

Exercise-Induced Proteomic Profile Changes in Patients with Advanced Heart Failure

 , , , ,
, , , , 
Abstract
1. Introduction
2. Material and Methods
2.1. Study Population and Design
2.1.1. Patients
2.1.2. Cardiopulmonary Exercise Test [9] (As Described Previously)
2.1.3. Blood Sampling and Storage
2.2. Laboratory Methods
2.2.1. Protein Digestion
2.2.2. Reversed-Phase Peptide Fractionation at High pH
2.2.3. Mass Spectrometry
3. Analytical Methods
3.1. Data Analysis
3.2. Protein Identification
3.3. Statistical Analysis
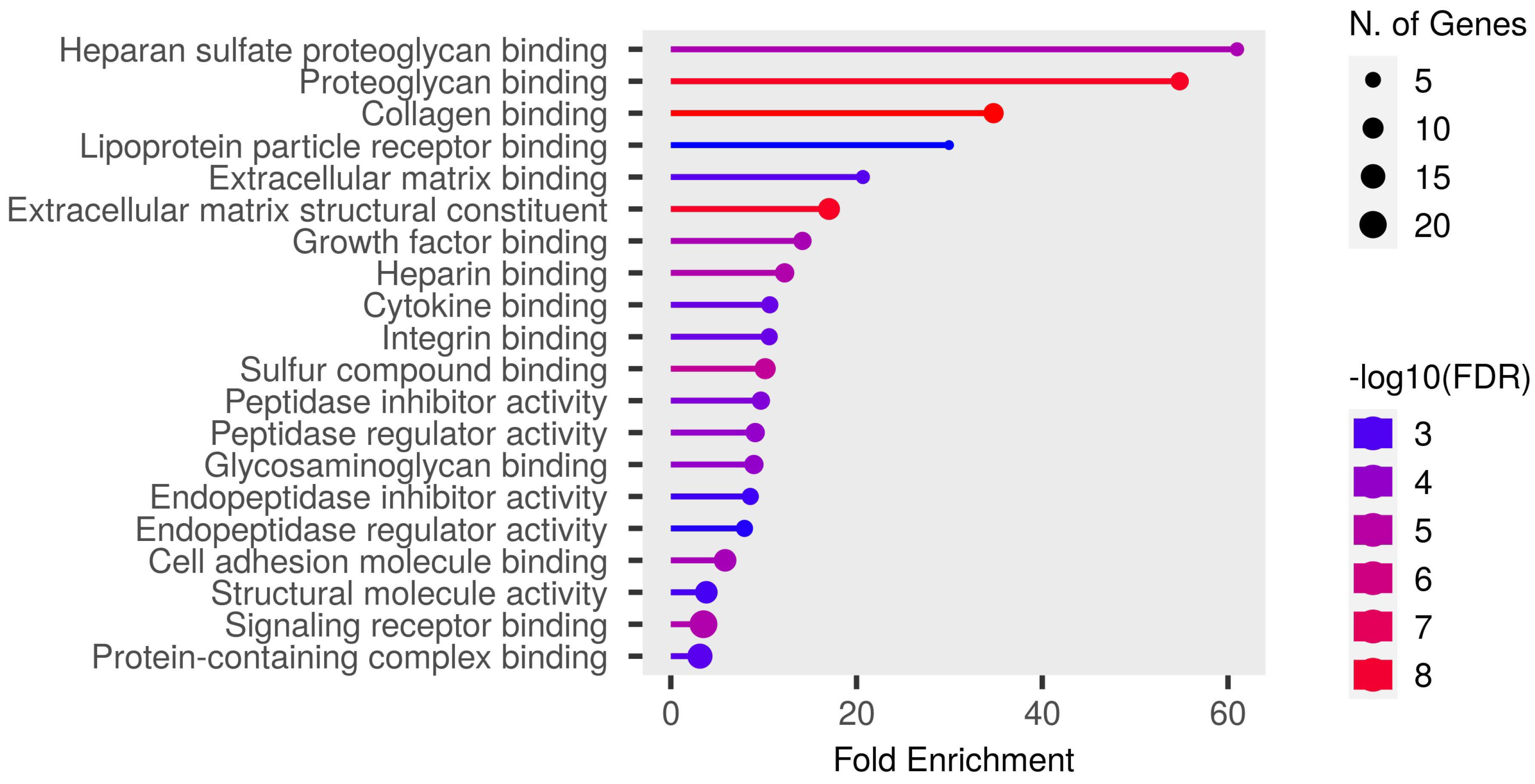
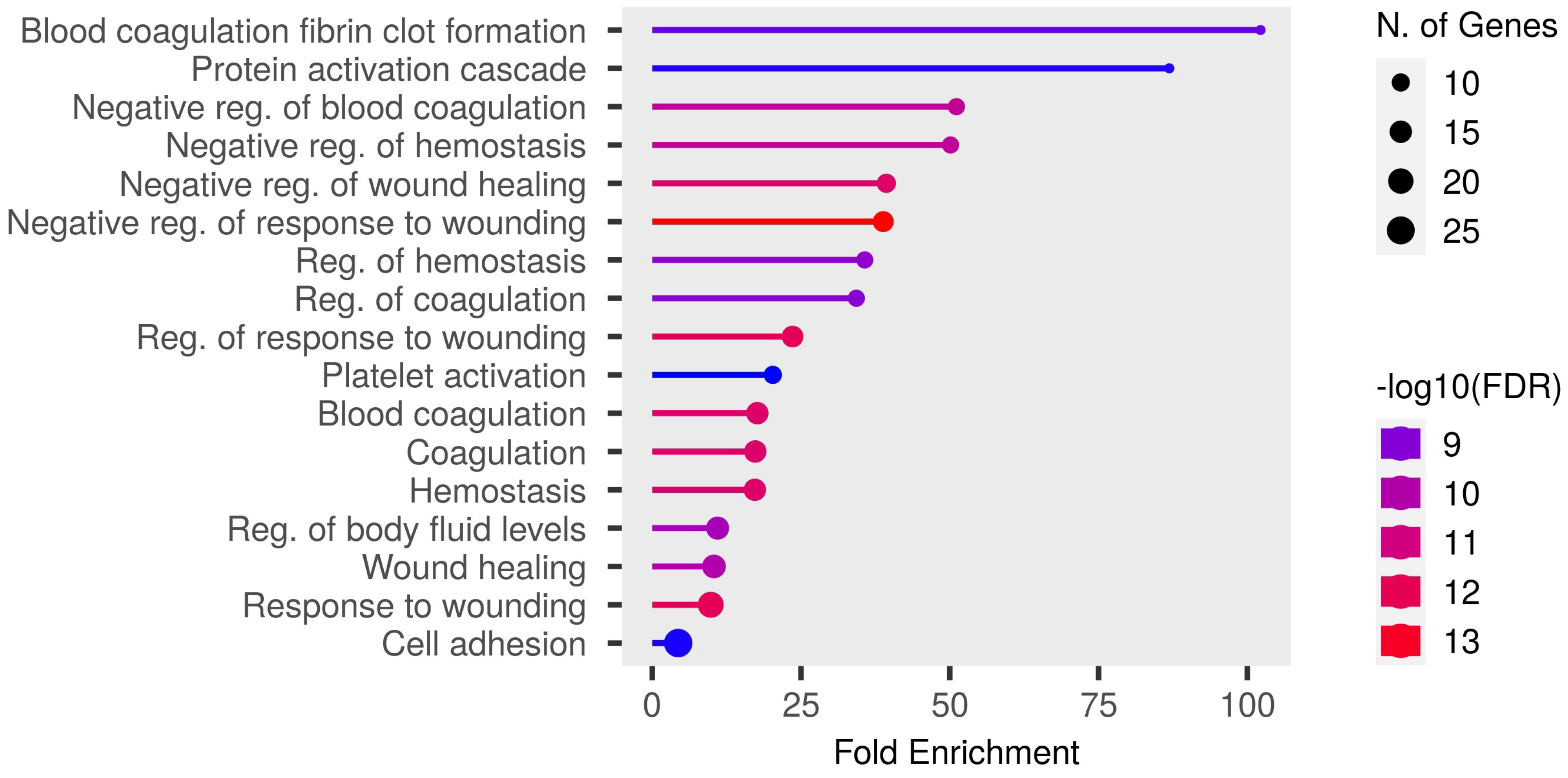
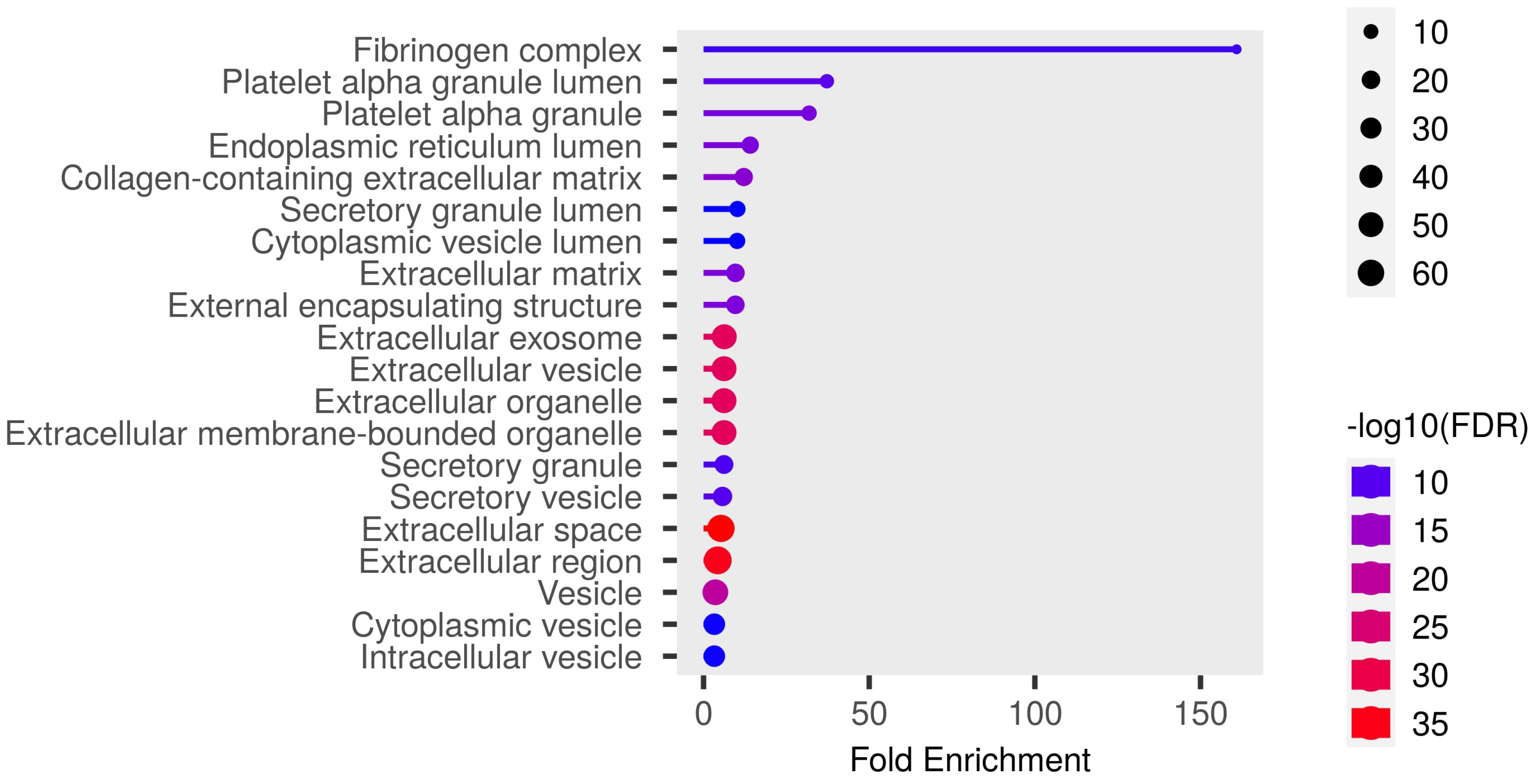
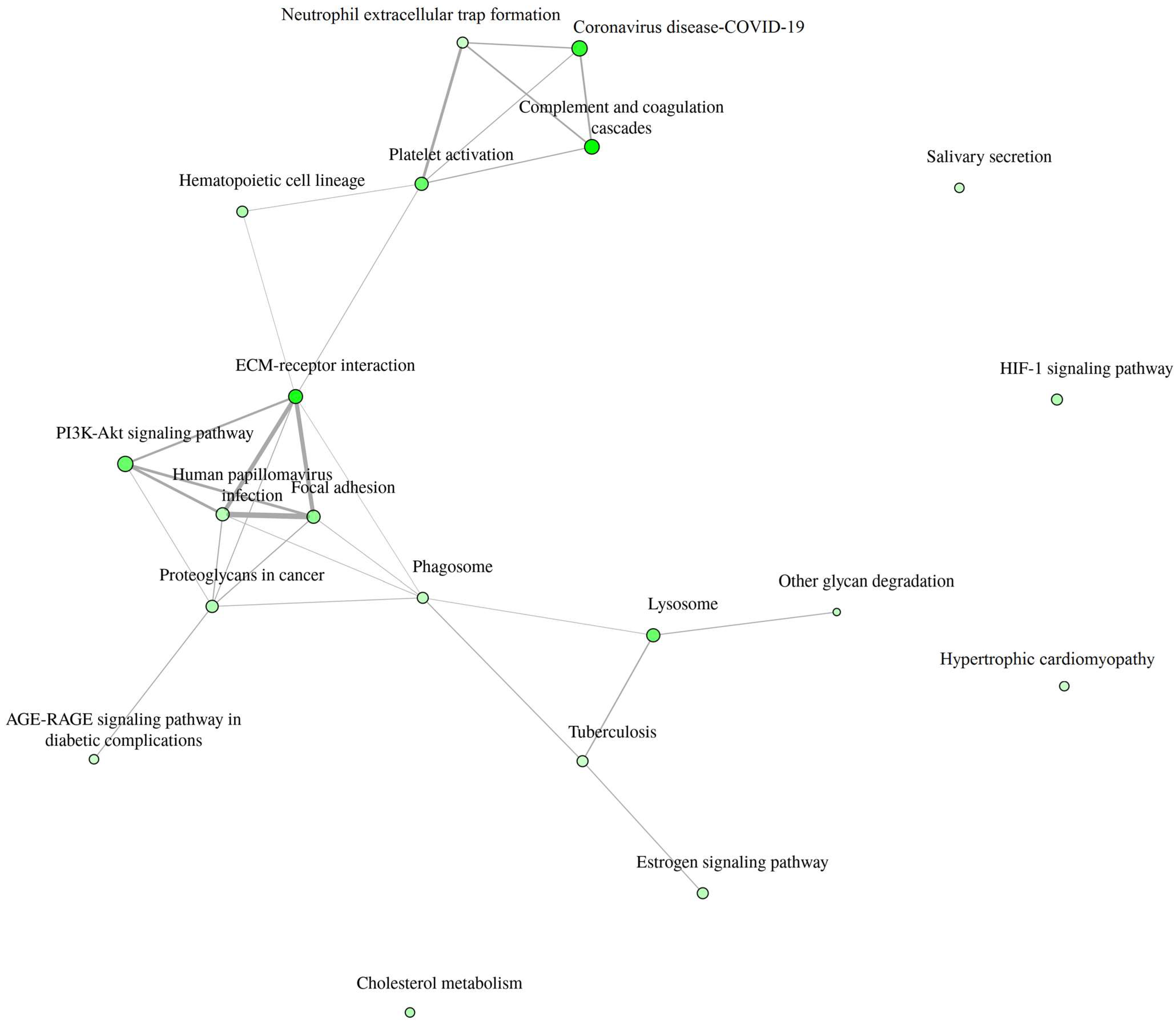
3.4. Gene Enrichment Analysis
4. Results
Enrichment Analysis
5. Discussion
5.1. Clinical Implications
5.2. Limitations of the Study
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Hear. Fail. 2022, 24, 4–131. [Google Scholar] [CrossRef] [PubMed]
- Phillips, S.A.; Vuckovic, K.; Cahalin, L.P.; Baynard, T. Defining the System: Contributors to Exercise Limitations in Heart Failure. Hear. Fail. Clin. 2015, 11, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Del Buono, M.G.; Arena, R.; Borlaug, B.A.; Carbone, S.; Canada, J.M.; Kirkman, D.L.; Garten, R.; Rodriguez-Miguelez, P.; Guazzi, M.; Lavie, C.J.; et