
Exploring the Therapeutic Potential of Quadripulse rTMS over the Visual Cortex: A Proof-of-Concept Study in Healthy Volunteers and Chronic Migraine Patients with Medication Overuse Headache

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Visual Evoked Potentials (VEP)
2.3. Quadripulse Repetitive Transcranial Magnetic Stimulation (QP rTMS)
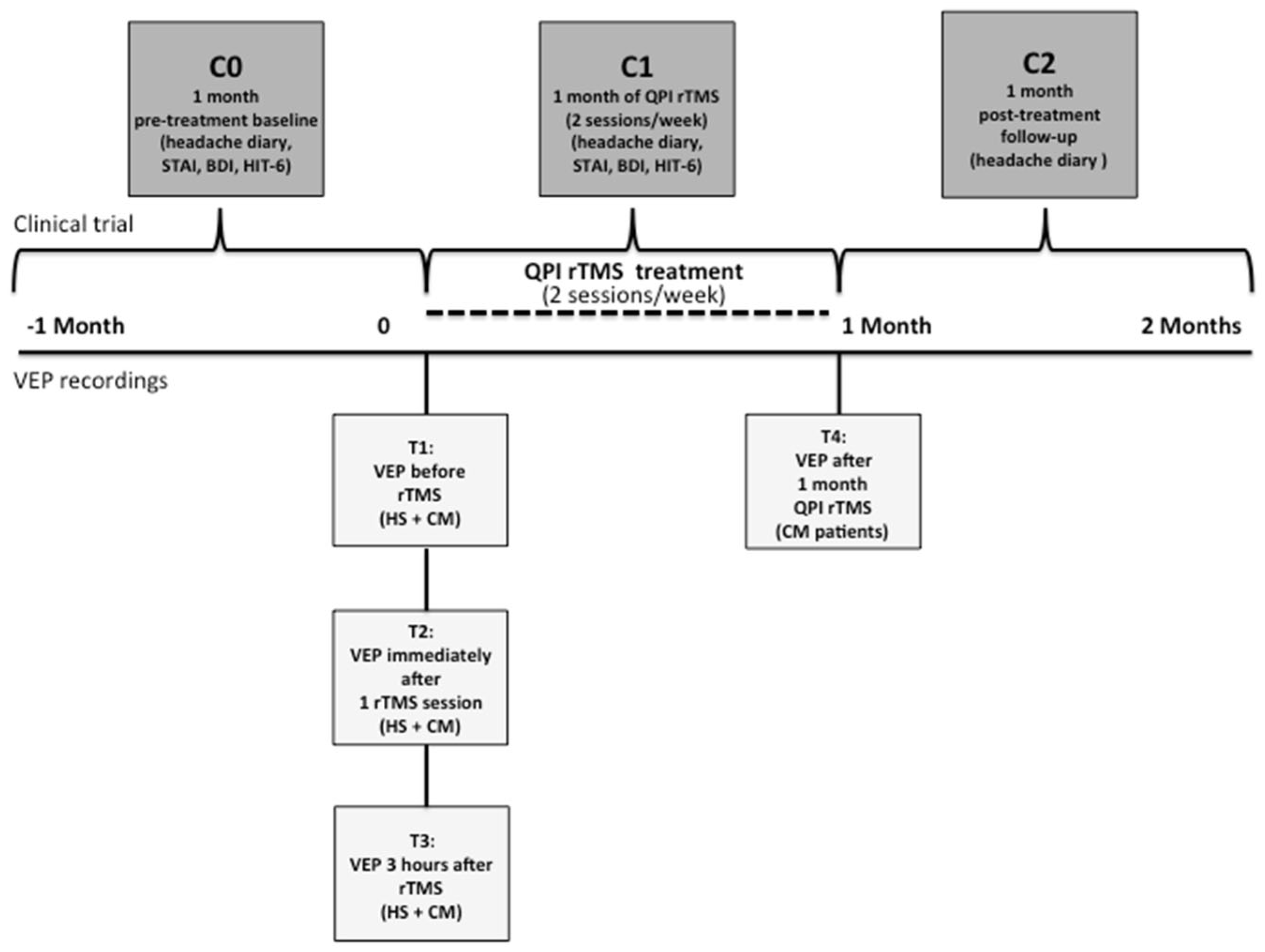
2.4. Study Design
- -
- Electrophysiological study in HS.
- -
- Proof-of-concept therapeutic and electrophysiological study in CM-MOH patients.
