
Altered Expression of Intestinal Tight Junction Proteins in Heart Failure Patients with Reduced or Preserved Ejection Fraction: A Pathogenetic Mechanism of Intestinal Hyperpermeability

 ,
,  , , , ,
, , , ,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Endotoxin and Cytokines Measurements
2.3. Histopathological Evaluation and Immunohistochemistry
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Patients
3.2. Histopathological Evaluation
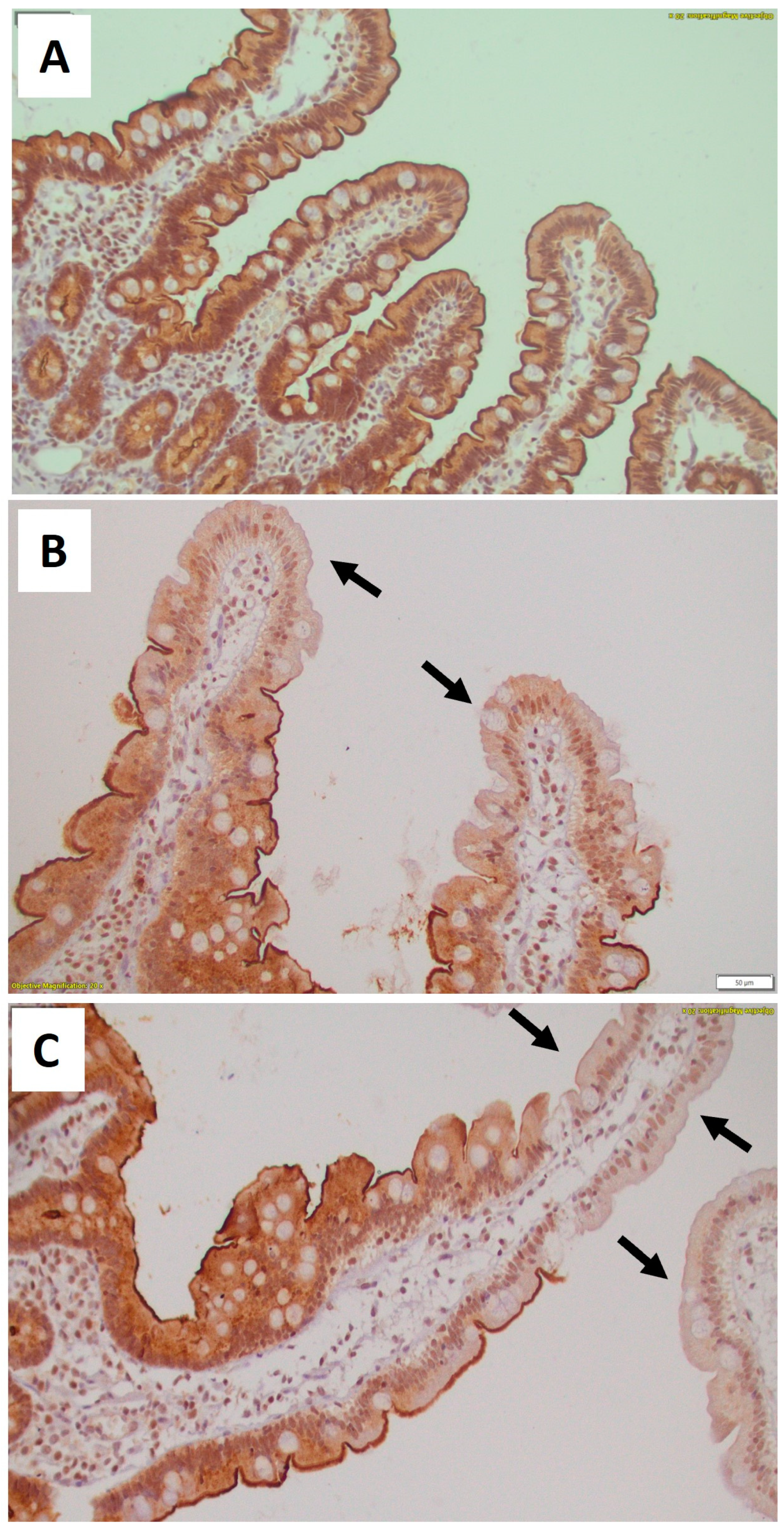
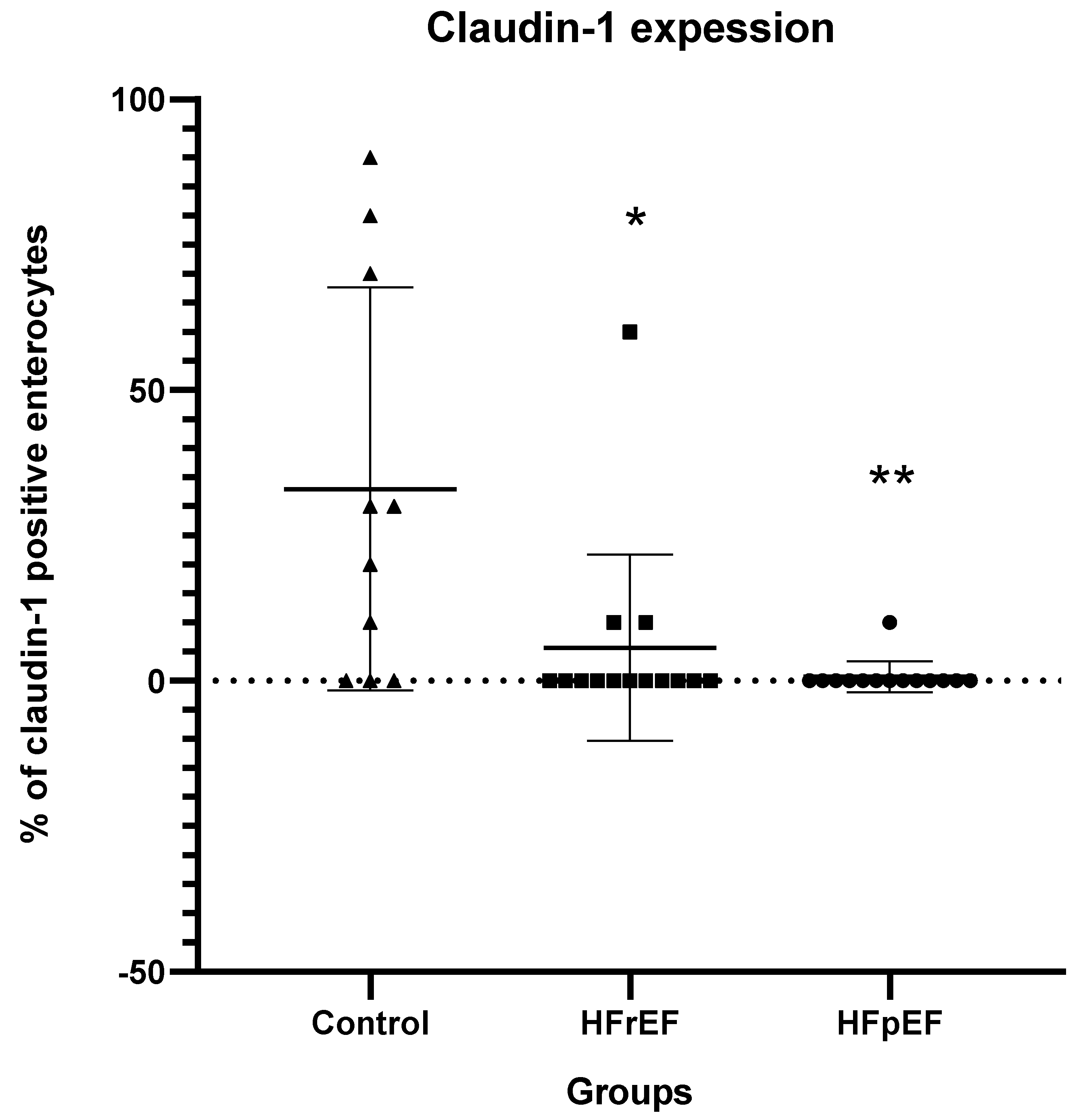
3.3. Immunohistochemical Results for TJ Proteins and Intraepithelial CD3+ T Cells
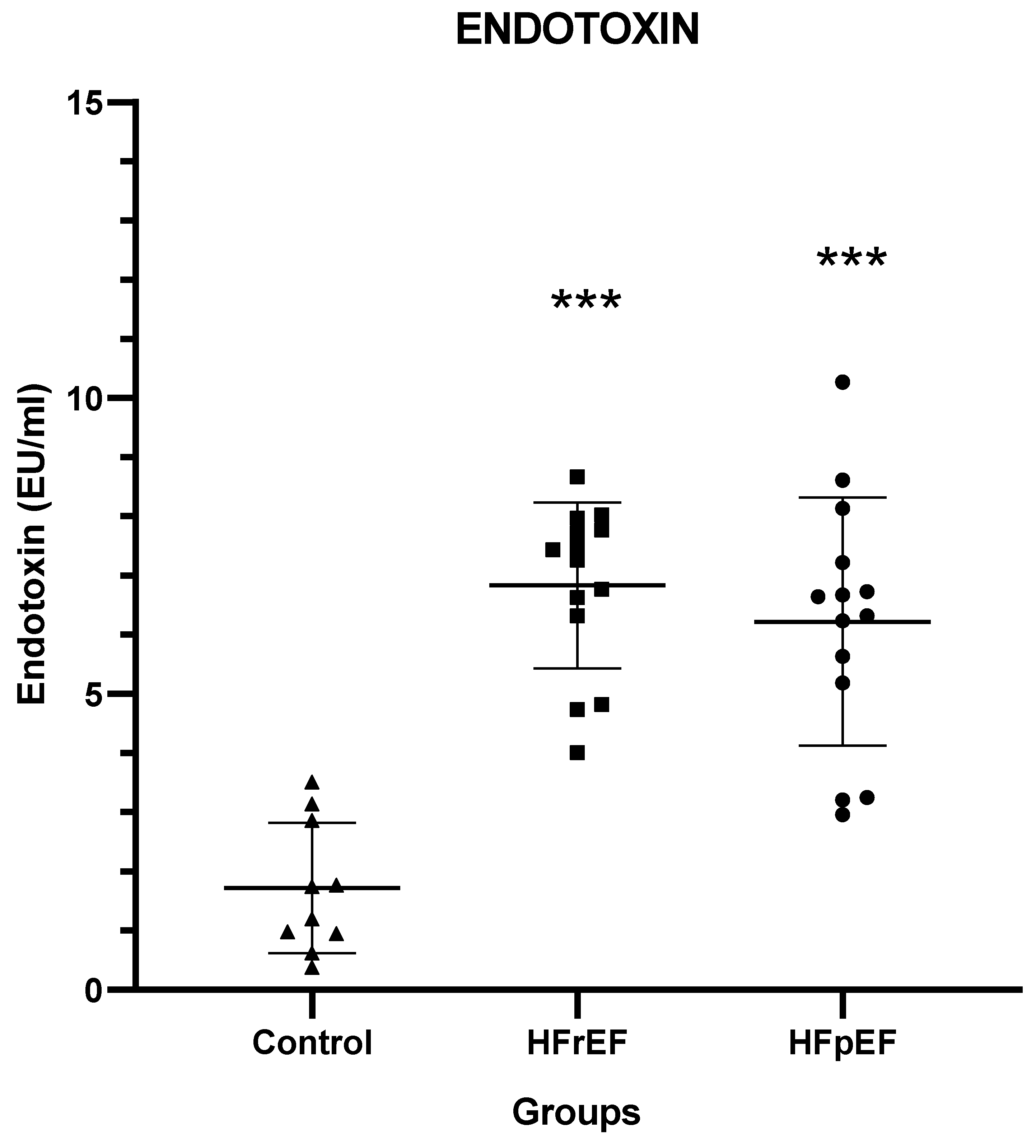
3.4. Endotoxin and Cytokine Levels
3.5. Correlations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cianci, R.; Franza, L.; Borriello, R.; Pagliari, D.; Gasbarrini, A.; Gambassi, G. The Role of Gut Microbiota in Heart Failure: When Friends Become Enemies. Biomedicines 2022, 10, 2712. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Mei, X.; Jiang, Y.; Chen, T.; Zhou, Y. Gut Microbiota in Heart Failure Patients with Preserved Ejection Fraction (GUMPTION Study). Front. Cardiovasc. Med. 2022, 8, 803744. [Google Scholar] [CrossRef] [PubMed]
- Branchereau, M.; Burcelin, R.; Heymes, C. The Gut Microbiome and Heart Failure: A Better Gut for a Better Heart. Rev. Endocr. Metab. Disord. 2019, 20, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Bu, J.; Wang, Z. Cross-Talk between Gut Microbiota and Heart via the Routes of Metabolite and Immunity. Gastroenterol. Res. Pract. 2018, 2018, 6458094. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.H.W.; Kitai, T.; Hazen, S.L. Gut Microbiota in Cardiovascular Health and Disease. Circ. Res. 2017, 120, 1183–1196. [Google Scholar] [CrossRef]
- Chen, X.; Li, H.Y.; Hu, X.M.; Zhang, Y.; Zhang, S.Y. Current Understanding of Gut Microbiota Alterations and Related Therapeutic Intervention Strategies in Heart Failure. Chin. Med. J. 2019, 132, 1843–1855. [Google Scholar] [CrossRef] [PubMed]
