
Comparative Analysis of Resmetirom vs. FGF21 Analogs vs. GLP-1 Agonists in MASLD and MASH: Network Meta-Analysis of Clinical Trials

Abstract
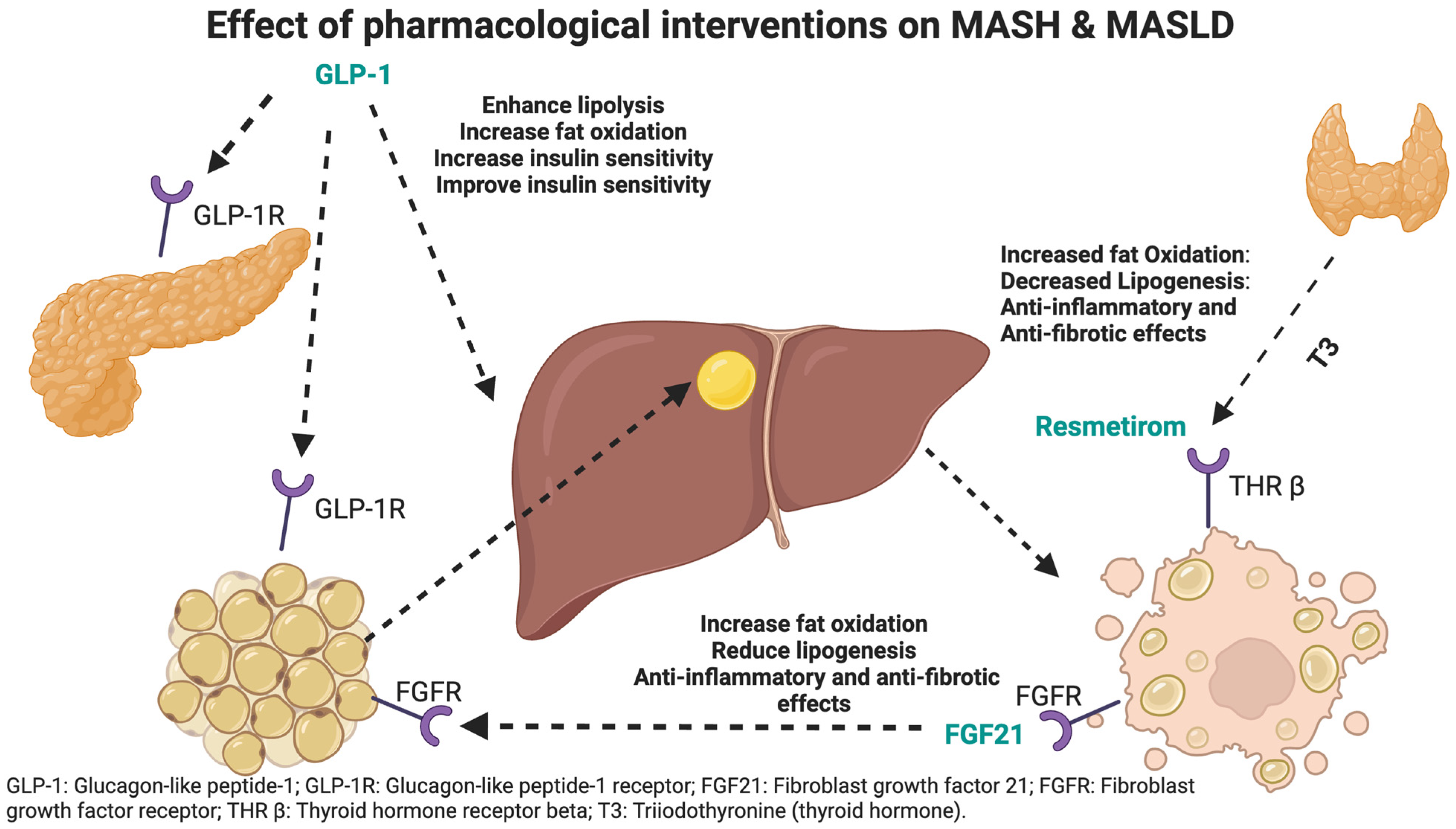
1. Introduction
2. Methods
2.1. Search Strategy
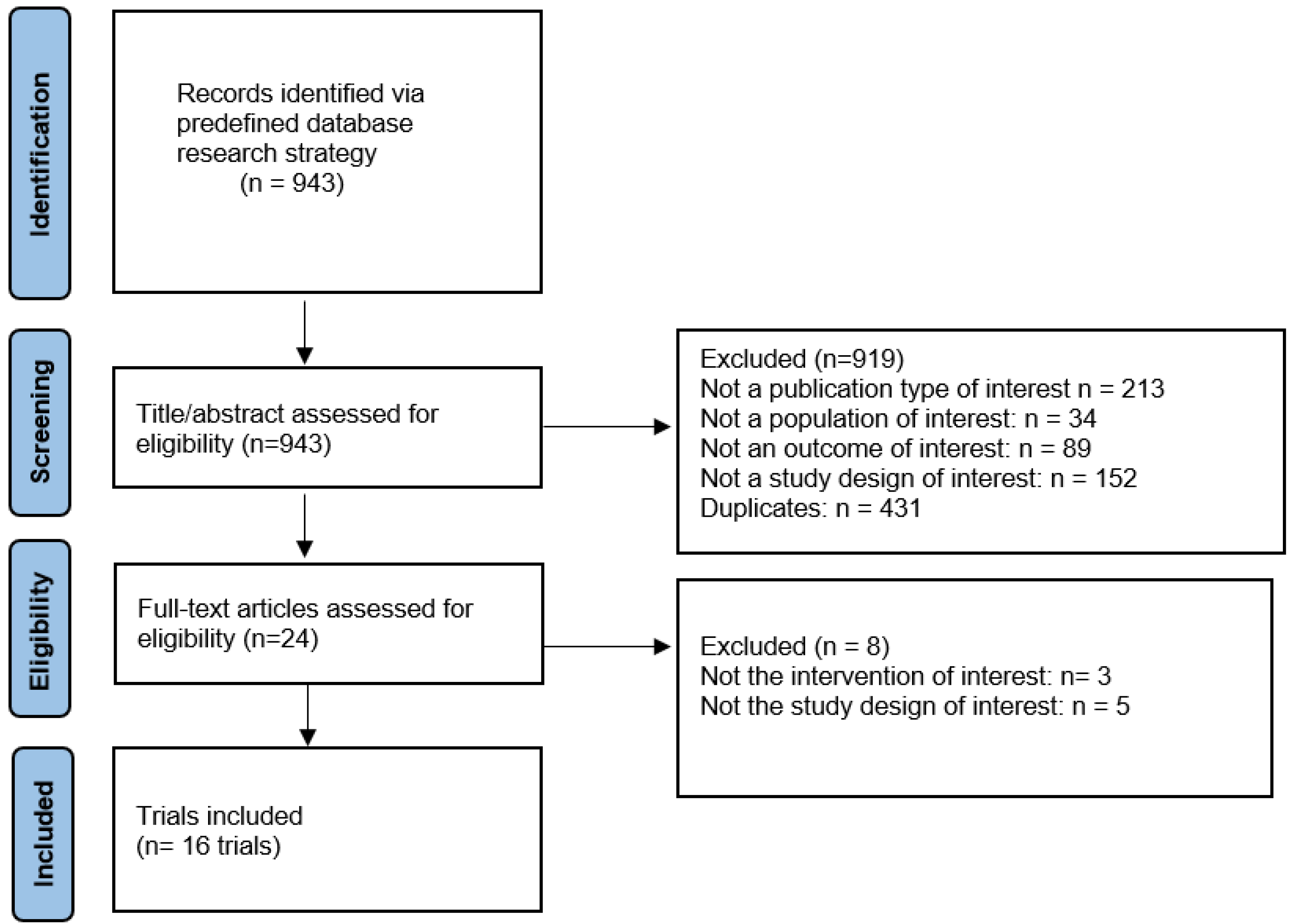
2.2. Screening Process
2.3. Study Selection
2.4. Data Extraction
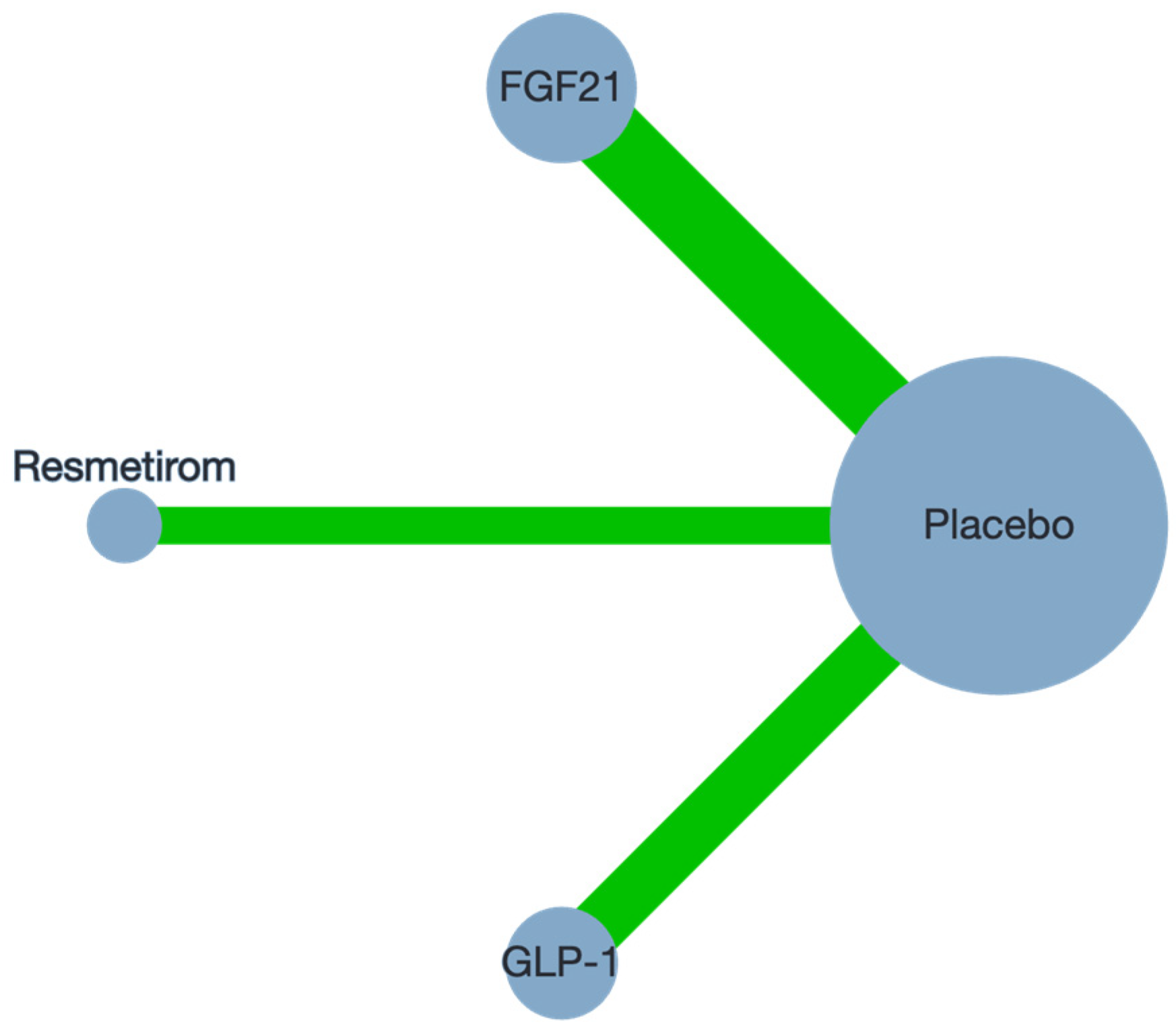
2.5. Statistical Analysis
2.6. Bias Assessment and Certainty of Evidence
3. Results
3.1. Study Characteristics
3.2. Sensitivity Analysis and Meta-Regression
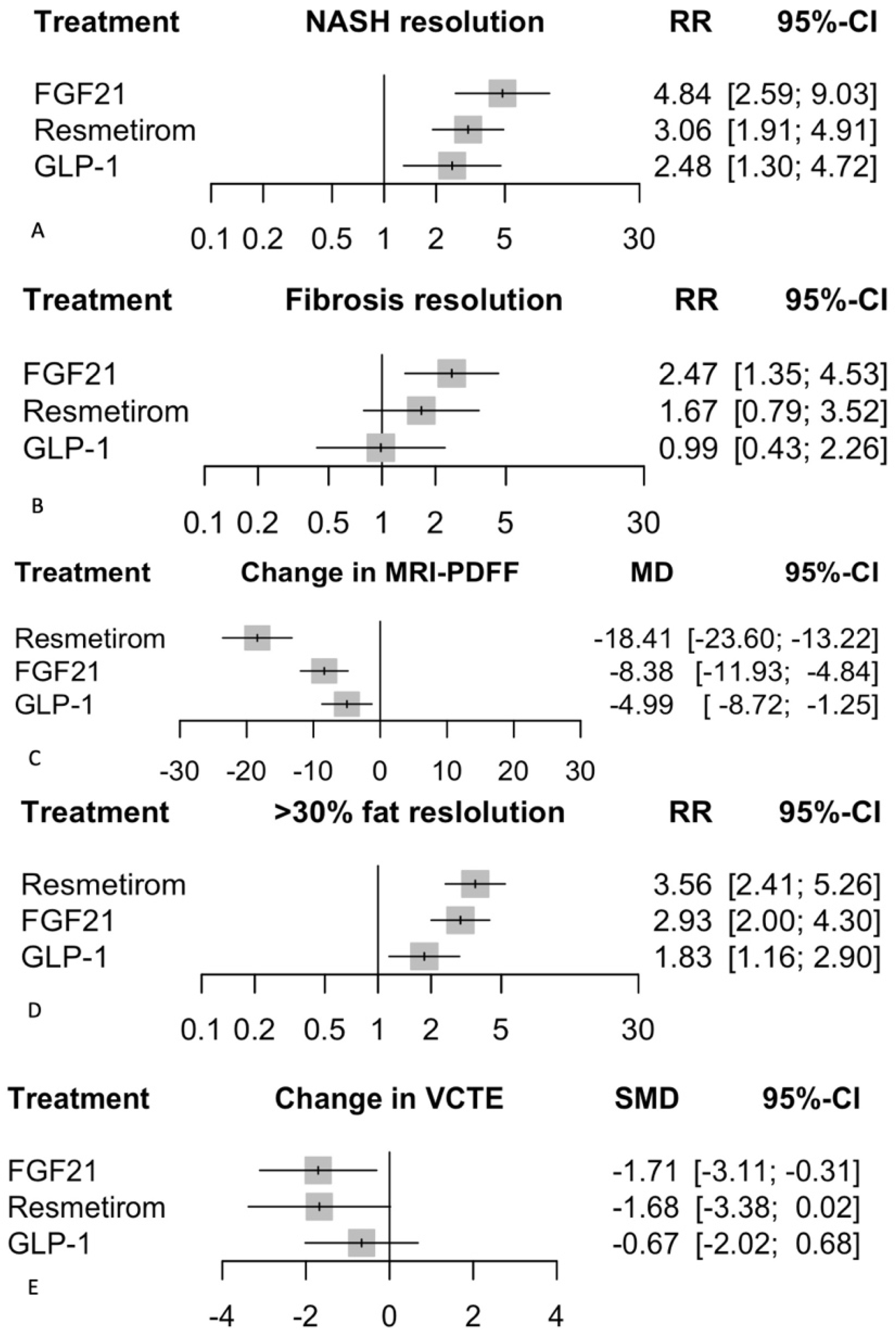
3.3. Biopsy Outcomes
3.3.1. NASH Resolution
3.3.2. Improvement in Fibrosis
3.4. Imaging Outcomes
3.4.1. Change in MRI-PDFF
3.4.2. >30% Fat Reduction on MRI-PDFF
3.4.3. Change in VCTE
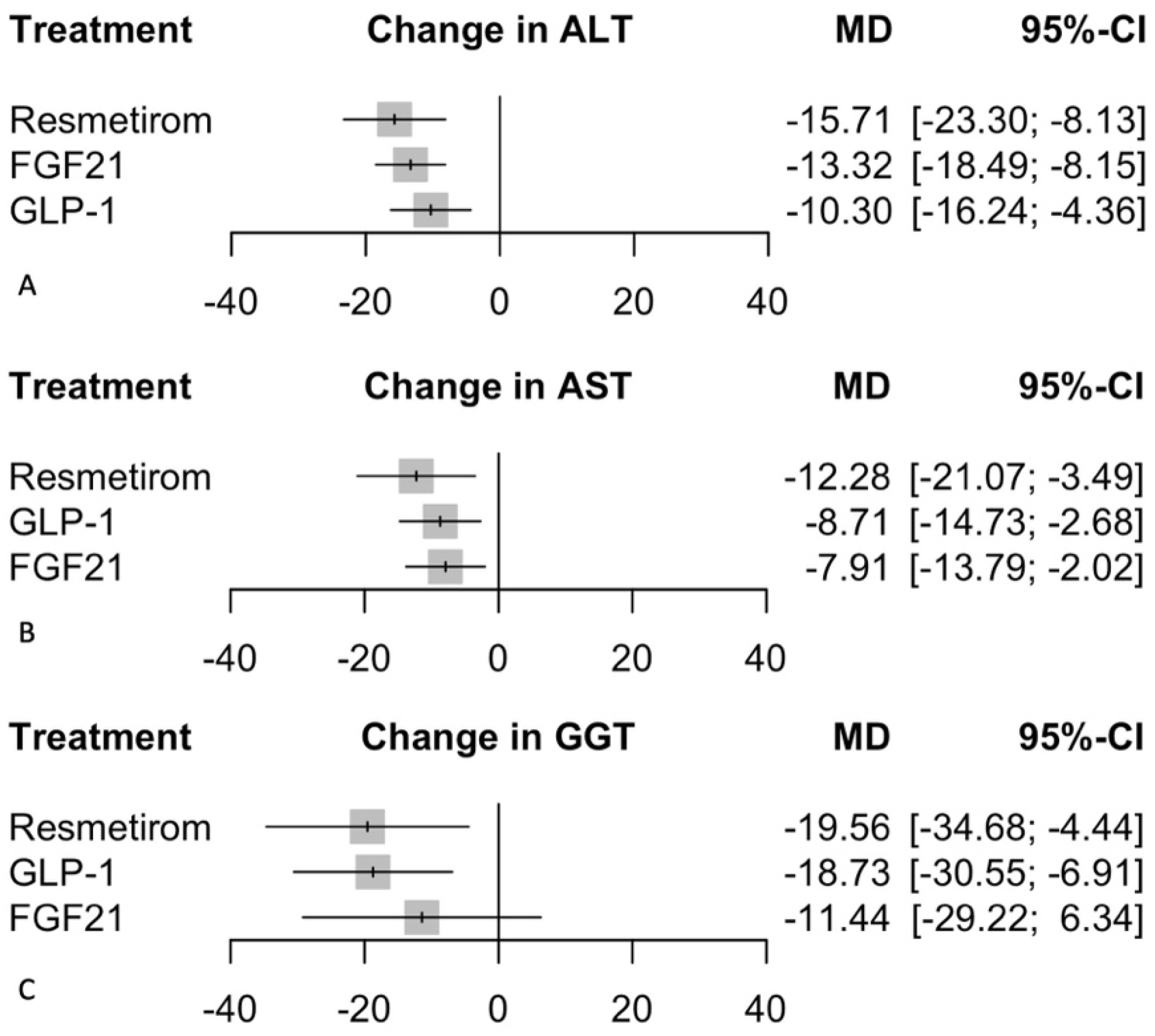
3.5. Biochemical Markers
3.5.1. Change in ALT
3.5.2. Change in AST
3.5.3. Change in GGT
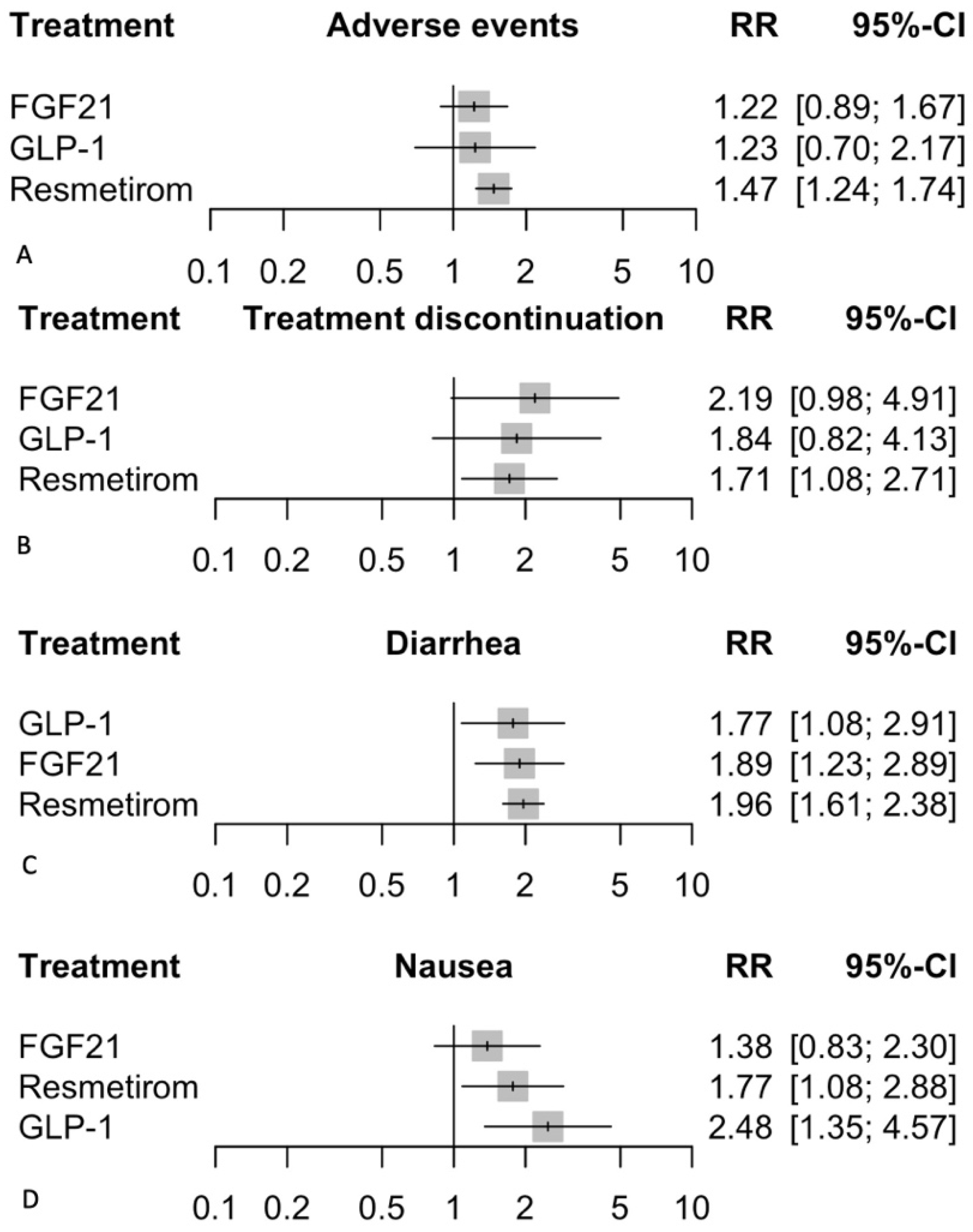
3.6. Safety Outcomes
3.6.1. Adverse Events
3.6.2. Treatment Discontinuation
3.6.3. Nausea
3.6.4. Diarrhea
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Targher, G.; Byrne, C.D.; Tilg, H. MASLD: A systemic metabolic disorder with cardiovascular and malignant complications. Gut 2024, 73, 691–702. [Google Scholar] [CrossRef] [PubMed]
- Sanyal, A.J.; Husain, M.; Diab, C.; Mangla, K.K.; Shoeb, A.; Lingvay, I.; Tapper, E.B. Cardiovascular disease in patients with metabolic dysfunction-associated steatohepatitis compared with metabolic dysfunction-associated steatotic liver disease and other liver diseases: A systematic review. Am. Heart J. Plus 2024, 41, 100386. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Harrison, S.A.; Bashir, M.R.; Guy, C.D.; Zhou, R.; A Moylan, C.; Frias, J.P.; Alkhouri, N.; Bansal, M.B.; Baum, S.; A Neuschwander-Tetri, B.; et al. Resmetirom (MGL-3196) for the treatment of non-alcoholic steatohepatitis: A multicentre, randomised, double-blind, placebo-controlled, phase 2 trial. Lancet 2019, 394, 2012–2024. [Google Scholar] [CrossRef]
- Kliewer, S.A.; Mangelsdorf, D.J. A Dozen Years of Discovery: Insights into the Physiology and Pharmacology of FGF21. Cell Metab. 2019, 29, 246–253. [Google Scholar] [CrossRef]
- Abdelmalek, M.F.; Harrison, S.A.; Sanyal, A.J. The role of glucagon-like peptide-1 receptor agonists in metabolic dysfunction-associated steatohepatitis. Diabetes Obes. Metab. 2024, 26, 2001–2016. [Google Scholar] [CrossRef]
- Ayesh, H. Comparative Analysis of Resmetirom vs FGF21 Agonists vs. GLP-1 Agonists in MASLD and MASH: Network Meta-Analysis of Clinical Trials. 2024. Available online: https://osf.io/hxvp3 (accessed on 15 June 2024).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Welch, V.; Higgins, J.P.; Thomas, J. Cochrane Handbook for Systematic Reviews of Interventions, Version 6.3 ed; Cochrane: Hoboken, NJ, USA, 2019. [Google Scholar]