2.5. Statistical Analyses
3. Results
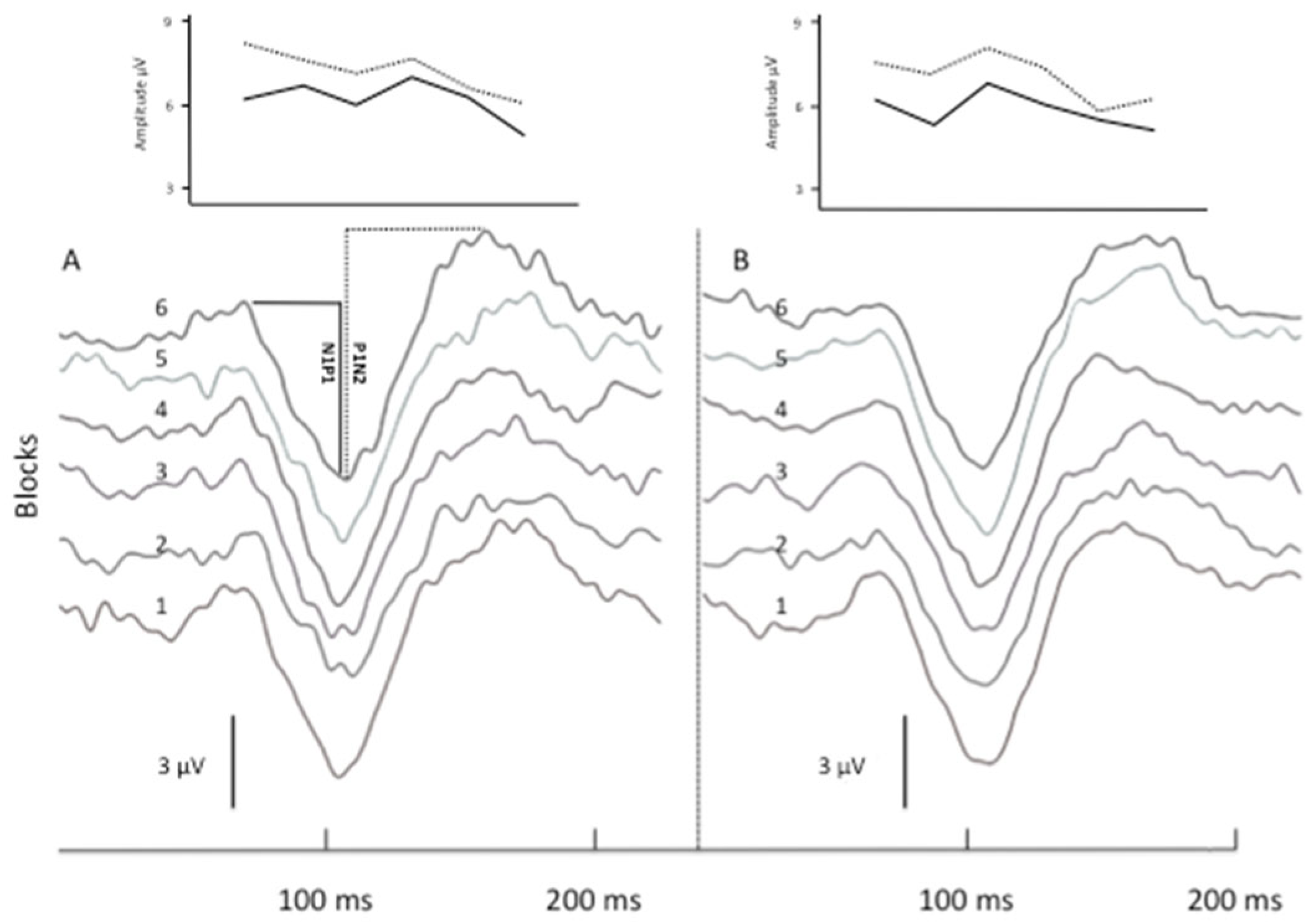
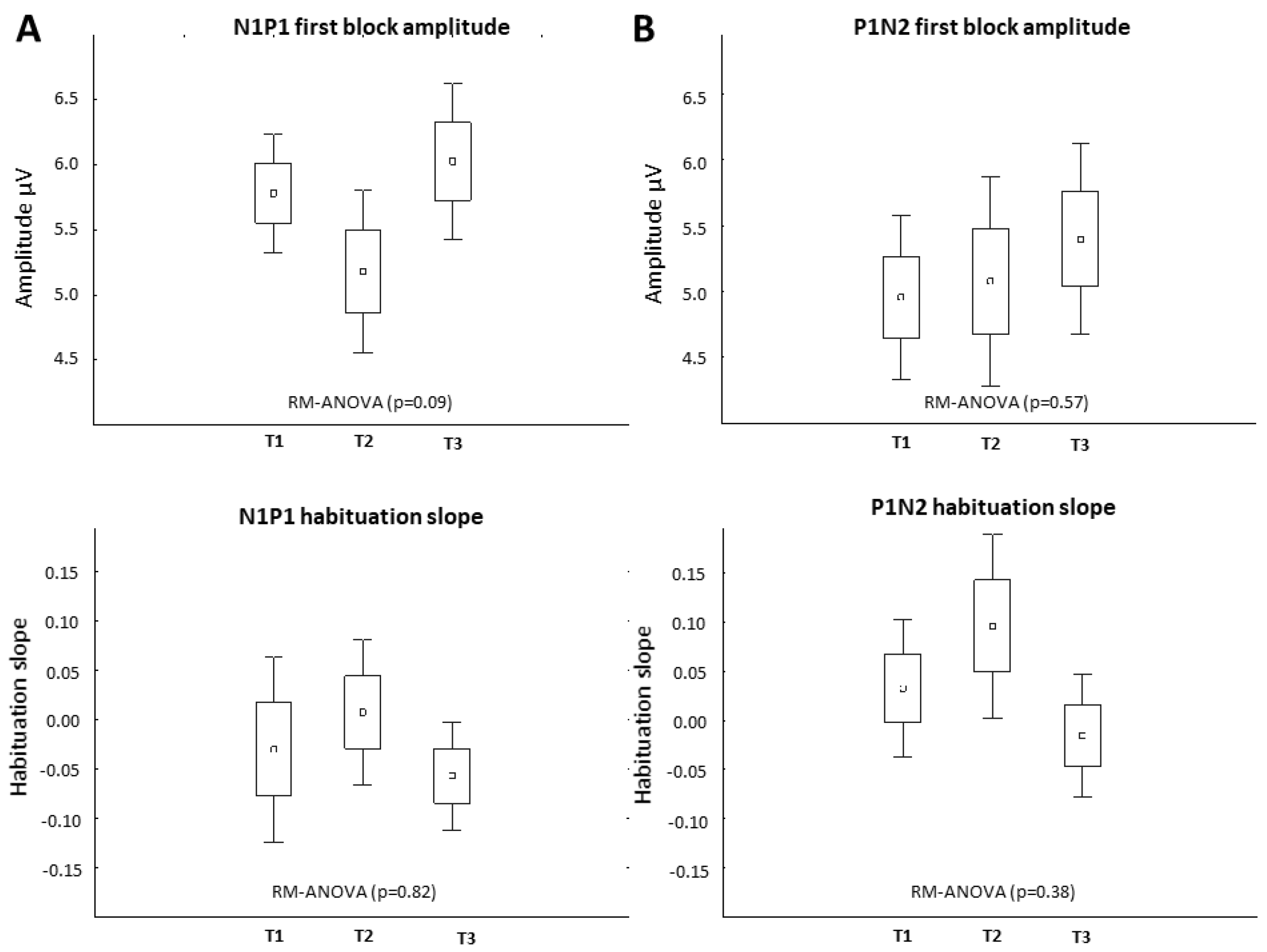
3.1. Electrophysiological Effects in Healthy Subjects
3.2. Clinical Effects of rTMS-QPI in CM-MOH Patients
3.3. Neurophysiological Effects of rTMS-QPI in CM-MOH Patients: Group Level
3.4. Neurophysiological Effects of rTMS-QPI in CM-MOH Patients: Responders vs. Non-Responders
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd Edition. Cephalalgia 2018, 38, 1–211. [CrossRef] [PubMed]
- Paemeleire, K.; Louis, P.; Magis, D.; Vandenheede, M.; Versijpt, J.; Vandersmissen, B.; Schoenen, J. Diagnosis, Pathophysiology and Management of Chronic Migraine: A Proposal of the Belgian Headache Society. Acta Neurol. Belg. 2015, 115, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Bøe, M.G.; Thortveit, E.; Vatne, A.; Mygland, Å. Chronic Headache with Medication Overuse: Long-Term Prognosis after Withdrawal Therapy. Cephalalgia 2017, 37, 1215–1221. [Google Scholar] [CrossRef] [PubMed]
- Schoenen, J.; Manise, M.; Nonis, R.; Gérard, P.; Timmermans, G. Monoclonal Antibodies Blocking CGRP Transmission: An Update on Their Added Value in Migraine Prevention. Rev. Neurol. 2020, 176, 788–803. [Google Scholar] [CrossRef] [PubMed]
- Schoenen, J.; Roberta, B.; Magis, D.; Coppola, G. Noninvasive Neurostimulation Methods for Migraine Therapy: The Available Evidence. Cephalalgia 2016, 36, 1170–1180. [Google Scholar] [CrossRef] [PubMed]
- Ansari, H.; Ziad, S. Drug-Drug Interactions in Headache Medicine. Headache 2016, 56, 1241–1248. [Google Scholar] [CrossRef] [PubMed]
- Viganò, A.; Toscano, M.; Puledda, F.; Di Piero, V. Treating Chronic Migraine With Neuromodulation: The Role of Neurophysiological Abnormalities and Maladaptive Plasticity. Front. Pharmacol. 2019, 10, 32. [Google Scholar] [CrossRef] [PubMed]
- Barker, A.T.; Shields, K. Transcranial Magnetic Stimulation: Basic Principles and Clinical Applications in Migraine. Headache 2017, 57, 517–524. [Google Scholar] [CrossRef]
- Andreou, A.P.; Holland, P.R.; Akerman, S.; Summ, O.; Fredrick, J.; Goadsby, P.J. Transcranial magnetic stimulation and potential cortical and trigeminothalamic mechanisms in migraine. Brain 2016, 139 Pt 7, 2002–2014. [Google Scholar] [CrossRef]
- Schoenen, J.; Ambrosini, A.; Sándor, P.S.; Maertens de Noordhout, A. Evoked Potentials and Transcranial Magnetic Stimulation in Migraine: Published Data and Viewpoint on Their Pathophysiologic Significance. Clin. Neurophysiol. 2003, 114, 955–972. [Google Scholar] [CrossRef]
