
Intravenous Thrombolysis in Posterior versus Anterior Circulation Stroke: Clinical Outcome Differs Only in Patients with Large Vessel Occlusion

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Baseline Data
2.3. Outcome Parameters
2.4. Statistical Analysis
3. Results

{kind=link}
{kind=link}
| Observed Parameter | n-Used | PCS Group n = 1166 (11.4%) | ACS Group n = 9045 (88.6%) | p |
|---|---|---|---|---|
| Demographics | ||||
| Women; n (%) | 10,211 | 459 (39.4) | 4151 (45.9) | <0.001 |
| Age; years, mean (SD) | 10,199 | 67.1 (13.3) | 70.7 (12.4) | <0.001 |
| Occurrence of vascular risk factors | ||||
| Arterial hypertension; n (%) | 10,043 | 821 (71.5) | 6794 (76.4) | 0.0003 |
| Congestive heart failure; n (%) | 10,003 | 64 (5.6) | 805 (9.1) | <0.0001 |
| Atrial fibrillation; n (%) | 10,039 | 197 (17.2) | 2000 (22.5) | <0.0001 |
| Diabetes mellitus; n (%) | 10,156 | 298 (25.6) | 2623 (29.2) | 0.012 |
| Hyperlipidemia; n (%) | 9925 | 398 (34.8) | 3108 (35.4) | 0.718 |
| Obesity; n (%) | 6197 | 236 (29.3) | 1476 (27.4) | 0.254 |
| Current smoking; n (%) | 9393 | 213 (19.3) | 1500 (18.1) | 0.319 |
| Previous stroke or TIA; n (%) | 10,118 | 207 (17.9) | 1643 (18.3) | 0.716 |
| Pre-stroke pharmacotherapy | ||||
| Anticoagulation; n (%) | 9502 | 45 (4.1) | 401 (4.8) | 0.326 |
| Antiplatelets; n (%) | 10,140 | 385 (33.1) | 3518 (39.2) | <0.001 |
| Statins; n (%) | 9434 | 324 (27.9) | 2574 (31.1) | 0.029 |
| Clinical parameters | ||||
| Baseline NIHSS; median (IQR) | 9918 | 6 (4–9) | 8 (5–14) | <0.0001 |
| Large vessel occlusion; n (%) | 6164 | 423 (52.9) | 2451 (45.7) | 0.0002 |
| Glucose; mmol/L, mean (SD) | 9642 | 8.0 (2.9) | 7.7 (2.8) | 0.0001 |
| Cholesterol; mmol/L, mean (SD) | 7016 | 4.9 (1.2) | 4.8 (1.2) | 0.172 |
| SBP; mmHg, mean (SD) | 9941 | 158.0 (26.3) | 159.4 (24.8) | 0.103 |
| DBP; mmHg, mean (SD) | 9941 | 85.6 (14.5) | 86.1 (14.2) | 0.291 |
| i.v. antihypertensive therapy before/during IVT; n (%) | 9584 | 191 (17.4) | 1461 (17.2) | 0.899 |
| ONT; min, mean (SD) | 9779 | 160.8 (76.3) | 144.7 (60.9) | <0.0001 |
| DNT; min, mean (SD) | 10,013 | 54.6 (37.2) | 51.2 (32.3) | 0.003 |
| Post-stroke pharmacotherapy | ||||
| LMWH; n (%) | 9113 | 644 (57.8) | 4267 (53.3) | 0.005 |
| Anticoagulation; n (%) | 8872 | 90 (8.1) | 577 (7.4) | 0.430 |
| Antiplatelets; n (%) | 9477 | 758 (65.2) | 4989 (60.0) | 0.0008 |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Neumann, J.; Šaňák, D.; Tomek, A.; Bar, M.; Herzig, R.; Kovář, M.; Mikulík, R.; Reková, P.; Součková, D.; Škoda, O.; et al. Doporučení pro intravenózní trombolýzu v léčbě akutního mozkového infarktu—Verze 2021. Cesk. Slov. Neurol. N. 2021, 84/117, 291–299. [Google Scholar] [CrossRef]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418. [Google Scholar] [CrossRef] [PubMed]
