

The Development of a Nomogram Predictive Model for Intracardiac Thrombosis Risk: A Study Based on Risk Factors in Patients with Acute Myocardial Infarction


Abstract
1. Introduction
2. Materials and Methods
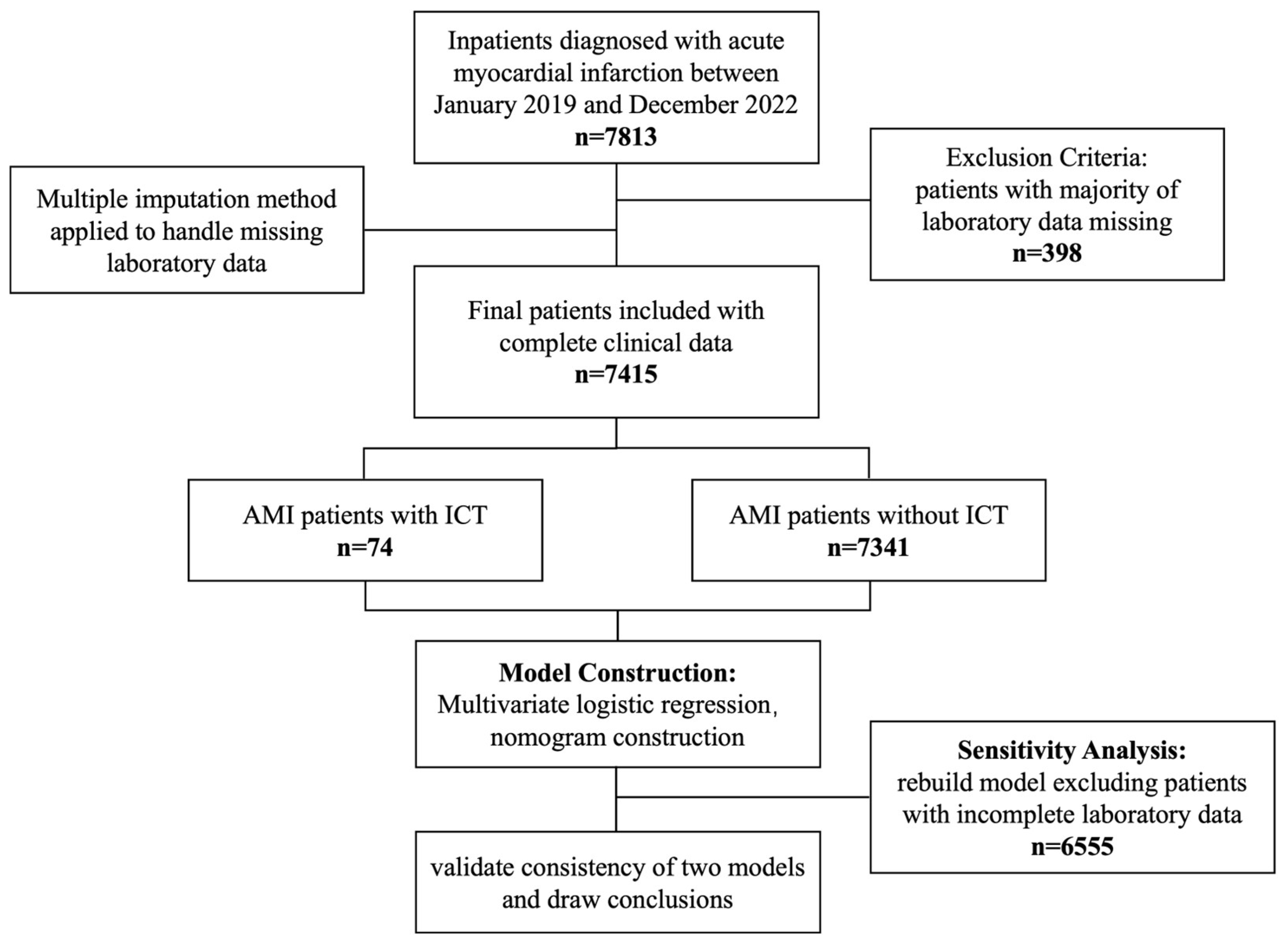
2.1. Study Design and Patients
2.2. Data Collection
2.3. Statistical Analyses
3. Results
3.1. The Subsection of Characteristics of the Studied Population
3.2. Risk Factors of ICT in AMI Patients
3.3. The Construction of the Nomogram Model
3.4. Model Accuracy Assessment
3.5. Sensitivity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Correction Statement
Abbreviations
| IQR | Interquartile range |
| ICT | Intracardiac thrombosis |
| AMI | Acute myocardial infarction |
| AWMI | Anterior wall myocardial infarction |
| AF | Atrial fibrillation |
| CKD | Chronic kidney disease |
| HDLC | High-density lipoprotein cholesterol |
| WBC | White blood cell |
| NEUs | Neutrophils |
| LYMs | Lymphocytes |
| BUN | Blood urea nitrogen |
| CK-MB | Creatine kinase-MB |
| CK | Creatine kinase |
| NT-proBNP | N-terminal pro-B-type natriuretic peptide |
| AST | Aspartate aminotransferase |
| ALT | Alanine aminotransferase |
| PT | Prothrombin time |
| INR | international normalized ratio |
| TT | Thrombin time |
| ROC curve | Receiver operating characteristic curve |
| AUC | Area under the ROC curve |
References
- Anderson, J.L.; Morrow, D.A. Acute Myocardial Infarction. N. Engl. J. Med. 2017, 376, 2053–2064. [Google Scholar] [CrossRef] [PubMed]
- Gong, F.F.; Vaitenas, I.; Malaisrie, S.C.; Maganti, K. Mechanical complications of acute myocardial infarction: A review. JAMA Cardiol. 2021, 6, 341–349. [Google Scholar] [CrossRef]
- Byrne, R.A.; Rossello, X.; Coughlan, J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.-A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the management of acute coronary syndromes: Developed by the task force on the management of acute coronary syndromes of the European Society of Cardiology (ESC). Eur. Heart J. Acute Cardiovasc. Care 2024, 13, 55–161. [Google Scholar] [CrossRef] [PubMed]
- Vaideeswar, P.; Divate, S.; Harke, M. Intracardiac thrombi in extracardiac disorders: An autopsy study. Cardiovasc. Pathol. 2012, 21, e1–e9. [Google Scholar] [CrossRef]
- Wang, P.; Ye, X.; Yan, D.; Peng, Y.; Zhang, Z. Incidence and risk factors of left ventricular thrombus in acute ST-segment elevation myocardial infarction treated by primary percutaneous coronary intervention: A meta-analysis. Med. Princ. Pract. 2022, 31, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Leow, A.S.; Sia, C.H.; Tan, B.Y.; Chan, M.Y.; Loh, J.P. Characterisation of patients with acute myocardial infarction complicated by left ventricular thrombus. Eur. J. Intern. Med. 2020, 74, 110–112. [Google Scholar] [CrossRef]