- Rossi, S.; Antal, A.; Bestmannm, S.; Bikson, M.; Brewer, C.; Brockmöller, J.; Carpenter, L.L.; Cincotta, M.; Chen, R.; Daskalakis, J.D.; et al. Basis of this article began with a Consensus Statement from the IFCN Workshop on “Present, Future of TMS: Safety, Ethical Guidelines”, Siena, 17–20 October 2018, updating through April 2020. Safety and recommendations for TMS use in healthy subjects and patient populations, with updates on training, ethical and regulatory issues: Expert Guidelines. Clin. Neurophysiol. 2021, 132, 269–306. [Google Scholar] [CrossRef] [PubMed]
- Coppola, G.; Di Lorenzo, C.; Serrao, M.; Parisi, V.; Schoenen, J.; Pierelli, F. Pathophysiological Targets for Non-Pharmacological Treatment of Migraine. Cephalalgia 2016, 36, 1103–1111. [Google Scholar] [CrossRef] [PubMed]
- De Tommaso, M.; Ambrosini, A.; Brighina, F.; Coppola, G.; Perrotta, A.; Pierelli, F.; Sandrini, G.; Valeriani, M.; Marinazzo, D.; Stramaglia, S.; et al. Altered Processing of Sensory Stimuli in Patients with Migraine. Nat. Rev. Neurol. 2014, 10, 144–155. [Google Scholar] [CrossRef] [PubMed]
- Puledda, F.; Viganò, A.; Sebastianelli, G.; Parisi, V.; Hsiao, F.-J.; Wang, S.-J.; Chen, W.-T.; Massimini, M.; Coppola, G. Electrophysiological Findings in Migraine May Reflect Abnormal Synaptic Plasticity Mechanisms: A Narrative Review. Cephalalgia 2023, 43, 3331024231195780. [Google Scholar] [CrossRef] [PubMed]
- Coppola, G.; Pierelli, F.; Schoenen, J. Is the Cerebral Cortex Hyperexcitable or Hyperresponsive in Migraine? Cephalalgia 2007, 27, 1427–1439. [Google Scholar] [CrossRef]
- Coppola, G.; Schoenen, J. Cortical Excitability in Chronic Migraine. Curr. Pain Headache Rep. 2012, 16, 93–100. [Google Scholar] [CrossRef]
- Chen, W.-T.; Wang, S.-J.; Fuh, J.-L.; Ko, Y.-C.; Lee, Y.-C.; Hämäläinen, M.S.; Lin, Y.-Y. Visual Cortex Excitability and Plasticity Associated with Remission from Chronic to Episodic Migraine. Cephalalgia 2012, 32, 537–543. [Google Scholar] [CrossRef]
- Burke, M.J.; Joutsa, J.; Cohen, A.L.; Soussand, L.; Cooke, D.; Burstein, R.; Fox, M.D. Mapping Migraine to a Common Brain Network. Brain J. Neurol. 2020, 143, 541–553. [Google Scholar] [CrossRef]
- Brighina, F.; Piazza, A.; Vitello, G.; Aloisio, A.; Palermo, A.; Daniele, O.; Fierro, B. RTMS of the Prefrontal Cortex in the Treatment of Chronic Migraine: A Pilot Study. J. Neurol. Sci. 2004, 227, 67–71. [Google Scholar] [CrossRef]
- Conforto, A.B.; Amaro, E.; Gonçalves, A.L.; Mercante, J.P.; Guendler, V.Z.; Ferreira, J.R.; Kirschner, C.C.; Peres, M.F. Randomized, Proof-of-Principle Clinical Trial of Active Transcranial Magnetic Stimulation in Chronic Migraine. Cephalalgia 2014, 34, 464–472. [Google Scholar] [CrossRef]
