
Network Analysis Integrating microRNA Expression Profiling with MRI Biomarkers and Clinical Data for Prostate Cancer Early Detection: A Proof of Concept Study

 , , , ,
, , , ,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Imaging and Targeted Biopsy Protocols
2.3. Sample Collection and miRNA Profiling
2.4. Network Analysis
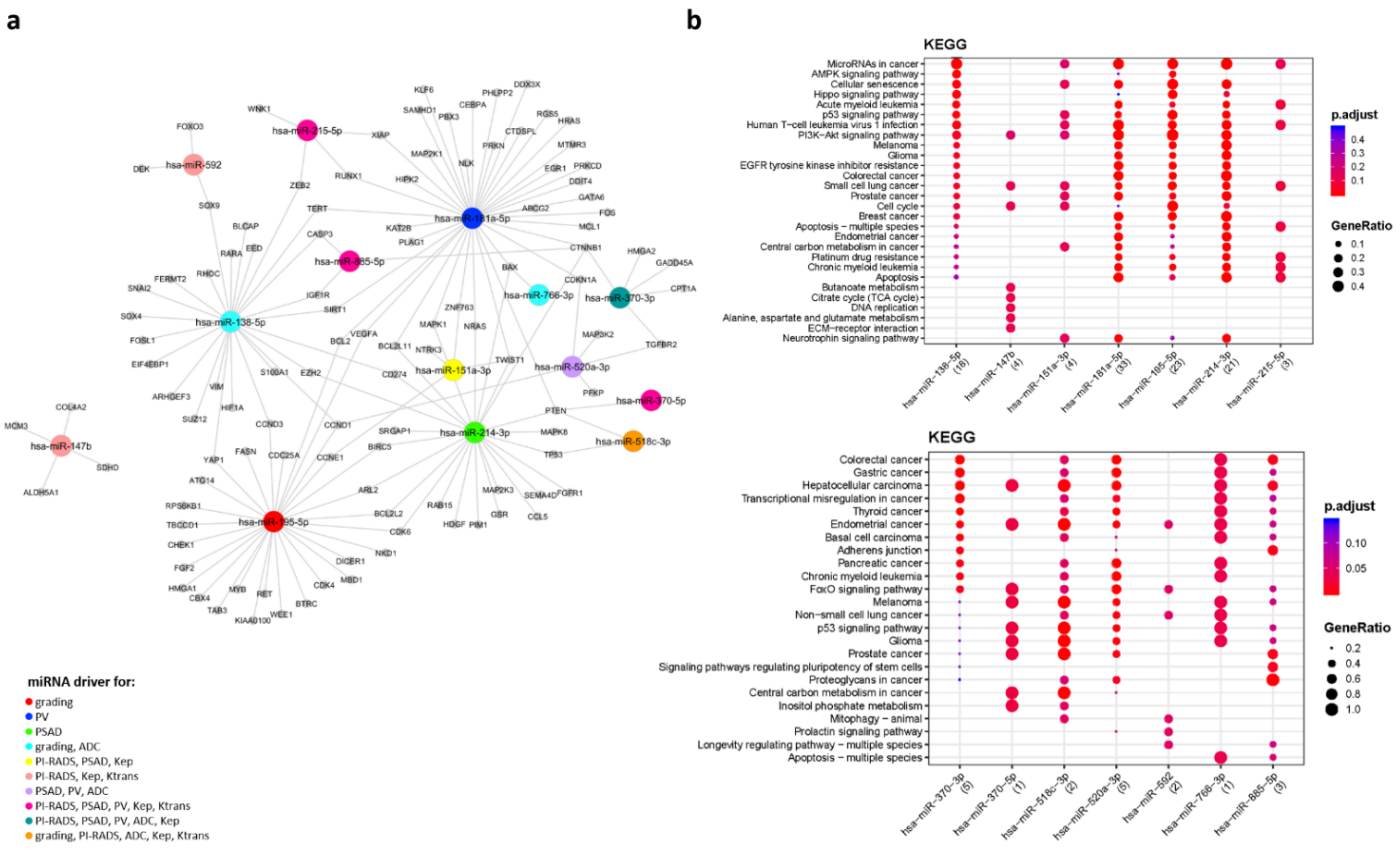
2.5. miRNA–Target Interaction Network
2.6. Functional Enrichment Analysis
2.7. RT-QPCR to Validate Differentially Expressed (DE) MicroRNAs
2.8. Statistical Analysis
3. Results
3.1. Analysis on the Cohort of Patients with PCa
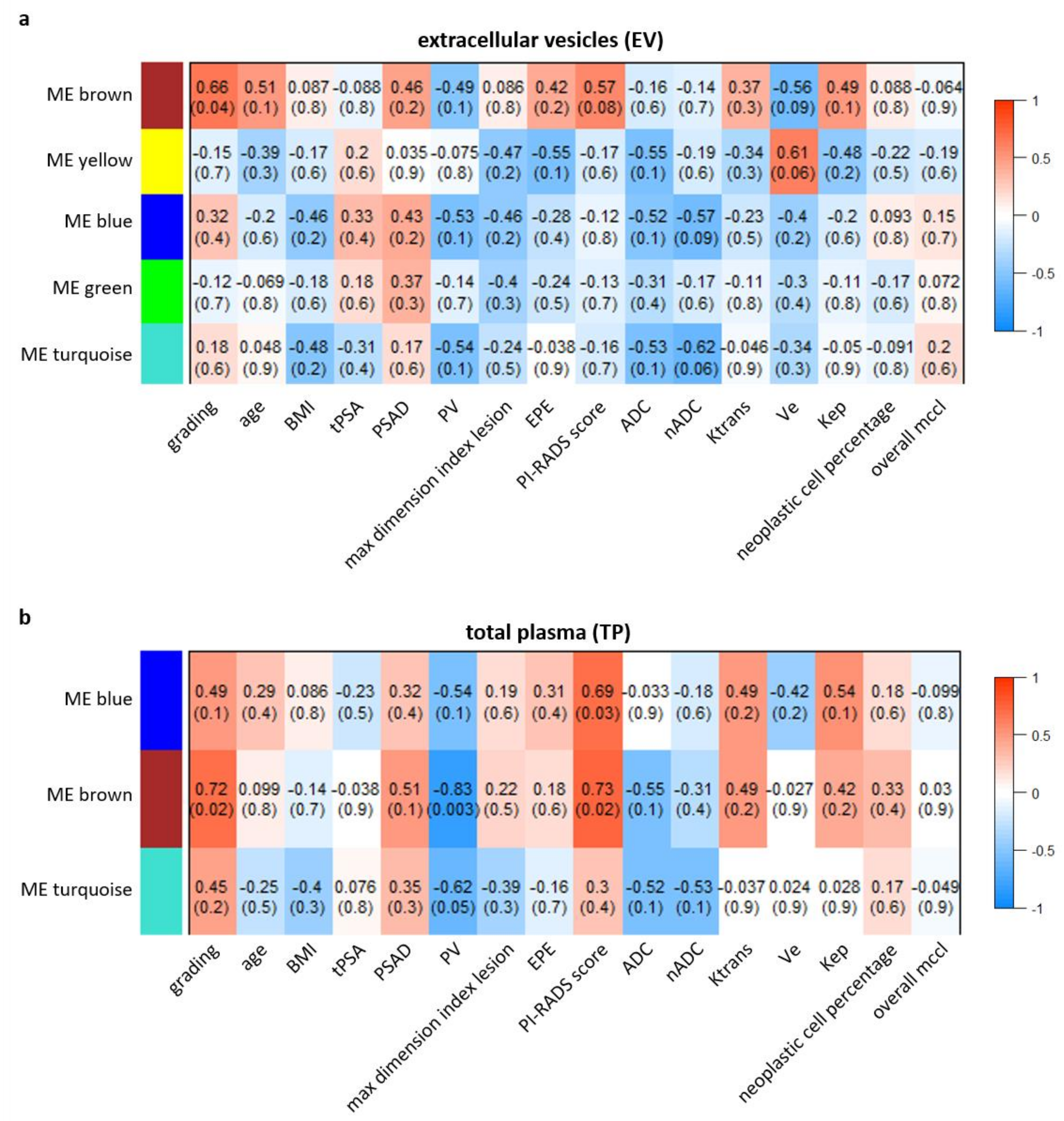
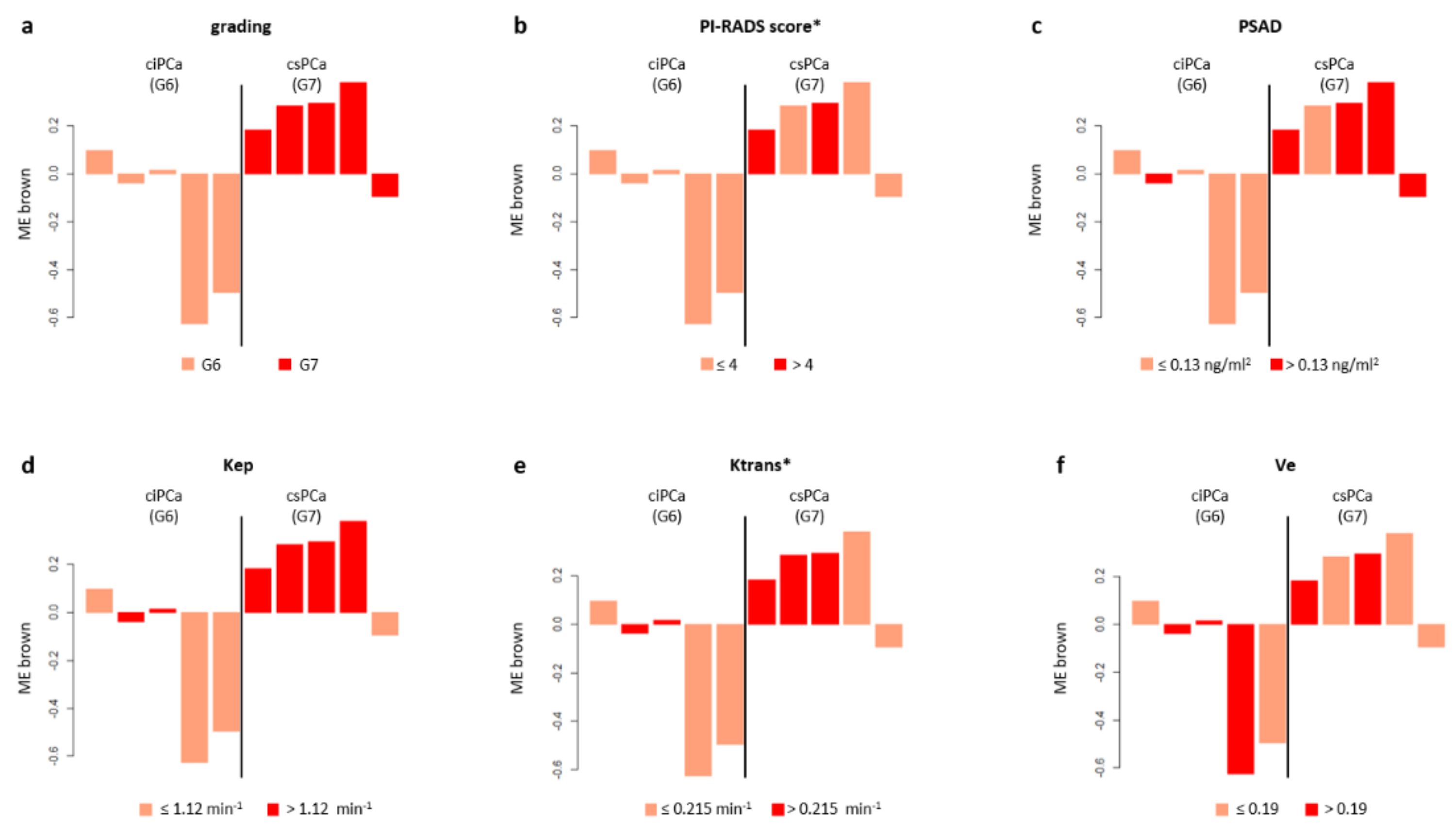
3.1.1. WGCNA on Extracellular Vesicles Data
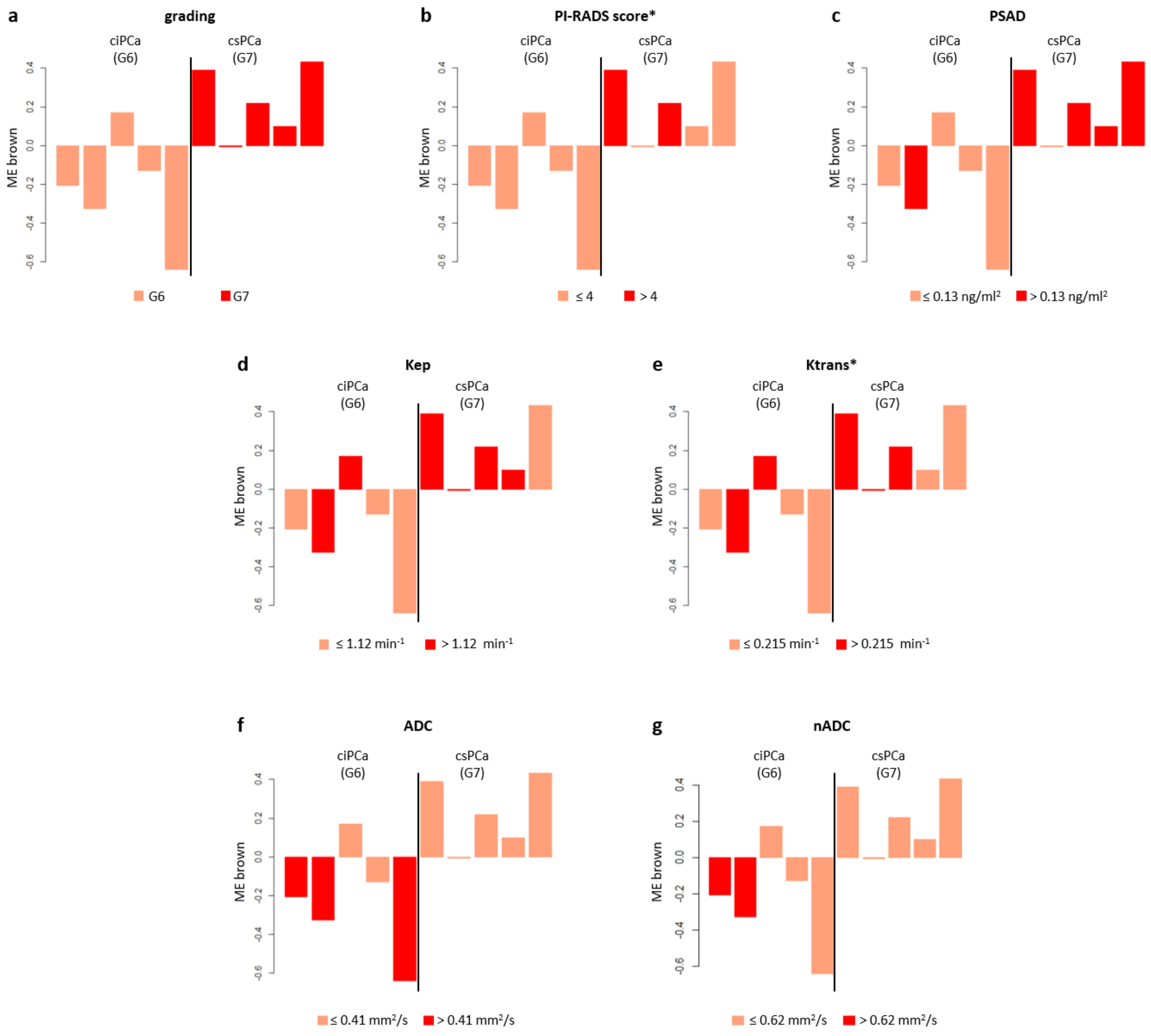
3.1.2. WGCNA on Total Plasma Data
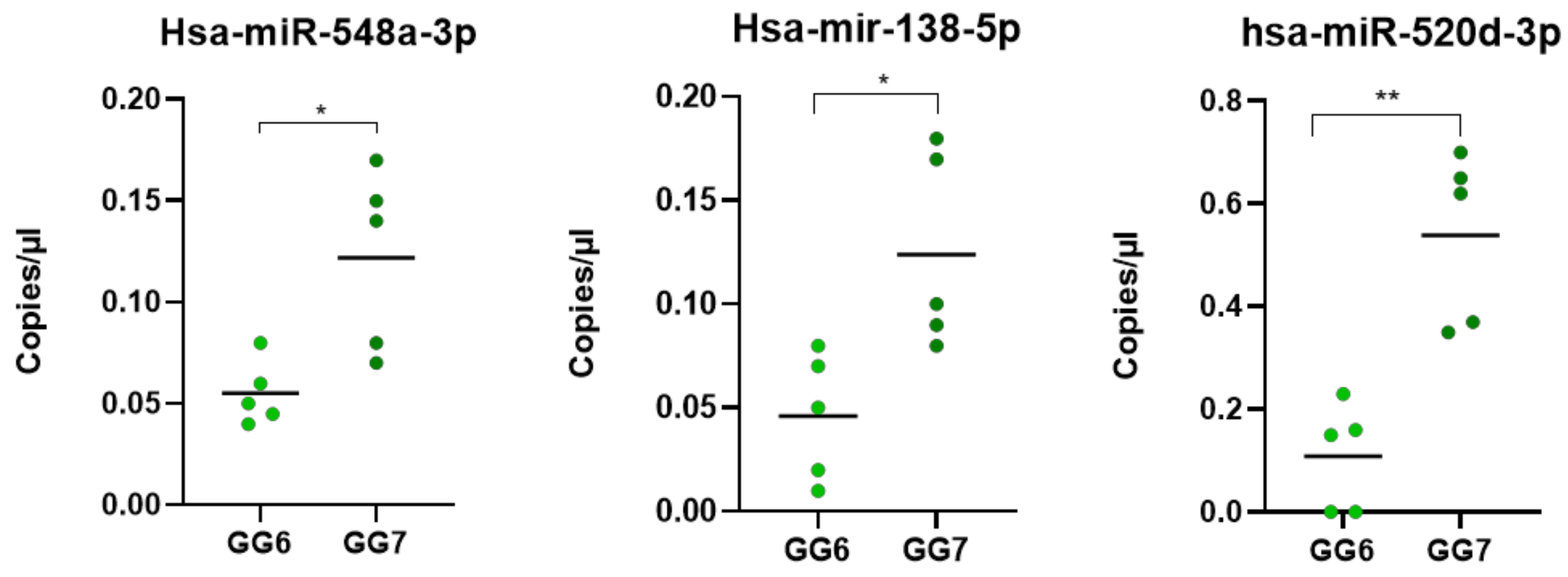
3.2. DEMs Validation Using RT-QPCR
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CAMCAP Study Group; The TCGA Consortium; Wedge, D.C.; Gundem, G.; Mitchell, T.; Woodcock, D.J.; Martincorena, I.; Ghori, M.; Zamora, J.; Butler, A.; et al. Sequencing of Prostate Cancers Identifies New Cancer Genes, Routes of Progression and Drug Targets. Nat. Genet. 2018, 50, 682–692. [Google Scholar] [CrossRef] [Green Version]
