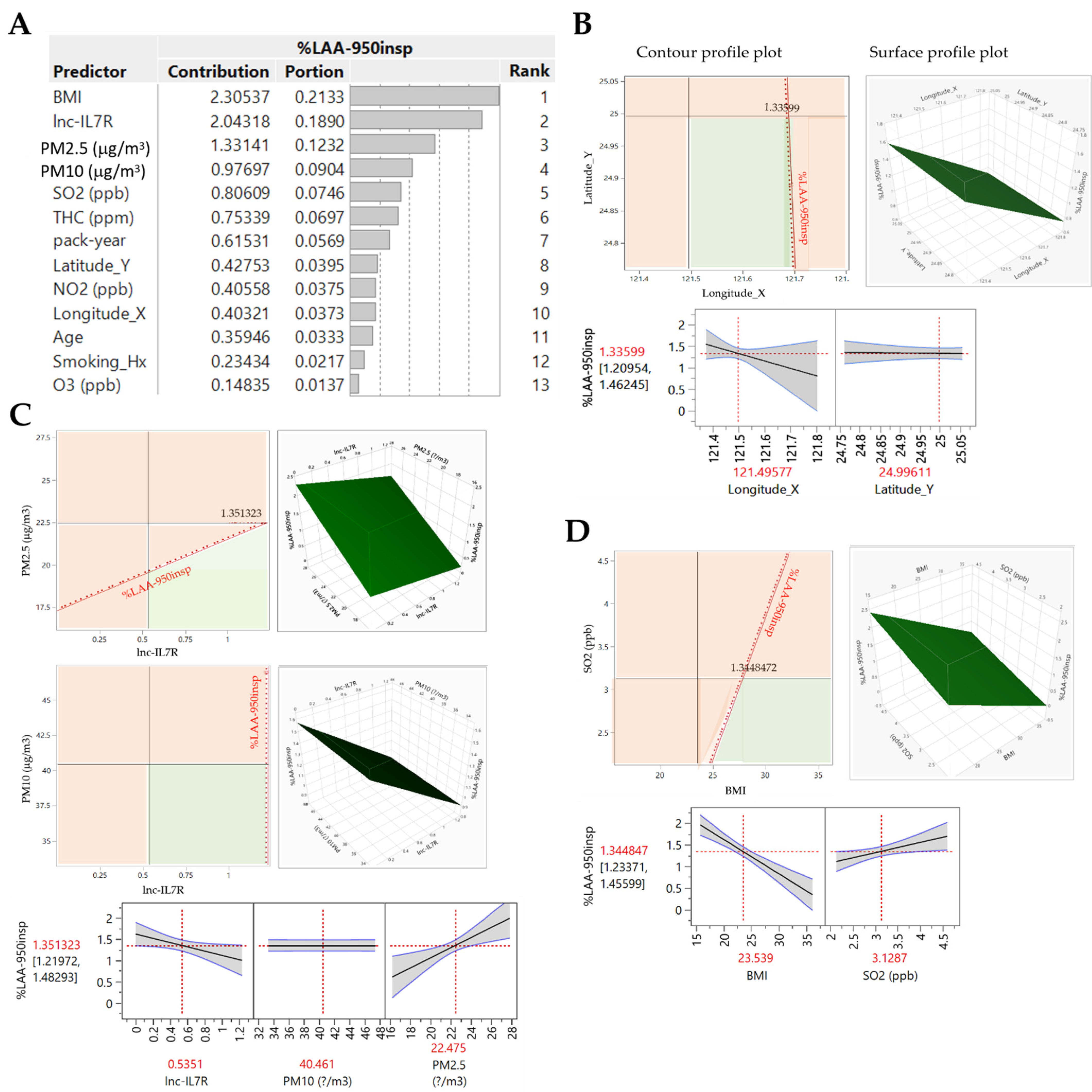
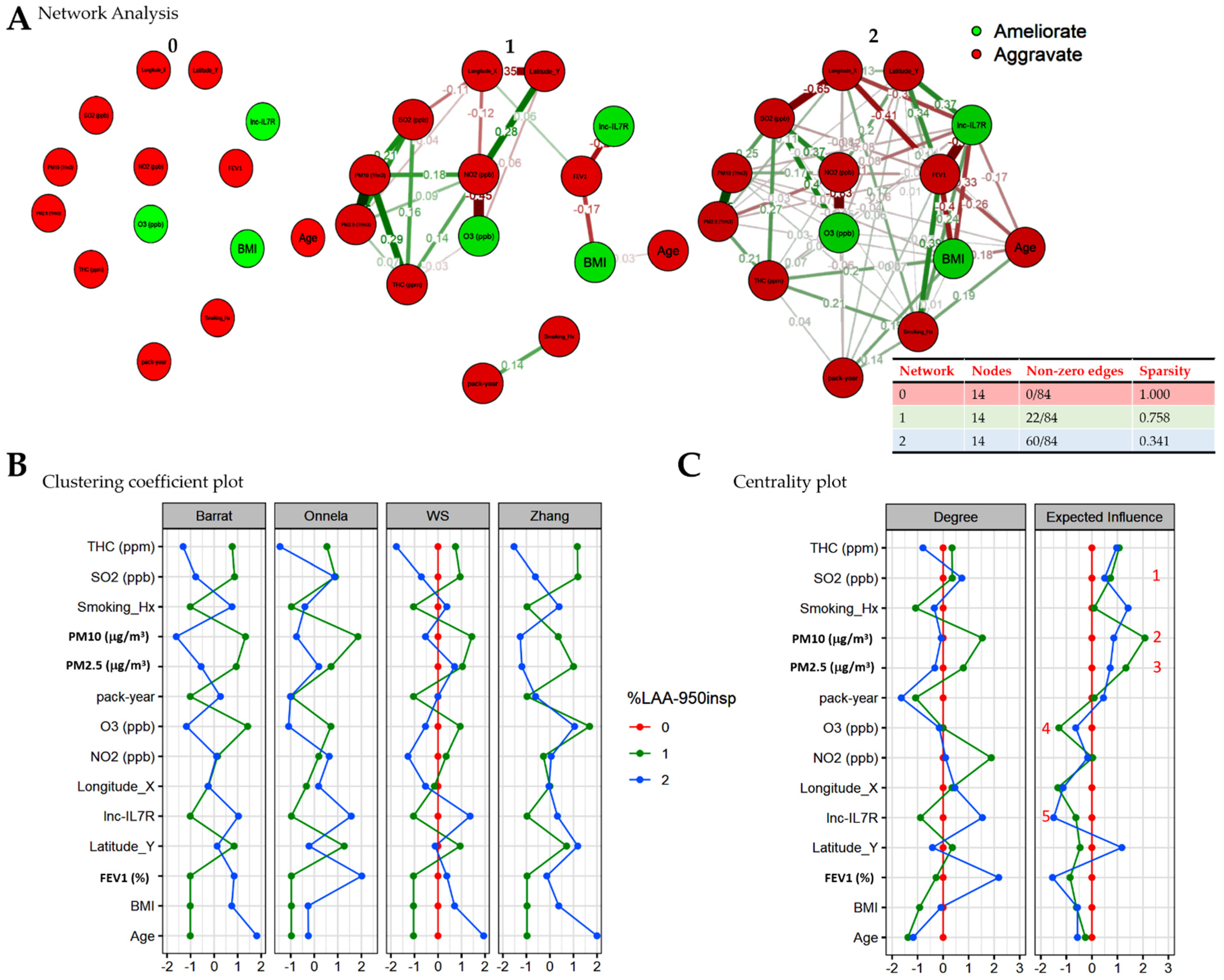
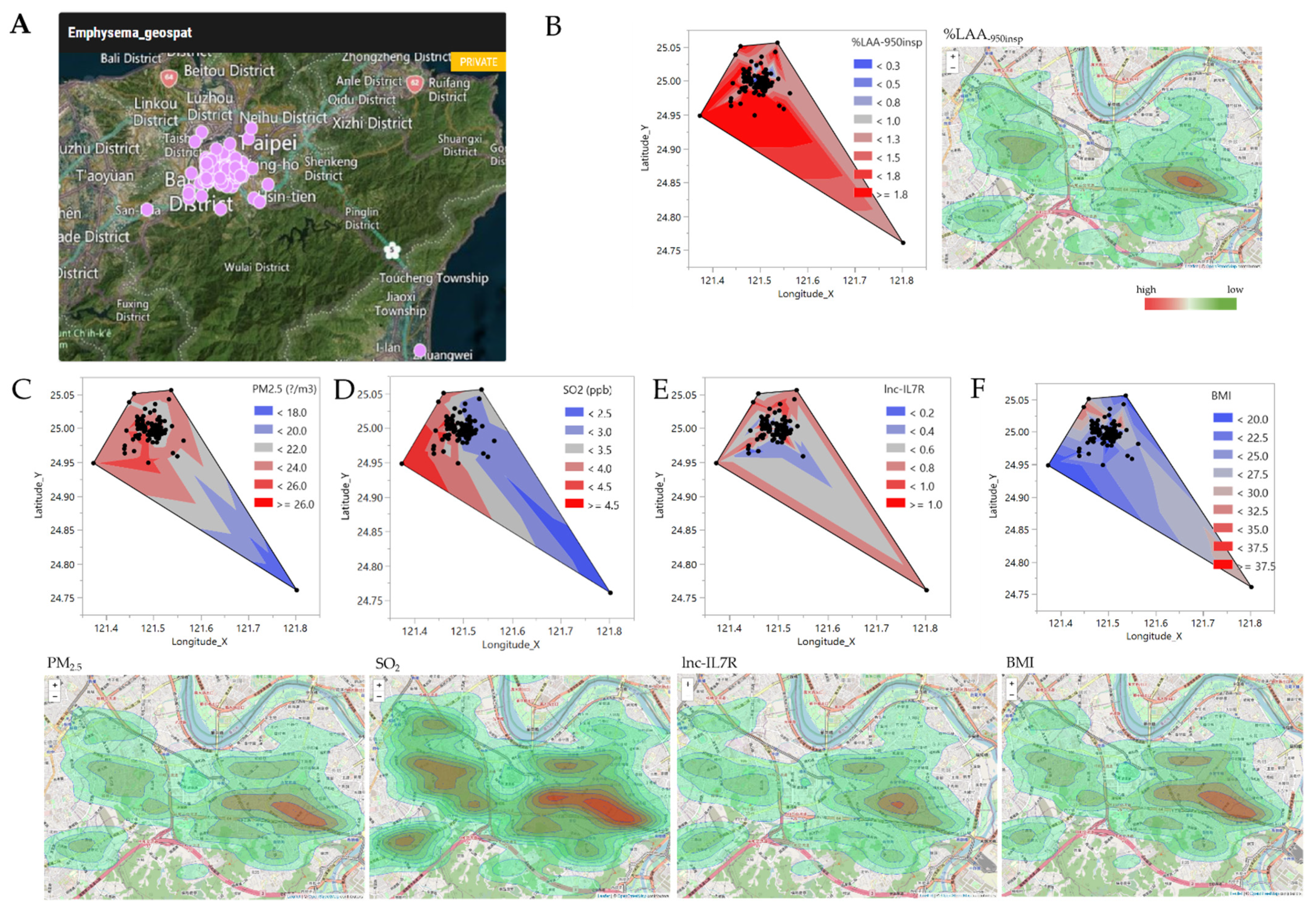
3.6. Low BMI, and lnc-IL7R, with Concomitant High PM2.5, and SO2 Levels Is Pathognomonic of Exacerbated/Severe COPD-E in New Taipei City, Taiwan
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Muneswarao, J.; Verma, A.K.; Hassali, M.A.A. Global initiative for chronic obstructive lung disease (GOLD) 2018 report: Highlighting an incorrect information. Pulm. Pharmacol. Ther. 2018, 49, 10. [Google Scholar] [CrossRef]
- Halpin, D.M.G.; Criner, G.J.; Papi, A.; Singh, D.; Anzueto, A.; Martinez, F.J.; Agusti, A.A.; Vogelmeier, C.F. Global Initiative for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease. The 2020 GOLD Science Committee Report on COVID-19 and Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2021, 203, 24–36. [Google Scholar] [CrossRef]
- Celli, B.R.; Locantore, N.; Tal-Singer, R.; Riley, J.; Miller, B.; Vestbo, J.; Yates, J.C.; Silverman, E.K.; Owen, C.A.; Divo, M.; et al. ECLIPSE Study Investigators. Emphysema and extrapulmonary tissue loss in COPD: A multi-organ loss of tissue phenotype. Eur. Respir. J. 2018, 51, 1702146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, P.L.; Herth, F.J.; van Geffen, W.H.; Deslee, G.; Slebos, D.J. Lung volume reduction for emphysema. Lancet Respir. Med. 2017, 5, 147–156. [Google Scholar] [CrossRef]
- Global Initiative for Chronic Obstructive Lung Disease Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease Global Initiative for Chronic Obstructive Lung Disease; 2020 [Updated 4 November 2020]. Available online: http://www.goldcopd.org/ (accessed on 12 December 2020).
