Abstract
Osteoarthritis (OA) of the temporomandibular joint (TMJ) occurs spontaneously in humans and various animal species, including horses. In humans, obtaining tissue samples is challenging and clinical symptoms appear late in the disease progression. Therefore, genetically modified, induced, and naturally occurring animal models play a crucial role in understanding the pathogenesis and evaluating potential therapeutic interventions for TMJ OA. Among the naturally occurring models, the equine TMJ OA model is characterized by slow, age-related progression, a wide range of clinical examinations, and imaging modalities that can be performed on horses, as well as easy tissue and synovial fluid collection. The morphological and functional similarities of TMJ structures in both species make the equine model of TMJ OA an excellent opportunity to track disease progression and response to treatment. However, much work remains to be carried out to determine the utility of human TMJ OA biomarkers in horses. Among the main TMJ OA biomarkers, IL-1, IL-6, TGF-β, TNF-α, and PGE2 have been recently investigated in the equine model. However, the majority of biomarkers for cartilage degradation, chondrocyte hypertrophy, angiogenesis, and TMJ overload—as well as any of the main signaling pathways—have not been studied so far. Therefore, it would be advisable to focus further research on equine specimens, considering both mediators and signaling.
1. Introduction
Osteoarthritis (OA) stands out as the most prevalent degenerative disease affecting the temporomandibular joint (TMJ), manifesting spontaneously in humans [1] and various animal species, such as mice [2,3], guinea pigs [4], and horses [5,6,7,8,9,10]. TMJ OA is characterized as a chronic disease marked by degenerative alterations in cartilage, accompanied by reparative processes in the surrounding tissues [1,11,12,13,14]. As the disease causes severe pain [12], joint swelling, and joint stiffness [1], limitation of mandibular motion [13] and subsequently a decreased quality of life [14] may be expected. The etiology of TMJ OA is complex and multifactorial, generally attributed to factors such as mechanical overloading, abnormal occlusion, trauma, and stress [1,11,15]. However, the specific causes of impaired cartilage and subchondral bone in the TMJ remain unclear [14,16], necessitating further research.
In the research, obtaining tissue samples from humans with TMJ OA poses challenges, and clinical symptoms often manifest late in the disease progression [14]. Consequently, animal models of TMJ OA play a pivotal role in comprehending the pathogenesis and assessing potential therapeutic interventions [17,18]. Given the morphological and functional differences in the TMJ across species, it is acknowledged that no single animal species can serve as a comprehensive model for all aspects of human TMJ pathophysiology [19]. Animal models of TMJ OA are therefore categorized into five groups: genetically modified, induced (surgically, chemically, or non-invasively), and naturally occurring models, depending on whether animals undergo intervention or not [14,20,21]. Genetically modified mice offer valuable insights into the molecular basis of TMJ OA by allowing the direct observation of individual gene influences [12,16]. However, human TMJ OA pathogenesis involves multiple genes [22] and genetically modified mice may not fully replicate the intricate multi-gene interactions [14]. Surgical induction models employing mice, rats, rabbits, pigs, and sheep are common [14], with rabbits preferred due to favorable outcomes [23,24]. Chemically induced models involving mice, rats, rabbits [14], and horses [25] are also widely utilized, with rats preferred due to low costs and ease of management [26,27]. Rats are frequently employed in non-invasive models using mechanical loading due to their tolerance to such devices [28,29]. However, induced models typically operate on one TMJ [14,23,24,25,26,27,28,29], overlooking its bilateral nature [30]. Non-invasive models overlook this limitation but face challenges due to differences in occlusion, TMJ movements, and TMJ structure between rodents and humans [1,31]. Therefore, larger animals like pigs, sheep, and horses, with greater medio-lateral TMJ mobility, are increasingly recommended [12].
Amongst large animal models, only horses exhibit the naturally occurring slow progression of TMJ OA [5,6,7,8,9,10], closely resembling the disease progression in humans [14,32]. Moreover, horses, similarly to humans [33], experience intra-articular disc mineralization, fractures involving TMJ, and septic arthritis [6,7,8,34], offering a promising platform for translational research. The equine naturally occurring model of TMJ OA offers significant advantages including the elimination of the need for invasive procedures [14], minimization of the potential side effects [14], and providing a means to study the pathophysiology, biological markers, and therapeutic agents [33,35]. Consequently, the improvement of the equine naturally occurring model addresses the need for more responsive outcome measures for both symptom- and structure-modifying agents for human TMJ by developing and qualifying biomarkers to enable the development of disease-modifying therapeutic strategies [12,16]. On the other hand, the utility of the equine model of TMJ OA is evident in tracking the course of the disease in veterinary medicine, particularly in equine sports medicine. Diagnosis and treatment of equine TMJ OA is a major clinical challenge as TMJ OA may significantly impair the performance of equine athletes [36,37]. Despite the development of several equine models for peripheral joint OA [35], TMJ OA still presents deficiencies with inconsistency in the level of disease between animals [6] and challenges in establishing biomarkers and signaling pathways for tracking TMJ OA [5].
This review sought to provide a general comparison of TMJ OA in humans and horses. Then, this review aims to focus on summarizing the currently investigated markers and signaling pathways in TMJ OA, discussing the gaps in their state of the art within the context of the equine model of TMJ OA.
2. TMJ OA in Humans and Horses
The equine OA models are anatomically and pathophysiologically similar to humans, particularly in cartilage thickness, spontaneous OA occurrence, age-related progression, pain-related clinical symptoms, radiographic signs, imaging modalities used, risk factors for OA development, and similar intra-articular OA mediation [33]. In horses, the OA model of the TMJ is still poorly understood [38,39,40,41], in contrast to equine OA models of the peripheral joints. In recent well-published research, significant similarities between the human knee joint OA and the equine metacarpophalangeal (MCP) joint OA [21,32,35] and stifle joint OA [32,42,43] have been evidenced. Additionally, a racehorse model was established as a specific joint-loading model used to measure the impact of effort on knee OA development, since microstructural changes in articular cartilage due to overloading of the equine joint were evidenced [44,45]. As the OA may progress differently in different joints [46], more research is still needed in equine TMJ OA, especially in the area of markers and signaling pathways.
OA occurs spontaneously in humans and equines in both peripheral joints and the TMJ [1,5,6,7,8,9,12,15]. The occurrence of slowly progressing equine OA closely resembles the natural progression of human primary OA [32]. Moreover, spontaneous OA is a common clinical problem in both humans [12,13,33,47,48,49] and horses [7,8,37,38], also in the TMJ. Focusing on TMJ OA in humans, one can observe that clinical symptoms of TMJ OA have been reported in 40–75% of adults [13], 67% of adults with coexisting OA in other joints [48], and in more than 70% of older people [49]. In horses, radiographic signs of TMJ OA have been found in over 30% of examined horses [6]. Moreover, the frequency of TMJ OA increases with age in both humans [1,50,51] and horses [6,8,10]. Clinically asymptomatic horses accumulate changes in the TMJs with age [10], similar to those seen in the TMJs of other species, including humans [32]. Like humans, horses experience age-related degeneration in the form of intra-articular disc mineralization [6,7] and changes in intra-articular proinflammatory cytokine profiles [5].
The main manifestations of TMJ OA include damage and degeneration of the articular cartilage, accompanied by remodeling of the surrounding tissue, beginning with the subchondral bone and progressively involving the synovium and other soft tissues [14]. As a result, alterations may manifest in all articular structures, including the articular cartilage, articular disc, subchondral bone, synovium, joint capsule, ligaments, and periarticular muscles [1,15,17]. As in peripheral joints, the role of synovitis in the pathogenesis of OA has been proven to be similar in humans [52] and horses [53,54]; it can be suspected in the TMJ as well. Moreover, equine articular cartilage is highly comparable to that of humans [32]. In the equine stifle joint, the articular cartilage has been shown to be very similar in thickness and cellular structure, and the biochemical makeup and properties of the cartilage are comparable to the human knee joint [42,43]. Thus, horses have been used to investigate articular cartilage repair and osteochondral defects [21,53,55]. Although the articular surface of the mandibular condyle is covered with fibrous cartilage, consisting of a mass of collagen fibers, instead of hyaline cartilage [56], some similarities may be suspected. Focusing specifically on the TMJ, like humans, naturally occurring degenerative changes in the equine TMJ may impact the compressive stiffness of the intra-articular disc in a region-dependent fashion [57,58]. The composition and mechanical properties of the equine intra-articular disc of the TMJ may deteriorate depending on the horse’s age, the region of the TMJ, and the specific degenerative changes [9]. Continuing the discussion toward the bones, one may observe that horses provide a naturally occurring model to study bone remodeling, which leads to bone cysts and osteophyte formation [6,59].
Among the clinical symptoms of TMJ OA, pain and limited function are the primary reasons for patients to seek treatment. In humans, severe pain, eating difficulties [12], joint swelling, joint stiffness [1], and limited mandibular motion [13] are reported. In the case of horses, which do not report pain themselves, aversion behavior suggestive of pain [8] and problems with horse riding [36,37] are reported by owners or trainers. In clinical examinations, effusion of the affected TMJ and distortion of the masticatory cycle [8,41] are detected. Thus, regardless of the reporting method, similar clinical symptoms are reported in both species, similarly decreasing their quality of life [14,40]. The outcome of clinical TMJ examination is routinely supported by various imaging modalities including conventional radiography, high-resolution ultrasonography, computed tomography (CT), and magnetic resonance imaging (MRI) [14]. Currently, CT and MRI are the most widely used imaging modalities in both humans [1,51,60] and horses [6,61,62], making radiographic signs a key feature for diagnosing TMJ OA. Radiographic signs of the mandibular condyle and zygomatic process of the temporal bone include flattening of the surface, erosive resorption, irregularities of the joint surfaces, subchondral bone sclerosis, osteophyte formation, and cyst-like changes. Similar bone changes can be observed on CT images in both humans [51,63] and horses [6,7,41,59]. Cartilage defects can be visualized using arthroscopy, more often in horses [34,59,64] than in humans [65], and MRI, on the contrary, more often in humans [49,60,66,67,68] than in horses [62,69].