- Rouse, B.; Chaimani, A.; Li, T. Network meta-analysis: An introduction for clinicians. Intern. Emerg. Med. 2017, 12, 103–111. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Allaire, J. RStudio: Integrated Development Environment for R; Posit Software; PBC: Boston, MA, USA, 2023. [Google Scholar]
- Balduzzi, S.; Rücker, G.; Nikolakopoulou, A.; Papakonstantinou, T.; Salanti, G.; Efthimiou, O.; Schwarzer, G. netmeta: An R Package for Network Meta-Analysis Using Frequentist Methods. J. Stat. Softw. 2023, 106, 1–40. [Google Scholar] [CrossRef]
- Rücker, G.; Schwarzer, G. Ranking treatments in frequentist network meta-analysis works without resampling methods. BMC Med. Res. Methodol. 2015, 15, 58. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Nikolakopoulou, A.; Higgins, J.P.T.; Papakonstantinou, T.; Chaimani, A.; Del Giovane, C.; Egger, M.; Salanti, G. CINeMA: An approach for assessing confidence in the results of a network meta-analysis. PLoS Med. 2020, 17, e1003082. [Google Scholar] [CrossRef] [PubMed]
- Abdelmalek, M.F.; Charles, E.D.; Sanyal, A.J.; Harrison, S.A.; Neuschwander-Tetri, B.A.; Goodman, Z.; Ehman, R.A.; Karsdal, M.; Nakajima, A.; Du, S.; et al. The FALCON program: Two phase 2b randomized, double-blind, placebo-controlled studies to assess the efficacy and safety of pegbelfermin in the treatment of patients with nonalcoholic steatohepatitis and bridging fibrosis or compensated cirrhosis. Contemp. Clin. Trials 2021, 104, 106335. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, M.J.; Gaunt, P.; Aithal, G.P.; Barton, D.; Hull, D.; Parker, R.; Hazlehurst, J.M.; Guo, K.; Abouda, G.; A Aldersley, M.; et al. Liraglutide safety and efficacy in patients with non-alcoholic steatohepatitis (LEAN): A multicentre, double-blind, randomised, placebo-controlled phase 2 study. Lancet 2016, 387, 679–690. [Google Scholar] [CrossRef]
- Flint, A.; Andersen, G.; Hockings, P.; Johansson, L.; Morsing, A.; Palle, M.S.; Vogl, T.; Loomba, R.; Plum-Mörschel, L. Randomised clinical trial: Semaglutide versus placebo reduced liver steatosis but not liver stiffness in subjects with non-alcoholic fatty liver disease assessed by magnetic resonance imaging. Aliment. Pharmacol. Ther. 2021, 54, 1150–1161. [Google Scholar] [CrossRef]
- Harrison, S.A.; Ruane, P.J.; Freilich, B.L.; Neff, G.; Patil, R.; Behling, C.A.; Hu, C.; Fong, E.; de Temple, B.; Tillman, E.J.; et al. Efruxifermin in non-alcoholic steatohepatitis: A randomized, double-blind, placebo-controlled, phase 2a trial. Nat. Med. 2021, 27, 1262–1271. [Google Scholar] [CrossRef]