- Hacke, W.; Kaste, M.; Bluhmki, E.; Brozman, M.; Dávalos, A.; Guidetti, D.; Larrue, V.; Lees, K.R.; Medeghri, Z.; ECASS Investigators; et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N. Engl. J. Med. 2008, 359, 1317–1329. [Google Scholar] [CrossRef] [PubMed]
- Lees, K.R.; Bluhmki, E.; von Kummer, R.; Brott, T.G.; Toni, D.; Grotta, J.C.; Albers, G.W.; Kaste, M.; Marler, J.R.; Hamilton, S.A.; et al. Time to treatment with intravenous alteplase and outcome in stroke: An updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet 2010, 375, 1695–1703. [Google Scholar] [CrossRef]
- Ma, H.; Campbell, B.C.V.; Parsons, M.W.; Churilov, L.; Levi, C.R.; Hsu, C.; Kleinig, T.J.; Wijeratne, T.; Curtze, S.; EXTEND Investigators; et al. Thrombolysis guided by perfusion imaging up to 9 hours after onset of stroke. N. Engl. J. Med. 2019, 380, 1795–1803. [Google Scholar] [CrossRef] [PubMed]
- Dorňák, T.; Král, M.; Hazlinger, M.; Herzig, R.; Veverka, T.; Buřval, S.; Šaňák, D.; Zapletalová, J.; Antalíková, K.; Kaňovský, P. Posterior vs. anterior circulation infarction: Demography, outcomes, and frequency of hemorrhage after thrombolysis. Int. J. Stroke 2015, 10, 1224–1228. [Google Scholar] [CrossRef]
- Förster, A.; Gass, A.; Kern, R.; Griebe, M.; Hennerici, M.G.; Szabo, K. Thrombolysis in posterior circulation stroke: Stroke subtypes and patterns, complications and outcome. Cerebrovasc. Dis. 2011, 32, 349–353. [Google Scholar] [CrossRef]
- Keselman, B.; Gdovinová, Z.; Jatuzis, D.; Mělo, T.P.E.; Vilionskis, A.; Cavallo, R.; Frol, S.; Jurak, L.; Koyuncu, B.; Nunes, A.P.; et al. Safety and outcomes of intravenous thrombolysis in posterior versus anterior circulation stroke: Results from the Safe Implementation of Treatments in Stroke Registry and meta-analysis. Stroke 2020, 51, 876–882. [Google Scholar] [CrossRef]
- Sung, S.F.; Chen, C.H.; Chen, Y.W.; Tseng, M.C.; Shen, H.C.; Lin, H.J. Predicting symptomatic intracerebral hemorrhage after intravenous thrombolysis: Stroke territory as a potential pitfall. J. Neurol. Sci. 2013, 335, 96–100. [Google Scholar] [CrossRef]
- De Marchis, G.M.; Kohler, A.; Renz, N.; Arnold, M.; Mono, M.L.; Jung, S.; Fischer, U.; Karameshev, A.I.; Brekenfeld, C.; Gralla, J.; et al. Posterior versus anterior circulation strokes: Comparison of clinical, radiological and outcome characteristics. J. Neurol. Neurosurg. Psychiatry 2011, 82, 33–37. [Google Scholar] [CrossRef]
- Nair, S.S.; Sylaja, P.N.; Pandian, J.; Srivastava, M.V.P.; Khurana, D.; Kaul, S.; Arora, D.; Sarma, P.S.; Khatter, H.; Singhal, A.B. Impact of revascularization therapies on outcome of posterior circulation ischemic stroke: The Indo-US stroke project. J. Neurol. Sci. 2021, 427, 117499. [Google Scholar] [CrossRef] [PubMed]