- Gomberg-Maitland, M.; Shah, S.J.; Guazzi, M. Inflammation in Heart Failure with Preserved Ejection Fraction Time to Put Out the Fire. JACC Heart Fail. 2016, 4, 325–328. [Google Scholar] [CrossRef]
- Balda, M.S.; Matter, K. Transmembrane Proteins of Tight Junctions. Semin. Cell Dev. Biol. 2000, 11, 281–289. [Google Scholar] [CrossRef]
- Schneeberger, E.E.; Lynch, R.D. The Tight Junction: A Multifunctional Complex. Am. J. Physiol. Cell Physiol. 2004, 286, 1213–1228. [Google Scholar] [CrossRef]
- Chiba, H.; Osanai, M.; Murata, M.; Kojima, T.; Sawada, N. Transmembrane Proteins of Tight Junctions. Biochim. Biophys. Acta Biomembr. 2008, 1778, 588–600. [Google Scholar] [CrossRef]
- Chelakkot, C.; Ghim, J.; Ryu, S.H. Mechanisms Regulating Intestinal Barrier Integrity and Its Pathological Implications. Exp. Mol. Med. 2018, 50, 1–9. [Google Scholar] [CrossRef]
- Madara, J.L. Warner-Lambert/Parke-Davis Award Lecture Pathobiology of the Intestinal Epithelial Barrier. Am. J. Pathol. 1990, 137, 1273–1281. [Google Scholar] [PubMed]
- Anderson, J.M.; Van Itallie, C.M. Tight Junctions and the Molecular Basis for Regulation of Paracellular Permeability. Am. J. Physiol. 1995, 269, G467–G475. [Google Scholar] [CrossRef]
- Fernandes, R.; Viana, S.D.; Nunes, S.; Reis, F. Diabetic Gut Microbiota Dysbiosis as an Inflammaging and Immunosenescence Condition That Fosters Progression of Retinopathy and Nephropathy. Biochim. Biophys. Acta Mol. Basis Dis. 2019, 1865, 1876–1897. [Google Scholar] [CrossRef] [PubMed]
- Almugadam, B.S.; Liu, Y.; Chen, S.M.; Wang, C.H.; Shao, C.Y.; Ren, B.W.; Tang, L. Alterations of Gut Microbiota in Type 2 Diabetes Individuals and the Confounding Effect of Antidiabetic Agents. J. Diabetes Res. 2020, 2020, 7253978. [Google Scholar] [CrossRef]