- Loomba, R.; Lawitz, E.J.; Frias, J.P.; Ortiz-Lasanta, G.; Johansson, L.; Franey, B.B.; Morrow, L.; Rosenstock, M.; Hartsfield, C.L.; Chen, C.-Y.; et al. Safety, pharmacokinetics, and pharmacodynamics of pegozafermin in patients with non-alcoholic steatohepatitis: A randomised, double-blind, placebo-controlled, phase 1b/2a multiple-ascending-dose study. Lancet Gastroenterol. Hepatol. 2023, 8, 120–132. [Google Scholar] [CrossRef]
- Harrison, S.A.; Bedossa, P.; Guy, C.D.; Schattenberg, J.M.; Loomba, R.; Taub, R.; Labriola, D.; Moussa, S.E.; Neff, G.W.; Rinella, M.E.; et al. A Phase 3, Randomized, Controlled Trial of Resmetirom in NASH with Liver Fibrosis. N. Engl. J. Med. 2024, 390, 497–509. [Google Scholar] [CrossRef] [PubMed]
- Harrison, S.A.; Taub, R.; Neff, G.W.; Lucas, K.J.; Labriola, D.; Moussa, S.E.; Alkhouri, N.; Bashir, M.R. Resmetirom for nonalcoholic fatty liver disease: A randomized, double-blind, placebo-controlled phase 3 trial. Nat. Med. 2023, 29, 2919–2928. [Google Scholar] [CrossRef] [PubMed]
- Harrison, S.A.; Ruane, P.J.; Freilich, B.; Neff, G.; Patil, R.; Behling, C.; Hu, C.; Shringarpure, R.; de Temple, B.; Fong, E.; et al. A randomized, double-blind, placebo-controlled phase IIa trial of efruxifermin for patients with compensated NASH cirrhosis. JHEP Rep. 2023, 5, 100563. [Google Scholar] [CrossRef] [PubMed]
- Harrison, S.A.; Frias, J.P.; Neff, G.; A Abrams, G.; Lucas, K.J.; Sanchez, W.; Gogia, S.; Sheikh, M.Y.; Behling, C.; Bedossa, P.; et al. Safety and efficacy of once-weekly efruxifermin versus placebo in non-alcoholic steatohepatitis (HARMONY): A multicentre, randomised, double-blind, placebo-controlled, phase 2b trial. Lancet Gastroenterol. Hepatol. 2023, 8, 1080–1093. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.; Abdelmalek, M.F.; Armstrong, M.J.; Jara, M.; Kjær, M.S.; Krarup, N.; Lawitz, E.; Ratziu, V.; Sanyal, A.J.; Schattenberg, J.M.; et al. Semaglutide 2·4 mg once weekly in patients with non-alcoholic steatohepatitis-related cirrhosis: A randomised, placebo-controlled phase 2 trial. Lancet Gastroenterol. Hepatol. 2023, 8, 511–522. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.; Sanyal, A.J.; Kowdley, K.V.; Bhatt, D.L.; Alkhouri, N.; Frias, J.P.; Bedossa, P.; Harrison, S.A.; Lazas, D.; Barish, R.; et al. Randomized, Controlled Trial of the FGF21 Analogue Pegozafermin in NASH. N. Engl. J. Med. 2023, 389, 998–1008. [Google Scholar] [CrossRef] [PubMed]
