
ES-SCLC Patients with PD-L1+ CTCs and High Percentages of CD8+PD-1+T Cells in Circulation Benefit from Front-Line Immunotherapy Treatment

 , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Blood Collection
2.2. Lymphocyte Isolation and Flow Cytometry Analysis
2.3. Isolation and Detection of CTCs
2.4. Statisical Analysis
3. Results
3.1. PD-1-Expressing CD8+ and CD4+ T-Cells in Peripheral Blood of SCLC Patients
3.2. PD-1 Expression Levels in SCLC Patients
3.3. PD-L1-Expressing CTCs and their Correlation with PD-1-Expressing T-Cells
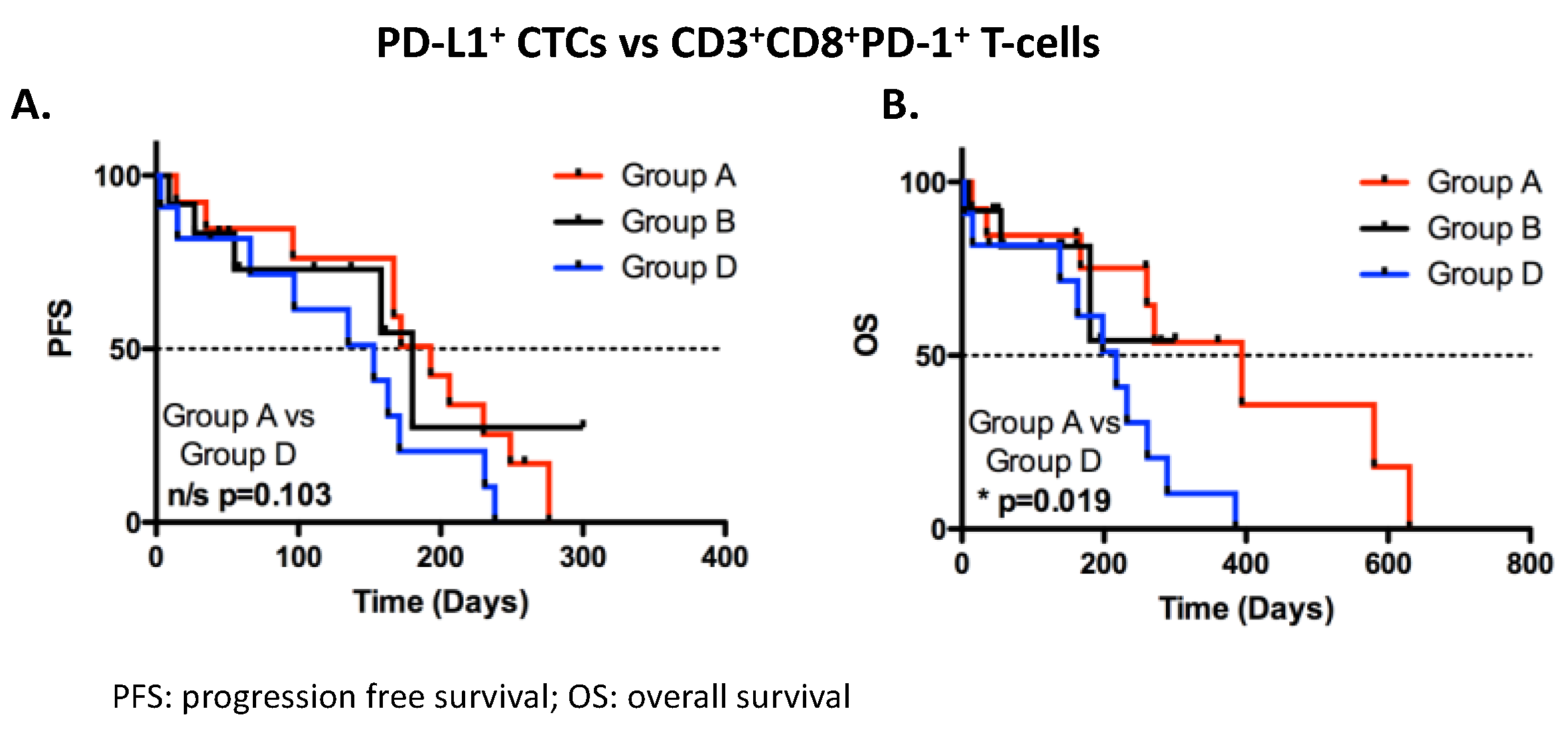
3.4. Correlation of Circulated T-Cells and CTCs with Clinical Outcome
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Liang, Y.; Yu, M.; Zhao, L.; Mei, Q.; Yu, Y.; Wang, N.; Zhang, D.; Wang, Z.; Jia, Y.; et al. Advances in immune checkpoint inhibitors therapy for small cell lung cancer. Cancer Med. 2023, 12, 11097–11106. [Google Scholar] [CrossRef]
- Peifer, M.; Fernández-Cuesta, L.; Sos, M.L.; George, J.; Seidel, D.; Kasper, L.H.; Plenker, D.; Leenders, F.; Sun, R.; Zander, T.; et al. Integrative genome analyses identify key somatic driver mutations of small-cell lung cancer. Nat. Genet. 2012, 44, 1104–1110. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, H.; Sen, T.; Rudin, C.M. Targeted Therapies and Biomarkers in Small Cell Lung Cancer. Front. Oncol. 2020, 10, 741. [Google Scholar] [CrossRef] [PubMed]
- Horn, L.; Mansfield, A.S.; Szczęsna, A.; Havel, L.; Krzakowski, M.; Hochmair, M.J.; Huemer, F.; Losonczy, G.; Johnson, M.L.; Nishio, M.; et al. First-Line Atezolizumab plus Chemotherapy in Extensive-Stage Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2220–2229. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Chen, Y.; Reinmuth, N.; Hotta, K.; Trukhin, D.; Statsenko, G.; Hochmair, M.; Özgüroğlu, M.; Ji, J.; Garassino, M.; et al. Durvalumab, with or without tremelimumab, plus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer: 3-year overall survival update from CASPIAN. ESMO Open 2022, 7, 100408. [Google Scholar] [CrossRef] [PubMed]
- Ding, X.-L.; Su, Y.-G.; Yu, L.; Bai, Z.-L.; Bai, X.-H.; Chen, X.-Z.; Yang, X.; Zhao, R.; He, J.-X.; Wang, Y.-Y. Clinical characteristics and patient outcomes of molecular subtypes of small cell lung cancer (SCLC). World J. Surg. Oncol. 2022, 20, 54. [Google Scholar] [CrossRef]
- Gay, C.M.; Stewart, C.A.; Park, E.M.; Diao, L.; Groves, S.M.; Heeke, S.; Nabet, B.Y.; Fujimoto, J.; Solis, L.M.; Lu, W.; et al. Patterns of transcription factor programs and immune pathway activation define four major subtypes of SCLC with distinct therapeutic vulnerabilities. Cancer Cell 2021, 39, 346–360.e347. [Google Scholar] [CrossRef]