- Granato, A.; Fantini, J.; Monti, F.; Furlanis, G.; Musho Ilbeh, S.; Semenic, M.; Manganotti, P. Dramatic Placebo Effect of High Frequency Repetitive TMS in Treatment of Chronic Migraine and Medication Overuse Headache. J. Clin. Neurosci. 2019, 60, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Hulla, R.; Liegey-Dougall, A. A Systematic Review of High-Frequency Transcranial Magnetic Stimulation on Motor Cortex Areas as a Migraine Preventive Treatment. Cephalalgia Rep. 2019, 2, 2515816319889971. [Google Scholar] [CrossRef]
- Misra, U.K.; Kalita, J.; Bhoi, S.K. High-Rate Repetitive Transcranial Magnetic Stimulation in Migraine Prophylaxis: A Randomized, Placebo-Controlled Study. J. Neurol. 2013, 260, 2793–2801. [Google Scholar] [CrossRef] [PubMed]
- Zhong, J.; Lan, W.; Feng, Y.; Yu, L.; Xiao, R.; Shen, Y.; Zou, Z.; Hou, X. Efficacy of Repetitive Transcranial Magnetic Stimulation on Chronic Migraine: A Meta-Analysis. Front. Neurol. 2022, 13, 1050090. [Google Scholar] [CrossRef] [PubMed]
- Lipton, R.B.; Dodick, D.W.; Silberstein, S.D.; Saper, J.R.; Aurora, S.K.; Pearlman, S.H.; Fischell, R.E.; Ruppel, P.L.; Goadsby, P.J. Single-Pulse Transcranial Magnetic Stimulation for Acute Treatment of Migraine with Aura: A Randomised, Double-Blind, Parallel-Group, Sham-Controlled Trial. Lancet Neurol. 2010, 9, 373–380. [Google Scholar] [CrossRef]
- Starling, A.J.; Tepper, S.J.; Marmura, M.J.; Shamim, E.A.; Robbins, M.S.; Hindiyeh, N.; Charles, A.C.; Goadsby, P.J.; Lipton, R.B.; Silberstein, S.D.; et al. A Multicenter, Prospective, Single Arm, Open Label, Observational Study of STMS for Migraine Prevention (ESPOUSE Study). Cephalalgia 2018, 38, 1038–1048. [Google Scholar] [CrossRef] [PubMed]
- Fumal, A.; Coppola, G.; Bohotin, V.; Gérardy, P.-Y.; Seidel, L.; Donneau, A.-F.; Vandenheede, M.; Maertens de Noordhout, A.; Schoenen, J. Induction of Long-Lasting Changes of Visual Cortex Excitability by Five Daily Sessions of Repetitive Transcranial Magnetic Stimulation (RTMS) in Healthy Volunteers and Migraine Patients. Cephalalgia 2006, 26, 143–149. [Google Scholar] [CrossRef]
- Hamada, M.; Terao, Y.; Hanajima, R.; Shirota, Y.; Nakatani-Enomoto, S.; Furubayashi, T.; Matsumoto, H.; Ugawa, Y. Bidirectional Long-Term Motor Cortical Plasticity and Metaplasticity Induced by Quadripulse Transcranial Magnetic Stimulation. J. Physiol. 2008, 586, 3927–3947. [Google Scholar] [CrossRef]
- Rossi, S.; Hallett, M.; Rossini, P.M.; Pascual-Leone, A. Safety of TMS Consensus Group Safety, Ethical Considerations, and Application Guidelines for the Use of Transcranial Magnetic Stimulation in Clinical Practice and Research. Clin. Neurophysiol. 2009, 120, 2008–2039. [Google Scholar] [CrossRef]
- Hamada, M.; Hanajima, R.; Terao, Y.; Okabe, S.; Nakatani-Enomoto, S.; Furubayashi, T.; Matsumoto, H.; Shirota, Y.; Ohminami, S.; Ugawa, Y. Primary Motor Cortical Metaplasticity Induced by Priming over the Supplementary Motor Area. J. Physiol. 2009, 587, 4845–4862. [Google Scholar] [CrossRef]