- Newsome, P.N.; Buchholtz, K.; Cusi, K.; Linder, M.; Okanoue, T.; Ratziu, V.; Sanyal, A.J.; Sejling, A.-S.; Harrison, S.A. A Placebo-Controlled Trial of Subcutaneous Semaglutide in Nonalcoholic Steatohepatitis. N. Engl. J. Med. 2021, 384, 1113–1124. [Google Scholar] [CrossRef] [PubMed]
- Kuchay, M.S.; Krishan, S.; Mishra, S.K.; Farooqui, K.J.; Singh, M.K.; Wasir, J.S.; Bansal, B.; Kaur, P.; Jevalikar, G.; Gill, H.K.; et al. Effect of Empagliflozin on Liver Fat in Patients with Type 2 Diabetes and Nonalcoholic Fatty Liver Disease: A Randomized Controlled Trial (E-LIFT Trial). Diabetes Care 2018, 41, 1801–1808. [Google Scholar] [CrossRef]
- Sanyal, A.; Charles, E.D.; Neuschwander-Tetri, B.A.; Loomba, R.; A Harrison, S.; Abdelmalek, M.F.; Lawitz, E.J.; Halegoua-DeMarzio, D.; Kundu, S.; Noviello, S.; et al. Pegbelfermin (BMS-986036), a PEGylated fibroblast growth factor 21 analogue, in patients with non-alcoholic steatohepatitis: A randomised, double-blind, placebo-controlled, phase 2a trial. Lancet 2019, 392, 2705–2717. [Google Scholar] [CrossRef]
- Guo, W.; Tian, W.; Lin, L.; Xu, X. Liraglutide or insulin glargine treatments improves hepatic fat in obese patients with type 2 diabetes and nonalcoholic fatty liver disease in twenty-six weeks: A randomized placebo-controlled trial. Diabetes Res. Clin. Pract. 2020, 170, 108487. [Google Scholar] [CrossRef]
- Leo, L.; Sunny, M.E. US FDA Approves First Drug for Fatty Liver Disease NASH. Reuters. Available online: https://www.reuters.com/business/healthcare-pharmaceuticals/us-fda-approves-first-drug-fatty-liver-disease-nash-2024-03-14 (accessed on 15 June 2024).
- Bio, I. 89bio Initiates Phase 3 ENLIGHTEN-Fibrosis Trial of Pegozafermin in Non-Cirrhotic Metabolic Dysfunction-Associated Steatohepatitis (MASH) Patients with Fibrosis. Available online: https://ir.89bio.com/news-releases/news-release-details/89bio-initiates-phase-3-enlighten-fibrosis-trial-pegozafermin (accessed on 4 October 2024).
- ClinicalTrials.gov. A Study of Semaglutide in Participants with Nonalcoholic Steatohepatitis (ESSENCE). 4 October 2024. Available online: https://clinicaltrials.gov/study/NCT04822181?cond=NCT04822181&rank=1 (accessed on 5 October 2024).
- Harrison, S.A.; Alkhouri, N.; Davison, B.A.; Sanyal, A.; Edwards, C.; Colca, J.R.; Lee, B.H.; Loomba, R.; Cusi, K.; Kolterman, O.; et al. Insulin sensitizer MSDC-0602K in non-alcoholic steatohepatitis: A randomized, double-blind, placebo-controlled phase IIb study. J. Hepatol. 2020, 72, 613–626. [Google Scholar] [CrossRef]