- Chan, J.M.; Quintanal-Villalonga, Á.; Gao, V.R.; Xie, Y.; Allaj, V.; Chaudhary, O.; Masilionis, I.; Egger, J.; Chow, A.; Walle, T.; et al. Signatures of plasticity, metastasis, and immunosuppression in an atlas of human small cell lung cancer. Cancer Cell 2021, 39, 1479–1496. [Google Scholar] [CrossRef]
- Xie, M.; Chugh, P.; Broadhurst, H.; Lai, Z.; Whitston, D.; Paz-Ares, L.; Gay, C.; Byers, L.; Rudin, C.M.; Stewart, R.; et al. Abstract CT024: Durvalumab (D) + platinum-etoposide (EP) in 1L extensive-stage small-cell lung cancer (ES-SCLC): Exploratory analysis of SCLC molecular subtypes in CASPIAN. Cancer Res. 2022, 82 (Suppl. S12), CT024. [Google Scholar] [CrossRef]
- Yu, J.; Wang, X.; Teng, F.; Kong, L. PD-L1 expression in human cancers and its association with clinical outcomes. OncoTargets Ther. 2016, 9, 5023–5039. [Google Scholar] [CrossRef] [PubMed]
- Blackhall, F.; Frese, K.K.; Simpson, K.; Kilgour, E.; Brady, G.; Dive, C. Will liquid biopsies improve outcomes for patients with small-cell lung cancer? Lancet Oncol. 2018, 19, e470–e481. [Google Scholar] [CrossRef] [PubMed]
- Messaritakis, I.; Politaki, E.; Kotsakis, A.; Dermitzaki, E.-K.; Koinis, F.; Lagoudaki, E.; Koutsopoulos, A.; Kallergi, G.; Souglakos, J.; Georgoulias, V. Phenotypic characterization of circulating tumor cells in the peripheral blood of patients with small cell lung cancer. PLoS ONE 2017, 12, e0181211. [Google Scholar] [CrossRef] [PubMed]
- Roumeliotou, A.; Pantazaka, E.; Xagara, A.; Dimitrakopoulos, F.-I.; Koutras, A.; Christopoulou, A.; Kourelis, T.; Aljarba, N.H.; Alkahtani, S.; Koinis, F.; et al. Phenotypic Characterization of Circulating Tumor Cells Isolated from Non-Small and Small Cell Lung Cancer Patients. Cancers 2022, 15, 171. [Google Scholar] [CrossRef] [PubMed]
- Strati, A.; Koutsodontis, G.; Papaxoinis, G.; Angelidis, I.; Zavridou, M.; Economopoulou, P.; Kotsantis, I.; Avgeris, M.; Mazel, M.; Perisanidis, C.; et al. Prognostic significance of PD-L1 expression on circulating tumor cells in patients with head and neck squamous cell carcinoma. Ann. Oncol. 2017, 28, 1923–1933. [Google Scholar] [CrossRef] [PubMed]
- Dall’Olio, F.G.; Gelsomino, F.; Conci, N.; Marcolin, L.; De Giglio, A.; Grilli, G.; Sperandi, F.; Fontana, F.; Terracciano, M.; Fragomeno, B.; et al. PD-L1 Expression in Circulating Tumor Cells as a Promising Prognostic Biomarker in Advanced Non–small-cell Lung Cancer Treated with Immune Checkpoint Inhibitors. Clin. Lung Cancer 2021, 22, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Kotsakis, A.; Kallergi, G.; Aggouraki, D.; Lyristi, Z.; Koinis, F.; Lagoudaki, E.; Koutsopoulos, A.; Georgoulias, V.; Vetsika, E.K. CD8(+) PD-1(+) T-cells and PD-L1(+) circulating tumor cells in chemotherapy-naive non-small cell lung cancer: Towards their clinical relevance? Ther. Adv. Med. Oncol. 2019, 11, 1758835919853193. [Google Scholar] [CrossRef]