- Sarikaya, H.; Arnold, M.; Engelter, S.T.; Lyrer, P.A.; Mattle, H.P.; Georgiadis, D.; Bonati, L.H.; Fluri, F.; Fischer, U.; Findling, O.; et al. Outcomes of intravenous thrombolysis in posterior versus anterior circulation stroke. Stroke 2011, 42, 2498–2502. [Google Scholar] [CrossRef] [PubMed]
- Sarraj, A.; Medrek, S.; Albright, K.; Martin-Schild, S.; Bibars, W.; Vahidy, F.; Grotta, J.C.; Savitz, S.I. Posterior circulation stroke is associated with prolonged door-to-needle time. Int. J. Stroke 2015, 10, 672–678. [Google Scholar] [CrossRef] [PubMed]
- Taha, N.A.; El Khawas, H.; Tork, M.A.; Roushdy, T.M. Intravenous thrombolysis outcome in posterior vs anterior circulation stroke in a tertiary stroke center in Egypt. Egypt. J. Neurol. Psychiatry Neurosurg. 2021, 57, 73. [Google Scholar] [CrossRef]
- Tong, X.; Liao, X.; Pan, Y.; Cao, Y.; Wang, C.; Liu, L.; Zheng, H.; Zhao, X.; Wang, C.; Wang, Y.; et al. Intravenous thrombolysis is more safe and effective for posterior circulation stroke: Data from the Thrombolysis Implementation and Monitor of Acute Ischemic Stroke in China (TIMS-China). Medicine 2016, 95, e3848. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Saver, J.L.; Alger, J.R.; Hao, Q.; Starkman, S.; Ali, L.K.; Kim, D.; Ovbiagele, B.; Vespa, P.M.; Froehler, M.T.; et al. Blood-brain barrier permeability derangements in posterior circulation ischemic stroke: Frequency and relation to hemorrhagic transformation. J. Neurol. Sci. 2012, 313, 142–146. [Google Scholar] [CrossRef]
- Menon, B.K.; O’Brien, B.; Bivard, A.; Spratt, N.J.; Demchuk, A.M.; Miteff, F.; Lu, X.; Levi, C.; Parsons, M.W. Assessment of leptomeningeal collaterals using dynamic CT angiography in patients with acute ischemic stroke. J. Cereb. Blood Flow Metab. 2013, 33, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Neumann, J.; Tomek, A.; Školoudík, D.; Škoda, O.; Mikulík, R.; Herzig, R.; Václavík, D.; Bar, M.; Šaňák, D. Doporučený postup pro intravenózní trombolýzu v léčbě akutního mozkového infarktu—Verze 2014. Cesk. Slov. Neurol. N. 2014, 77/110, 381–385. [Google Scholar]
- Škoda, O.; Herzig, R.; Mikulík, R.; Neumann, J.; Václavík, D.; Bar, M.; Šaňák, D.; Tomek, A.; Školoudík, D. Klinický standard pro diagnostiku a léčbu pacientů s ischemickou cévní mozkovou příhodou a s tranzitorní ischemickou atakou—Verze 2016. Cesk. Slov. Neurol. N. 2016, 79/112, 351–363. [Google Scholar] [CrossRef]
- Školoudík, D.; Bar, M.; Mikulík, R.; Neumann, J.; Václavík, D.; Herzig, R.; Škoda, O.; Kalita, Z.; Šaňák, D.; Polívka, J. Standard pro podání systémové trombolýzy pacientům s akutním mozkovým infarktem. Neurol. Pro Praxi 2006, 1, 55–58. [Google Scholar]
- SITS. Available online: https://db.sitsinternational.org/ (accessed on 15 December 2023).