al. Exercise Intolerance in Patients with Heart Failure: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 73, 2209–2225. [Google Scholar] [CrossRef] [PubMed]
- Safdar, A.; Saleem, A.; Tarnopolsky, M.A. The potential of endurance exercise-derived exosomes to treat metabolic diseases. Nat. Rev. Endocrinol. 2016, 12, 504–517. [Google Scholar] [CrossRef] [PubMed]
- Contrepois, K.; Wu, S.; Moneghetti, K.J.; Hornburg, D.; Ahadi, S.; Tsai, M.-S.; Metwally, A.A.; Wei, E.; Lee-McMullen, B.; Quijada, J.V.; et al. Molecular Choreography of Acute Exercise. Cell 2020, 181, 1112–1130. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mi, M.Y.; Barber, J.L.; Rao, P.; Farrell, L.A.; Sarzynski, M.A.; Bouchard, C.; Robbins, J.M.; Gerszten, R.E. Plasma Proteomic Kinetics in Response to Acute Exercise. Mol. Cell. Proteom. 2023, 22, 100601. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Guseh, J.S.; Churchill, T.W.; Yeri, A.; Lo, C.; Brown, M.; Houstis, N.E.; Aragam, K.G.; Lieberman, D.E.; Rosenzweig, A.; Baggish, A.L. An expanded repertoire of intensity-dependent exercise-responsive plasma proteins tied to loci of human disease risk. Sci. Rep. 2020, 10, 10831. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kurgan, N.; Noaman, N.; Pergande, M.R.; Cologna, S.M.; Coorssen, J.R.; Klentrou, P. Changes to the Human Serum Proteome in Response to High Intensity Interval Exercise: A Sequential Top-Down Proteomic Analysis. Front. Physiol. 2019, 10, 362. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Drohomirecka, A.; Waś, J.; Wiligórska, N.; Rywik, T.M.; Komuda, K.; Sokołowska, D.; Lutyńska, A.; Zieliński, T. L-arginine and Its Derivatives Correlate with Exercise Capacity in Patients with Advanced Heart Failure. Biomolecules 2023, 13, 423. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nynca, J.; Malinowska, A.; Świderska, B.; Wiśniewska, J.; Dobosz, S.; Ciereszko, A. Triploidization of rainbow trout affects proteins related to ovary development and reproductive activity. Aquaculture 2023, 565, 739145. [Google Scholar] [CrossRef]
- Tyanova, S.; Temu, T.; Cox, J. The MaxQuant computational platform for mass spectrometry-based shotgun proteomics. Nat. Protoc. 2016, 11, 2301. [Google Scholar] [CrossRef] [PubMed]
- Tyanova, S.; Temu, T.; Sinitcyn, P.; Carlson, A.; Hein, M.Y.; Geiger, T.; Mann, M.; Cox, J. The Perseus computational platform for comprehensive analysis of (prote)omics data. Nat. Methods 2016, 13, 731. [Google Scholar] [CrossRef] [PubMed]