- Vardas, V.; Tolios, A.; Christopoulou, A.; Georgoulias, V.; Xagara, A.; Koinis, F.; Kotsakis, A.; Kallergi, G. Immune Checkpoint and EMT-Related Molecules in Circulating Tumor Cells (CTCs) from Triple Negative Breast Cancer Patients and Their Clinical Impact. Cancers 2023, 15, 1974. [Google Scholar] [CrossRef]
- Acheampong, E.; Abed, A.; Morici, M.; Spencer, I.; Beasley, A.B.; Bowyer, S.; Asante, D.-B.; Lomma, C.; Lin, W.; Millward, M.; et al. Evaluation of PD-L1 expression on circulating tumour cells in small-cell lung cancer. Transl. Lung Cancer Res. 2022, 11, 440–451. [Google Scholar] [CrossRef]
- Meng, S.; Tripathy, D.; Frenkel, E.P.; Shete, S.; Naftalis, E.Z.; Huth, J.F.; Beitsch, P.D.; Leitch, M.; Hoover, S.; Euhus, D.; et al. Circulating Tumor Cells in Patients with Breast Cancer Dormancy. Clin. Cancer Res. 2004, 10, 8152–8162. [Google Scholar] [CrossRef]
- Arrieta, O.; Montes-Servín, E.; Hernandez-Martinez, J.-M.; Cardona, A.F.; Casas-Ruiz, E.; Crispín, J.C.; Motola, D.; Flores-Estrada, D.; Barrera, L. Expression of PD-1/PD-L1 and PD-L2 in peripheral T-cells from non-small cell lung cancer patients. Oncotarget 2017, 8, 101994–102005. [Google Scholar] [CrossRef]
- Wherry, E.J. T cell exhaustion. Nat. Immunol. 2011, 12, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Kallergi, G.; Vetsika, E.-K.; Aggouraki, D.; Lagoudaki, E.; Koutsopoulos, A.; Koinis, F.; Katsarlinos, P.; Trypaki, M.; Messaritakis, I.; Stournaras, C.; et al. Evaluation of PD-L1/PD-1 on circulating tumor cells in patients with advanced non-small cell lung cancer. Ther. Adv. Med. Oncol. 2018, 10, 1758834017750121. [Google Scholar] [CrossRef] [PubMed]
- Katsarou, S.D.; Messaritakis, I.; Voumvouraki, A.; Kakavogiannis, S.; Κotsakis, A.; Alkahtani, S.; Stournaras, C.; Martin, S.S.; Georgoulias, V.; Kallergi, G. Detyrosinated α-Tubulin, Vimentin and PD-L1 in Circulating Tumor Cells (CTCs) Isolated from Non-Small Cell Lung Cancer (NSCLC) Patients. J. Pers. Med. 2022, 12, 154. [Google Scholar] [CrossRef] [PubMed]
- Longo, V.; Catino, A.; Montrone, M.; Pizzutilo, P.; Annese, T.; Pesola, F.; Ribatti, D.; Galetta, D. What Are the Biomarkers for Immunotherapy in SCLC? Int. J. Mol. Sci. 2021, 22, 11123. [Google Scholar] [CrossRef]
- Hou, W.; Zhou, X.; Yi, C.; Zhu, H. Immune Check Point Inhibitors and Immune-Related Adverse Events in Small Cell Lung Cancer. Front. Oncol. 2021, 11, 604227. [Google Scholar] [CrossRef]