- Breton, J.; Galmiche, M.; Déchelotte, P. Dysbiotic Gut Bacteria in Obesity: An Overview of the Metabolic Mechanisms and Therapeutic Perspectives of Next-Generation Probiotics. Microorganisms 2022, 10, 452. [Google Scholar] [CrossRef]
- Fukui, H. Increased Intestinal Permeability and Decreased Barrier Function: Does It Really Influence the Risk of Inflammation? Inflamm. Intest. Dis. 2016, 1, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Trøseid, M.; Andersen, G.Ø.; Broch, K.; Hov, J.R. The Gut Microbiome in Coronary Artery Disease and Heart Failure: Current Knowledge and Future Directions. EBioMedicine 2020, 52, 102649. [Google Scholar] [CrossRef] [PubMed]
- Gallo, A.; Macerola, N.; Favuzzi, A.M.; Nicolazzi, M.A.; Gasbarrini, A.; Montalto, M. The Gut in Heart Failure: Current Knowledge and Novel Frontiers. Med. Princ. Pract. 2022, 31, 203–214. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, Y.; Ke, B.; Du, J. TMAO: How Gut Microbiota Contributes to Heart Failure. Transl. Res. 2021, 228, 109–125. [Google Scholar] [CrossRef]
- Madan, S.; Mehra, M.R. The Heart–Gut Microbiome Axis in Advanced Heart Failure. J. Heart Lung Transplant. 2020, 39, 891–893. [Google Scholar] [CrossRef]
- Jia, Q.; Li, H.; Zhou, H.; Zhang, X.; Zhang, A.; Xie, Y.; Li, Y.; Lv, S.; Zhang, J. Role and Effective Therapeutic Target of Gut Microbiota in Heart Failure. Cardiovasc. Ther. 2019, 2019, 5164298. [Google Scholar] [CrossRef]
- Sun, Y.J.; Chen, W.M.; Zhang, T.Z.; Cao, H.J.; Zhou, J. Effects of Cardiopulmonary Bypass on Tight Junction Protein Expressions in Intestinal Mucosa of Rats. World J. Gastroenterol. 2008, 14, 5868–5875. [Google Scholar] [CrossRef] [PubMed]
- Yuzefpolskaya, M.; Bohn, B.; Nasiri, M.; Zuver, A.M.; Onat, D.D.; Royzman, E.A.; Nwokocha, J.; Mabasa, M.; Pinsino, A.; Brunjes, D.; et al. Gut Microbiota, Endotoxemia, Inflammation, and Oxidative Stress in Patients with Heart Failure, Left Ventricular Assist Device, and Transplant. J. Heart Lung Transplant. 2020, 39, 880–890. [Google Scholar] [CrossRef]