- PCF/SU2C International Prostate Cancer Dream Team; Armenia, J.; Wankowicz, S.A.M.; Liu, D.; Gao, J.; Kundra, R.; Reznik, E.; Chatila, W.K.; Chakravarty, D.; Han, G.C.; et al. The Long Tail of Oncogenic Drivers in Prostate Cancer. Nat. Genet. 2018, 50, 645–651. [Google Scholar] [CrossRef]
- Abeshouse, A.; Ahn, J.; Akbani, R.; Ally, A.; Amin, S.; Andry, C.D.; Annala, M.; Aprikian, A.; Armenia, J.; Arora, A.; et al. The Molecular Taxonomy of Primary Prostate Cancer. Cell 2015, 163, 1011–1025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamoun, A.; Cancel-Tassin, G.; Fromont, G.; Elarouci, N.; Armenoult, L.; Ayadi, M.; Irani, J.; Leroy, X.; Villers, A.; Fournier, G.; et al. Comprehensive Molecular Classification of Localized Prostate Adenocarcinoma Reveals a Tumour Subtype Predictive of Non-Aggressive Disease. Ann. Oncol. 2018, 29, 1814–1821. [Google Scholar] [CrossRef] [PubMed]
- Mottet, N.; Bellmunt, J.; Briers, E.; Bolla, M.; Bourke, L.; Cornford, P.; De Santis, M.; Henry, A.M.; Joniau, S.; Lam, T.B.; et al. EAU–ESTR –ESUR–SIOG Guidelines on Prostate Cancer. In Proceedings of the EAU Annual Congress, Amsterdam, EAU Guidelines Office, Arnhem, The Netherlands, 1 March 2021; ISBN 978-94-92671-07-3. [Google Scholar]