- Ge, S.X.; Jung, D.; Yao, R. ShinyGO: A graphical gene-set enrichment tool for animals and plants. Bioinformatics 2020, 36, 2628–2629. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Womack, C.J.; Nagelkirk, P.R.; Coughlin, A.M. Exercise-Induced Changes in Coagulation and Fibrinolysis in Healthy Populations and Patients with Cardiovascular Disease. Sports Med. 2003, 33, 795–807. [Google Scholar] [CrossRef] [PubMed]
- Zegeye, M.M.; Lindkvist, M.; Fälker, K.; Kumawat, A.K.; Paramel, G.; Grenegård, M.; Sirsjö, A.; Ljungberg, L.U. Activation of the JAK/STAT3 and PI3K/AKT pathways are crucial for IL-6 trans-signaling-mediated pro-inflammatory response in human vascular endothelial cells. Cell Commun. Signal. 2018, 16, 55. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ouwerkerk, W.; Pereira, J.P.B.; Maasland, T.; Emmens, J.E.; Figarska, S.M.; Tromp, J.; Koekemoer, A.L.; Nelson, C.P.; Nath, M.; Romaine, S.P.; et al. Multiomics Analysis Provides Novel Pathways Related to Progression of Heart Failure. J. Am. Coll. Cardiol. 2023, 82, 1921–1931. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Liu, S.; Zhang, R.-Y.; Luo, H.; Chen, L.; He, W.