- Hamada, M.; Ugawa, Y. Quadripulse stimulation—A new patterned rTMS. Restor. Neurol. Neurosci. 2010, 28, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Shirahige, L.; Melo, L.; Nogueira, F.; Rocha, S.; Monte-Silva, K. Efficacy of Noninvasive Brain Stimulation on Pain Control in Migraine Patients: A Systematic Review and Meta-Analysis. Headache 2016, 56, 1565–1596. [Google Scholar] [CrossRef]
- Chen, Y.L.; Chen, Q.; Li, L.W.; Hua, C.; Zhang, X.Y.; Zheng, H. Non-invasive brain stimulation treatments for migraine prophylaxis: A network meta-analysis of randomized controlled trials. Acta Neurol. Belg. 2023, 123, 1481–1493. [Google Scholar] [CrossRef] [PubMed]
- Reuter, U.; McClure, C.; Liebler, E.; Pozo-Rosich, P. Non-invasive neuromodulation for migraine and cluster headache: A systematic review of clinical trials. J. Neurol. Neurosurg. Psychiatry 2019, 90, 796–804. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Zhang, B.; Zhang, J.; Yin, Y. Effects of Non-invasive Brain Stimulation on Headache Intensity and Frequency of Headache Attacks in Patients With Migraine: A Systematic Review and Meta-Analysis. Headache 2019, 59, 1436–1447. [Google Scholar] [CrossRef] [PubMed]
- Moisset, X.; Pereira, B.; Ciampi de Andrade, D.; Fontaine, D.; Lantéri-Minet, M.; Mawet, J. Neuromodulation techniques for acute and preventive migraine treatment: A systematic review and meta-analysis of randomized controlled trials. J. Headache Pain 2020, 21, 142. [Google Scholar] [CrossRef]
- Cheng, Y.C.; Zeng, B.Y.; Hung, C.M.; Su, K.P.; Wu, Y.C.; Tu, Y.K.; Lin, P.Y.; Stubbs, B.; Carvalho, A.F.; Liang, C.S.; et al. Effectiveness and acceptability of noninvasive brain and nerve stimulation techniques for migraine prophylaxis: A network meta-analysis of randomized controlled trials. J. Headache Pain 2022, 23, 28. [Google Scholar] [CrossRef]
- Lan, L.; Zhang, X.; Li, X.; Rong, X.; Peng, Y. The efficacy of transcranial magnetic stimulation on migraine: A meta-analysis of randomized controlled trails. J. Headache Pain 2017, 18, 86. [Google Scholar] [CrossRef]
- Sahu, A.K.; Sinha, V.K.; Goyal, N. Effect of adjunctive intermittent theta-burst repetitive transcranial magnetic stimulation as a prophylactic treatment in migraine patients: A double-blind sham-controlled study. Indian J. Psychiatry 2019, 61, 139–145. [Google Scholar] [CrossRef]
- Kalita, J.; Laskar, S.; Bhoi, S.K.; Misra, U.K. Efficacy of single versus three sessions of high-rate repetitive transcranial magnetic stimulation in chronic migraine and tension-type headache. J. Neurol. 2016, 263, 2238–2246. [Google Scholar] [CrossRef]