- Drost, F.-J.H.; Osses, D.F.; Nieboer, D.; Steyerberg, E.W.; Bangma, C.H.; Roobol, M.J.; Schoots, I.G. Prostate MRI, with or without MRI-Targeted Biopsy, and Systematic Biopsy for Detecting Prostate Cancer. Cochrane Database Syst. Rev. 2019, 4. [Google Scholar] [CrossRef] [PubMed]
- Sathianathen, N.J.; Omer, A.; Harriss, E.; Davies, L.; Kasivisvanathan, V.; Punwani, S.; Moore, C.M.; Kastner, C.; Barrett, T.; Van Den Bergh, R.C.; et al. Negative Predictive Value of Multiparametric Magnetic Resonance Imaging in the Detection of Clinically Significant Prostate Cancer in the Prostate Imaging Reporting and Data System Era: A Systematic Review and Meta-Analysis. Eur. Urol. 2020, 78, 402–414. [Google Scholar] [CrossRef]
- Panebianco, V.; Barchetti, G.; Simone, G.; Del Monte, M.; Ciardi, A.; Grompone, M.D.; Campa, R.; Indino, E.L.; Barchetti, F.; Sciarra, A.; et al. Negative Multiparametric Magnetic Resonance Imaging for Prostate Cancer: What’s Next? Eur. Urol. 2018, 74, 48–54. [Google Scholar] [CrossRef] [Green Version]
- Wilt, T.J.; Jones, K.M.; Barry, M.J.; Andriole, G.L.; Culkin, D.; Wheeler, T.; Aronson, W.J.; Brawer, M.K. Follow-up of Prostatectomy versus Observation for Early Prostate Cancer. N. Engl. J. Med. 2017, 377, 132–142. [Google Scholar] [CrossRef]