One may highlight the functional similarities between the human and horse TMJs. When considering TMJ load, the horse’s mastication cycle consists of an opening stroke, a closing stroke, and a power stroke [57,70]. The power stroke in horses is unimodal, involving a medio-lateral movement of the mandibles [57]. However, equine TMJs are also capable of latero-ventral movement of the working side during the opening stroke and a marked medio-dorsal movement of the working side during the power stroke [71]. This mastication type is much more similar to humans [72] than the mastication type observed in rodents [1]. The mandibular condyles of rodents extend antero-posteriorly, while in humans, they extend medio-laterally [31]. Thus, the mandibular condyle axis is transversal in humans for tridimensional motions, including opening, deduction, and propulsion, whereas it is sagittal in rodents for propulsion movement [72]. Like humans, the transversal axis of equine mandibular condyles provides tridimensional motions which are provided by the cooperation of the temporal muscle, masseter muscle, medial pterygoid muscle, and lateral pterygoid muscle [61,73]. Such a structure allows for adjustment of the masticatory cycle when compensation in the case of TMJ OA is required; therefore, horses with experimentally induced unilateral TMJ OA do not hesitate to eat and do not show significant pain on TMJ palpation [8,25]. Additionally, the biochemical composition of articular discs in horses [57,58] is similar to that of goats, pigs, bovines, and humans [19]. Moreover, the similarity also extends to the anisotropy of the composition and compressive stiffness of the articular disc. In horses, the orientation of disc anisotropy is similar to that in humans, albeit to a higher degree than observed in the human articular disc [9]. Thus, the regional variations in articular disc composition and compressive stiffness [9] align with the regional distribution of biomechanical stresses and preferred movement directions [57].
These morphological and functional similarities are in line with one fundamental mechanism of OA development, which is an ‘abnormal’ loading on ‘normal’ cartilage [35]. The second one, a ‘normal’ loading on ‘abnormal’ cartilage [35], required further research. It is still not known how the equine TMJ, including the intra-articular disc with ‘normal’ or ‘abnormal’ composition [57,58], withstands ‘normal’ or ‘abnormal’ medio-lateral loading during mastication [9]. Understanding the effect of compressibility on overall TMJ function may, through functional assessment and biomarker evaluation [12,16], shed new light on the pathophysiology of equine TMJ OA and its translation to humans [33]. Such investigations may involve the evaluation of OA biomarkers, which are most effectively obtained directly from the joint [21]. One may note that sampling synovial fluid, articular cartilage, and articular disc in the study of TMJ OA in humans is limited [14,35]. However, these specimens can be effectively investigated using equine OA models [74]. In contrast, the sampling of synovial fluid in the small joints of small animal models is not always feasible [32]. Although biomarkers can be measured from other specimens, such as blood or urine, their levels are influenced by other diseases or metabolic conditions. This limitation is also recognized in human clinical studies [33,49,51,65,66]. Therefore, every effort should be made to establish more and more biomarkers in the equine TMJ OA model.
Figure 1A–C summarize the main similarities between human and equine TMJ OA, while Figure 1D,E illustrate the main signaling pathways of TMJ OA initiation and progression, indicating molecules that can be used as TMJ OA biomarkers.
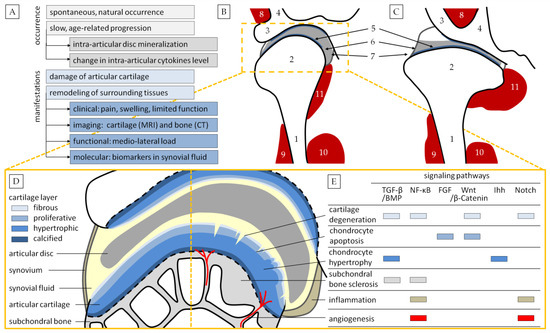
Figure 1.
Comparison of temporomandibular joint osteoarthritis (TMJ OA) in humans and horses. A concise summary of occurrence and manifestation (A). Schematic representation of the middle plane transverse section of TMJ in humans (B) and horses (C). 1. Ramus of the mandible; 2. mandibular condyle; 3. zygomatic process of the temporal bone; 4. squamous part of the temporal bone; 5. articular cartilage; 6. articular disc; 7. joint capsule with ligaments; 8. temporal muscle; 9. masseter muscle; 10. medial pterygoid muscle; 11. lateral pterygoid muscle. Schematic representation of normal TMJ (D) and TMJ OA (E). Abbreviations: TGF-β/BMP, transforming growth factor β/bone morphogenic protein signaling; NF-κB, nuclear factor kappaB signaling; FGF, fibroblast growth factor signaling; Wnt/β-Catenin signaling; Ihh, Indian hedgehog signaling; Notch signaling.
3. Biomarkers of TMJ OA
The TMJ function remains in balance with occlusion, thanks to remodeling, which is the essential biological response to TMJ loading [15]. The TMJ exhibits high adaptability to variable load, as its fibrocartilage is highly resistant to shear force [75]. However, when the load exceeds the joint adaptation level, degenerative changes may be initiated. Correlations between occlusal interferences, nonworking-side occlusal contacts, and TMJ OA in adult humans were demonstrated [76], indicating that excessive or prolonged TMJ overload may result in incorrect remodeling [15]. Thus ‘abnormal’ loading on ‘normal’ cartilage may be considered as one of the mechanisms of TMJ OA development [35]. On the other hand, when TMJ adaptability to load is reduced [15], ‘normal’ loading on ‘abnormal’ cartilage [35] may initiate a disruption in the remodeling of the TMJ [17].
‘Abnormal’ cartilage may be produced as a consequence of compromised chondrocyte activity and survival [12], leading to abnormal extracellular matrix (ECM) metabolism [77]. This results in fibrillation, erosion, and cracking in the superficial cartilage layer [14], remodeling of the subchondral bone [15,78], and hastening of the progression of TMJ OA [12]. Chondrocytes mediate the balance of the cartilage matrix [12], and their abnormal anabolic and catabolic activity [77] leads to disruption between ECM synthesis and degradation [12]. In the case of OA, the number of hypertrophic and apoptotic chondrocytes significantly increases [79,80]. Chondrocyte apoptosis results in a decrease in the total number of chondrocytes, creating space for angiogenesis [80]. Through apoptosis, the suppression of autophagy occurs. Autophagy protects chondrocytes against environmental alterations by destroying stored materials and releasing reusable tiny molecules, making it a crucial chondrocyte survival strategy [81]. Chondrocytes with a suppressed survival strategy release apoptotic bodies [80], constituting the origin of cartilage mineralization. This mineral deposition in the ECM [82] and osteoclast activity [15,68] are also stimulated by angiogenesis, so that newly created vessels enter the cartilage and are integrated with osteophytes [82]. Thus, vascular endothelial growth factor (VEGF), crucial for angiogenesis, is considered a key modulator of TMJ OA [82,83]. Hypertrophic chondrocytes induce the degradation of the ECM and calcification of cartilage [80], activating the complement system and the production of cartilage-degrading molecules. Since the cartilage ECM is mainly structured with collagen fibers, mostly type I and type II collagen [84], and proteoglycans [85], the synthesis of matrix metalloproteinases (MMPs, mainly MMP-3, 7, 8, 9, 13, 16, 17, and 19), and other degradative molecules such as a disintegrin and metalloproteinase production with thrombospondin motifs (ADAMTS, mainly ADAMTS-4 and -5) and prostaglandin E2 (PGE2) initiate collagen and proteoglycan degradation in articular cartilage [12,15,85,86].
Cartilage modeling is often accompanied by bone remodeling related to a decrease in osteoblasts’ activity and amount, as well as an increase in osteoclasts’ activity [87,88]. Osteoblasts participate in the subchondral bone sclerotization so that newly created bone has a high density and volume but low mineralization [89], whereas osteoclasts are involved in bone resorption [90]. Moreover, osteocytes, which are sensitive to joint mechanical loading [91], increase MMP secretion in response to overload, thus promoting the degeneration of the bone matrix and leading to subchondral bone remodeling [92]. On the other hand, the decrease in the sensitivity of chondrocytes to mechanical loading is mediated by the decreased secretion of high mobility group protein B2 (HMGB2) [93] and the activation of hypoxia-induced transcription factor-1 (HIF-1), which promote osteoclastogenesis and VEGF expression [94,95]. VEGF, produced by chondrocytes, stimulates autocrinely the production of MMP-13 and reduces the production of tissue matrix metalloproteinase inhibitor (TIMP-1) [82,94], leading to cartilage degradation [15,68].
These processes occurring in articular cartilage and subchondral bone are accompanied by an inadequate inflammatory response, where immune cells release inflammatory mediators, such as cytokines and chemokines [15,78]. Among them, interleukin 12 (IL-12) [96] and IL-1β [96,97,98,99,100,101,102] seems to be the most important. However, concentrations of IL-2, IL-6, IL-17, IL-18, tumor necrosis factor (TNF-α and TNF-β), and interferon (IFN-γ) were also higher in the synovial fluid from patients with TMJ OA than that of healthy ones [12,96]. IL-1β and TNF-α activate osteoclasts leading to bone resorption [97] and upregulated MMP production in chondrocytes suppressing ECM synthesis, thus contributing to articular and disc cartilage degradation [98]. IL-1β and TNF-α [99], as well as PGE2 [103], act in TMJ pain sensation by stimulating nociceptive receptors. IL-1β also stimulates synoviocytes to monocyte chemoattractant protein-1 (MCP-1) production [100], triggering the persistence of inflammation [101]. IL-1β and IL-6 stimulate VEGF transcription in the nucleus and, thus, increase angiogenesis [102]. Due to increased angiogenesis, all these molecules may act not only locally but also by distribution throughout the entire joint [82].
The deregulation of chondrocytes, remodeling of subchondral bone, and activation of immune cells occur as a consequence of a sequence of molecular changes in the TMJ’s tissues. The six main signaling pathways in TMJ OA include transforming growth factor β (TGF-β)/bone morphogenic protein (BMP) signaling, nuclear factor kappaB (NF-κB) signaling, fibroblast growth factor (FGF) signaling, Wnt/β-Catenin signaling, Indian hedgehog (Ihh) signaling, and Notch signaling [12,16]. Table 1 summarizes their members, biological role, activation effects, and role in TMJ OA pathogenesis.

Table 1.
Summary of the six main signaling pathways in temporomandibular osteoarthritis (TMJ OA).