- Caswell, D.R.; Swanton, C. The role of tumour heterogeneity and clonal cooperativity in metastasis, immune evasion and clinical outcome. BMC Med. 2017, 15, 133. [Google Scholar] [CrossRef]
- Krebs, M.G.; Hou, J.-M.; Sloane, R.; Lancashire, L.; Priest, L.; Nonaka, D.; Ward, T.H.; Backen, A.; Clack, G.; Hughes, A.; et al. Analysis of Circulating Tumor Cells in Patients with Non-small Cell Lung Cancer Using Epithelial Marker-Dependent and -Independent Approaches. J. Thorac. Oncol. 2012, 7, 306–315. [Google Scholar] [CrossRef]
- Rossi, E.; Aieta, M.; Tartarone, A.; Pezzuto, A.; Facchinetti, A.; Santini, D.; Ulivi, P.; Ludovini, V.; Possidente, L.; Fiduccia, P.; et al. A fully automated assay to detect the expression of pan-cytokeratins and of EML4-ALK fusion protein in circulating tumour cells (CTCs) predicts outcome of non-small cell lung cancer (NSCLC) patients. Transl. Lung Cancer Res. 2021, 10, 80–92. [Google Scholar] [CrossRef]
- Vardas, V.; Ju, J.A.; Christopoulou, A.; Xagara, A.; Georgoulias, V.; Kotsakis, A.; Alix-Panabières, C.; Martin, S.S.; Kallergi, G. Functional Analysis of Viable Circulating Tumor Cells from Triple-Negative Breast Cancer Patients Using TetherChip Technology. Cells 2023, 12, 1940. [Google Scholar] [CrossRef]
- Zhang, Z.; Liu, S.; Zhang, B.; Qiao, L.; Zhang, Y. T Cell Dysfunction and Exhaustion in Cancer. Front. Cell Dev. Biol. 2020, 8, 17. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Ahn, E.; Kissick, H.T.; Ahmed, R. Reinvigorating Exhausted T Cells by Blockade of the PD-1 Pathway. Forum Immunopathol. Dis. Ther. 2015, 6, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Gros, A.; Parkhurst, M.R.; Tran, E.; Pasetto, A.; Robbins, P.F.; Ilyas, S.; Prickett, T.D.; Gartner, J.J.; Crystal, J.S.; Roberts, I.M.; et al. Prospective identification of neoantigen-specific lymphocytes in the peripheral blood of melanoma patients. Nat. Med. 2016, 22, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Gros, A.; Tran, E.; Parkhurst, M.R.; Ilyas, S.; Pasetto, A.; Groh, E.M.; Robbins, P.F.; Yossef, R.; Garcia-Garijo, A.; Fajardo, C.A.; et al. Recognition of human gastrointestinal cancer neoantigens by circulating PD-1+ lymphocytes. J. Clin. Investig. 2019, 129, 4992–5004. [Google Scholar] [CrossRef]
- Kwon, M.; An, M.; Klempner, S.J.; Lee, H.; Kim, K.-M.; Sa, J.K.; Cho, H.J.; Hong, J.Y.; Lee, T.; Min, Y.W.; et al. Determinants of Response and Intrinsic Resistance to PD-1 Blockade in Microsatellite Instability–High Gastric Cancer. Cancer Discov. 2021, 11, 2168–2185. [Google Scholar] [CrossRef]
- MacFarlane, A.W.; Jillab, M.; Plimack, E.R.; Hudes, G.R.; Uzzo, R.G.; Litwin, S.; Dulaimi, E.; Al-Saleem, T.; Campbell, K.S. PD-1 Expression on Peripheral Blood Cells Increases with Stage in Renal Cell Carcinoma Patients and Is Rapidly Reduced after Surgical Tumor Resection. Cancer Immunol. Res. 2014, 2, 320–331. [Google Scholar] [CrossRef]