- Sciarra, A.; Panebianco, V.; Ciccariello, M.; Salciccia, S.; Lisi, D.; Osimani, M.; Alfarone, A.; Gentilucci, A.; Parente, U.; Passariello, R.; et al. Magnetic Resonance Spectroscopic Imaging (1 H-MRSI) and Dynamic Contrast-Enhanced Magnetic Resonance (DCE-MRI): Pattern Changes From Inflammation to Prostate Cancer. Cancer Investig. 2010, 28, 424–432. [Google Scholar] [CrossRef]
- Kasivisvanathan, V.; Rannikko, A.S.; Borghi, M.; Panebianco, V.; Mynderse, L.A.; Vaarala, M.H.; Briganti, A.; Budäus, L.; Hellawell, G.; Hindley, R.G.; et al. MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N. Engl. J. Med. 2018, 378, 1767–1777. [Google Scholar] [CrossRef]
- Ahmed, H.U.; El-Shater Bosaily, A.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. Diagnostic Accuracy of Multi-Parametric MRI and TRUS Biopsy in Prostate Cancer (PROMIS): A Paired Validating Confirmatory Study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef] [Green Version]
- Van der Leest, M.; Cornel, E.; Israël, B.; Hendriks, R.; Padhani, A.R.; Hoogenboom, M.; Zamecnik, P.; Bakker, D.; Setiasti, A.Y.; Veltman, J.; et al. Head-to-Head Comparison of Transrectal Ultrasound-Guided Prostate Biopsy Versus Multiparametric Prostate Resonance Imaging with Subsequent Magnetic Resonance-Guided Biopsy in Biopsy-Naïve Men with Elevated Prostate-Specific Antigen: A Large Prospective