3.1. Search Strategies and Selection Process of Equine TMJ OA Biomarkers
Summarizing the main biomarkers of TMJ OA and considering their role in TMJ OA pathogenesis (Table 2), the following keywords for literature search were selected: ADAMTS-5 (ADAMTS), Col2, HIF-1, HMGB2, Ihh, IL-1β, IL-6, IL-12 (IL), MMP-3, MMP-13 (MMP), PGE2, PTHrP, TGF-β (TGF), TIMP-1 (TIMP), TNF-α (TNF), and VEGF. The keyword list was then extended by signaling pathway abbreviations: TGF-β/BMP (TGF, BMP), NF-κB, FGF, Wnt/β-Catenin (Wnt, β-Catenin), Ihh, and Notch. Duplicates (TGF, Ihh) were removed.
Table 2.
Summary of main biomarkers in temporomandibular osteoarthritis (TMJ OA).
A literature search was performed using major information sources, including PubMed, Google Scholar, and ScienceDirect. The search queries involved biomarker keyword searches in combination with (temporomandibular* or TMJ*) and (horse* or equine*) and (arthritis* or osteoarthritis* or OA*), (degeneration* or disease*). Each keyword ((ADAMTS-5* or ADAMTS* or a disintegrin and metalloproteinase production with thrombospondin motifs*), (Col2* or collagen type II*), (HIF-1* or hypoxia-induced transcription factor*), (HMGB2* or high mobility group protein), (IL-1β* or IL* or interleukin*), (IL-6* or IL* or interleukin*), (IL-12* or IL* or interleukin*), (MMP-3* or MMP* or matrix metalloproteinase*), (MMP-13* or MMP* or matrix metalloproteinase*), (PGE2* or prostaglandin E2*), (PTHrP* or parathyroid hormone-related peptide*), (TIMP-1* or TIMP* or tissue matrix metalloproteinase inhibitors*), (TNF-α* or TNF* or tumor necrosis factor*), (VEGF* or vascular endothelial growth factor*), (TGF-β/BMP* or TGF-β* or TGF* or transforming growth factor* or BMP* or bone morphogenic protein*), NF-κB, FGF, (Wnt/β-Catenin* or Wnt* or β-Catenin*), Ihh, Notch) was combined separately. Due to the low number of gathered records, search queries involving combinations with (temporomandibular* or TMJ*) and (horse* or equine*) were performed. Additionally, the manual searches of reference lists from the included articles were performed.
A total of 52 articles were gathered from the period until 2023. Duplicates were removed. The inclusion criterion was the English language of articles. The exclusion criteria were article not related to horses, article not relevant to the aims of this review, published conference abstracts, and articles in journals that did not have a documented, transparent peer-review process. From the gathered articles, only four covered the review area of equine TMJ OA biomarkers.
3.2. Biomarkers of Equine TMJ OA
Most equine TMJ research focuses on joint morphology and function [10,38,39,40,41,57,58] and imaging modalities [6,7,41,61,62], as well as practical implications and treatment [34,36,37,59,63]. Only a few key biomarkers of equine TMJ OA [5,9,25,137] have been investigated and they are summarized in Table 3. While these studies effectively address the clinical needs of equine medicine, the similarity to the underlying molecular components of human TMJ OA is still poorly understood.
Table 3.
Summary of biomarkers investigated in temporomandibular osteoarthritis (TMJ OA) in equine specimens.
Carmalt et al. [5] investigated IL-1, IL-6, IL-8, TNF-α, and TGF-β in the synovial fluid collected from clinically healthy horses. The horses were grouped in two ways: based on age and based on dental diseases. This grouping was guided by the equine dentistry hypothesis, which mirrors concepts in human dentistry [138], suggesting that dental diseases may lead to clinically manifested TMJ OA, including pain and reduced performance. However, this study failed to confirm the hypothesis, as no dental-disease-related differences were demonstrated in any of the examined biomarkers. In this study, the concentrations of IL-8 and TGF-β1 increased with age. The authors speculated that this rise in IL-8 and TGF-β concentration could indicate low-grade inflammation associated with dental wearing, even in the absence of typical OA clinical symptoms. However, it is worth noting that not all TMJs underwent a detailed examination and they were not grouped based on OA symptoms. Therefore, establishing a direct relationship with TMJ OA may be considered controversial [5].
Cota et al. [9] assessed changes in the composition and mechanical properties of the articular disc in relation to location, age, and OA severity. This post mortem study aimed to characterize the articular disc to enhance the understanding of TMJ function and the potential role of articular disc degradation in equine TMJ OA. Among the evaluated indicators of biochemical composition, histological structure, and compressive properties, sulfated glycosaminoglycan (GAG) and total collagen (TC) may be considered as informative biomarkers, if not main ones. The authors observed regional variations in articular disc composition and compressive stiffness, with increasing GAG content related to increasing compressive stiffness. Thus, the authors speculated that, in horses, the caudal part of the TMJ may be more susceptible to degeneration. In this study, the articular disc exhibited increasing GAG content and compressive stiffness with increasing age, and a region-specific increase in GAG content associated with OA severity [9].
Carmalt et al. [25] expanded on their previous research [5] by employing a chemically induced OA model. The authors investigated IL-6, TNF-α, TGF-β, and total protein (TP) in the synovial fluid collected from the TMJ and the MCP joint, known to be frequently affected by OA. In this study, TNF-α concentration was higher, whereas TP concentration was lower, in the TMJ OA compared to the control TMJ. However, both biomarker concentrations were higher in the TMJ OA than in the MCP OA. In contrast, TGF-β concentration was lower in the TMJ OA than in the MCP OA. Thus, the authors suggested that the TMJ responds differently to acute OA than peripheral joints but they were unable to precisely explain the reason for the observed differences, suggesting that further research concerning MMPs and TLR-4 is required [25]. Therefore, we can support this suggestion by expanding research on the NF-κB signaling pathway, since this pathway is activated by TLR-4 and may regulate the transcription of MMPs, ILs, and TNF-α [109,113,129].
Pereira et al. [137] explored a load-induced OA model to mimic the TMJ stresses typical of routine equine dental care. Considering that overload may initiate degenerative changes in the TMJ [15,76], the authors hypothesized that the application of a full-mouth speculum for 60 min may lead to clinical symptoms of TMJ OA. Among the main biomarkers, the authors investigated PGE2 in the synovial fluid and, additionally, TP, GAG, chondroitin sulfate (CS), hyaluronic acid (HA), and white blood cells (WBC) were also assessed in the synovial fluid. In this study, only WBC count was higher after load induction. However, the lack of clinical symptoms and thermographic signs of OA suggests that the used load-time was too short for disease induction, and such a load remains in the range of TMJ adaptability. This observation is beneficial for horse owners and practitioners, ensuring the safety and lack of PGE2-mediated pain during dental care procedures. The authors concluded that the used load does not indicate the occurrence of turnover changes in articular cartilage; however, they suggested the need for monitoring each horse subjected to prolonged full-mouth speculum placement [137]. We can support this suggestion by using overload biomarkers, including HMGB2, HIF-1, VEGF, MMPs, and TIMP-1 [82,93,94,95], which may make it feasible to expand further research on the safety of routine and interventional equine dental care.
4. Limitations and Future Directions
Despite the discussed advantages of the equine TMJ OA model, the following disadvantages should be considered. Recently, challenges such as the difficulty and expense of housing and managing horses [139], as well as the high cost, long research period, and slow disease progression [14], have been highlighted. While it is acknowledged that horses represent an expensive experimental model, the numerous studies referenced focusing on both equine athletes and experimental horses suggest that they are manageable subjects [5,6,7,8,25,34,36,37,38,39,40,41,59,61,62,64,137].
However, none of the previous reviews of animal models have highlighted the functional differences between human and equine TMJ. Different mandibular movements occur during mastication in humans, rodents, carnivores, and herbivores [140], while horses represent typical herbivores. The most significant difference is the restriction in lateral movement, which is most strongly expressed in rodents [35], present in carnivores [141], and least expressed in herbivores, while horses are capable of both latero-ventral movements and medio-dorsal movements [70,71]. Moreover, equine masticatory forces are higher [70] than those in humans [142], and both differ depending on the kind of food intake [71,143]. Horses usually consume roughage such as grass and hay, along with concentrates, most often based on oats. Harder additions may include a piece of dry bread, a carrot, and a horse cookie [71], whereas the human diet, considered in chewing studies, is much more varied [143,144,145]. Despite these and other functional differences, animal studies serve as a source for new insights into human TMJ diseases or for targeting novel treatment strategies [140].
The relatively high prevalence of TMJ OA and the longer lifespan of horses, compared to other domestic animals, offer an opportunity to examine potential age- and OA-related changes in the TMJ, making it easier to form research groups of different ages rather than tracking the slow progression of the disease over time [9]. Furthermore, recent developments in equine medicine, including the availability of helical fan beam CT imaging of the equine head in a standing position [146,147], have significantly increased the suitability of horses as model animals for TMJ OA. Therefore, the equine naturally occurring model appears to be feasible for studying TMJ OA, including cartilage degradation and bone remodeling. With improved biomarker evaluation, TMJ OA can provide valuable evidence for studying the pathogenesis of TMJ OA at different ages.
One may observe that the value of animal models mainly depends on how well they correspond with human disease. Therefore, improving animal TMJ OA models may be considered the primary means of testing potential therapeutic agents to determine their potential efficacy in this specific disease [14,16]. On the other hand, evaluating treatments in clinical equine practice [6,7,34,36,37,40,59,64] faces similar challenges to those in humans [35]. In both cases, high-quality randomized, controlled trials with well-validated outcome measures are needed to improve the investigation of the efficacy of TMJ OA treatment strategies.
Currently, the treatments of TMJ OA mainly aim to reduce pain, restore TMJ function, and improve the quality of life of patients [1,15,19,67]. Given the limited understanding of TMJ OA pathogenesis and the limited regeneration possibility of the articular cartilage, no clinically approved therapeutics are still available to restore the TMJ structure [1,45,89]. Giving the example of a possible therapeutic target in the signaling pathway of TMJ OA, one may observe that an inhibition of TGF-β signaling may delay the effect of mechanical load on cartilage degradation in TMJ OA [148]. Inhibition of NF-κB signaling protects condylar cartilage from degradation [149] and ameliorates chondrocytes during TMJ inflammation [150]. The inhibition of FGF signaling in chondrocytes delays and ameliorates TMJ OA progression by promotion of the autophagic activity of chondrocytes [118]. The inhibition of Wnt/β-catenin signaling promotes cell proliferation and inhibits cell death in articular cartilage [122]. The inhibition of Ihh signaling prevents chondrocyte differentiation and maturation [151] and chondrocyte terminal differentiation in TMJ OA, delaying the overload OA lesions [124]. Finally, the inhibition of Notch signaling delays the progression of cartilage damage in TMJ OA [146].