- Kamphorst, A.O.; Pillai, R.N.; Yang, S.; Nasti, T.H.; Akondy, R.S.; Wieland, A.; Sica, G.L.; Yu, K.; Koenig, L.; Patel, N.T.; et al. Proliferation of PD-1+ CD8 T cells in peripheral blood after PD-1–targeted therapy in lung cancer patients. Proc. Natl. Acad. Sci. USA 2017, 114, 4993–4998. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Sub-Categories | Values |
|---|---|---|
| Median age | 70 years (range 44–84 years) | |
| Gender | Male | 34 (79%) |
| Female | 9 (21%) | |
| Stage | Limited | 6 (14%) |
| Extensive | 37 (86%) | |
| Metastasis | Brain | 11 (25%) |
| Lung | 13 (30%) | |
| Liver | 15 (35%) | |
| Bones | 8 (17%) | |
| Adrenal gland | 6 (14%) | |
| LNs | 7 (16%) | |
| Pleural | 14 (33%) | |
| other | 4 (9%) | |
| Best Response | PR | 26 (60%) |
| SD | 1 (2%) | |
| Mixed | 2 (5%) | |
| Unknown | 14 (33%) | |
| Smoking Status | Never | 1 (2%) |
| Former | 10 (23%) | |
| Curent | 28 (65%) | |
| Unknown | 4 (9%) | |
| <40 pack year | 8 (19%) | |
| 40–80 pack year | 13 (31%) | |
| >80 pack year | 15 (36%) | |
| Unknown | 6 (14%) |
| PD-1+ CD3+CD8+ T-Cells | PD-1+ CD3+CD4+ T-Cells | ||||||
|---|---|---|---|---|---|---|---|
| CTCs | Total | Teff | Tem | Total | Teff | Tem | |
| CK+CD45- | Spewrman r | 0.351 | −0.94 | 0.011 | 0.010 | −0.137 | −0.188 |
| p-value | 0.038 | 0.611 | 0.952 | 0.957 | 0.485 | 0.336 | |
| 95% CI | 0.010 to 0.619 | −0.443 to 0.278 | −0.354 to 0.373 | −0.374 to 0.392 | −0.494 to 0.259 | −0.533 to 0.209 | |
| CK+CD45-PD-L1- | Spewrman r | −0.064 | −0.165 | −0.72 | −0.059 | −0.198 | −0.276 |
| p-value | 0.713 | 0.374 | 0.697 | 0.765 | 0.310 | 0.154 | |
| 95% CI | −0.398 to 0.284 | −0.499 to 0.211 | −0.425 to 0.299 | −0.433 to 0.330 | −0.540 to 0.199 | −0.596 to 0.119 | |
| CK+CD45-PD-L1+ | Spewrman r | 0.342 | −0.132 | −0.65 | 0.064 | −0.132 | −0.119 |
| p-value | 0.044 | 0.477 | 0.727 | 0.744 | 0.501 | 0.544 | |
| 95% CI | −0.000 to 0.612 | −0.473 to 0.243 | −0.419 to 0.306 | −0.326 to 0.436 | −0.490 to 0.264 | −0.480 to 0.276 | |
| Progresion Free Survival | Overall Survival | |||||||
|---|---|---|---|---|---|---|---|---|
| T-Cell Populations | ROC Cut Off | Median (Days) | 95% HR CI | p Value | Median (Days) | 95% CI | p Value | |
| CD3+CD8+ | 24 | High | 171 | 0.1988 to 1.283 | 0.150 | 271 | 0.1498 to 1.317 | 0.143 |
| Low | 153 | 198 | ||||||
| CD3+CD8+PD-1 | 22 | High | 172 | 0.1731 to 0.9486 | 0.037 | 394 | 0.1830 to 1.054 | 0.065 |
| Low | 153 | 217 | ||||||
| CD8+ Teff | 25 | High | 180 | 0.1402 to 0.8555 | 0.021 | 261 | 0.1826 to 1.273 | 0.140 |
| Low | 158 | 232 | ||||||