Multicenter Clinical Study. Eur. Urol. 2019, 75, 570–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rouvière, O.; Puech, P.; Renard-Penna, R.; Claudon, M.; Roy, C.; Mège-Lechevallier, F.; Decaussin-Petrucci, M.; Dubreuil-Chambardel, M.; Magaud, L.; Remontet, L.; et al. Use of Prostate Systematic and Targeted Biopsy on the Basis of Multiparametric MRI in Biopsy-Naive Patients (MRI-FIRST): A Prospective, Multicentre, Paired Diagnostic Study. Lancet Oncol. 2019, 20, 100–109. [Google Scholar] [CrossRef]
- Kasivisvanathan, V.; Stabile, A.; Neves, J.B.; Giganti, F.; Valerio, M.; Shanmugabavan, Y.; Clement, K.D.; Sarkar, D.; Philippou, Y.; Thurtle, D.; et al. Magnetic Resonance Imaging-Targeted Biopsy Versus Systematic Biopsy in the Detection of Prostate Cancer: A Systematic Review and Meta-Analysis. Eur. Urol. 2019, 76, 284–303. [Google Scholar] [CrossRef] [Green Version]
- Osses, D.; Roobol, M.; Schoots, I. Prediction Medicine: Biomarkers, Risk Calculators and Magnetic Resonance Imaging as Risk Stratification Tools in Prostate Cancer Diagnosis. Int. J. Mol. Sci. 2019, 20, 1637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammond, S.M. An Overview of MicroRNAs. Adv. Drug Deliv. Rev. 2015, 87, 