- Lau, C.I.; Chen, W.H.; Walsh, V. The visual system as target of non-invasive brain stimulation for migraine treatment: Current insights and future challenges. Prog. Brain Res. 2020, 255, 207–247. [Google Scholar] [CrossRef] [PubMed]
- Coppola, G.; Currà, A.; Di Lorenzo, C.; Parisi, V.; Gorini, M.; Sava, S.L.; Schoenen, J.; Pierelli, F. Abnormal Cortical Responses to Somatosensory Stimulation in Medication-Overuse Headache. BMC Neurol. 2010, 10, 126. [Google Scholar] [CrossRef] [PubMed]
- Kalita, J.; Bhoi, S.K.; Misra, U.K. Effect of High Rate RTMS on Somatosensory Evoked Potential in Migraine. Cephalalgia 2017, 37, 1222–1230. [Google Scholar] [CrossRef] [PubMed]
- Vezzani, A.; Viviani, B. Neuromodulatory Properties of Inflammatory Cytokines and Their Impact on Neuronal Excitability. Neuropharmacology 2015, 96, 70–82. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.-A.; Jung, K.-Y.; Park, B.; Kim, T.-J.; Jun, J.-S.; Kim, K.T.; Yang, T.-W.; Lee, S.-T.; Jung, K.-H.; Chu, K.; et al. Impact of a Selective Cyclooxygenase-2 Inhibitor, Celecoxib, on Cortical Excitability and Electrophysiological Properties of the Brain in Healthy Volunteers: A Randomized, Double-Blind, Placebo-Controlled Study. PLoS ONE 2019, 14, e0212689. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.; Roy, A.; Kundu, M.; Jana, M.; Luan, C.-H.; Gonzalez, F.J.; Pahan, K. Aspirin Binds to PPARα to Stimulate Hippocampal Plasticity and Protect Memory. Proc. Natl. Acad. Sci. USA 2018, 115, E7408–E7417. [Google Scholar] [CrossRef] [PubMed]
- Cortese, F.; Pierelli, F.; Pauri, F.; Di Lorenzo, C.; Lepre, C.; Malavolta, G.; Merluzzo, C.; Parisi, V.; Serrao, M.; Coppola, G. Short-Term Cortical Synaptic Depression/Potentiation Mechanisms in Chronic Migraine Patients with or without Medication Overuse. Cephalalgia 2019, 39, 237–244. [Google Scholar] [CrossRef]
- Meissner, K.; Fässler, M.; Rücker, G.; Kleijnen, J.; Hróbjartsson, A.; Schneider, A.; Antes, G.; Linde, K. Differential Effectiveness of Placebo Treatments: A Systematic Review of Migraine Prophylaxis. JAMA Intern. Med. 2013, 173, 1941–1951. [Google Scholar] [CrossRef]
- Omland, P.M.; Nilsen, K.B.; Uglem, M.; Gravdahl, G.; Linde, M.; Hagen, K.; Sand, T. Visual evoked potentials in interictal migraine: No confirmation of abnormal habituation. Headache 2013, 53, 1071–1086. [Google Scholar] [CrossRef]
- Abbas Abdulhussein, M.; Alyasseri, Z.A.A.; Mohammed, H.J.; An, X. Lack of Habituation in Migraine Patients Based on High-Density EEG Analysis Using the Steady State of Visual Evoked Potential. Entropy 2022, 24, 1688. [Google Scholar] [CrossRef]
- Chamanzar, A.; Haigh, S.M.; Grover, P.; Behrmann, M. Abnormalities in cortical pattern of coherence in migraine detected using ultra high-density EEG. Brain Commun. 2021, 3, fcab061. [Google Scholar] [CrossRef] [PubMed]