- Goldstein, L.B.; Samsa, G.P. Reliability of the National Institutes of Health Stroke Scale. Extension to non-neurologists in the context of a clinical trial. Stroke 1997, 28, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Hacke, W.; Kaste, M.; Fieschi, C.; von Kummer, R.; Davalos, A.; Meier, D.; Larrue, V.; Bluhmki, E.; Davis, S.; Donnan, G.; et al. for the Second European-Australasian Acute Stroke Study Investigators. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Lancet 1998, 352, 1245–1251. [Google Scholar] [CrossRef]
- Wahlgren, N.; Ahmed, N.; Dávalos, A.; Ford, G.A.; Grond, M.; Hacke, W.; Hennerici, M.G.; Kaste, M.; Kuelkens, S.; SITS-MOST Investigators; et al. Thrombolysis with alteplase for acute ischaemic stroke in the Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST): An observational study. Lancet 2007, 369, 275–282. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N. Engl. J. Med. 1995, 333, 1581–1587. [Google Scholar] [CrossRef]
- Hong, K.S.; Saver, J.L. Quantifying the value of stroke disability outcomes: WHO global burden of disease project disability weights for each level of the modified Rankin Scale. Stroke 2009, 40, 3828–3833. [Google Scholar] [CrossRef]
- Kim, J.T.; Park, M.S.; Choi, K.H.; Kim, B.J.; Han, M.K.; Park, T.H.; Park, S.S.; Lee, K.B.; Lee, B.C.; Yu, K.H.; et al. Clinical outcomes of posterior versus anterior circulation infarction with low National Institutes of Health Stroke Scale scores. Stroke 2017, 48, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Hacke, W.; Kaste, M.; Fieschi, C.; Toni, D.; Lesaffre, E.; von Kummer, R.; Boysen, G.; Bluhmki, E.; Höxter, G.; Mahagne, M.H.; et al. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke: The European Cooperative Acute Stroke Study (ECASS). JAMA 1995, 274, 1017–1025. [Google Scholar] [CrossRef]
- Inoa, V.; Aron, A.W.; Staff, I.; Fortunato, G.; Sansing, L.H. Lower NIH stroke scale scores are required to accurately predict a good prognosis in posterior circulation stroke. Cerebrovasc. Dis. 2014, 37, 251–255. [Google Scholar] [CrossRef]
- Kasner, S.E. Clinical interpretation and use of stroke scales. Lancet Neurol. 2006, 5, 603–612. [Google Scholar] [CrossRef]
- Martin-Schild, S.; Albright, K.C.; Tanksley, J.; Pandav, V.; Jones, E.B.; Grotta, J.C.; Savitz, S.I. Zero on the NIHSS does not equal the absence of stroke. Ann. Emerg. Med. 2011, 57, 42–45. [Google Scholar] [CrossRef]