| CD8+ Teff PD-1 | 12.7 | High | 167 | 0.1562 to 1.450 | 0.191 | 289 | 0.03718 to 0.6173 | 0.008 |
| Low | 149 | 190 | ||||||
| CD8+ Tem | 33.6 | High | 164 | 0.8099 to 3.692 | 0.157 | 232 | 0.7701 to 5.062 | 0.156 |
| Low | 167 | 394 | ||||||
| CD8+ Tem PD-1 | 38 | High | 172 | 0.4013 to 2.091 | 0.835 | 394 | 0.2135 to 1.424 | 0.218 |
| Low | 164 | 260 | ||||||
| CD3+CD4+ | 41 | High | 158 | 0.4671 to 2.096 | 0.977 | 385 | 0.2410 to 1.380 | 0.216 |
| Low | 165 | 246 | ||||||
| CD3+CD4+PD-1 | 7.5 | High | 158 | 0.3293 to 1.667 | 0.468 | 289 | 0.2277 to 1.453 | 0.242 |
| Low | 164 | 232 | ||||||
| CD4+ Teff | 10.7 | High | 157 | 0.4969 to 3.160 | 0.632 | 261 | 0.2563 to 1.668 | 0.374 |
| Low | 164 | 232 | ||||||
| CD4+ Teff PD-1 | 18 | High | 163 | 0.6510 to 3.038 | 0.385 | 232 | 0.6423 to 3.869 | 0.320 |
| Low | 167 | 271 | ||||||
| CD4+ Tem | 33.2 | High | 167 | 0.2170 to 1.573 | 0.287 | 232 | 0.4638 to 3.653 | 0.616 |
| Low | 153 | 337 | ||||||
| CD4+ Tem PD-1 | 7.7 | High | 158 | 0.5744 to 2.720 | 0.573 | 232 | 0.5109 to 3.050 | 0.626 |
| Low | 186 | 265 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xagara, A.; Roumeliotou, A.; Kokkalis, A.; Tsapakidis, K.; Papakonstantinou, D.; Papadopoulos, V.; Samaras, I.; Chantzara, E.; Kallergi, G.; Kotsakis, A. ES-SCLC Patients with PD-L1+ CTCs and High Percentages of CD8+PD-1+T Cells in Circulation Benefit from Front-Line Immunotherapy Treatment. Biomedicines 2024, 12, 146. https://doi.org/10.3390/biomedicines12010146
Xagara A, Roumeliotou A, Kokkalis A, Tsapakidis K, Papakonstantinou D, Papadopoulos V, Samaras I, Chantzara E, Kallergi G, Kotsakis A. ES-SCLC Patients with PD-L1+ CTCs and High Percentages of CD8+PD-1+T Cells in Circulation Benefit from Front-Line Immunotherapy Treatment. Biomedicines. 2024; 12(1):146. https://doi.org/10.3390/biomedicines12010146
Chicago/Turabian StyleXagara, Anastasia, Argyro Roumeliotou, Alexandros Kokkalis, Konstantinos Tsapakidis, Dimitris Papakonstantinou, Vassilis Papadopoulos, Ioannis Samaras, Evagelia Chantzara, Galatea Kallergi, and Athanasios Kotsakis. 2024. "ES-SCLC Patients with PD-L1+ CTCs and High Percentages of CD8+PD-1+T Cells in Circulation Benefit from Front-Line Immunotherapy Treatment" Biomedicines 12, no. 1: 146. https://doi.org/10.3390/biomedicines12010146
APA StyleXagara, A., Roumeliotou, A., Kokkalis, A., Tsapakidis, K., Papakonstantinou, D., Papadopoulos, V., Samaras, I., Chantzara, E., Kallergi, G., & Kotsakis, A. (2024). ES-SCLC Patients with PD-L1+ CTCs and High Percentages of CD8+PD-1+T Cells in Circulation Benefit from Front-Line Immunotherapy Treatment. Biomedicines, 12(1), 146. https://doi.org/10.3390/biomedicines12010146