- Thiele, A.; Klehr, L.; Strauß, S.; Angermaier, A.; Schminke, U.; Kronenbuerger, M.; Naegel, S.; Fleischmann, R. Preventive treatment with CGRP monoclonal antibodies restores brain stem habituation deficits and excitability to painful stimuli in migraine: Results from a prospective case-control study. J. Headache Pain 2021, 22, 149. [Google Scholar] [CrossRef] [PubMed]
- Di Lorenzo, C.; Coppola, G.; Bracaglia, M.; Di Lenola, D.; Sirianni, G.; Rossi, P.; Di Lorenzo, G.; Parisi, V.; Serrao, M.; Cervenka, M.C.; et al. A ketogenic diet normalizes interictal cortical but not subcortical responsivity in migraineurs. BMC Neurol. 2019, 19, 136. [Google Scholar] [CrossRef]
- Helling, R.M.; Perenboom, M.J.L.; Bauer, P.R.; Carpay, J.A.; Sander, J.W.; Ferrari, M.D.; Visser, G.H.; Tolner, E.A. TMS-evoked EEG potentials demonstrate altered cortical excitability in migraine with aura. Brain Topogr. 2023, 36, 269–281. [Google Scholar] [CrossRef] [PubMed]
- Bauer, P.R.; Helling, R.M.; Perenboom, M.J.L.; Lopes da Silva, F.H.; Tolner, E.A.; Ferrari, M.D.; Sander, J.W.; Visser, G.H.; Kalitzin, S.N. Phase clustering in transcranial magnetic stimulation-evoked EEG responses in genetic generalized epilepsy and migraine. Epilepsy Behav. 2019, 93, 102–112. [Google Scholar] [CrossRef]
- D’Ambrosio, S.; Jiménez-Jiménez, D.; Silvennoinen, K.; Zagaglia, S.; Perulli, M.; Poole, J.; Comolatti, R.; Fecchio, M.; Sisodiya, S.M.; Balestrini, S. Physiological symmetry of transcranial magnetic stimulation-evoked EEG spectral features. Hum Brain Mapp. 2022, 43, 5465–5477. [Google Scholar] [CrossRef] [PubMed]
- Rosanova, M.; Casali, A.; Bellina, V.; Resta, F.; Mariotti, M.; Massimini, M. Natural frequencies of human corticothalamic circuits. J. Neurosci. 2009, 29, 7679–7685. [Google Scholar] [CrossRef] [PubMed]
- Chamanzar, A.; Behrmann, M.; Grover, P. Neural silences can be localized rapidly using noninvasive scalp EEG. Commun. Biol. 2021, 4, 429. [Google Scholar] [CrossRef]
- Mansour, A.G.; Ahdab, R.; Khazen, G.; El-Khoury, C.; Sabbouh, T.M.; Salem, M.; Yamak, W.; Chalah, M.A.; Ayache, S.S.; Riachi, N. Transcranial Direct Current Stimulation of the Occipital Cortex in Medication Overuse Headache: A Pilot Randomized Controlled Cross-Over Study. J. Clin. Med. 2020, 9, 1075. [Google Scholar] [CrossRef]
- Groves, P.M.; Thompson, R.F. Habituation: A dual-process theory. Psychol. Rev. 1970, 77, 419–450. [Google Scholar] [CrossRef]
- Thompson, R.F.; Spencer, W.A. Habituation: A model phenomenon for the study of neuronal substrates of behavior. Psychol. Rev. 1966, 73, 16–43. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| rTMS-QPE | ||||||
|---|---|---|---|---|---|---|
| VEP | T1 | T2 | T3 | T1–T2 Δ | T1–T3 Δ | |