- Patel, M.; Wei, X.; Weigel, K.; Gertz, Z.M.; Kron, J.; Robinson, A.A.; Trankle, C.R. Diagnosis and treatment of intracardiac thrombus. J. Cardiovasc. Pharmacol. 2021, 78, 361–371. [Google Scholar] [CrossRef]
- McCarthy, C.P.; Vaduganathan, M.; McCarthy, K.J.; Januzzi, J.L.; Bhatt, D.L.; McEvoy, J.W. Left ventricular thrombus after acute myocardial infarction: Screening, prevention, and treatment. JAMA Cardiol. 2018, 3, 642–649. [Google Scholar] [CrossRef]
- Weinsaft, J.W.; Kim, H.W.; Shah, D.J.; Klem, I.; Crowley, A.L.; Brosnan, R.; James, O.G.; Patel, M.R.; Heitner, J.; Parker, M.; et al. Detection of left ventricular thrombus by delayed-enhancement cardiovascular magnetic resonance prevalence and markers in patients with systolic dysfunction. J. Am. Coll. Cardiol. 2008, 52, 148–157. [Google Scholar] [CrossRef]
- Chang, P.; Xiao, J.; Hu, Z.; Kwan, A.C.; Fan, Z. Imaging of left heart intracardiac thrombus: Clinical needs, current imaging, and emerging cardiac magnetic resonance techniques. Ther. Adv. Cardiovasc. Dis. 2022, 16, 17539447221107737. [Google Scholar] [CrossRef]
- Boivin-Proulx, L.-A.; Ieroncig, F.; Demers, S.-P.; Nozza, A.; Soltani, M.; Ghersi, I.; Verreault-Julien, L.; Alansari, Y.; Massie, C.; Simard, P.; et al. Contemporary incidence and predictors of left ventricular thrombus in patients with anterior acute myocardial infarction. Clin. Res. Cardiol. 2023, 112, 558–565. [Google Scholar] [CrossRef] [PubMed]
- Levine, G.N.; Bates, E.R.; Bittl, J.A.; Brindis, R.G.; Fihn, S.D.; Fleisher, L.A.; Granger, C.B.; Lange, R.A.; Mack, M.J.; Mauri, L.; et al. 2016 ACC/AHA guideline focused update on duration of dual antiplatelet therapy in patients with coronary artery disease: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines: An update of the 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention, 2011 ACCF/AHA guideline for coronary artery bypass graft surgery, 2012 ACC/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease, 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction, 2014 AHA/ACC guideline for the management of patients with non–ST-elevation acute coronary syndromes, and 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery. Circulation 2016, 134, e123–e155. [Google Scholar]