-F.; Lei, R.; Liu, M.-R.; Hu, H.-X.; Chen, M. Association Between C1q/TNF-Related Protein-1 Levels in Human Plasma and Epicardial Adipose Tissues and Congestive Heart Failure. Cell. Physiol. Biochem. 2017, 42, 2130–2143. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.L.; Myers, J.; Bonikowske, A.R. Practical guidelines for exercise prescription in patients with chronic heart failure. Hear. Fail. Rev. 2023, 28, 1285–1296. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032, Erratum in Circulation 2022, 145, e1033. https://doi.org/10.1161/CIR.0000000000001073. Erratum in Circulation 2022, 146, e185. https://doi.org/10.1161/CIR.0000000000001097. Erratum in Circulation 2023, 147, e674. https://doi.org/10.1161/CIR.0000000000001142. [Google Scholar] [CrossRef] [PubMed]
- SalubrisBio. Salubris Biotherapeutics Presents Positive 6-Month Data from Phase 1b Clinical Trial of JK07 in Late-Breaking Session at The Heart Failure Society of America Annual Meeting 2023. Available online: https://www.salubrisbio.com/2023/10/10/salubris-biotherapeutics-presents-positive-6-month-data-from-phase-1b-clinical-trial-of-jk07-in-late-breaking-session-at-the-heart-failure-society-of-america-annual-meeting-2023/ (accessed on 22 September 2024).