| N1P1 | 1st Block Amplitude (μV) | 6.7 ± 2.44 | 6.6 ± 2.44 | 6.6 ± 1.89 | = | = |
| Habituation Slope | −0.22 ± 0.31 | −0.21 ± 0.14 | −0.22 ± 0.25 | = | = | |
| P1N2 | 1st Block Amplitude (μV) | 5.4 ± 2.38 | 5.5 ± 1.71 | 6.3 ± 2.13 | = | 🡹 |
| Habituation Slope | −0.13 ± 0.31 | −0.14 ± 0.22 | −0.27 ± 0.36 | = | 🢃 | |
| rTMS-QPI | ||||||
| VEP | ||||||
| N1P1 | 1st Block Amplitude (μV) | 5.5 ± 2.39 | 5.3 ± 2.07 | 5.2 ± 2.34 | = | 🢃 |
| Habituation Slope | −0.04 ± 0.16 | −0.12 ± 0.24 | 0.04 ± 0.23 | = | 🡹 | |
| P1N2 | 1st Block Amplitude (μV) | 6.1 ± 2.17 | 5.2 ± 1.77 | 5.0 ± 1.99 | 🢃 | 🢃 |
| Habituation Slope | −0.08 ± 0.23 | 0.01 ± 0.24 | 0.06 ± 0.19 | 🡹 | 🡹 | |
| rTMS-QPI | |||||
|---|---|---|---|---|---|
| VEP | T1 | T4 | |||
| 1st Block Amplitude | N1P1 | Responders | 6.39 ± 1.44 | 7.70 ± 1.75 | = |
| Non-responders | 5.29 ± 1.23 | 5.23 ± 1.28 | = | ||
| P1N2 | Responders | 5.70 ± 1.75 | 6.96 ± 0.72 | = | |
| Non-responders | 4.36 ± 1.97 | 4.20 ± 0.66 | = | ||
| Habituation slope | N1P1 | Responders | −0.08 ± 0.36 | −0.33 ± 0.26 | 🢃 |
| Non-responders | 0.01 ± 0.24 | 0.21 ± 0.36 | = | ||
| P1N2 | Responders | −0.001 ± 0.19 | −0.23 ± 0.25 | 🢃 | |
| Non-responders | 0.06 ± 0.24 | 0.37 ± 0.46 | = | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viganò, A.; Sasso D’Elia, T.; Sava, S.L.; Colosimo, A.; Di Piero, V.; Magis, D.; Schoenen, J. Exploring the Therapeutic Potential of Quadripulse rTMS over the Visual Cortex: A Proof-of-Concept Study in Healthy Volunteers and Chronic Migraine Patients with Medication Overuse Headache. Biomedicines 2024, 12, 288. https://doi.org/10.3390/biomedicines12020288
Viganò A, Sasso D’Elia T, Sava SL, Colosimo A, Di Piero V, Magis D, Schoenen J. Exploring the Therapeutic Potential of Quadripulse rTMS over the Visual Cortex: A Proof-of-Concept Study in Healthy Volunteers and Chronic Migraine Patients with Medication Overuse Headache. Biomedicines. 2024; 12(2):288. https://doi.org/10.3390/biomedicines12020288
Chicago/Turabian StyleViganò, Alessandro, Tullia Sasso D’Elia, Simona Liliana Sava, Alfredo Colosimo, Vittorio Di Piero, Delphine Magis, and Jean Schoenen. 2024. "Exploring the Therapeutic Potential of Quadripulse rTMS over the Visual Cortex: A Proof-of-Concept Study in Healthy Volunteers and Chronic Migraine Patients with Medication Overuse Headache" Biomedicines 12, no. 2: 288. https://doi.org/10.3390/biomedicines12020288
APA StyleViganò, A., Sasso D’Elia, T., Sava, S. L., Colosimo, A., Di Piero, V., Magis, D., & Schoenen, J. (2024). Exploring the Therapeutic Potential of Quadripulse rTMS over the Visual Cortex: A Proof-of-Concept Study in Healthy Volunteers and Chronic Migraine Patients with Medication Overuse Headache. Biomedicines, 12(2), 288. https://doi.org/10.3390/biomedicines12020288