- Guo, C.; Zhang, Z.; Lau, A.K.H.; Lin, C.Q.; Chuang, Y.C.; Chan, J.; Jiang, W.K.; Tam, T.; Yeoh, E.K.; Chan, T.C.; et al. Effect of long-term exposure to fine particulate matter on lung function decline and risk of chronic obstructive pulmonary disease in Taiwan: A longitudinal, cohort study. Lancet Planet. Health 2018, 2, e114–e125. [Google Scholar] [CrossRef]
- Wang, M.; Aaron, C.P.; Madrigano, J.; Hoffman, E.A.; Angelini, E.; Yang, J.; Laine, A.; Vetterli, T.M.; Kinney, P.L.; Sampson, P.D.; et al. Association between Long-term Exposure to Ambient Air Pollution and Change in Quantitatively Assessed Emphysema and Lung Function. JAMA 2019, 322, 546–556. [Google Scholar] [CrossRef]
- Yang, X.; Zhang, T.; Zhang, Y.; Chen, H.; Sang, S. Global burden of COPD attributable to ambient PM2.5 in 204 countries and territories, 1990 to 2019: A systematic analysis for the Global Burden of Disease Study 2019. Sci. Total Environ. 2021, 796, 148819. [Google Scholar] [CrossRef]
- Agusti, A.; Calverley, P.M.; Celli, B.; Coxson, H.O.; Edwards, L.D.; Lomas, D.A.; MacNee, W.; Miller, B.E.; Rennard, S.; Silverman, E.K.; et al. Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) investigators. Characterisation of COPD heterogeneity in the ECLIPSE cohort. Respir. Res. 2010, 11, 122. [Google Scholar] [CrossRef]
- Barnes, P.J. Chapter 47—Genomics in the Evaluation and Management of Chronic Obstructive Pulmonary Disease. In Essentials of Genomic and Personalized Medicine; Ginsburg, G.S., Willard, H.F., Eds.; Academic Press: Cambridge, MA, USA, 2010; pp. 603–615. [Google Scholar] [CrossRef]
- Wu, D.D.; Song, J.; Bartel, S.; Krauss-Etschmann, S.; Rots, M.G.; Hylkema, M.N. The potential for targeted rewriting of epigenetic marks in COPD as a new therapeutic approach. Pharmacol. Ther. 2018, 182, 1–14. [Google Scholar] [CrossRef]
- Ruvuna, L.; Sood, A. Epidemiology of Chronic Obstructive Pulmonary Disease. Clin. Chest Med. 2020, 41, 315–327. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.C.; Sin, D.D.; Bourbeau, J.; Hernandez, P.; Chapman, K.R.; Cowie, R.; FitzGerald, J.M.; Marciniuk, D.D.; Maltais, F.; Buist, A.S.; et al. Characteristics of COPD in never-smokers and ever-smokers in the general population: Results from the CanCOLD study. Thorax 2015, 70, 822–829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schamberger, A.C.; Mise, N.; Meiners, S.; Eickelberg, O. Epigenetic mechanisms in COPD: Implications for pathogenesis and drug discovery. Expert Opin. Drug Discov. 2014, 9, 609–628. [Google Scholar] [CrossRef] [PubMed]
- Zeng, H.; Li, T.; He, X.; Cai, S.; Luo, H.; Chen, P.; Chen, Y. Oxidative stress mediates the apoptosis and epigenetic modification of the Bcl-2 promoter via DNMT1 in a cigarette smoke-induced emphysema model. Respir. Res. 2020, 21, 229. [Google Scholar] [CrossRef]