However, all these studies were performed on mice [118,122,148,149,150,151,152] and rat [124,149] models, focusing on the identification of symptom-modifying OA drug (SMOAD) effects rather than the disease-modifying activity of the drug [35]. Thus, there is a need to develop pre-clinical animal models for research on a disease-modifying OA drug (DMOAD) that will better correspond with human TMJ OA progression and outcomes after treatment [14,19,35]. Such models should include long-term cartilage and bone structure recovery, biomechanical analyses concerning functional joint recovery [14], and validatable and detailed imaging modalities, as well as synovial fluid and serum biomarker evaluation [12,16,35] to define DMOAD activity. Moreover, the use of recently available multiplex panels rather than individual ELISAs and non-targeted transcriptomic techniques enable the expanded evaluation of OA biomarkers [153,154,155], so also TMJ OA biomarkers [156,157].
As equine sports medicine develops rapidly parallelly to human medicine, the equine TMJ OA model potentially offers high-quality research and well-validated outcome measures using, for example, dual-energy, multidetector standing fan-beam CT and high-field MRI. Therefore, every effort should be made to fill the gaps in the biomarkers and signaling pathways of equine research, and establish more multi-factor models of equine TMJ OA. So, the hope is that further studies on TMJ OA in horses provide great potential for targets of regenerative treatment for advancement in both human and equine medicine.
5. Conclusions
Different types of animal models simulate different pathological expressions of TMJ OA and have their unique characteristics. Currently, mice, rats, and rabbits are commonly used in the study of TMJ OA; however, naturally occurring large-animal models are still needed for preclinical studies to evaluate the clinical processes and treatment of TMJ OA. Among the naturally occurring models, equine TMJ OA is characterized by spontaneous OA occurring; morphological and functional similarities to human TMJ structures; and a wide range of clinical examinations and imaging modalities that can be performed on horses. However, the numerous biomarkers of disease progression in equine TMJ OA model require further research. Among the main TMJ OA biomarkers, IL-1, IL-6, TGF-β, TNF-α, and PGE2 have recently been investigated in the equine model. However, the majority of biomarkers for cartilage degradation (MMPs, TIMP-1, ADAMTSs), chondrocyte apoptosis (TNF-α) and hypertrophy (Col2, Ihh, PTHrP), angiogenesis (VEGF), and TMJ overload (HMGB2, HIF-1, VEGF, MMPs, TIMP-1), as well as the main signaling pathways (TGF-β/BMP, NF-κB, FGF, Wnt/β-Catenin, Ihh, and Notch), have not been studied so far. Considering the disadvantages of equine TMJ OA, mainly related to high costs and long disease progression, it would be advisable to focus further research on horse specimens, considering HMGB2, HIF-1, VEGF, MMPs, TIMP-1, and ADAMTSs, as well as NF-kB and Ihh signaling pathways. Although TMJ OA is underinvestigated in equine medicine, it has great potential in targeted treatment research.
Author Contributions
Conceptualization, T.J., W.B. and M.D.; methodology, T.J. and M.D.; validation, B.T. and M.K.; formal analysis, T.J., K.S., J.B. and M.D.; investigation, T.J., B.T., M.K., K.S., J.B. and M.D.; data curation, T.J.; writing—original draft preparation, T.J., B.T. and M.D.; writing—review and editing, T.J., B.T., M.K., W.B., K.S., J.B. and M.D.; visualization, M.D.; supervision, B.T. and W.B; project administration, T.J. and M.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Wang, X.D.; Zhang, J.N.; Gan, Y.H.; Zhou, Y.H. Current Understanding of Pathogenesis and Treatment of TMJ Osteoarthritis. J. Dent. Res. 2015, 94, 666–673. [Google Scholar] [CrossRef] [PubMed]
- Yamashita-Futani, Y.; Jokaji, R.; Ooi, K.; Kobayashi, K.; Kanakis, I.; Liu, K.; Kawashiri, S.; Bou-Gharios, G.; Nakamura, H. Metalloelastase-12 Is Involved in the Temporomandibular Joint Inflammatory Response as Well as Cartilage Degradation by Aggrecanases in Str/Ort Mice. Biomed. Rep. 2021, 14, 51. [Google Scholar] [CrossRef]
- Cui, C.; Zheng, L.; Fan, Y.; Zhang, J.; Xu, R.; Xie, J.; Zhou, X. Parathyroid Hormone Ameliorates Temporomandibular Joint Osteoarthritic-like Changes Related to Age. Cell Prolif. 2020, 53, E12755. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Lu, H.; Yu, F.; Zhou, Y. Trend of Cadherin-11 Expression and its Impact on Cartilage Degradation in the Temporomandibular Joints of Guinea Pigs with Spontaneous Osteoarthritis. J. Oral Pathol. Med. 2020, 45, 534–538. [Google Scholar] [CrossRef]
- Carmalt, J.L.; Gordon, J.R.; Allen, A.L. Temporomandibular joint cytokine profiles in the horse. J. Vet. Dent. 2006, 23, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Carmalt, J.L.; Kneissl, S.; Rawlinson, J.E.; Zwick, T.; Zekas, L.; Ohlerth, S.; Bienert-Zeit, A. Computed tomographic appearance of the temporomandibular joint in 1018 asymptomatic horses: A multi-institution study. Vet. Radiol. Ultrasound 2016, 57, 237–245. [Google Scholar] [CrossRef] [PubMed]
- Smyth, T.; Allen, A.L.; Carmalt, J.L. Clinically significant, nontraumatic, degenerative joint disease of the temporomandibular joints in a horse. Equine Vet. Educ. 2017, 29, 72–77. [Google Scholar] [CrossRef]
- Smyth, T.T. Osteoarthritis of the Equine Temporomandibular Joint. 2017. Available online: http://hdl.handle.net/10388/7939 (accessed on 15 November 2023).
- Cota, J.M.G.; Leale, D.M.; Arzi, B.; Cissell, D.D. Regional and disease-related differences in properties of the equine temporomandibular joint disc. J. Biomech. 2019, 82, 54–61. [Google Scholar] [CrossRef]
- Smyth, T.T.; Allen, A.L.; Carmalt, J.L. Histologic Assessment of Age-Related Changes in the Temporomandibular Joints of Horses. Am. J. Vet. Res. 2019, 80, 1107–1113. [Google Scholar] [CrossRef]
- Monasterio, G.; Castillo, F.; Betancur, D.; Hernández, A.; Flores, G.; Díaz, W.; Hernández, M.; Vernal, R. Osteoarthritis of the Temporomandibular Joint: Clinical and Imagenological Diagnosis, Pathogenic Role of the Immuno-Inflammatory Response, and Immunotherapeutic Strategies Based on T Regulatory Lymphocytes. In Temporomandibular Joint Pathology-Current Approaches and Understanding; IntechOpen: London, UK, 2018. [Google Scholar]
- Lu, K.; Ma, F.; Yi, D.; Yu, H.; Tong, L.; Chen, D. Molecular signaling in temporomandibular joint osteoarthritis. J. Orthop. Transl. 2022, 32, 21–27. [Google Scholar] [CrossRef]
- Alzarea, B.K. Temporomandibular disorders (TMD) in edentulous patients: A review and proposed classification (dr. Bader’s classification). J. Clin. Diagn. Res. 2015, 9, ZE06–ZE09. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; An, Y.; Zhou, L.; Wu, F.; Wu, G.; Wang, J.; Chen, L. Animal models of temporomandibular joint osteoarthritis: Classification and selection. Front. Physiol. 2022, 13, 859517. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, E.; Detamore, M.S.; Mercuri, L.G. Degenerative Disorders of the Temporomandibular Joint: Etiology, Diagnosis, and Treatment. J. Dent. Res. 2008, 87, 296–307. [Google Scholar] [CrossRef] [PubMed]
- Cardoneanu, A.; Macovei, L.A.; Burlui, A.M.; Mihai, I.R.; Bratoiu, I.; Rezus, I.I.; Rezus, E. Temporomandibular joint osteoarthritis: Pathogenic mechanisms involving the cartilage and subchondral bone, and potential therapeutic strategies for joint regeneration. Int. J. Mol. Sci. 2022, 24, 171. [Google Scholar] [CrossRef]
- Vapniarsky, N.; Huwe, L.W.; Arzi, B.; Houghton, M.K.; Wong, M.E.; Wilson, J.W.; Hatcher, D.C.; Hu, J.C.; Athanasiou, K.A. Tissue Engineering toward Temporomandibular Joint Disc Regeneration. Sci. Transl. Med. 2018, 10, eaaq1802. [Google Scholar] [CrossRef]
- Liu, Q.; Yang, H.; Zhang, M.; Zhang, J.; Lu, L.; Yu, S.; Wu, Y.; Wang, M. Initiation and Progression of Dental-Stimulated Temporomandibular Joints Osteoarthritis. Osteoarthr. Cartil. 2021, 29, 633–642. [Google Scholar] [CrossRef]
- Almarza, A.J.; Brown, B.N.; Arzi, B.; Ângelo, D.F.; Chung, W.; Badylak, S.F.; Detamore, M. Preclinical animal models for temporomandibular joint tissue engineering. Tissue Eng. Part B Rev. 2018, 24, 171–178. [Google Scholar] [CrossRef]