- Sato, S.; Toyoda, K.; Uehara, T.; Toratani, N.; Yokota, C.; Moriwaki, H.; Naritomi, H.; Minematsu, K. Baseline NIH Stroke Scale score predicting outcome in anterior and posterior circulation strokes. Neurology 2008, 70, 2371–2377. [Google Scholar] [CrossRef] [PubMed]
- Schneck, M.J. Current stroke scales may be partly responsible for worse outcomes in posterior circulation stroke. Stroke 2018, 49, 2565–2566. [Google Scholar] [CrossRef] [PubMed]
- Sommer, P.; Seyfang, L.; Posekany, A.; Ferrari, J.; Lang, W.; Fertl, E.; Serles, W.; Töll, T.; Kiechl, S.; Greisenegger, S. Prehospital and intra-hospital time delays in posterior circulation stroke: Results from the Austrian Stroke Unit Registry. J. Neurol. 2017, 264, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Halúsková, S.; Herzig, R.; Krajíčková, D.; Hamza, A.; Krajina, A.; Chovanec, V.; Lojík, M.; Raupach, J.; Renc, O.; Šimůnek, L.; et al. Acute management should be optimized in patients with less specific stroke symptoms: Findings from a retrospective observational study. J. Clin. Med. 2021, 10, 1143. [Google Scholar] [CrossRef]
- Dornak, T.; Herzig, R.; Sanak, D.; Skoloudik, D. Management of acute basilar artery occlusion: Should any treatment strategy prevail? Biomed. Pap. Med. Fac. Univ. Palacky. Olomouc Czech Repub. 2014, 158, 528–534. [Google Scholar] [CrossRef]
- Zhu, X.; Wang, N.; Lin, H.; Zhang, P.; Chen, L.; Zhang, M.; Deng, B.; Wu, T. Safety and efficacy of intravenous thrombolytic therapy in patients with acute posterior circulation stroke: A single-center study. J. Stroke Cerebrovasc. Dis. 2020, 29, 104537. [Google Scholar] [CrossRef]
- Sand, K.M.; Næss, H.; Nilsen, R.M.; Thomassen, L.; Hoff, J.M. Less thrombolysis in posterior circulation infarction—A necessary evil? Acta Neurol. Scand. 2017, 135, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Handelsmann, H.; Herzog, L.; Kulcsar, Z.; Luft, A.R.; Wegener, S. Predictors for affected stroke territory and outcome of acute stroke treatments are different for posterior versus anterior circulation strokea. Sci. Rep. 2021, 11, 10544. [Google Scholar] [CrossRef]
- Zürcher, E.; Richoz, B.; Faouzi, M.; Michel, P. Differences in ischemic anterior and posterior circulation strokes: A clinico-radiological and outcome analysis. J. Stroke Cerebrovasc. Dis. 2019, 28, 710–718. [Google Scholar] [CrossRef]
- Lee, S.H.; Han, J.H.; Jung, I.; Jung, J.M. Do thrombolysis outcomes differ between anterior circulation stroke and posterior circulation stroke? A systematic review and meta-analysis. Int. J. Stroke 2020, 15, 849–857. [Google Scholar] [CrossRef]