- Ratziu, V.; Harrison, S.A.; Francque, S.; Bedossa, P.; Lehert, P.; Serfaty, L.; Romero-Gomez, M.; Boursier, J.; Abdelmalek, M.; Caldwell, S.; et al. Elafibranor, an Agonist of the Peroxisome Proliferator-Activated Receptor-α and -δ, Induces Resolution of Nonalcoholic Steatohepatitis Without Fibrosis Worsening. Gastroenterology 2016, 150, 1147–1159.e5. [Google Scholar] [CrossRef] [PubMed]
- Khoo, J.; Hsiang, J.C.; Taneja, R.; Koo, S.H.; Soon, G.H.; Kam, C.J.; Law, N.M.; Ang, T.L. Randomized trial comparing effects of weight loss by liraglutide with lifestyle modification in non-alcoholic fatty liver disease. Liver Int. 2019, 39, 941–949. [Google Scholar] [CrossRef]
- Metzner, V.; Herzog, G.; Heckel, T.; Bischler, T.; Hasinger, J.; Otto, C.; Fassnacht, M.; Geier, A.; Seyfried, F.; Dischinger, U. Liraglutide + PYY(3-36) Combination Therapy Mimics Effects of Roux-en-Y Bypass on Early NAFLD Whilst Lacking-Behind in Metabolic Improvements. J. Clin. Med. 2022, 11, 753. [Google Scholar] [CrossRef] [PubMed]
- Javanbakht, M.; Fishman, J.; Moloney, E.; Rydqvist, P.; Ansaripour, A. Early Cost-Effectiveness and Price Threshold Analyses of Resmetirom: An Investigational Treatment for Management of Nonalcoholic Steatohepatitis. Pharmacoecon Open 2023, 7, 93–110. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.A.; Minnich, A.; Sanyal, A.J.; Loomba, R.; Du, S.; Schwarz, J.; Ehman, R.L.; Karsdal, M.; Leeming, D.J.; Cizza, G.; et al. Effect of pegbelfermin on NASH and fibrosis-related biomarkers and correlation with histological response in the FALCON 1 trial. JHEP Rep. 2023, 5, 100661. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Yu, B.; Bu, Y.; Lou, J.; Jin, Y. Pegbelfermin for reducing transaminase levels in patients with non-alcoholic steatohepatitis: A dose-response meta-analysis of randomized controlled trials. Front. Med. 2024, 11, 1293336. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhao, W.; Bu, H.; Toshiyoshi, M.; Zhao, Y. Liraglutide on type 2 diabetes mellitus with nonalcoholic fatty liver disease: A systematic review and meta-analysis of 16 RCTs. Medicine 2023, 102, e32892. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Design | Registration | Duration | Treatment Arms | Primary Outcomes | Secondary Outcomes | Population |
|---|---|---|---|---|---|---|---|
| Abdelmalek, 2024 [6] | Phase2b, RCT, DB, PC | NCT04031729 | 24 weeks | Pegbelfermin (10 mg, 20 mg, 40 mg weekly), placebo | Improvement in fibrosis without worsening of NASH | NAFLD activity score, liver variables, metabolic variables, safety | Patients with NASH, aged 21–75 years, fibrosis stage F2/F3, NAFLD score ≥4 |