- Bhatt, D.L.; Lopes, R.D.; Harrington, R.A. Diagnosis and treatment of acute coronary syndromes: A review. JAMA 2022, 327, 662–675. [Google Scholar] [CrossRef] [PubMed]
- Bittl, J.A.; Baber, U.; Bradley, S.M.; Wijeysundera, D.N. Duration of dual antiplatelet therapy: A systematic review for the 2016 ACC/AHA guideline focused update on duration of dual antiplatelet therapy in patients with coronary artery disease: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2016, 68, 1116–1139. [Google Scholar]
- Strom, J.; Manning, W. Identification of Intracardiac Thrombus. In Essential Echocardiography: A Companion to Braunwald’s Heart Disease; Elsevier Health Sciences: Amsterdam, The Netherlands, 2017; p. 392. [Google Scholar]
- Shah, T.; Haimi, I.; Yang, Y.; Gaston, S.; Taoutel, R.; Mehta, S.; Lee, H.J.; Zambahari, R.; Baumbach, A.; Henry, T.D. Meta-analysis of gender disparities in in-hospital care and outcomes in patients with ST-segment elevation myocardial infarction. Am. J. Cardiol. 2021, 147, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Medzikovic, L.; Azem, T.; Sun, W.; Rejali, P.; Esdin, L.; Rahman, S.; Dehghanitafti, A.; Aryan, L.; Eghbali, M. Sex differences in therapies against myocardial ischemia-reperfusion injury: From basic science to clinical perspectives. Cells 2023, 12, 2077. [Google Scholar] [CrossRef]
- Kaplan, A.; Abidi, E.; Diab, R.; Ghali, R.; Al-Awassi, H.; Booz, G.W.; Zouein, F.A. Sex differences in cardiac remodeling post myocardial infarction with acute cigarette smoking. Biol. Sex Differ. 2022, 13, 36. [Google Scholar] [CrossRef]
- D’Onofrio, G.; Safdar, B.; Lichtman, J.H.; Strait, K.M.; Dreyer, R.P.; Geda, M.; Spertus, J.A.; Krumholz, H.M. Sex differences in reperfusion in young patients with ST-segment–elevation myocardial infarction: Results from the VIRGO study. Circulation 2015, 131, 1324–1332. [Google Scholar] [CrossRef]
- Díez-Delhoyo, F.; Gutiérrez-Ibañes, E.; Sanz-Ruiz, R.; Vázquez-Álvarez, M.E.; González Saldívar, H.; Rivera Juárez, A.; Sarnago, F.; Martínez-Sellés, M.; Bermejo, J.; Soriano, J. Prevalence of microvascular and endothelial dysfunction in the nonculprit territory in patients with acute myocardial infarction: The FISIOIAM study. Circ. Cardiovasc. Interv. 2019, 12, e007257. [Google Scholar] [CrossRef]
- Grover-Páez, F.; Zavalza-Gómez, A.B. Endothelial dysfunction and cardiovascular risk factors. Diabetes Res. Clin. Pract. 2009, 84, 1–10. [Google Scholar] [CrossRef]