3–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panebianco, V.; Pecoraro, M.; Fiscon, G.; Paci, P.; Farina, L.; Catalano, C. Prostate Cancer Screening Research Can Benefit from Network Medicine: An Emerging Awareness. npj Syst. Biol. Appl. 2020, 6, 13. [Google Scholar] [CrossRef]
- Langfelder, P.; Horvath, S. WGCNA: An R Package for Weighted Correlation Network Analysis. BMC Bioinform. 2008, 9, 559. [Google Scholar] [CrossRef] [Green Version]
- Zhang, B.; Horvath, S. A General Framework for Weighted Gene Co-Expression Network Analysis. Stat. Appl. Genet. Mol. Biol. 2005, 4. [Google Scholar] [CrossRef]
- Turkbey, B.; Rosenkrantz, A.B.; Haider, M.A.; Padhani, A.R.; Villeirs, G.; Macura, K.J.; Tempany, C.M.; Choyke, P.L.; Cornud, F.; Margolis, D.J.; et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur. Urol. 2019, 76, 340–351. [Google Scholar] [CrossRef]
- Giganti, F.; Pecoraro, M.; Fierro, D.; Campa, R.; Del Giudice, F.; Punwani, S.; Kirkham, A.; Allen, C.; Emberton, M.; Catalano, C.; et al. DWI and PRECISE Criteria in Men on Active Surveillance for Prostate Cancer: A Multicentre Preliminary Experience of Different ADC Calculations. Magn. Reson. Imaging 2020, 67, 50–58. [Google Scholar] [CrossRef] [Green Version]
- RefFinder. Available online: https://www.heartcure.com.au/reffinder/ (accessed on 30 September 2021).