- Fang, S.J.; Wu, X.S.; Han, Z.H.; Zhang, X.X.; Wang, C.M.; Li, X.Y.; Lu, L.Q.; Zhang, J.L. Neuregulin-1 preconditioning protects the heart against ischemia/reperfusion injury through a PI3K/Akt-dependent mechanism. Chin. Med. J. 2010, 123, 3597–3604. [Google Scholar] [PubMed]
- Drohomirecka, A.; Waś, J.; Sitkiewicz, E.; Świderska, B.; Lutyńska, A.; Rywik, T.; Zieliński, T. Exercise-induced proteomic profile changes in patients with advanced heart failure–A pilot study. In Proceedings of the Heart Failure Congress of the European Society of Cardiology, Lisbon, Portugal, 11–14 May 2024. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Population (n = 20) | |
|---|---|
| Clinical characteristics | |
| Age, years | 53.3 ± 8.3 |
| Gender, % male | 20 (100) |
| Ischemic etiology of HF | 10 (50) |
| Atrial fibrillation | 11 (55) |
| Hypertension | 7 (35) |
| Diabetes mellitus | 9 (45) |
| COPD | 2 (10) |
| ICD/CRT-D | 12 (60)/6 (30) |
| II NYHA class, patients (%) | 1 (5) |
| II/III NYHA class, patients (%) | 4 (20) |
| III NYHA class, patients (%) | 15 (75) |
| Echocardiographic parameters | |
| LVEF [%] | 22.2 ± 6.2 (range:12.5–35%) |
| LVEDD [mm] | 73.5 ± 9.6 |
| TAPSE [mm] | 18.4 ± 2.4 |
| Mitral regurgitation *, patients (%) | 15 (75) |
| Tricuspid regurgitation *, patients (%) | 10 (50) |
| Laboratory test results | |
| NT-pro-BNP [pg/mL], median (interquartile range) | 3187 (2011–4887) |
| eGFR, mL/min/1.73 m2 | 60.1 ± 14.1 |
| bilirubin [mmol/L] | 22.4 ± 11.7 |
| Medication | |
| Beta-blockers [n, %] | 20 (100.0) |
| ACEI/ARB/ARNI [n, %] | 20 (100.0) |
| Spironolactone/eplerenone [n, %] | 20 (100) |
| Loop diuretics [n, %] | 20 (100) |
| More than one diuretic administered (except from MRA) [n, %] | 10 (50) |
| Cardiopulmonary exercise test results | |
| pVO2 [mL/kg/min] | 10.5 ± 3.3 |
| pVO2 adjusted for sex and age adjusted pVO2 [%] | 34.5 ± 10.9 |
| RER at peak exhaustion | 1.1 ± 0.1 |
| VE/VCO2 slope | 45.2 ± 11.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drohomirecka, A.; Waś, J.; Sitkiewicz, E.; Świderska, B.; Lutyńska, A.; Rywik, T.; Zieliński, T. Exercise-Induced Proteomic Profile Changes in Patients with Advanced Heart Failure. Biomedicines 2024, 12, 2267. https://doi.org/10.3390/biomedicines12102267
Drohomirecka A, Waś J, Sitkiewicz E, Świderska B, Lutyńska A, Rywik T, Zieliński T. Exercise-Induced Proteomic Profile Changes in Patients with Advanced Heart Failure. Biomedicines. 2024; 12(10):2267. https://doi.org/10.3390/biomedicines12102267
Chicago/Turabian StyleDrohomirecka, Anna, Joanna Waś, Ewa Sitkiewicz, Bianka Świderska, Anna Lutyńska, Tomasz Rywik, and Tomasz Zieliński. 2024. "Exercise-Induced Proteomic Profile Changes in Patients with Advanced Heart Failure" Biomedicines 12, no. 10: 2267. https://doi.org/10.3390/biomedicines12102267
APA StyleDrohomirecka, A., Waś, J., Sitkiewicz, E., Świderska, B., Lutyńska, A., Rywik, T., & Zieliński, T. (2024). Exercise-Induced Proteomic Profile Changes in Patients with Advanced Heart Failure. Biomedicines, 12(10), 2267. https://doi.org/10.3390/biomedicines12102267