- Lampropoulou-Adamidou, K.; Lelovas, P.; Karadimas, E.V.; Liakou, C.; Triantafillopoulos, I.K.; Dontas, I.; Papaioannou, N.A. Useful Animal Models for the Research of Osteoarthritis. Eur. J. Orthop. Surg. Traumatol. 2014, 24, 263–271. [Google Scholar] [CrossRef]
- McCoy, A.M. Animal Models of Osteoarthritis. Vet. Pathol. 2015, 52, 803–818. [Google Scholar] [CrossRef]
- Pitsillides, A.A.; Beier, F. Cartilage Biology in Osteoarthritis-Lessons from Developmental Biology. Nat. Rev. Rheumatol. 2011, 7, 654–663. [Google Scholar] [CrossRef]
- Imai, H.; Sakamoto, I.; Yoda, T.; Yamashita, Y. A Model for Internal Derangement and Osteoarthritis of the Temporomandibular Joint with Experimental Traction of the Mandibular Ramus in Rabbit. Oral Dis. 2001, 7, 185–191. [Google Scholar] [CrossRef]
- Saito, Y.; Tsutsui, T.; Takayama, A.; Moroi, A.; Yoshizawa, K.; Ueki, K. Effect of Low-Intensity Pulsed Ultrasound on Injured Temporomandibular Joints with or without Articular Disc Removal in A Rabbit Model. J. Dent. Sci. 2021, 16, 287–295. [Google Scholar] [CrossRef]
- Carmalt, J.L.; Bell, C.D.; Tatarniuk, D.M.; Suri, S.S.; Singh, B.; Waldner, C. Comparison of the response to experimentally induced short-term inflammation in the temporomandibular and metacarpophalangeal joints of horses. Am. J. Vet. Res. 2011, 72, 1586–1591. [Google Scholar] [CrossRef]
- Xu, L.; Guo, H.; Li, C.; Xu, J.; Fang, W.; Long, X. A Time-dependent Degeneration Manner of Condyle in Rat CFA-Induced Inflamed TMJ. Am. J. Transl. Res. 2016, 8, 556–567. [Google Scholar] [PubMed]
- Xu, T.; Xu, G.; Gu, Z.; Wu, H. Hedgehog Signal Expression in Articular Cartilage of Rat Temporomandibular Joint and Association with Adjuvant-Induced Osteoarthritis. J. Oral Pathol. Med. 2017, 46, 284–291. [Google Scholar] [CrossRef]
- Li, Y.; Yang, J.; Liu, Y.; Yan, X.; Zhang, Q.; Chen, J.; Zhang, Q.; Yuan, X. Inhibition of mTORC1 in the Rat Condyle Subchondral Bone Aggravates Osteoarthritis Induced by the Overly Forward Extension of the Mandible. Am. J. Transl. Res. 2021, 13, 270–285. [Google Scholar]
- Zou, Y.; Cai, S.; Lin, H.; Cai, J.; Zheng, D.L.; Lu, Y.G.; Xu, L. Experimental functional shift-induced osteoarthritis-like changes at the TMJ and altered integrin expression in a rat model. Ann. N. Y. Acad. Sci. 2022, 1511, 210–227. [Google Scholar] [CrossRef] [PubMed]
- Cohen, W.A.; Servais, J.M.; Polur, I.; Li, Y.; Xu, L. Articular Cartilage Degeneration in the Contralateral Non-surgical Temporomandibular Joint in Mice with A Unilateral Partial Discectomy. J. Oral Pathol. Med. 2014, 43, 162–165. [Google Scholar] [CrossRef] [PubMed]
- Bermejo, A.; González, O.; González, J.M. The Pig as an Animal Model for Experimentation on the Temporomandibular Articular Complex. Oral Surg. Oral Med. Oral Pathol. 1993, 75, 18–23. [Google Scholar] [CrossRef]
- Kuyinu, E.L.; Narayanan, G.; Nair, L.S.; Laurencin, C.T. Animal models of osteoarthritis: Classification, update, and measurement of outcomes. J. Orthop. Surg. Res. 2016, 11, 19. [Google Scholar] [CrossRef]
- Almarza, A.J.; Mercuri, L.G.; Arzi, B.; Gallo, L.M.; Granquist, E.; Kapila, S.; Detamore, M.S. Temporomandibular Joint Bioengineering Conference: Working together toward improving clinical outcomes. J. Biomech. Eng. 2020, 142, 020801. [Google Scholar] [CrossRef]
- Elzer, E.J.; Wulster, K.B.; Richardson, D.W.; Ortved, K.F. Standing arthroscopic treatment of temporomandibular joint sepsis in a horse. J. Vet. Dent. 2020, 37, 94–99. [Google Scholar] [CrossRef]
- McIlwraith, C.W.; Frisbie, D.D.; Kawcak, C.E. The horse as a model of naturally occurring osteoarthritis. Bone Jt. Res. 2012, 1, 297–309. [Google Scholar] [CrossRef]
- Jørgensen, E.; Christophersen, M.T.; Kristoffersen, M.; Puchalski, S.; Verwilghen, D. Does temporomandibular joint pathology affect performance in an equine athlete? Equine Vet. Educ. 2015, 27, 126–130. [Google Scholar] [CrossRef]
- Carmalt, J.L. Equine poor performance: The logical, progressive, diagnostic approach to determining the role of the temporomandibular joint. J. Am. Vet. Med. Assoc. 2023, 262, 397–404. [Google Scholar] [CrossRef]
- Baker, G.J. Equine temporomandibular joints (TMJ): Morphology, function and clinical disease. AAEP Proc. 2002, 48, 442–447. [Google Scholar]
- Ramzan, P. The temporomandibular joint: Component of clinical complexity. Equine Vet. J. 2006, 38, 102–104. [Google Scholar] [CrossRef]
- Carmalt, J.L. Equine temporomandibular joint (TMJ) disease: Fact or fiction? Equine Vet. Educ. 2014, 26, 64–65. [Google Scholar] [CrossRef]
- Carmalt, J.L.; Simhofer, H.; Bienert-Zeit, A.; Rawlinson, J.E.; Waldner, C.L. The association between oral examination findings and computed tomographic appearance of the equine temporomandibular joint. Equine Vet. J. 2017, 49, 780–783. [Google Scholar] [CrossRef]
- Frisbie, D.D.; Cross, M.W.; McIlwraith, C.W. A comparative study of articular cartilage thickness in the stifle of animal species used in human pre-clinical studies compared to articular cartilage thickness in the human knee. Vet. Comp. Orthop. Traumatol. 2006, 19, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Malda, J.; Benders, K.E.; Klein, T.J.; de Grauw, J.C.; Kik, M.J.; Hutmacher, D.W.; Saris, D.B.; van Weeren, P.R.; Dhert, W.J. Comparative study of depth-dependent characteristics of equine and human osteochondral tissue from the medial and lateral femoral condyles. Osteoarthr. Cartil. 2012, 20, 1147–1151. [Google Scholar] [CrossRef]
- Norrdin, R.W.; Kawcak, C.E.; Capwell, B.A.; McIlwraith, C.W. Subchondral bone failure in an equine model of overload arthrosis. Bone 1998, 22, 133–139. [Google Scholar] [CrossRef]
- Turley, S.M.; Thambyah, A.; Riggs, C.M.; Firth, E.C.; Broom, N.D. Microstructural changes in cartilage and bone related to repetitive overloading in an equine athlete model. J. Anat. 2014, 224, 647–658. [Google Scholar] [CrossRef]
- Nazet, U.; Neubert, P.; Schatz, V.; Grässel, S.; Proff, P.; Jantsch, J.; Schröder, A.; Kirschneck, C. Differential gene expression response of synovial fibroblasts from temporomandibular joints and knee joints to dynamic tensile stress. J. Orofac. Orthop. 2022, 83, 361–375. [Google Scholar] [CrossRef]
- Murphy, M.K.; MacBarb, R.F.; Wong, M.E.; Athanasiou, K.A. Temporomandibular joint disorders: A review of etiology, clinical management, and tissue engineering strategies. Int. J. Oral Maxillofac. Implants. 2013, 28, e393. [Google Scholar] [CrossRef]
- Abrahamsson, A.K.; Kristensen, M.; Arvidsson, L.Z.; Kvien, T.K.; Larheim, T.A.; Haugen, I.K. Frequency of temporomandibular joint osteoarthritis and related symptoms in a hand osteoarthritis cohort. Osteoarthr. Cartil. 2017, 25, 654–657. [Google Scholar] [CrossRef] [PubMed]
- Schmitter, M.; Essig, M.; Seneadza, V.; Balke, Z.; Schroder, J.; Rammelsberg, P. Prevalence of clinical and radiographic signs of osteoarthrosis of the temporomandibular joint in an older persons community. Dentomaxillofacial Radiol. 2010, 39, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Haskin, C.L.; Milam, S.B.; Cameron, I.L. Pathogenesis of Degenerative Joint Disease in the Human Temporomandibular Joint. Crit. Rev. Oral Biol. Med. 1995, 6, 248–277. [Google Scholar] [CrossRef]
- Zhao, Y.P.; Zhang, Z.Y.; Wu, Y.T.; Zhang, W.L.; Ma, X.C. Investigation of the clinical and radiographic features of osteoarthrosis of the temporomandibular joints in adolescents and young adults. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2011, 111, e27–e34. [Google Scholar] [CrossRef]
- Sellam, J.; Bernbaum, F. The role of synovitis in pathophysiology and clinical symptoms of osteoarthritis. Nature Rev. Rheum. 2010, 6, 625–635. [Google Scholar] [CrossRef] [PubMed]
- McIlwraith, C.W. Frank Milne Lecture: From arthroscopy to gene therapy: 30 years of looking in joints. Am. Assoc. Equine Pract. 2005, 51, 65–113. [Google Scholar]
- Trumble, T.N.; Trotter, G.W.; Oxford, J.R.; McIlwraith, C.W.; Cammarata, S.; Goodnight, J.L.; Billinghurst, R.C.; Frisbie, D.D. Synovial fluid gelatinase concentrations and matrix metalloproteinase and cytokine expression in naturally occurring joint disease in horses. Am. J. Vet. Res. 2001, 62, 1467–1477. [Google Scholar] [CrossRef] [PubMed]