- Licursi, V.; Conte, F.; Fiscon, G.; Paci, P. MIENTURNET: An Interactive Web Tool for MicroRNA-Target Enrichment and Network-Based Analysis. BMC Bioinform. 2019, 20, 545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanehisa, M.; Sato, Y.; Kawashima, M.; Furumichi, M.; Tanabe, M. KEGG as a Reference Resource for Gene and Protein Annotation. Nucleic Acids Res. 2016, 44, D457–D462. [Google Scholar] [CrossRef] [Green Version]
- Bajgiran, A.M.; Mirak, S.A.; Sung, K.; Sisk, A.E.; Reiter, R.E.; Raman, S.S. Apparent Diffusion Coefficient (ADC) Ratio Versus Conventional ADC for Detecting Clinically Significant Prostate Cancer With 3-T MRI. Am. J. Roentgenol. 2019, 213, W134–W142. [Google Scholar] [CrossRef]
- Meyer, H.-J.; Wienke, A.; Surov, A. Discrimination between Clinical Significant and Insignificant Prostate Cancer with Apparent Diffusion Coefficient—A Systematic Review and Meta Analysis. BMC Cancer 2020, 20, 482. [Google Scholar] [CrossRef] [PubMed]
- Hötker, A.M.; Mazaheri, Y.; Aras, Ö.; Zheng, J.; Moskowitz, C.S.; Gondo, T.; Matsumoto, K.; Hricak, H.; Akin, O. Assessment of Prostate Cancer Aggressiveness by Use of the Combination of Quantitative DWI and Dynamic Contrast-Enhanced MRI. Am. J. Roentgenol. 2016, 206, 756–763. [Google Scholar] [CrossRef] [Green Version]
- Wei, C.; Jin, B.; Szewczyk-Bieda, M.; Gandy, S.; Lang, S.; Zhang, Y.; Huang, Z.; Nabi, G. Quantitative Parameters in Dynamic Contrast-Enhanced Magnetic Resonance Imaging for the Detection and Characterization of Prostate Cancer. Oncotarget 2018, 9, 15997–16007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Distler, F.A.; Radtke, J.P.; Bonekamp, D.; Kesch, C.; Schlemmer, H.-P.; Wieczorek, K.; Kirchner, M.; Pahernik, S.; Hohenfellner, M.; Hadaschik, B.A. The Value of PSA Density in Combination with PI-RADSTM for the Accuracy of Prostate Cancer Prediction. J. Urol. 2017, 198, 575–582. [Google Scholar] [CrossRef]
- Washino, S.; Okochi, T.; Saito, K.; Konishi, T.; Hirai, M.; Kobayashi, Y.; Miyagawa, T. Combination of Prostate Imaging Reporting and Data System (PI-RADS) Score and Prostate-Specific Antigen (PSA) Density Predicts Biopsy Outcome in Prostate Biopsy Naïve Patients. Bju Int. 2017, 119, 225–233. [Google Scholar] [CrossRef] [Green Version]
- Bhat, N.R.; Vetter, J.M.; Andriole, G.L.; Shetty, A.S.; Ippolito, J.E.; Kim, E.H. Magnetic Resonance Imaging-Defined Prostate-Specific Antigen Density Significantly Improves the Risk Prediction for Clinically Significant Prostate Cancer on Biopsy. Urology 2019, 126, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Stoyanova, R.; Pollack, A.; Takhar, M.; Lynne, C.; Parra, N.; Lam, L.L.C.; Alshalalfa, M.; Buerki, C.; Castillo, R.; Jorda, M.; et al. Association of Multiparametric MRI Quantitative Imaging Features with Prostate Cancer Gene Expression in MRI-Targeted Prostate Biopsies. Oncotarget 2016, 7, 53362–53376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norris, J.M.; Simpson, B.S.; Parry, M.A.; Allen, C.; Ball, R.; Freeman, A.; Kelly, D.; Kim, H.L.; Kirkham, A.; You, S.; et al. Genetic Landscape of Prostate Cancer Conspicuity on Multiparametric Magnetic Resonance Imaging: A Systematic Review and Bioinformatic Analysis. Eur. Urol. Open Sci. 2020, 20, 37–47. [Google Scholar] [CrossRef]
- Gulyaeva, L.F.; Kushlinskiy, N.E. Regulatory Mechanisms of MicroRNA Expression. J. Transl. Med. 2016, 14, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Xu, L.; Hu, Y.; Huang, Y.; Zhang, Y.; Zheng, X.; Wang, S.; Wang, Y.; Yu, Y.; Zhang, M.; et al. MiRNA Let-7b Modulates Macrophage Polarization and Enhances Tumor-Associated Macrophages to Promote Angiogenesis and Mobility in Prostate Cancer. Sci. Rep. 2016, 6, 25602. [Google Scholar] [CrossRef] [Green Version]