- Wang, Z.; Cai, Z.; Ferrari, M.W.; Liu, Y.; Li, C.; Zhang, T.; Lyu, G. The Correlation between Gut Microbiota and Serum Metabolomic in Elderly Patients with Chronic Heart Failure. Mediators Inflamm. 2021, 2021, 5587428. [Google Scholar] [CrossRef] [PubMed]
- Rao, R.K.; Basuroy, S.; Rao, V.U.; Karnaky, K.J.; Gupta, A. Tyrosine Phosphorylation and Dissociation of Occludin-ZO-1 and E-Cadherin-β-Catenin Complexes from the Cytoskeleton by Oxidative Stress. Biochem. J. 2002, 368, 471–481. [Google Scholar] [CrossRef]
- Caldarelli, M.; Franza, L.; Rio, P.; Gasbarrini, A.; Gambassi, G.; Cianci, R. Gut–Kidney–Heart: A Novel Trilogy. Biomedicines 2023, 11, 3063. [Google Scholar] [CrossRef] [PubMed]
- Assimakopoulos, S.F.; Vagianos, C.E. Pathophysiology of Increased Intestinal Permeability in Obstructive Jaundice. World J. Gastroenterol. 2007, 13, 6458–6464. [Google Scholar] [CrossRef]
- Assimakopoulos, S.F.; Vagianos, C.E.; Nikolopoulou, V.N. Intestinal Barrier Dysfunction in Obstructive Jaundice: Current Concepts in Pathophysiology and Potential Therapies. Ann. Gastroenterol. 2007, 20, 116–123. [Google Scholar]
- Assimakopoulos, S.F.; Tsamandas, A.C.; Louvros, E.; Vagianos, C.E.; Nikolopoulou, V.N.; Thomopoulos, K.C.; Charonis, A.; Scopa, C.D. Intestinal Epithelial Cell Proliferation, Apoptosis and Expression of Tight Junction Proteins in Patients with Obstructive Jaundice. Eur. J. Clin. Invest. 2011, 41, 117–125. [Google Scholar] [CrossRef]
- Boicean, A.; Birlutiu, V.; Ichim, C.; Brusnic, O.; Onișor, D.M. Fecal Microbiota Transplantation in Liver Cirrhosis. Biomedicines 2023, 11, 2930. [Google Scholar] [CrossRef]
- Assimakopoulos, S.F. Enterocytes’ Tight Junctions: From Molecules to Diseases. World J. Gastrointest. Pathophysiol. 2011, 2, 123. [Google Scholar] [CrossRef] [PubMed]