- McIlwraith, C.W.; Fortier, L.A.; Frisbie, D.D.; Nixon, A.J. Equine models of articular cartilage repair. Cartilage 2011, 2, 317–326. [Google Scholar] [CrossRef] [PubMed]
- Toller, P.A. Temporomandibular Arthropathy. Proc. R. Soc. Med. 1974, 67, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Adams, K.; Schulz-Kornas, E.; Arzi, B.; Failing, K.; Vogelsberg, J.; Staszyk, C. Functional anatomy of the equine temporomandibular joint: Collagen fiber texture of the articular surfaces. Vet. J. 2016, 217, 58–64. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Adams, K.; Schulz-Kornas, E.; Arzi, B.; Failing, K.; Vogelsberg, J.; Staszyk, C. Functional anatomy of the equine temporomandibular joint: Histological characteristics of the articular surfaces and underlining tissues. Vet. J. 2018, 239, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Carmalt, J.L.; Reisbig, N.A. Arthroscopic treatment of bilateral mandibular condylar cysts and associated osteoarthritis of the temporomandibular joints in a horse. Equine Vet. Educ. 2022, 34, e352–e358. [Google Scholar] [CrossRef]
- Talmaceanu, D.; Lenghel, L.M.; Bolog, N.; Hedesiu, M.; Buduru, S.; Rotar, H.; Baciut, M.; Baciut, G. Imaging Modalities for Temporomandibular Joint Disorders: An Update. Clujul Med. 2018, 91, 280–287. [Google Scholar] [CrossRef]
- Rodríguez, M.J.; Latorre, R.; Lopez-Albors, O.; Soler, M.; Aguirre, C.; Vázquez, J.M.; Agut, A. Computed tomographic anatomy of the temporomandibular joint in the young horse. Equine Vet. J. 2008, 40, 566–571. [Google Scholar] [CrossRef]
- Rodríguez, M.J.; Agut, A.; Soler, M.; Lopez-Albors, O.; Arredondo, J.; Querol, M.; Latorre, R. Magnetic resonance imaging of the equine temporomandibular joint anatomy. Equine Vet. J. 2010, 42, 200–207. [Google Scholar] [CrossRef]
- Larheim, T.A.; Abrahamsson, A.K.; Kristensen, M.; Arvidsson, L.Z. Temporomandibular joint diagnostics using CBCT. Dentomaxillofacial Radiol. 2015, 44, 20140235. [Google Scholar] [CrossRef]
- Carmalt, J.L.; Pimentel, K.L. The Equine Temporomandibular Joint: Comparisons Between Standard and Needle Arthroscopic Examination of Cadaver Specimens and Standing Horses. Front. Vet. Sci. 2022, 9, 876041. [Google Scholar] [CrossRef]
- López, J.P.; Orjuela, M.P.; González, L.V.; Peraza-Labrador, A.J.; Díaz-Baez, D. Comparison of the Clinical Effectiveness of Intra-Articular Injection with Different Substances After TMJ Arthroscopy: A Systematic Review and Meta-Analysis. J. Maxillofac. Oral Surg. 2023, 1–10. [Google Scholar] [CrossRef]
- De Riu, G.; Vaira, L.A.; Carta, E.; Meloni, S.M.; Sembronio, S.; Robiony, M. Bone marrow nucleated cell concentrate autograft in temporomandibular joint degenerative disorders: 1-year results of a randomized clinical trial. J. Cranio Maxillofac. Surg. 2019, 47, 1728–1738. [Google Scholar] [CrossRef] [PubMed]
- Li, F.L.; Wu, C.B.; Sun, H.J.; Zhou, Q. Comparison of autologous platelet-rich plasma and chitosan in the treatment of temporomandibular joint osteoarthritis: A retrospective cohort study. J. Oral Maxillofac. Surg. 2021, 79, 324–332. [Google Scholar] [CrossRef]
- Derwich, M.; Mitus-Kenig, M.; Pawlowska, E. Interdisciplinary approach to the temporomandibular joint osteoarthritis—Review of the literature. Medicina 2020, 56, 225. [Google Scholar] [CrossRef] [PubMed]
- Manso-Díaz, G.; Taeymans, O.; García-López, J.M.; Weller, R. Application and indications of magnetic resonance imaging and computed tomography of the equine head. Equine Vet. Educ. 2021, 33, 31–46. [Google Scholar] [CrossRef]
- Huthmann, S.; Staszyk, C.; Jacob, H.G.; Rohn, K.; Gasse, H. Biomechanical evaluation of the equine masticatory action: Calculation of the masticatory forces occurring on the cheek tooth battery. J. Biomech. 2009, 42, 67–70. [Google Scholar] [CrossRef]
- Bonin, S.J.; Clayton, H.M.; Lanovaz, J.L.; Johnson, T.J. Kinematics of the equine temporomandibular joint. Am. J. Vet. Res. 2006, 67, 423–428. [Google Scholar] [CrossRef]
- Orset, E.; Chaffanjon, P.; Bettega, G. Temporomandibular JointModel: Anatomic and Radiologic Comparison between Rat and Human. Surg. Radiol. Anat. 2014, 36, 163–166. [Google Scholar] [CrossRef] [PubMed]
- Alomar, X.; Medrano, J.; Cabratosa, J.; Clavero, J.A.; Lorente, M.; Serra, I.; Salvador, A. Anatomy of the temporomandibular joint. Semin. Ultrasound CT MRI 2007, 28, 170–183. [Google Scholar] [CrossRef] [PubMed]
- Anderson, D.D.; Chubinskaya, S.; Guilak, F.; Martin, J.A.; Oegema, T.R.; Olson, S.A.; Buckwalter, J.A. Post-traumatic osteoarthritis: Improving understanding and opportunities for early intervention. J. Orthop. Res. 2011, 29, 802–809. [Google Scholar] [CrossRef] [PubMed]
- Milam, S.B. Pathogenesis of Degenerative Temporomandibular Joint Arthritides. Odontology 2005, 93, 7–15. [Google Scholar] [CrossRef]
- Gesch, D.; Bernhardt, O.; Kirbschus, A. Association of malocclusion and functional occlusion with temporomandibular disorders (TMD) in adults: A systematic review of population-based studies. Quintessence Int. 2004, 35, 211–221. [Google Scholar] [PubMed]
- Utreja, A.; Dyment, N.A.; Yadav, S.; Villa, M.M.; Li, Y.; Jiang, X.; Nanda, R.; Rowe, D.W. Cell and Matrix Response of Temporomandibular Cartilage to Mechanical Loading. Osteoarthr. Cartil. 2016, 24, 335–344. [Google Scholar] [CrossRef]
- Kalladka, M.; Quek, S.; Heir, G.; Eliav, E.; Mupparapu, M.; Viswanath, A. Temporomandibular Joint Osteoarthritis: Diagnosis and Long-Term Conservative Management: A Topic Review. J. Indian Prosthodont. Soc. 2013, 14, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Wen, Y.; Zhang, M.; Liu, Q.; Zhang, H.; Zhang, J.; Lu, L.; Ye, T.; Bai, X.; Xiao, G.; et al. MTORC1 Coordinates the Autophagy and Apoptosis Signaling in Articular Chondrocytes in Osteoarthritic Temporomandibular Joint. Autophagy 2019, 16, 271–288. [Google Scholar] [CrossRef]
- Yan, J.; Qin, W.; Xiao, B.; Wan, Q.; Tay, F.R.; Niu, L.; Jiao, K. Pathological Calcification in Osteoarthritis: An Outcome or a Disease Initiator? Biol. Rev. 2020, 95, 960–985. [Google Scholar] [CrossRef]
- Cheng, N.-T.; Guo, A.; Meng, H. The Protective Role of Autophagy in Experimental Osteoarthritis, and the Therapeutic Effects of Torin 1 on Osteoarthritis by Activating Autophagy. BMC Musculoskelet. Disord. 2016, 17, 150. [Google Scholar] [CrossRef]
- Li, B.; Guan, G.; Mei, L.; Jiao, K.; Li, H. Pathological Mechanism of Chondrocytes and the Surrounding Environment during Osteoarthritis of Temporomandibular Joint. J. Cell. Mol. Med. 2021, 25, 4902–4911. [Google Scholar] [CrossRef]
- Qin, W.; Zhang, Z.; Yan, J.; Han, X.; Niu, L.-N.; Jiao, K. Interaction of Neurovascular Signals in the Degraded Condylar Cartilage. Front. Bioeng. Biotechnol. 2022, 10, 901749. [Google Scholar] [CrossRef]
- Wadhwa, S.; Kapila, S. TMJ disorders: Future innovations in diagnostics and therapeutics. J. Dent. Educ. 2008, 72, 930–947. [Google Scholar] [CrossRef]
- Shi, Y.; Hu, X.; Cheng, J.; Zhang, X.; Zhao, F.; Shi, W.; Ren, B.; Yu, H.; Yang, P.; Li, Z.; et al. A Small Molecule Promotes Cartilage Extracellular Matrix Generation and Inhibits Osteoarthritis Development. Nat. Commun. 2019, 10, 1914. [Google Scholar] [CrossRef]
- Lian, C.; Wang, X.; Qiu, X.; Wu, Z.; Gao, B.; Liu, L.; Liang, G.; Zhou, H.; Yang, X.; Peng, Y.; et al. Collagen Type II Suppresses Articular Chondrocyte Hypertrophy and Osteoarthritis Progression by Promoting Integrin β1-SMAD1 Interaction. Bone Res. 2019, 7, 8. [Google Scholar] [CrossRef]
- Embree, M.; Ono, M.; Kilts, T.; Walker, D.; Langguth, J.; Mao, J.; Bi, Y.; Barth, J.L.; Young, M. Role of subchondral bone during early-stage experimental TMJ osteoarthritis. J. Dent. Res. 2011, 90, 1331–1338. [Google Scholar] [CrossRef]
- Burr, D.B.; Gallant, M.A. Bone remodelling in osteoarthritis. Nat. Rev. Rheumatol. 2012, 8, 665–673. [Google Scholar] [CrossRef]
- Li, G.; Yin, J.; Gao, J.; Cheng, T.S.; Pavlos, N.J.; Zhang, C.; Zheng, M.H. Subchondral Bone in Osteoarthritis: Insight into Risk Factors and Microstructural Changes. Arthritis Res. Ther. 2013, 15, 223. [Google Scholar] [CrossRef]