- Bang, O.Y.; Saver, J.L.; Kim, S.J.; Kim, G.M.; Chung, C.S.; Ovbiagele, B.; Lee, K.H.; Liebeskind, D.S.; UCLA-Samsung Stroke Collaborators. Collateral flow averts hemorrhagic transformation after endovascular therapy for acute ischemic stroke. Stroke 2011, 42, 2235–2239. [Google Scholar] [CrossRef]
- Chuang, Y.-M.; Chan, L.; Lai, Y.J.; Kuo, K.H.; Chiou, Y.H.; Huang, L.W.; Kwok, Y.T.; Lai, T.H.; Lee, S.P.; Wu, H.M.; et al. Configuration of the circle of Willis is associated with less symptomatic intracerebral hemorrhage in ischemic stroke patients treated with intravenous thrombolysis. J. Crit. Care 2013, 28, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Lindgren, A.; Norrving, B.; Rudling, O.; Johansson, B.B. Comparison of clinical and neuroradiological findings in first-ever stroke. A population-based study. Stroke 1994, 25, 1371–1377. [Google Scholar] [CrossRef] [PubMed]
- Singer, O.C.; Humpich, M.C.; Fiehler, J.; Albers, G.W.; Lansberg, M.G.; Kastrup, A.; Rovira, A.; Liebeskind, D.S.; Gass, A.; Rosso, C.; et al. Risk for symptomatic intracerebral hemorrhage after thrombolysis assessed by diffusion-weighted magnetic resonance imaging. Ann. Neurol. 2008, 63, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Bang, O.Y.; Saver, J.L.; Alger, J.R.; Shah, S.H.; Buck, B.H.; Starkman, S.; Ovbiagele, B.; Liebeskind, D.S.; UCLA MRI Permeability Investigators. Patterns and predictors of blood-brain barrier permeability derangements in acute ischemic stroke. Stroke 2009, 40, 454–461. [Google Scholar] [CrossRef] [PubMed]
- Jones, H.R., Jr.; Millikan, C.H.; Sandok, B.A. Temporal profile (clinical course) of acute vertebrobasilar system cerebral infarction. Stroke 1980, 11, 173–177. [Google Scholar] [CrossRef] [PubMed]
- McDowell, F.H.; Potes, J.; Groch, S. The natural history of internal carotid and vertebral-basilar artery occlusion. Neurology 1961, 11, 153–157. [Google Scholar] [CrossRef]
- Frid, P.; Drake, M.; Giese, A.K.; Wasselius, J.; Schirmer, M.D.; Donahue, K.L.; Cloonan, L.; Irie, R.; Bouts, M.J.R.J.; McIntosh, E.C.; et al. Detailed phenotyping of posterior vs. anterior circulation ischemic stroke: A multi-center MRI study. J. Neurol. 2020, 267, 649–658. [Google Scholar] [CrossRef]
- Dorňák, T.; Král, M.; Sedláčková, Z.; Šaňák, D.; Čecháková, E.; Divišová, P.; Zapletalová, J.; Kaňovský, P. Predictors for intracranial hemorrhage following intravenous thrombolysis in posterior circulation stroke. Transl. Stroke Res. 2018, 9, 582–588. [Google Scholar] [CrossRef]