| Armstrong, 2016 [19] | RCT, DB, PC | NCT01237119 | 48 weeks | Liraglutide (1.8 mg daily), placebo | Resolution of NASH without worsening of fibrosis | Changes in NAFLD activity score, liver enzymes, metabolic parameters, quality of life | Patients with NASH, aged 18–75 years, NAFLD activity score ≥4 |
| Flint, 2021 [20] | RCT, DB, PC | NCT03486899 | 48 weeks | Semaglutide (0.4 mg daily), placebo | Change in liver stiffness (MRE) | Changes in liver fat content, liver enzymes, glucose metabolism, cardiovascular risk factors, safety | Patients with NASH, aged 18–75 years, liver stiffness by MRE ≥3.64 kPa |
| Guo, 2020 [32] | RCT, PC | ChiCTR2000035091 | 26 weeks | Placebo, insulin glargine, liraglutide | Changes in IHCL, abdominal adiposity (SAT and VAT) | Changes in liver function (AST, ALT), glycemia (HbA1c, FPG), body weight, BMI | Adults with T2D and NAFLD |
| Harrison, 2021 [21] | RCT, DB, PC, phase 2a | NCT03976401 | 16 weeks | Placebo, efruxifermin 28 mg, 50 mg, 70 mg | Absolute change in hepatic fat fraction (HFF) | Percent change in HFF, responders, change in ALT, safety and tolerability | Adults with biopsy-proven NASH |
| Harrison, 2023 [26] | RCT, DB, PC, phase IIa | NCT03976401 | 26 weeks | Placebo, efruxifermin 50 mg weekly | Safety, tolerability | Change in liver stiffness, non-invasive biomarkers of fibrosis, liver histopathology, markers of liver injury and metabolism | NASH with compensated cirrhosis |
| Harrison, 2023 [25] | RCT, DB, PC, phase 2b | NCT04767529 | 24 weeks | Placebo, efruxifermin 28 mg weekly, 50 mg weekly | Improvement in liver fibrosis by ≥1 stage without worsening of NASH | NASH resolution, change in HFF by MRI-PDFF, non-invasive markers of fibrosis, glycaemic control, lipid metabolism, safety, tolerability, immunogenicity | Adults with NASH and fibrosis stages 2–3 |
| Kuchay, 2018 [30] | RCT, open-label, controlled | NCT02686476 | 20 weeks | Control, empagliflozin 10 mg daily | Change in liver fat content (MRI-PDFF) | Changes in AST, ALT, GGT levels | Adults with T2D and NAFLD |
| Loomba, 2023 [22] | RCT, DB, PC, phase 1b/2a | NCT04048135 | 12 weeks | Placebo, pegozafermin 3 mg, 9 mg, 18 mg weekly, 27 mg weekly, 18 mg biweekly, 36 mg biweekly | Safety, tolerability, pharmacokinetics | Changes in hepatic fat fraction (MRI-PDFF), bodyweight, lipid profile, liver enzymes, immunogenicity | Adults with NASH |
| Loomba, 2023 [28] | Multinational, RCT, DB, PC, phase 2b | NCT04929483 | 24 weeks | Pegozafermin (15 mg, 30 mg weekly, 44 mg biweekly), placebo | Improvement in liver fibrosis, NASH resolution | NAFLD activity score, liver variables, metabolic variables, safety | Patients with NASH, aged 21–75 years, fibrosis stage F2/F3, NAFLD score ≥4 |