- Kucharzik, T.; Walsh, S.V.; Chen, J.; Parkos, C.A.; Nusrat, A. Short Communication Neutrophil Transmigration in Inflammatory Bowel Disease Is Associated with Differential Expression of Epithelial Intercellular Junction Proteins. Am. J. Pathol. 2001, 159, 2001–2009. [Google Scholar] [CrossRef]
- Bhat, A.A.; Uppada, S.; Achkar, I.W.; Hashem, S.; Yadav, S.K.; Shanmugakonar, M.; Al-Naemi, H.A.; Haris, M.; Uddin, S. Tight Junction Proteins and Signaling Pathways in Cancer and Inflammation: A Functional Crosstalk. Front. Physiol. 2019, 10, 1942. [Google Scholar] [CrossRef] [PubMed]
- Manzanares, W.; Lemieux, M.; Langlois, P.L.; Wischmeyer, P.E. Probiotic and Synbiotic Therapy in Critical Illness: A Systematic Review and Meta-Analysis. Crit. Care 2016, 20, 262. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.C.; Lee, S.; McPhail, M.J.W.; Da Silva, K.; Guilly, S.; Zamalloa, A.; Witherden, E.; Støy, S.; Manakkat Vijay, G.K.; Pons, N.; et al. Rifaximin-α Reduces Gut-Derived Inflammation and Mucin Degradation in Cirrhosis and Encephalopathy: RIFSYS Randomised Controlled Trial. J. Hepatol. 2022, 76, 332–342. [Google Scholar] [CrossRef]
- Costanza, A.C.; Moscavitch, S.D.; Faria Neto, H.C.C.; Mesquita, E.T. Probiotic Therapy with Saccharomyces Boulardii for Heart Failure Patients: A Randomized, Double-Blind, Placebo-Controlled Pilot Trial. Int. J. Cardiol. 2015, 179, 348–350. [Google Scholar] [CrossRef]
- Awoyemi, A.; Mayerhofer, C.; Felix, A.S.; Hov, J.R.; Moscavitch, S.D.; Lappegård, K.T.; Hovland, A.; Halvorsen, S.; Halvorsen, B.; Gregersen, I.; et al. Rifaximin or Saccharomyces Boulardii in Heart Failure with Reduced Ejection Fraction: Results from the Randomized GutHeart Trial. EBioMedicine 2021, 70, 103511. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Controls (n = 10) | HFrEF (n = 14) | HFpEF (n = 14) | Statistics |