- Wu, S.M.; Feng, P.H.; Chuang, H.C.; Ho, S.C.; Fan, C.K.; Chen, K.Y.; Wu, G.S.; Chen, T.T.; Tseng, C.H.; Liu, W.T.; et al. Impaired lnc-IL7R modulatory mechanism of Toll-like receptors is associated with an exacerbator phenotype of chronic obstructive pulmonary disease. FASEB J. 2020, 34, 13317–13332. [Google Scholar] [CrossRef]
- Occhipinti, M.; Paoletti, M.; Bartholmai, B.J.; Rajagopalan, S.; Karwoski, R.A.; Nardi, C.; Inchingolo, R.; Larici, A.R.; Camiciottoli, G.; Lavorini, F.; et al. Spirometric assessment of emphysema presence and severity as measured by quantitative CT and CT-based radiomics in COPD. Respir. Res. 2019, 20, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, T.T.; Wu, S.M.; Ho, S.C.; Chuang, H.C.; Liu, C.Y.; Chan, Y.F.; Kuo, L.W.; Feng, P.H.; Liu, W.T.; Chen, K.Y.; et al. SUV39H1 Reduction Is Implicated in Abnormal Inflammation in COPD. Sci. Rep. 2017, 7, 46667. [Google Scholar] [CrossRef] [PubMed]
- Masuda, N.; Sakaki, M.; Ezaki, T.; Watanabe, T. Clustering Coefficients for Correlation Networks. Front. Neuroinform. 2018, 12, 7. [Google Scholar] [CrossRef]
- Clemente, G.P.; Grassi, R. Directed clustering in weighted networks: A new perspective. Chaos Soliton Fract. 2018, 107, 26–38. [Google Scholar] [CrossRef] [Green Version]
- Pepelyshev, A. The Role of the Nugget Term in the Gaussian Process Method. In mODa 9—Advances in Model-Oriented Design and Analysis. Contributions to Statistics; Giovagnoli, A., Atkinson, A., Torsney, B., May, C., Eds.; Physica HD: Geneva, Switzerland, 2010. [Google Scholar] [CrossRef] [Green Version]
- Li, K.; Jacob, D.J.; Liao, H.; Shen, L.; Zhang, Q.; Bates, K.H. Anthropogenic drivers of 2013–2017 trends in summer surface ozone in China. Proc. Natl. Acad. Sci. USA 2019, 116, 422–427. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.J.; Wei, Y.; Fang, Z. Ozone Pollution: A Major Health Hazard Worldwide. Front. Immunol. 2019, 10, 2518. [Google Scholar] [CrossRef] [Green Version]
- Hernández, A.; Viñals, M.; Isidoro, T.; Vilás, F. Potential Role of Oxygen-Ozone Therapy in Treatment of COVID-19 Pneumonia. Am. J. Case Rep. 2020, 21, e925849. [Google Scholar] [CrossRef]
- Celli, B.R.; Cote, C.G.; Marin, J.M.; Casanova, C.; Montes de Oca, M.; Mendez, R.A.; Pinto Plata, V.; Cabral, H.J. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N. Engl. J. Med. 2004, 350, 1005–1012. [Google Scholar] [CrossRef] [Green Version]
- Vestbo, J.; Hurd, S.S.; Agustí, A.G.; Jones, P.W.; Vogelmeier, C.; Anzueto, A.; Barnes, P.J.; Fabbri, L.M.; Martinez, F.J.; Nishimura, M.; et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am. J. Respir. Crit. Care Med. 2013, 187, 347–365. [Google Scholar] [CrossRef]