| Loomba, 2023 [27] | RCT, DB, PC phase 2 trial | NCT03987451 | 48 weeks | Semaglutide 2.4 mg once weekly vs. placebo | Improvement in liver fibrosis without worsening NASH | Liver fat content change (MRI-PDFF), NASH resolution, fibrosis stage change, adverse events | Biopsy-confirmed NASH-related cirrhosis, BMI ≥27 kg/m2 |
| Newsome, 2021 [29] | RCT, DB, PC | NCT02970942 | 72 weeks | Semaglutide (0.1 mg, 0.2 mg, 0.4 mg daily), placebo | Resolution of NASH without worsening of fibrosis | Changes in fibrosis stage, liver enzymes, metabolic parameters, safety | Patients with NASH, aged 18–75 years, fibrosis stage F1-F3, NAFLD score ≥4 |
| Sanyal, 2018 [31] | RCT, DB, PC, phase 2a | NCT02413372 | 16 weeks | Placebo, pegbelfermin 10 mg daily, 20 mg weekly | Safety, tolerability, hepatic fat fraction change | Pharmacokinetics, immunogenicity, exploratory endpoints | NASH patients |
| Harrison, 2019 [4] | DB, RCT, PC | NCT03987451 | 36 weeks | Resmetirom 80 mg, placebo | Percent relative change in hepatic fat fraction by MRI-PDFF at 12 weeks | Proportions of patients with ≥30% hepatic fat reduction at 12 and 36 weeks; absolute hepatic fat reduction at 12 and 36 weeks; changes in liver enzymes, fibrosis biomarkers, and lipids | Adults with biopsy-confirmed NASH; ≥18 years; ≥10% hepatic fat on screening MRI-PDFF |
| Harrison, 2023 [24] | RCT, DB, PC, phase 3 | NCT04197479 | 52 weeks | Resmetirom 100 mg OL, resmetirom 100 mg DB, resmetirom 80 mg DB, placebo DB | Safety and tolerability of resmetirom in patients with NAFLD (presumed NASH) | Proportion of patients achieving ≥30% reduction in liver fat content (MRI-PDFF); changes in liver volume, liver fat volume, VAT, SAT, body weight, waist circumference, BMI, liver enzymes, glucose metabolism, cardiovascular risk factors, and exploratory blood biomarkers | Adults ≥18 years with ≥3 metabolic risk factors; Patients with NAFLD (presumed NASH); Acceptable standard blood chemistry and hematology results; ≥8% hepatic fat (MRI-PDFF) |
| Harrison, 2024 [23] | RCT, DB, PC, phase 3 | NCT03900429 | 52 weeks | Resmetirom 80 mg, resmetirom 100 mg, placebo | ≥2 point reduction in NAFLD activity score without worsening fibrosis. Fibrosis improvement: ≥1 stage increase without worsening NAFLD activity score | Change in LDL cholesterol at week 24; changes in liver enzymes and noninvasive tests | Adults with biopsy-confirmed NASH and fibrosis stages F1B, F2, or F3; 966 patients |
| Study | Participants | Age (years) | Sex (Male) (%) | BMI (kg/m2) | ALT (U/L) | AST (U/L) | HbA1c (%) |
|---|---|---|---|---|---|---|---|
| Abdelmalek, 2024 [6] | 154 | 59.4(8.7) | 36.0 | 35.6(6.1) | 48.6(26.3) | 45.5(24.1) | 6.9(1.1) |