- Choi, U.L.; Park, J.-H.; Sun, B.J.; Oh, J.K.; Seong, S.W.; Lee, J.-H.; Choi, S.W.; Jeong, J.-O.; Kwon, I.S.; Seong, I.-W. Impaired left ventricular diastolic function is related to the formation of left ventricular apical thrombus in patients with acute anterior myocardial infarction. Heart Vessel. 2018, 33, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Keren, A.; Goldberg, S.; Gottlieb, S.; Klein, J.; Schuger, C.; Medina, A.; Tzivoni, D.; Stern, S. Natural history of left ventricular thrombi: Their appearance and resolution in the posthospitalization period of acute myocardial infarction. J. Am. Coll. Cardiol. 1990, 15, 790–800. [Google Scholar] [CrossRef] [PubMed]
- Ram, P.; Shah, M.; Sirinvaravong, N.; Lo, K.B.; Patil, S.; Patel, B.; Tripathi, B.; Garg, L.; Figueredo, V. Left ventricular thrombosis in acute anterior myocardial infarction: Evaluation of hospital mortality, thromboembolism, and bleeding. Clin. Cardiol. 2018, 41, 1289–1296. [Google Scholar] [CrossRef]
- Delewi, R.; Zijlstra, F.; Piek, J.J. Left ventricular thrombus formation after acute myocardial infarction. Heart 2012, 98, 1743–1749. [Google Scholar] [CrossRef] [PubMed]
- Camaj, A.; Fuster, V.; Giustino, G.; Bienstock, S.W.; Sternheim, D.; Mehran, R.; Dangas, G.D.; Kini, A.; Sharma, S.K.; Halperin, J. Left ventricular thrombus following acute myocardial infarction: JACC state-of-the-art review. J. Am. Coll. Cardiol. 2022, 79, 1010–1022. [Google Scholar] [CrossRef]
- Rathore, S.S.; Berger, A.K.; Weinfurt, K.P.; Schulman, K.A.; Oetgen, W.J.; Gersh, B.J.; Solomon, A.J. Acute myocardial infarction complicated by atrial fibrillation in the elderly: Prevalence and outcomes. Circulation 2000, 101, 969–974. [Google Scholar] [CrossRef] [PubMed]
- Espe, E.K.; Aronsen, J.M.; Eriksen, M.; Sejersted, O.M.; Zhang, L.; Sjaastad, I. Regional dysfunction after myocardial infarction in rats. Circ. Cardiovasc. Imaging 2017, 10, e005997. [Google Scholar] [CrossRef]
- Leancă, S.A.; Crișu, D.; Petriș, A.O.; Afrăsânie, I.; Genes, A.; Costache, A.D.; Tesloianu, D.N.; Costache, I.I. Left ventricular remodeling after myocardial infarction: From physiopathology to treatment. Life 2022, 12, 1111. [Google Scholar] [CrossRef]
- Low, C.J.; Leow, A.S.-T.; Syn, N.L.-X.; Tan, B.Y.-Q.; Yeo, L.L.-L.; Tay, E.L.-W.; Yeo, T.-C.; Chan, M.Y.-Y.; Loh, J.P.-Y.; Sia, C.-H. Outcomes of left ventricular thrombosis in post-acute myocardial infarction patients stratified by antithrombotic strategies: A meta-analysis with meta-regression. Int. J. Cardiol. 2021, 329, 36–45. [Google Scholar] [CrossRef]