- Borciani, G.; Montalbano, G.; Baldini, N.; Cerqueni, G.; Vitale-Brovarone, C.; Ciapetti, G. Co-Culture Systems of Osteoblasts and Osteoclasts: Simulating in vitro Bone Remodeling in Regenerative Approaches. Acta Biomater. 2020, 108, 22–45. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Onal, M.; Jilka, R.L.; Weinstein, R.S.; Manolagas, S.C.; O’Brien, C.A. Matrix-Embedded Cells Control Osteoclast Formation. Nat. Med. 2011, 17, 1235–1241. [Google Scholar] [CrossRef] [PubMed]
- Dole, N.S.; Mazur, C.M.; Acevedo, C.; Lopez, J.P.; Monteiro, D.A.; Fowler, T.W.; Gludovatz, B.; Walsh, F.; Regan, J.N.; Messina, S.; et al. Osteocyte-Intrinsic TGF-β Signaling Regulates Bone Quality through Perilacunar/Canalicular Remodeling. Cell Rep. 2017, 21, 2585–2596. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Lu, H.; Deng, L.; Lin, C.-H.; Pennington Klein, K.; Wu, M. HMGB2 Is Associated with Pressure Loading in Chondrocytes of Temporomandibular Joint: In Vitro and In Vivo Study. Cytokine 2020, 126, 154875. [Google Scholar] [CrossRef]
- Chen, Y.; Zhao, B.; Zhu, Y.; Zhao, H.; Ma, C. HIF-1-VEGF-Notch mediates angiogenesis in temporomandibular joint osteoarthritis. Am. J. Transl. Res. 2019, 11, 2969–2982. [Google Scholar] [PubMed]
- Shirakura, M.; Tanimoto, K.; Eguchi, H.; Miyauchi, M.; Nakamura, H.; Hiyama, K.; Tanimoto, K.; Tanaka, E.; Takata, T.; Tanne, K. Activation of the Hypoxia-Inducible Factor-1 in Overloaded Temporomandibular Joint, and Induction of Osteoclastogenesis. Biochem. Biochem. Biophys. Res. Commun. 2010, 393, 800–805. [Google Scholar] [CrossRef] [PubMed]
- Vernal, R.; Velasquez, E.; Gamonal, J.; Garcia–Sanz, J.A.; Silva, A.; Sanz, M. Expression of proinflammatory cytokines in osteoarthritis of the temporomandibular joint. Arch. Oral Biol. 2008, 53, 910–915. [Google Scholar] [CrossRef]
- Wehmeyer, C.; Pap, T.; Buckley, C.D.; Naylor, A.J. The Role of Stromal Cells in Inflammatory Bone Loss. Clin. Exp. Immunol. 2017, 189, 1–11. [Google Scholar] [CrossRef]
- Deschner, J.; Rath-Deschner, B.; Agarwal, S. Regulation of matrix metalloproteinase expression by dynamic tensile strain in rat fibrochondrocytes. Osteoarthr. Cartil. 2006, 14, 264–272. [Google Scholar] [CrossRef]
- Schaible, H.G. Nociceptive neurons detect cytokines in arthritis. Arthritis Res. Ther. 2014, 16, 470. [Google Scholar] [CrossRef] [PubMed]
- Ogura, N.; Satoh, K.; Akutsu, M.; Tobe, M.; Kuyama, K.; Kuboyama, N.; Sakamaki, H.; Kujiraoka, H.; Kondoh, T. MCP-1 Production in Temporomandibular Joint Inflammation. J. Dent. Res. 2010, 89, 1117–1122. [Google Scholar] [CrossRef]
- Ibi, M.; Horie, S.; Kyakumoto, S.; Chosa, N.; Yoshida, M.; Kamo, M.; Ohtsuka, M.; Ishisaki, A. Cell–Cell Interactions between Monocytes/Macrophages and Synoviocyte-like Cells Promote Inflammatory Cell Infiltration Mediated by Augmentation of MCP-1 Production in Temporomandibular Joint. Biosci. Rep. 2018, 38, BSR20171217. [Google Scholar] [CrossRef]
- Xu, J.; Cai, H.; Meng, Q.; Li, Y.; Chen, G.; Fang, W.; Long, X. IL-1β-Regulating Angiogenic Factors Expression in Perforated Temporomandibular Disk Cells via NF–KB Pathway. J. Oral Pathol. Med. 2016, 45, 605–612. [Google Scholar] [CrossRef]
- Zhang, J.; Zhang, H.Y.; Zhang, M.; Qiu, Z.Y.; Wu, Y.P.; Callaway, D.A.; Jiang, J.X.; Lu, L.; Jing, L.; Yang, T.; et al. Connexin43 hemichannels mediate small molecule exchange between chondrocytes and matrix in biomechanically-stimulated temporomandibular joint cartilage. Osteoarthr. Cartil. 2014, 22, 822–830. [Google Scholar] [CrossRef]
- Wagner, D.O.; Sieber, C.; Bhushan, R.; Borgermann, J.H.; Graf, D.; Knaus, P. BMPs: From bone to body morphogenetic proteins. Sci. Signal. 2010, 3, mr1. [Google Scholar]
- Tang, Y.; Wu, X.; Lei, W.; Pang, L.; Wan, C.; Shi, Z.; Zhao, L.; Nagy, T.R.; Peng, X.; Hu, J.; et al. TGF-beta1-induced migration of bone mesenchymal stem cells couples bone resorption with formation. Nat. Med. 2009, 15, 757–765. [Google Scholar] [CrossRef]
- Li, W.; Zhao, S.; Yang, H.; Zhang, C.; Kang, Q.; Deng, J.; Xu, Y.; Ding, Y.; Li, S. Potential Novel Prediction of TMJ-Oa: Mir-140-5p Regulates Inflammation through SMAD/TGF-β Signaling. Front. Pharmacol. 2019, 10, 15. [Google Scholar] [CrossRef]
- Zheng, L.; Pi, C.; Zhang, J.; Fan, Y.; Cui, C.; Zhou, Y.; Sun, J.; Yuan, Q.; Xu, X.; Ye, L.; et al. Aberrant Activation of Latent Transforming Growth Factor-β Initiates the Onset of Temporomandibular Joint Osteoarthritis. Bone Res. 2018, 6, 26. [Google Scholar] [CrossRef] [PubMed]
- Jiao, K.; Zhang, M.; Niu, L.; Yu, S.; Zhen, G.; Xian, L.; Yu, B.; Yang, K.; Liu, P.; Cao, X.; et al. Overexpressed TGF-beta in subchondral bone leads to mandibular condyle degradation. J. Dent. Res. 2014, 93, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Lenardo, M.J.; Baltimore, D. 30 Years of NF–κB: A blossoming of relevance to human pathobiology. Cell 2017, 168, 37–57. [Google Scholar] [CrossRef] [PubMed]
- Abed, É.; Delalandre, A.; Lajeunesse, D. Beneficial Effect of Resveratrol on Phenotypic Features and Activity of Osteoarthritic Osteoblasts. Arthritis Res. Ther. 2017, 19, 151. [Google Scholar] [CrossRef] [PubMed]
- Chijimatsu, R.; Kunugiza, Y.; Taniyama, Y.; Nakamura, N.; Tomita, T.; Yoshikawa, H. Expression and pathological effects of periostin in human osteoarthritis cartilage. BMC Musculoskelet. Disord. 2015, 16, 215. [Google Scholar] [CrossRef] [PubMed]
- Jiao, K.; Zeng, G.; Niu, L.-N.; Yang, H.-X.; Ren, G.-T.; Xu, X.-Y.; Li, F.-F.; Tay, F.R.; Wang, M.-Q. Activation of α2A-Adrenergic Signal Transduction in Chondrocytes Promotes Degenerative Remodelling of Temporomandibular Joint. Sci. Rep. 2016, 6, 30085. [Google Scholar] [CrossRef]
- Liu, X.; Cai, H.X.; Cao, P.Y.; Feng, Y.; Jiang, H.H.; Liu, L.; Ke, J.; Long, X. TLR4 contributes to the damage of cartilage and subchondral bone in discectomy–induced TMJOA mice. J. Cell. Mol. Med. 2020, 24, 11489–11499. [Google Scholar] [CrossRef]
- Ornitz, D.M.; Itoh, N. The Fibroblast Growth Factor Signaling Pathway. Wiley Interdiscip. Rev. Dev. Biol. 2015, 4, 215–266. [Google Scholar] [CrossRef]
- Su, N.; Du, X.; Chen, L. FGF signaling: Its role in bone development and human skeleton diseases. Front. Biosci. 2008, 13, 2842–2865. [Google Scholar] [CrossRef]
- Foldynova-Trantirkova, S.; Wilcox, W.R.; Krejci, P. Sixteen years and counting: The current understanding of fibroblast growth factor receptor 3 (FGFR3) signaling in skeletal dysplasias. Hum. Mutat. 2012, 33, 29–41. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Lin, S.; Li, T.; Jiang, Y.; Huang, Z.; Wen, J.; Cheng, W.; Li, H. Mechanical Force-Mediated Pathological Cartilage Thinning Is Regulated by Necroptosis and Apoptosis. Osteoarthr. Cartil. 2017, 25, 1324–1334. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Huang, J.; Zhou, S.; Luo, F.; Tan, Q.; Sun, X.; Ni, Z.; Chen, H.; Du, X.; Xie, Y.; et al. Loss of Fgfr1 in chondrocytes inhibits osteoarthritis by promoting autophagic activity in temporomandibular joint. J. Biol. Chem. 2018, 293, 8761–8774. [Google Scholar] [CrossRef] [PubMed]
- Cevidanes, L.H.; Walker, D.; Schilling, J.; Sugai, J.; Giannobile, W.; Paniagua, B.; Benavides, E.; Zhu, H.; Marron, J.S.; Jung, B.T.; et al. 3D osteoarthritic changes in TMJ condylar morphology correlates with specific systemic and local biomarkers of disease. Osteoarthr. Cartil. 2014, 22, 1657–1667. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.; Tang, D.; Wu, Q.; Hao, S.; Chen, M.; Xie, C.; Rosier, R.N.; O’Keefe, R.J.; Zuscik, M.; Chen, D. Activation of β-Catenin Signaling in Articular Chondrocytes Leads to Osteoarthritis-like Phenotype in Adult β-Catenin Conditional Activation Mice. J. Bone Miner. Res. 2009, 24, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Zhang, J.; Cao, Y.; Zhang, M.; Jing, L.; Jiao, K.; Yu, S.; Chang, W.; Chen, D.; Wang, M. Wnt5a/Ror2 mediates temporomandibular joint subchondral bone remodeling. J. Dent. Res. 2015, 94, 803–812. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Shu, B.; Xie, R.; Huang, J.; Zheng, L.; Zhou, X.; Xiao, G.; Zhao, L.; Chen, D. Deletion of axin1 in Condylar Chondrocytes Leads to Osteoarthritis–like Phenotype in Temporomandibular Joint via Activation of β-Catenin and FGF Signaling. J. Cell. Physiol. 2018, 234, 1720–1729. [Google Scholar] [CrossRef] [PubMed]