- Rennard, S.I.; Locantore, N.; Delafont, B.; Tal-Singer, R.; Silverman, E.K.; Vestbo, J.; Miller, B.E.; Bakke, P.; Celli, B.; Calverley, P.M.; et al. Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints. Identification of five chronic obstructive pulmonary disease subgroups with different prognoses in the ECLIPSE cohort using cluster analysis. Ann. Am. Thorac. Soc. 2015, 12, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.U.; Lee, J.H.; Kim, J.S.; Hwang, Y.I.; Kim, T.H.; Lim, S.Y.; Yoo, K.H.; Jung, K.S.; Kim, Y.K.; Rhee, C.K. Comparison of World Health Organization and Asia-Pacific body mass index classifications in COPD patients. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 2465–2475. [Google Scholar] [CrossRef] [Green Version]
- Wei, Y.F.; Tsai, Y.H.; Wang, C.C.; Kuo, P.H. Impact of overweight and obesity on acute exacerbations of COPD—Subgroup analysis of the Taiwan Obstructive Lung Disease cohort. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 2723–2729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Y.; Milne, S.; Jaw, J.E.; Yang, C.X.; Xu, F.; Li, X.; Obeidat, M.; Sin, D.D. BMI is associated with FEV1 decline in chronic obstructive pulmonary disease: A meta-analysis of clinical trials. Respir. Res. 2019, 20, 236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devadoss, D.; Long, C.; Langley, R.J.; Manevski, M.; Nair, M.; Campos, M.A.; Borchert, G.; Rahman, I.; Chand, H.S. Long Noncoding Transcriptome in Chronic Obstructive Pulmonary Disease. Am. J. Respir. Cell Mol. Biol. 2019, 61, 678–688. [Google Scholar] [CrossRef] [PubMed]
- Vogel, C.F.A.; Van Winkle, L.S.; Esser, C.; Haarmann-Stemmann, T. The aryl hydrocarbon receptor as a target of environmental stressors—Implications for pollution mediated stress and inflammatory responses. Redox Biol. 2020, 34, 101530. [Google Scholar] [CrossRef]
- Zemans, R.L.; Jacobson, S.; Keene, J.; Kechris, K.; Miller, B.E.; Tal-Singer, R.; Bowler, R.P. Multiple biomarkers predict disease severity, progression and mortality in COPD. Respir. Res. 2017, 18, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schikowski, T.; Mills, I.C.; Anderson, H.R.; Cohen, A.; Hansell, A.; Kauffmann, F.; Krämer, U.; Marcon, A.; Perez, L.; Sunyer, J.; et al. Ambient air pollution: A cause of COPD? Eur. Respir. J. 2014, 43, 250–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, S.O.; Hong, S.H.; Han, Y.J.; Bak, S.H.; Kim, J.; Lee, M.K.; London, S.J.; Kim, W.J.; Kim, S.Y. Long-term exposure to PM10 and NO2 in relation to lung function and imaging phenotypes in a COPD cohort. Respir. Res. 2020, 21, 247. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Healthy Controls (n = 43) | Patients with COPD (GOLD Stage, n = 125) | ||||
|---|---|---|---|---|---|---|
| Non-Smoker (n = 21) | Smoker (n = 22) | I (n = 18) | II (n = 58) | III (n = 38) | IV (n = 11) | |