- Hansen, C.H.; Ritschel, V.; Halvorsen, S.; Andersen, G.; Bjørnerheim, R.; Eritsland, J.; Arnesen, H.; Seljeflot, I. Markers of thrombin generation are associated with myocardial necrosis and left ventricular impairment in patients with ST-elevation myocardial infarction. Thromb. J. 2015, 13, 31. [Google Scholar] [CrossRef]
- Zhang, Q.; Si, D.; Zhang, Z.; Wang, C.; Zheng, H.; Li, S.; Huang, S.; Zhang, W. Value of the platelet-to-lymphocyte ratio in the prediction of left ventricular thrombus in anterior ST-elevation myocardial infarction with left ventricular dysfunction. BMC Cardiovasc. Disord. 2020, 20, 428. [Google Scholar] [CrossRef] [PubMed]
- Smid, M.; Dielis, A.; Winkens, M.; Spronk, H.; Van Oerle, R.; Hamulyak, K.; Prins, M.; Rosing, J.; Waltenberger, J.; Ten Cate, H. Thrombin generation in patients with a first acute myocardial infarction. J. Thromb. Haemost. 2011, 9, 450–456. [Google Scholar] [CrossRef] [PubMed]
- Cirakoglu, O.F.; Aslan, A.O.; Yilmaz, A.S.; Şahin, S.; Akyüz, A.R. Association between C-reactive protein to albumin ratio and left ventricular thrombus formation following acute anterior myocardial infarction. Angiology 2020, 71, 804–811. [Google Scholar] [CrossRef] [PubMed]
- Osherov, A.B.; Borovik-Raz, M.; Aronson, D.; Agmon, Y.; Kapeliovich, M.; Kerner, A.; Grenadier, E.; Hammerman, H.; Nikolsky, E.; Roguin, A. Incidence of early left ventricular thrombus after acute anterior wall myocardial infarction in the primary coronary intervention era. Am. Heart J. 2009, 157, 1074–1080. [Google Scholar] [CrossRef]
- Gianstefani, S.; Douiri, A.; Delithanasis, I.; Rogers, T.; Sen, A.; Kalra, S.; Charangwa, L.; Reiken, J.; Monaghan, M.; MacCarthy, P. Incidence and predictors of early left ventricular thrombus after ST-elevation myocardial infarction in the contemporary era of primary percutaneous coronary intervention. Am. J. Cardiol. 2014, 113, 1111–1116. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 7415) | Control Group (n = 7341) | ICT Group (n = 74) | p-Value |
|---|---|---|---|---|
| Enrollment basic characteristics | ||||
| Age (years, IQR) | 61.00 (53.0–69.0) | 61.00 (53.00–69.00) | 60.00 (49.25–69.75) | 0.408 |
| Female (n, %) | 1407 (18.98) | 1400 (19.07) | 7 (9.46) | 0.036 |
| Location of AMI | ||||
| AWMI (n, %) | 2185 (29.47) | 2122 (28.91) | 63 (85.14) | <0.001 |
| Comorbidities | ||||
| Ventricular aneurysm (n, %) | 280 (3.78) | 237 (3.23) | 43 (58.11) | <0.001 |
| AF (n, %) | 366 (4.94) | 361 (4.92) | 5 (6.76) | 0.648 |
| Hypertension (n, %) | 3908 (52.70) | 3870 (52.72) | 38 (51.35) | 0.815 |
| Diabates (n, %) | 2187 (29.49) | 2163 (29.46) | 24 (32.43) | 0.577 |
| CKD (n, %) | 160 (2.16) | 159 (2.17) | 1 (1.35) | 0.938 |