- Lin, S.F.; Chen, C.I.; Hu, H.H.; Bai, C.H. Predicting functional outcomes of posterior circulation acute ischemic stroke in first 36 h of stroke onset. J. Neurol. 2018, 265, 926–932. [Google Scholar] [CrossRef]
- Liu, M.; Pan, Y.; Zhou, L.; Wang, Y. Predictors of post-thrombolysis symptomatic intracranial hemorrhage in Chinese patients with acute ischemic stroke. PLoS ONE 2017, 12, e0184646. [Google Scholar] [CrossRef] [PubMed]
- Jalali, N.; Sadeghi Hokmabadi, E.; Ghoreishi, A.; Sariaslan, P.; Rafie, S.; Borhani-Haghighi, A.; Moghadam Ahmadi, A.; Azin, H.; Vakilian, A.; Khalili, P.; et al. Outcome predictors in anterior and posterior ischemic strokes: A study based on the Iranian SITS registry. Sci. Rep. 2023, 13, 1231. [Google Scholar] [CrossRef] [PubMed]

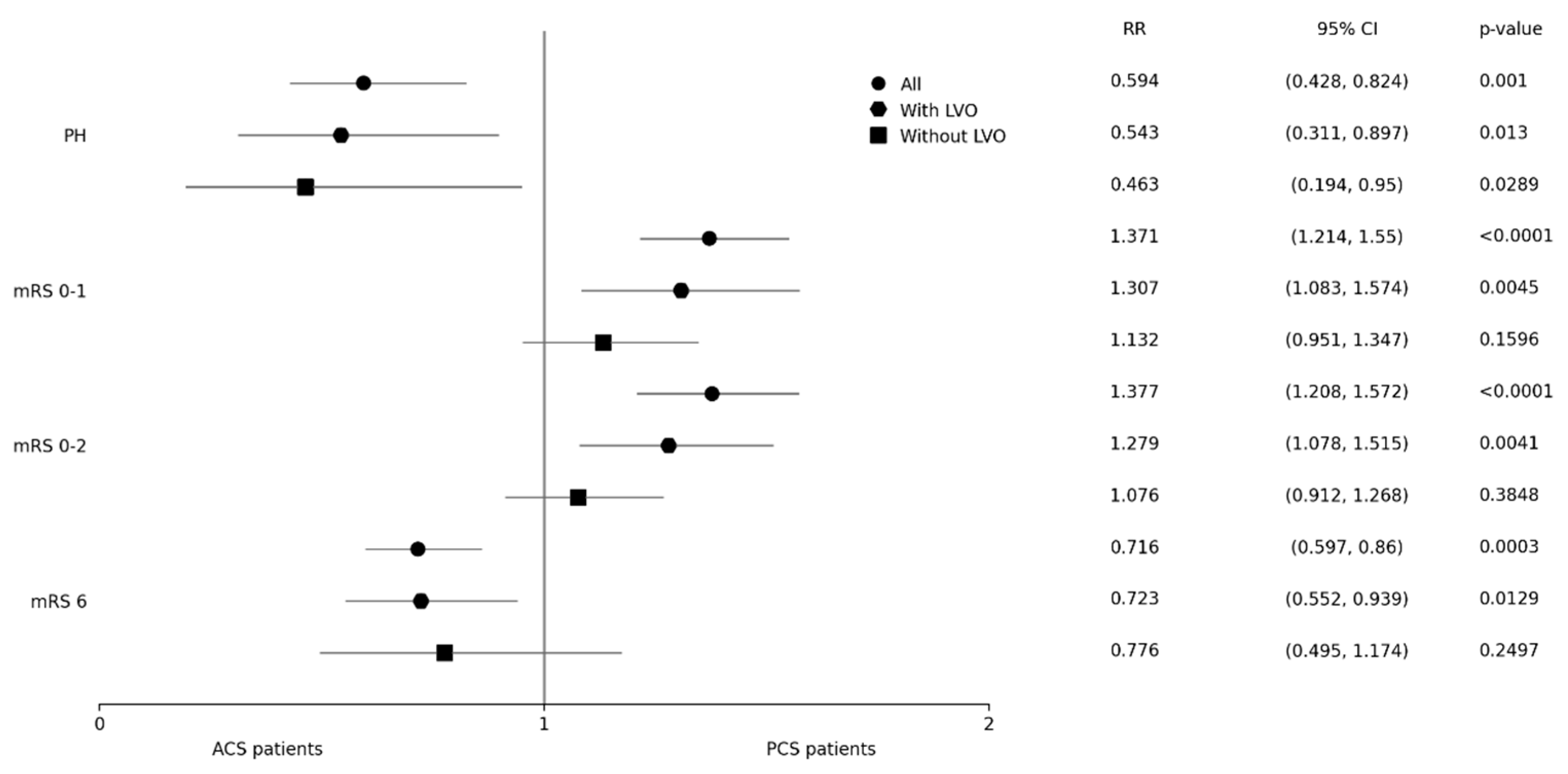
| Observed Parameter n (%) | n-Used | PCS Group All 1166 (11.4) | ACS Group All 9045 (88.6) | p | n-Used | PCS Group with LVO 423 (36.3) | ACS Group with LVO 2451 (27.1) | p <0.0001 | PCS Group without LVO 377 (32.3) | ACS Group without LVO 2913 (32.2) | p 0.9498 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| PH | 9695 | 40 (3.6) | 505 (5.9) | 0.001 | 5854 | 18 (4.4) | 178 (7.8) | 0.013 | 8 (2.2) | 131 (4.7) | 0.0289 |
| mRS 0–1 | 10,211 | 647 (55.5) | 4307 (47.6) | <0.0001 | 6164 | 208 (49.2) | 922 (37.6) | 0.0045 | 251 (66.6) | 1713 (58.8) | 0.1596 |
| mRS 0–2 | 10,211 | 815 (69.9) | 5676 (62.8) | <0.0001 | 6164 | 273 (64.5) | 1237 (50.5) | 0.0041 | 299 (79.3) | 2148 (73.7) | 0.3848 |
| mRS 6 | 10,211 | 145 (12.4) | 1497 (16.6) | 0.0003 | 6164 | 78 (18.4) | 625 (25.5) | 0.0129 | 27 (7.2) | 269 (9.2) | 0.2497 |
| Observed Parameter | OR | 95% CI | p Value |
|---|---|---|---|
| Predictors of the PH | |||
| Age | 1.020 | 1.005–1.035 | 0.009 |
| NIHSS | 1.043 | 1.017–1.069 | 0.001 |
| i.v. antihypertensive therapy before/during IVT | 1.729 | 1.216–2.459 | 0.002 |
| Predictors of mRS 0–1 | |||
| Age | 0.968 | 0.962–0.974 | <0.0001 |
| Previous stroke or TIA | 0.723 | 0.612–0.855 | <0.0001 |
| NIHSS | 0.861 | 0.849–0.873 | <0.0001 |
| Large vessel occlusion | 0.660 | 0.578–0.754 | <0.0001 |
| Glucose level | 0.937 | 0.915–0.959 | <0.0001 |
| i.v. antihypertensive therapy before/during IVT | 0.581 | 0.482–0.700 | <0.0001 |
| ONT | 0.998 | 0.997–1.000 | 0.005 |
| Post-stroke prophylaxis of deep venous thrombosis with LMWH | 0.834 | 0.732–0.950 | 0.006 |