| Age (years) | ||||||
| Mean ± SD (Min-Max) | 68.33 ± 7.02 (50.00–80.00) | 67.45 ± 6.75 (47.00–80.00) | 69.39 ± 5.78 (61.00–80.00) | 67.97 ± 8.91 (41.00–9.00) | 71.24 ± 6.95 (56.00–80.00) | 67.09 ± 5.38 (61.00–79.00) |
| Median (IQR) | 69.00 (67.00–73.00) | 69.00 (65.25–71.00) | 68.00 (65.25–71.50) | 68.50 (62.25–73.00) | 70.50 (67.00–77.25) | 66.00 (63.00–69.00) |
| Sex, n (%) | ||||||
| Male | 8 (38.10) | 17 (77.27) | 17 (94.44) | 55 (94.83) | 31 (81.58) | 9 (81.82) |
| Female | 13 (61.90) | 5 (22.73) | 1 (5.56) | 3 (5.17) | 7 (18.42) | 2 (18.18) |
| BMI, kg∙m−2 | ||||||
| Mean ± SD (Min-Max) | 22.79 ± 2.15 (20.50–28.80) | 23.14 ± 2.58 (19.11–29.20) | 24.05 ± 3.12 (19.10–29.36) | 24.33 ± 4.41 (16.40–34.80) | 22.50 ± 3.77 (15.80–36.20) | 21.31 ± 3.60 (16.20–27.70) |
| Median (IQR) | 22.00 (21.20–24.00) | 22.76 (21.85–23.95) | 23.90 (21.63–26.29) | 24.14 (21.16–26.60) | 22.30 (20.00–24.50) | 20.60 (19.90–22.98) |
| Tobacco Smoking, n (%) | ||||||
| Current smoker | 0 (0.00) | 13 (59.09) | 5 (27.78) | 31 (53.44) | 11 (28.95) | 2 (18.18) |
| Ex-smoker | 0 (0.00) | 9 (40.91) | 13 (72.22) | 23 (39.66) | 22 (57.89) | 8 (72.73) |
| Never-smoker | 100 (100) | 0 (0.00) | 0 (0.00) | 4 (6.90) | 5 (13.16) | 1 (9.09) |
| Smoking pack-years | ||||||
| Mean ± SD (Min-Max) | 0 (0.00–0.00) | 65.00 ± 31.43 (30.00–145.00) | 48.89 ± 35.19 (5.00–150.00) | 49.02 ± 36.34 (0.00–180.00) | 49.30 ± 35.66 (0.00–156.00) | 56.73 ± 37.65 (0.00–123.00) |
| Median (IQR) | 0 (0.00–0.00) | 57.00 (40.00–79.50) | 42.50 (20.50–60.00) | 40.00 (23.00–60.00) | 40.00 (25.00–75.00) | 46.00 (35.00–85.00) |
| Pulmonary function indices | ||||||
| FEV1 (L) Mean ± SD (Min-Max) | 1.98 ± 0.37 (1.26–2.76) | 2.18 ± 0.42 (1.74–3.47) | 1.95 ± 0.26 (1.55–2.56) | 1.67 ± 0.40 (1.01–3.07) | 0.98 ± 0.25 (0.61–1.51) | 0.61 ± 0.13 (0.43–0.87) |
| Median (IQR) | 1.97 (1.80–2.06) | 2.09 (1.90–2.29) | 1.90 (1.74–2.11) | 1.61 b’ (1.38–1.90 | 0.99 a’b’c’d’ (0.74–1.12) | 0.58 a’b’c’d’ (0.52–0.66) |
| FEV1 % Mean ± SD (Min-Max) | 101.43 ± 5.10 (95.00–117.00) | 98.60 ± 6.68 (90.00–111.00) | 85.42 ± 5.24 (80.00–97.70) | 63.81 ± 8.57 (50.00–79.00) | 40.01 ± 5.71 (32.00–49.80) | 24.85 ± 3.98 (17.50–29.90) |
| Median (IQR) | 101.00 (98.00–103.00) | 96.85 (93.00–103.00) | 84.55 (81.3–86.68) | 65.00 a’b’c (57.38–72.00) | 39.05 a’b’c’d’ (35.00–45.00) | 25.00 a’b’c’d’ (22.10–27.95) |
| FEV1/FVC % Mean ± SD (Min-Max) | 100.76 ± 9.42 (80.00–125.00) | 100.45 ± 8.01 (90.00–120.00) | 63.49 ± 4.05 (54.64–68.26) | 59.33 ± 6.86 (45.00–69.72) | 47.93 ± 8.60 (28.00–65.00) | 38.84 ± 8.41 (27.00–49.61) |
| Median (IQR) | 100.00 (98.00–105.00) | 98.00 (95.25–107.75) | 63.68 (61.25–66.87) | 59.25 a’b’ (54.12–65.50) | 46.50 a’b’c’d’ (42.11–55.25) | 41.41 a’b’c’d’ (30.93–45.67) |
| Emphysema severity | ||||||