| Hyperlipemia (n, %) | 5345 (72.08) | 5297 (72.16) | 48 (64.86) | 0.164 |
| Low HDLC (n, %) | 5052 (68.13) | 5006 (68.19) | 46 (62.16) | 0.268 |
| Killip classification (n, %) | ||||
| I | 5848 (78.87) | 5805 (79.08) | 43 (58.11) | <0.001 |
| II | 1170 (15.78) | 1144 (15.58) | 26 (35.14) | <0.001 |
| III | 156 (2.10) | 153 (2.08) | 3 (4.05) | 0.443 |
| IV | 241 (3.25) | 239 (3.26) | 2 (2.70) | 1.000 |
| Laboratory results | ||||
| WBC (×109/L, IQR) | 8.67 (6.76–11.16) | 8.65 (6.76–11.15) | 9.43 (7.34–11.64) | 0.072 |
| NEUs (×109/L, IQR) | 6.41 (4.66–9.00) | 6.40 (4.65–8.99) | 7.31 (5.31–9.69) | 0.026 |
| LYMs (×109/L, IQR) | 1.41 (1.03–1.88) | 1.42 (1.03–1.88) | 1.33 (0.94–1.71) | 0.087 |
| Creatinine (μmol/L, IQR) | 65.00 (54.0–78.0) | 65.00 (54.00–78.00) | 70.00 (53.25–82.50) | 0.126 |
| BUN (mmol/L, IQR) | 5.56 (4.48–6.92) | 5.55 (4.47–6.92) | 6.00 (4.98–7.49) | 0.013 |
| CK-MB (U/L, IQR) | 29.40 (15.00–94.00) | 29.30 (15.0–93.5) | 34.70 (17.77–126.93) | 0.112 |
| CK (U/L, IQR) | 257.00 (102.00–831.50) | 257.00 (101.0–827.0) | 249.00 (117.75–1440.50) | 0.231 |
| D-dimer (mg/L, IQR) | 0.47 (0.27–0.87) | 0.46 (0.27–0.86) | 1.10 (0.62–2.28) | <0.001 |
| AST (U/L, IQR) | 45.00 (26.00–100.50) | 44.00 (26.0–100.0) | 58.00 (33.00–196.50) | 0.012 |
| ALT (U/L, IQR) | 31.00 (21.00–48.00) | 31.00 (21.0–48.0) | 38.50 (26.50–67.00) | 0.007 |
| PT (s, IQR) | 13.00 (11.80–13.80) | 13.0 (11.80–13.80) | 13.70 (12.93–14.67) | <0.001 |
| Prothrombin activity (%, IQR) | 98.00 (86.0–108.0) | 98.0 (86.00–108.10) | 87.10 (73.25–97.00) | <0.001 |
| INR (IQR) | 1.02 (0.97–1.09) | 1.02 (0.96–1.09) | 1.07 (1.02–1.17) | <0.001 |
| TT (s, IQR) | 17.20 (16.40–18.40) | 17.20 (16.40–18.40) | 16.75 (16.02–18.15) | 0.036 |
| Univariate Regression | Multivariate Analysis | |||
|---|---|---|---|---|
| Variables | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| Gender (male) | 2.936 (1.101–6.024) | 0.029 | 2.936 (1.322–6.751) | 0.009 |
| AWMI | 5.761 (2.808–11.819) | <0.001 | 5.186 (2.569–10.467) | <0.001 |
| Ventricular aneurysm | 20.657 (11.779–36.226) | <0.001 | 21.216 (12.455–36.183) | <0.001 |
| Killip I | 1.534 (0.508–4.634) | 0.448 | ||
| Killip II | 2.667 (0.866–8.216) | 0.087 | ||
| NEUs (×109/L) | 0.927 (0.853–1.007) | 0.073 | ||
| LYMs (×109/L) | 0.852 (0.553–1.312) | 0.467 | ||
| BUN (mmol/L) | 1.069 (0.998–1.146) | 0.058 | ||
| D-dimer (mg/L) | 1.001 (0.974–1.029) | 0.929 | ||
| AST (U/L) | 1.000 (0.999–1.001) | 0.683 | ||
| ALT (U/L) | 1.001 (1.000–1.002) | 0.199 | ||