|---|---|---|---|---|
| Age | 45.9 ± 16.3 | 65.21 ± 9.67 * | 69.35 ± 10.42 ** | p = 0.001 |
| Gender | 5 M/5 F | 7 M/7 F | 6 M/8 F | p = 0.913 |
| Overweight (BMI 25–29.9) | 3/10 | 3/14 | 4/14 | p = 0.869 |
| Smoking | 2/10 | 3/14 | 2/14 | p = 0.878 |
| Hypertension | N/A | 5/14 | 5/14 | p = 1 |
| Hypercholesterolemia | N/A | 5/14 | 4/14 | p = 0.685 |
| Coronary artery disease | N/A | 5/14 | 4/14 | p = 0.685 |
| Histopathological Features | Controls (n = 10) | HFrEF (n = 14) | HFpEF (n = 14) | Statistics |
|---|---|---|---|---|
| Apoptotic body count | 0.1 (0.1–0.1) | 0.1 (0.1–0.3) | 0 (0–0.15) | p = 0.075 |
| Mitotic count | 0.5 (0.2–0.5) | 0.4 (0.25–0.60) | 0.4 (0.27–0.60) | p = 0.886 |
| Villus length (mm) | 0.39 ± 0.08 | 0.39 ± 0.09 | 0.40 ± 0.09 | p = 0.904 |
| Intraepithelial CD3+ lymphocytes/100 intestinal epithelial cells | 15 (10–20) | 15 (10–15) | 10 (10–20) | p = 0.410 |
| Occludin Expression | Controls (n = 10) | HFrEF (n = 14) | HFpEF (n = 14) | Statistics |
|---|---|---|---|---|
| Part of the villi | ||||
| Τip | 84 ± 9.66 | 48.57 ± 34.16 * | 40.71 ± 30.50 ** | p = 0.003 |
| Μiddle | 94 ± 6.99 | 82.14 ± 18.47 | 82.14 ± 8.02 ** | p = 0.011 |
| Crypt | 97 ± 4.83 | 91.43 ± 8.64 | 92.14 ± 6.99 | p = 0.142 |
| Total expression | 90 ± 6.67 | 75 ± 13.45 ** | 74.29 ± 11.58 ** | p = 0.002 |
| Cytokine | Controls (n = 10) | HFrEF (n = 14) | HFpEF (n = 14) | Statistics |
|---|---|---|---|---|
| IL-1β(pg/mL) | 0 (0–0.58) | 0 (0–0) | 0 (0–0) | p = 0.706 |
| IL-6 (pg/mL) | 0.57 (0.42–1.51) | 6.28 (4.21–11.02) * | 10.14 (9.33–24.44) ** | p < 0.001 |
| IL-8 (pg/mL) | 3.3 (2.40–6.94) | 24.25 (10.33–29.42) * | 23.7 (15.80–116.25) * | p = 0.008 |
| IL-10 (pg/mL) | 0.24 (0.16–0.40) | 1.28 (0.20–1.71) * | 1.83 (1.28–2.80) ** | p < 0.001 |
| IL-12 (pg/mL) | 0 (0–0) | 0 (0–0) | 0 (0–0) | p = 0.270 |