- Jeon, J.; Olkhov-Mitsel, E.; Xie, H.; Yao, C.Q.; Zhao, F.; Jahangiri, S.; Cuizon, C.; Scarcello, S.; Jeyapala, R.; Watson, J.D.; et al. Temporal Stability and Prognostic Biomarker Potential of the Prostate Cancer Urine MiRNA Transcriptome. Jnci J. Natl. Cancer Inst. 2020, 112, 247–255. [Google Scholar] [CrossRef]
- Cai, C.; Chen, Q.-B.; Han, Z.-D.; Zhang, Y.-Q.; He, H.-C.; Chen, J.-H.; Chen, Y.-R.; Yang, S.-B.; Wu, Y.-D.; Zeng, Y.-R.; et al. MiR-195 Inhibits Tumor Progression by Targeting RPS6KB1 in Human Prostate Cancer. Clin. Cancer Res. 2015, 21, 4922–4934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.; Ji, A.; Wang, X.; Zhu, Y.; Yu, Y.; Lin, Y.; Liu, Y.; Li, S.; Liang, Z.; Xu, X.; et al. MicroRNA-195-5p, a New Regulator of Fra-1, Suppresses the Migration and Invasion of Prostate Cancer Cells. J. Transl. Med. 2015, 13, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arámbula-Meraz, E.; Bergez-Hernández, F.; Leal-León, E.; Romo-Martínez, E.; Picos-Cárdenas, V.; Luque-Ortega, F.; Romero-Quintana, J.; Alvarez-Arrazola, M.; García-Magallanes, N. Expression of MiR-148b-3p Is Correlated with Overexpression of Biomarkers in Prostate Cancer. Genet. Mol. Biol. 2020, 43, e20180330. [Google Scholar] [CrossRef]
- Tay, Y.; Tan, S.M.; Karreth, F.A.; Lieberman, J.; Pandolfi, P.P. Characterization of Dual PTEN and P53-Targeting MicroRNAs Identifies MicroRNA-638/Dnm2 as a Two-Hit Oncogenic Locus. Cell Rep. 2014, 8, 714–722. [Google Scholar] [CrossRef] [Green Version]
- Boyerinas, B.; Park, S.-M.; Hau, A.; Murmann, A.E.; Peter, M.E. The Role of Let-7 in Cell Differentiation and Cancer. Endocr.-Relat. Cancer 2010, 17, F19–F36. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Biopsed Cohort |
|---|---|
| Mean age (years), SD | 64.8 ± 9.40 |
| Mean PSA value (ng/mL), SD | 7.62 ± 2.59 |
| Mean PSA density (ng/mL2), SD | 0.17 ± 0.12 |
| Mean prostate volume (ml), SD | 57.6 ± 36.43 |
| PCa-negative, n (%) | 5 (33) |
| PCa-positive, n (%) | 10 (67) |
| Gleason grade 1, n (%) | 5 (33) |
| Gleason grade 2, n (%) | 5 (33) |
| Peripheral zone, n (%) | 13 (87) |
| Transition zone, n (%) | 2 (13) |
| PI-RADS scoring: | |
| PI-RADS 3, n (%) | 5 (33) |
| PI-RADS 4, n (%) | 8 (54) |
| PI-RADS 5, n (%) | 2 (13) |
| Prior TURP, n | 2 (13) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Panebianco, V.; Paci, P.; Pecoraro, M.; Conte, F.; Carnicelli, G.; Besharat, Z.M.; Catanzaro, G.; Splendiani, E.; Sciarra, A.; Farina, L.; et al. Network Analysis Integrating microRNA Expression Profiling with MRI Biomarkers and Clinical Data for Prostate Cancer Early Detection: A Proof of Concept Study. Biomedicines 2021, 9, 1470. https://doi.org/10.3390/biomedicines9101470
Panebianco V, Paci P, Pecoraro M, Conte F, Carnicelli G, Besharat ZM, Catanzaro G, Splendiani E, Sciarra A, Farina L, et al. Network Analysis Integrating microRNA Expression Profiling with MRI Biomarkers and Clinical Data for Prostate Cancer Early Detection: A Proof of Concept Study. Biomedicines. 2021; 9(10):1470. https://doi.org/10.3390/biomedicines9101470
Chicago/Turabian StylePanebianco, Valeria, Paola Paci, Martina Pecoraro, Federica Conte, Giorgia Carnicelli, Zein Mersini Besharat, Giuseppina Catanzaro, Elena Splendiani, Alessandro Sciarra, Lorenzo Farina, and et al. 2021. "Network Analysis Integrating microRNA Expression Profiling with MRI Biomarkers and Clinical Data for Prostate Cancer Early Detection: A Proof of Concept Study" Biomedicines 9, no. 10: 1470. https://doi.org/10.3390/biomedicines9101470
APA StylePanebianco, V., Paci, P., Pecoraro, M., Conte, F., Carnicelli, G., Besharat, Z. M., Catanzaro, G., Splendiani, E., Sciarra, A., Farina, L., Catalano, C., & Ferretti, E. (2021). Network Analysis Integrating microRNA Expression Profiling with MRI Biomarkers and Clinical Data for Prostate Cancer Early Detection: A Proof of Concept Study. Biomedicines, 9(10), 1470. https://doi.org/10.3390/biomedicines9101470