| Armstrong, 2016 [19] | 52 | 51.0(11.5) | 60.0 | 35.9(5.5) | 71.5(38.0) | 51.0(24.5) | 6.0(0.8) |
| Flint, 2021 [20] | 67 | 60.0(9.3) | 65.0 | 35.4(5.9) | 37.5(83.7) | 30.0(67.2) | 7.4(1.0) |
| Guo, 2020 [32] | 91 | 57.1(11.2) | 46.0 | 34.6(7.5) | 54.4(28.6) | 29.5(16.3) | 6.7(1.3) |
| Harrison, 2019 [4] | 125 | 50.2(11.5) | 51.0 | 35.1(6.1) | 52.6(30.8) | 37.2(18.6) | 6.3(1.1) |
| Harrison, 2021 [21] | 80 | 54.3(12.0) | 48.0 | 37.7(6.8) | 51.5(30.0) | 37.4(17.4) | 6.6(1.2) |
| Harrison, 2023 [24] | 1185 | 55.8(11.8) | 51.8 | 35.5(6.1) | 37.0(25.4) | 25.7(14.1) | 6.0(0.0) |
| Harrison, 2023 [26] | 30 | 51.1(11.6) | 41.0 | 38.4(8.1) | 58.6(29.2) | 40.3(18.4) | 6.3(1.0) |
| Harrison, 2023 [25] | 128 | 52.7(13.0) | 38.1 | 37.5(7.3) | 37.0(13.8) | 37.0(13.8) | 6.7(1.1) |
| Harrison, 2024 [23] | 966 | 56.7(11.0) | 55.8 | 35.7(6.8) | 54.6(32.0) | 40.4(23.0) | - |
| Kuchay, 2018 [30] | 42 | 52.3(6.9) | - | 29.7(3.5) | 56.8(30.3) | 44.9(23.9) | 9.0(1.1) |
| Loomba, 2023 [22] | 81 | 51.9(9.8) | 38.5 | 34.6(4.8) | 55.4(39.2) | 30.9(20.7) | 9.0(1.1) |
| Loomba, 2023 [28] | 71 | 59.2(8.2) | 30.0 | 35.0(5.9) | 44.5(58.2) | 44.4(45.8) | 7.2(1.3) |
| Loomba, 2023 [27] | 71 | 55.5(10.5) | 34.0 | 36.8(5.6) | 56.8(30.6) | 44.0(23.0) | 6.8(1.2) |
| Newsome, 2021 [29] | 320 | 55.0(10.5) | 58.0 | 35.8(6.4) | 54.0(86.0) | 43.0(79.0) | 7.3(1.2) |
| Sanyal, 2018 [31] | 75 | 50.3(11.6) | 35.8 | 35.4(5.6) | 42.5(22.4) | 53.5(33.4) | 6.1(1.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayesh, H.; Beran, A.; Suhail, S.; Ayesh, S.; Niswender, K. Comparative Analysis of Resmetirom vs. FGF21 Analogs vs. GLP-1 Agonists in MASLD and MASH: Network Meta-Analysis of Clinical Trials. Biomedicines 2024, 12, 2328. https://doi.org/10.3390/biomedicines12102328
Ayesh H, Beran A, Suhail S, Ayesh S, Niswender K. Comparative Analysis of Resmetirom vs. FGF21 Analogs vs. GLP-1 Agonists in MASLD and MASH: Network Meta-Analysis of Clinical Trials. Biomedicines. 2024; 12(10):2328. https://doi.org/10.3390/biomedicines12102328
Chicago/Turabian StyleAyesh, Hazem, Azizullah Beran, Sajida Suhail, Suhail Ayesh, and Kevin Niswender. 2024. "Comparative Analysis of Resmetirom vs. FGF21 Analogs vs. GLP-1 Agonists in MASLD and MASH: Network Meta-Analysis of Clinical Trials" Biomedicines 12, no. 10: 2328. https://doi.org/10.3390/biomedicines12102328
APA StyleAyesh, H., Beran, A., Suhail, S., Ayesh, S., & Niswender, K. (2024). Comparative Analysis of Resmetirom vs. FGF21 Analogs vs. GLP-1 Agonists in MASLD and MASH: Network Meta-Analysis of Clinical Trials. Biomedicines, 12(10), 2328. https://doi.org/10.3390/biomedicines12102328