| PT (s) | 1.019 (0.998–1.040) | 0.072 | ||
| Prothrombin activity (%) | 1.039 (1.018–1.062) | <0.001 | 1.039 (1.018–1.062) | <0.001 |
| INR | 0.501 (0.131–1.911) | 0.311 | ||
| TT (s, IQR) | 1.003 (0.998–1.008) | 0.207 | ||
| Univariate Regression | Multivariate Analysis | |||
|---|---|---|---|---|
| Variables | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| Gender (male) | 2.837 (1.037–7.079) | 0.025 | 2.564 (1.506–5.814) | 0.005 |
| AWMI | 13.052 (6.64–25.658) | <0.001 | 4.578 (2.155–9.728) | <0.001 |
| Ventricular aneurysm | 43.362 (25.925–72.525) | <0.001 | 22.253 (12.239–40.459) | <0.001 |
| Killip I | 0.378 (0.228–0.625) | <0.001 | 1.359 (0.459–4.022) | 0.579 |
| Killip II | 2.650 (1.558–4.509) | <0.001 | 1.868 (0.615–5.671) | 0.27 |
| NEUs (×109/L) | 1.056 (0.992–1.123) | 0.085 | ||
| LYMs (×109/L) | 0.658 (0.436–0.994) | 0.047 | 0.969 (0.627–1.498) | 0.887 |
| BUN (mmol/L) | 1.064 (1.004–1.042) | 0.037 | 0.998 (0.972–1.025) | 0.876 |
| D-dimer (mg/L) | 1.000 (1.004–1.042) | 0.017 | 1.059 (0.978–1.147) | 0.156 |
| AST (U/L) | 1.000 (1.000–1.001) | 0.023 | 1.000 (0.999–1.001) | 0.651 |
| ALT (U/L) | 1.001 (1.000–1.002) | 0.134 | ||
| PT (s) | 1.020 (0.998–1.043) | 0.080 | ||
| Prothrombin activity (%) | 1.026 (1.015–1.036) | <0.001 | 1.025 (1.018–1.062) | <0.001 |
| INR | 0.520 (0.998–1.575) | 0.052 | ||
| TT (s, IQR) | 1.004 (1.000–1.008) | 0.062 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huo, X.; Lian, Z.; Dang, P.; Zhang, Y. The Development of a Nomogram Predictive Model for Intracardiac Thrombosis Risk: A Study Based on Risk Factors in Patients with Acute Myocardial Infarction. Biomedicines 2025, 13, 679. https://doi.org/10.3390/biomedicines13030679
Huo X, Lian Z, Dang P, Zhang Y. The Development of a Nomogram Predictive Model for Intracardiac Thrombosis Risk: A Study Based on Risk Factors in Patients with Acute Myocardial Infarction. Biomedicines. 2025; 13(3):679. https://doi.org/10.3390/biomedicines13030679
Chicago/Turabian StyleHuo, Xiaowei, Zizhu Lian, Peizhu Dang, and Yongjian Zhang. 2025. "The Development of a Nomogram Predictive Model for Intracardiac Thrombosis Risk: A Study Based on Risk Factors in Patients with Acute Myocardial Infarction" Biomedicines 13, no. 3: 679. https://doi.org/10.3390/biomedicines13030679
APA StyleHuo, X., Lian, Z., Dang, P., & Zhang, Y. (2025). The Development of a Nomogram Predictive Model for Intracardiac Thrombosis Risk: A Study Based on Risk Factors in Patients with Acute Myocardial Infarction. Biomedicines, 13(3), 679. https://doi.org/10.3390/biomedicines13030679