| Predictors of mRS 0–2 | |||
| Age | 0.950 | 0.943–0.957 | <0.0001 |
| Atrial fibrillation | 0.770 | 0.640–0.926 | 0.006 |
| NIHSS | 0.858 | 0.846–0.870 | <0.0001 |
| Large vessel occlusion | 0.630 | 0.543–0.730 | <0.0001 |
| Glucose level | 0.914 | 0.891–0.937 | <0.0001 |
| i.v. antihypertensive therapy before/during IVT | 0.558 | 0.465–0.671 | <0.0001 |
| ONT | 0.998 | 0.996–0.999 | <0.0001 |
| Predictors of mRS 6 | |||
| Female sex | 0.703 | 0.558–0.885 | 0.003 |
| Age | 1.080 | 1.066–1.094 | <0.0001 |
| Atrial fibrillation | 1.399 | 1.010–1.781 | <0.006 |
| NIHSS | 1.146 | 1.125–1.167 | <0.0001 |
| Large vessel occlusion | 2.057 | 1.624–2.605 | <0.0001 |
| Glucose level | 1.115 | 1.077–1.156 | <0.0001 |
| Cholesterol level | 0.852 | 0.770–0.942 | 0.002 |
| i.v. antihypertensive therapy before/during IVT | 2.121 | 1.648–2.729 | <0.0001 |
| ONT | 1.004 | 1.002–1.005 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Halúsková, S.; Herzig, R.; Mikulík, R.; Bělašková, S.; Reiser, M.; Jurák, L.; Václavík, D.; Bar, M.; Klečka, L.; Řepík, T.; et al. Intravenous Thrombolysis in Posterior versus Anterior Circulation Stroke: Clinical Outcome Differs Only in Patients with Large Vessel Occlusion. Biomedicines 2024, 12, 404. https://doi.org/10.3390/biomedicines12020404
Halúsková S, Herzig R, Mikulík R, Bělašková S, Reiser M, Jurák L, Václavík D, Bar M, Klečka L, Řepík T, et al. Intravenous Thrombolysis in Posterior versus Anterior Circulation Stroke: Clinical Outcome Differs Only in Patients with Large Vessel Occlusion. Biomedicines. 2024; 12(2):404. https://doi.org/10.3390/biomedicines12020404
Chicago/Turabian StyleHalúsková, Simona, Roman Herzig, Robert Mikulík, Silvie Bělašková, Martin Reiser, Lubomír Jurák, Daniel Václavík, Michal Bar, Lukáš Klečka, Tomáš Řepík, and et al. 2024. "Intravenous Thrombolysis in Posterior versus Anterior Circulation Stroke: Clinical Outcome Differs Only in Patients with Large Vessel Occlusion" Biomedicines 12, no. 2: 404. https://doi.org/10.3390/biomedicines12020404
APA StyleHalúsková, S., Herzig, R., Mikulík, R., Bělašková, S., Reiser, M., Jurák, L., Václavík, D., Bar, M., Klečka, L., Řepík, T., Šigut, V., Tomek, A., Hlinovský, D., Šaňák, D., Vyšata, O., Vališ, M., & on behalf of the Czech SITS Investigators. (2024). Intravenous Thrombolysis in Posterior versus Anterior Circulation Stroke: Clinical Outcome Differs Only in Patients with Large Vessel Occlusion. Biomedicines, 12(2), 404. https://doi.org/10.3390/biomedicines12020404