| Null/Mild (%) | 66.67 | 19.05 | 0.00 | 0.00 | ||
| Moderate (%) | 33.33 | 66.67 | 69.23 | 20.00 | ||
| Severe (%) | 0.00 | 14.28 | 30.77 | 80.00 | ||
| Column | Theta | Total Sensitivity | Main Effect | lnc-IL7R Interaction | PM10 Interaction | PM2.5 Interaction |
|---|---|---|---|---|---|---|
| lnc-IL7R | 0.0003 | 0.1667 | 0.1667 | - | 0 | 5.35 × 10−9 |
| PM10 | 4.82 × 10−9 | 0 | 0 | 0 | - | 0 |
| PM2.5 | 1.70 × 10−9 | 0.8333 | 0.8333 | 5.35 × 10−9 | 0 | - |
| μ | σ2 | Nugget | ||||
| 1.3155 | 470.0283 | 0.001 | ||||
| −2*Loglikelihood | ||||||
| 240.6087 | ||||||
| Column | Theta | Total Sensitivity | Main Effect | Longitude Interaction | Latitude Interaction |
|---|---|---|---|---|---|
| Longitude | 0.0046 | 0.9986 | 0.9986 | - | 0 |
| Latitude | 0.0003 | 0.0014 | 0.0014 | 0 | - |
| μ | σ2 | Nugget | |||
| 1.4838 | 520.33 | 0.001 | |||
| −2*Loglikelihood | |||||
| 285.8087 | |||||
| Column | Theta | Total Sensitivity | Main Effect | BMI Interaction | SO2 Interaction |
|---|---|---|---|---|---|
| BMI | 8.21 × 10−6 | 0.6833 | 0.6833 | - | 2.74 × 10−7 |
| SO2 | 8.75 × 10−5 | 0.3167 | 0.3167 | 2.74 × 10−7 | - |
| μ | σ2 | Nugget | |||
| 1.1118 | 390.41 | 0.001 | |||
| −2*Loglikelihood | |||||
| 248.4064 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, S.-M.; Sun, W.-L.; Lee, K.-Y.; Lin, C.-W.; Feng, P.-H.; Chuang, H.-C.; Ho, S.-C.; Chen, K.-Y.; Chen, T.-T.; Liu, W.-T.; et al. Determinants of Pulmonary Emphysema Severity in Taiwanese Patients with Chronic Obstructive Pulmonary Disease: An Integrated Epigenomic and Air Pollutant Analysis. Biomedicines 2021, 9, 1833. https://doi.org/10.3390/biomedicines9121833
Wu S-M, Sun W-L, Lee K-Y, Lin C-W, Feng P-H, Chuang H-C, Ho S-C, Chen K-Y, Chen T-T, Liu W-T, et al. Determinants of Pulmonary Emphysema Severity in Taiwanese Patients with Chronic Obstructive Pulmonary Disease: An Integrated Epigenomic and Air Pollutant Analysis. Biomedicines. 2021; 9(12):1833. https://doi.org/10.3390/biomedicines9121833
Chicago/Turabian StyleWu, Sheng-Ming, Wei-Lun Sun, Kang-Yun Lee, Cheng-Wei Lin, Po-Hao Feng, Hsiao-Chi Chuang, Shu-Chuan Ho, Kuan-Yuan Chen, Tzu-Tao Chen, Wen-Te Liu, and et al. 2021. "Determinants of Pulmonary Emphysema Severity in Taiwanese Patients with Chronic Obstructive Pulmonary Disease: An Integrated Epigenomic and Air Pollutant Analysis" Biomedicines 9, no. 12: 1833. https://doi.org/10.3390/biomedicines9121833
APA StyleWu, S.-M., Sun, W.-L., Lee, K.-Y., Lin, C.-W., Feng, P.-H., Chuang, H.-C., Ho, S.-C., Chen, K.-Y., Chen, T.-T., Liu, W.-T., Tseng, C.-H., & Bamodu, O. A. (2021). Determinants of Pulmonary Emphysema Severity in Taiwanese Patients with Chronic Obstructive Pulmonary Disease: An Integrated Epigenomic and Air Pollutant Analysis. Biomedicines, 9(12), 1833. https://doi.org/10.3390/biomedicines9121833