- Nachury, M.V.; Mick, D.U. Establishing and regulating the composition of cilia for signal transduction. Nat. Rev. Mol. Cell Biol. 2019, 20, 389–405. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Zhang, M.; Liu, Q.; Zhang, H.; Zhang, J.; Lu, L.; Xie, M.; Chen, D.; Wang, M. Inhibition of Ihh reverses temporomandibular joint osteoarthritis via a PTH1R signaling dependent mechanism. Int. J. Mol. Sci. 2019, 20, 3797. [Google Scholar] [CrossRef] [PubMed]
- Alman, B.A. The role of hedgehog signalling in skeletal health and disease. Nat. Rev. Rheumatol. 2015, 11, 552–560. [Google Scholar] [CrossRef] [PubMed]
- Lanske, B.; Karaplis, A.C.; Lee, K.; Luz, A.; Vortkamp, A.; Pirro, A.; Karperien, M.; Defize, L.H.; Ho, C.; Mulligan, R.C.; et al. PTH/PTHrP receptor in early development and Indian hedgehog—Regulated bone growth. Science 1996, 273, 663–666. [Google Scholar] [CrossRef]
- D’Souza, B.; Meloty-Kapella, L.; Weinmaster, G. Canonical and non–canonical Notch ligands. Curr. Top. Dev. Biol. 2010, 92, 73–129. [Google Scholar]
- Kopan, R.; Ilagan, M.X. The canonical Notch signaling pathway: Unfolding the activation mechanism. Cell 2009, 137, 216–233. [Google Scholar] [CrossRef]
- Saito, T.; Tanaka, S. Molecular mechanisms underlying osteoarthritis development: Notch and NF-κB. Arthritis Res. Ther. 2017, 19, 94. [Google Scholar] [CrossRef]
- Yoon, K.; Gaiano, N. Notch signaling in the mammalian central nervous system: Insights from mouse mutants. Nat. Neurosci. 2005, 8, 709–715. [Google Scholar] [CrossRef]
- Wang, Q.Y.; Dai, J.; Kuang, B.; Zhang, J.; Yu, S.B.; Duan, Y.Z.; Wang, M.Q. Osteochondral angiogenesis in rat mandibular condyles with osteoarthritis-like changes. Arch. Oral Biol. 2012, 57, 620–629. [Google Scholar] [CrossRef]
- Mahjoub, M.; Sassi, N.; Driss, M.; Laadhar, L.; Allouche, M.; Hamdoun, M.; Romdhane, K.B.; Sellami, S.; Makni, S. Expression patterns of Notch receptors and their ligands in human osteoarthritic and healthy articular cartilage. Tissue Cell 2012, 44, 182–194. [Google Scholar] [CrossRef]
- Liao, L.; Zhang, S.; Zhou, G.Q.; Ye, L.; Huang, J.; Zhao, L.; Chen, D. Deletion of Runx2 in condylar chondrocytes disrupts TMJ tissue homeostasis. J. Cell. Physiol. 2019, 234, 3436–3444. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.Y.; Chen, Y.; Tang, X.J.; Jiang, L.H.; Ji, P. AMD3100 attenuates matrix metalloprotease-3 and -9 expressions and prevents cartilage degradation in a monosodium iodo-acetate—Induced rat model of temporomandibular osteoarthritis. J. Oral Maxillofac. Surg. 2016, 74, 927.e1–927.e13. [Google Scholar] [CrossRef]
- Du, J.; Jiang, Q.; Mei, L.; Yang, R.; Wen, J.; Lin, S.; Li, H. Effect of high fat diet and excessive compressive mechanical force on pathologic changes of temporomandibular joint. Sci. Rep. 2020, 10, 17457. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Hu, Y.; Wang, C.; Zhang, X.; He, D. CircGCN1L1 promotes synoviocyte proliferation and chondrocyte apoptosis by targeting miR-330-3p and TNF-α in TMJ osteoarthritis. Cell Death Dis. 2020, 11, 284. [Google Scholar] [CrossRef]
- Pereira, T.P.; Staut, F.T.; Machado, T.S.; Brossi, P.M.; Baccarin, R.Y.; Michelotto, P.V. Effects of the oral examination on the equine temporomandibular joint. J. Equine Vet. Sci. 2016, 43, 48–54. [Google Scholar] [CrossRef]
- Rashed, M.Z.; Sharawy, M.M.; Koole, P. Histopathological and immunocytochemical studies of the effect of raised occlusal vertical dimension on the condylar cartilage of the rabbit. CRANIO 1993, 11, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Little, C.; Smith, M. Animal models of osteoarthritis. Curr. Rheumatol. Rev. 2008, 4, 175–182. [Google Scholar] [CrossRef]
- Slavicek, G. Human mastication. J. Stomat. Occ. Med. 2010, 3, 29–41. [Google Scholar] [CrossRef]
- Wall, C.E.; Smith, K.K. Ingestion in Mammals. Enc. Life Sci. 2001, 1, 1–6. [Google Scholar]
- Sella-Tunis, T.; Pokhojaev, A.; Sarig, R.; O’Higgins, P.; May, H. Human mandibular shape is associated with masticatory muscle force. Sci. Rep. 2018, 8, 6042. [Google Scholar] [CrossRef]
- Duizer, L.M.; Winger, R.J. Instrumental measures of bite forces associated with crisp products. J. Texture Stud. 2006, 37, 1–15. [Google Scholar] [CrossRef]
- Kohyama, K.; Sasaki, T.; Hayakawa, F.; Hatakeyama, E. Effects of cross-sectional area on human bite studied with raw carrot and Surimi gel. Biosci. Biotechnol. Biochem. 2004, 68, 2104–2110. [Google Scholar] [CrossRef]
- Kamegai, T.; Tatsuki, T.; Nagano, H.; Mitsuhashi, H.; Kumeta, J.; Tatsuki, Y.; Kamegai, T.; Inaba, D. A determination of bite force in northern Japanese children. Eur. J. Orthod. 2005, 27, 53–57. [Google Scholar] [CrossRef]
- Stieger-Vanegas, S.M.; Hanna, A.L. The role of computed tomography in imaging non-neurologic disorders of the head in equine patients. Front. Vet. Sci. 2022, 9, 798216. [Google Scholar] [CrossRef]
- Brounts, S.H.; Henry, T.; Lund, J.R.; Whitton, R.C.; Ergun, D.L.; Muir, P. Use of a novel helical fan beam imaging system for computed tomography of the head and neck in sedated standing horses: 120 cases (2019–2020). J. Am. Vet. Med. Assoc. 2022, 260, 1361–1368. [Google Scholar] [CrossRef] [PubMed]
- Fang, J.; Xiao, L.; Chen, R.; Zhao, Z. Conditional removal of the canonical TGF-β1 signaling delays condylar cartilage degeneration induced by a partial discectomy in mice. PLoS ONE 2017, 12, e0177826. [Google Scholar] [CrossRef]
- Yuan, J.; Ding, W.; Wu, N.; Jiang, S.; Li, W. Protective effect of genistein on condylar cartilage through downregulating NF-κB expression in experimentally created osteoarthritis rats. BioMed. Res. Int. 2019, 2019, 2629791. [Google Scholar] [CrossRef] [PubMed]
- Ou, F.; Huang, Y.; Sun, J.; Su, K.; He, Y.; Zeng, R.; Tang, D.; Liao, G. Yohimbine ameliorates temporomandibular joint chondrocyte inflammation with suppression of NF-κB pathway. Inflammation 2021, 44, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Bechtold, T.E.; Saunders, C.; Decker, R.S.; Um, H.B.; Cottingham, N.; Salhab, I.; Kurio, N.; Billings, P.C.; Pacifici, M.; Nah, H.D.; et al. Osteophyte formation and matrix mineralization in a TMJ osteoarthritis mouse model are associated with ectopic hedgehog signaling. Matrix Biol. 2016, 52–54, 339–354. [Google Scholar] [CrossRef]
- Luo, X.; Jiang, Y.; Bi, R.; Jiang, N.; Zhu, S. Inhibition of notch signaling pathway temporally postpones the cartilage degradation progress of temporomandibular joint arthritis in mice. J. Cranio. Maxillo. Facial Surg. 2018, 46, 1132–1138. [Google Scholar] [CrossRef]
- Hendriks, J.; Sharif, M.; Saris, D.B.; Karperien, M. A highly sensitive multiplex biomarker assay for the early diagnosis of osteoarthritis. Osteoarthr. Cartil. 2019, 27, S108. [Google Scholar] [CrossRef]
- Hendriks, J.; Karperien, M.; Krabbe, H. Clinically feasible multiplex biomarker assay for assessing joint health and stratifying osteoarthritis patient population. Osteoarthr. Cartil. 2021, 29, S160. [Google Scholar] [CrossRef]
- Maloley, P.M.; England, B.R.; Sayles, H.R.; Thiele, G.M.; Duryee, M.J.; Hunter, C.D.; Payne, J.B.; Mikuls, T.R. Performance of a commercially available multiplex platform in the assessment of circulating cytokines and chemokines in patients with rheumatoid arthritis and osteoarthritis. J. Immunol. Methods 2021, 495, 113048. [Google Scholar] [CrossRef] [PubMed]
- Bernotiene, E.; Bagdonas, E.; Kirdaite, G.; Bernotas, P.; Kalvaityte, U.; Uzieliene, I.; Thudium, C.S.; Hannula, H.; Lorite, G.S.; Dvir-Ginzberg, M.; et al. Emerging technologies and platforms for the immunodetection of multiple biochemical markers in osteoarthritis research and therapy. Front. Med. 2020, 7, 572977. [Google Scholar] [CrossRef] [PubMed]
- Ratneswaran, A.; Rockel, J.S.; Antflek, D.; Matelski, J.J.; Shestopaloff, K.; Kapoor, M.; Baltzer, H. Investigating Molecular Signatures Underlying Trapeziometacarpal Osteoarthritis Through the Evaluation of Systemic Cytokine Expression. Front. Immunol. 2022, 12, 794792. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).