| TNF-a (pg/mL) | 0 (0–0.40) | 0 (0–0) | 0 (0–7.10) | p = 0.699 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koufou, E.-E.; Assimakopoulos, S.F.; Bosgana, P.; de Lastic, A.-L.; Grypari, I.-M.; Georgopoulou, G.-A.; Antonopoulou, S.; Mouzaki, A.; Kourea, H.P.; Thomopoulos, K.; et al. Altered Expression of Intestinal Tight Junction Proteins in Heart Failure Patients with Reduced or Preserved Ejection Fraction: A Pathogenetic Mechanism of Intestinal Hyperpermeability. Biomedicines 2024, 12, 160. https://doi.org/10.3390/biomedicines12010160
Koufou E-E, Assimakopoulos SF, Bosgana P, de Lastic A-L, Grypari I-M, Georgopoulou G-A, Antonopoulou S, Mouzaki A, Kourea HP, Thomopoulos K, et al. Altered Expression of Intestinal Tight Junction Proteins in Heart Failure Patients with Reduced or Preserved Ejection Fraction: A Pathogenetic Mechanism of Intestinal Hyperpermeability. Biomedicines. 2024; 12(1):160. https://doi.org/10.3390/biomedicines12010160
Chicago/Turabian StyleKoufou, Eleni-Evangelia, Stelios F. Assimakopoulos, Pinelopi Bosgana, Anne-Lise de Lastic, Ioanna-Maria Grypari, Georgia-Andriana Georgopoulou, Stefania Antonopoulou, Athanasia Mouzaki, Helen P. Kourea, Konstantinos Thomopoulos, and et al. 2024. "Altered Expression of Intestinal Tight Junction Proteins in Heart Failure Patients with Reduced or Preserved Ejection Fraction: A Pathogenetic Mechanism of Intestinal Hyperpermeability" Biomedicines 12, no. 1: 160. https://doi.org/10.3390/biomedicines12010160
APA StyleKoufou, E.-E., Assimakopoulos, S. F., Bosgana, P., de Lastic, A.-L., Grypari, I.-M., Georgopoulou, G.-A., Antonopoulou, S., Mouzaki, A., Kourea, H. P., Thomopoulos, K., & Davlouros, P. (2024). Altered Expression of Intestinal Tight Junction Proteins in Heart Failure Patients with Reduced or Preserved Ejection Fraction: A Pathogenetic Mechanism of Intestinal Hyperpermeability. Biomedicines, 12(1), 160. https://doi.org/10.3390/biomedicines12010160