
Lymphocyte Subsets and Pulmonary Nodules to Predict the Progression of Sarcoidosis

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Enrollment
2.2. Follow-Up Testing and Modeling for Predicting the Course of Sarcoidosis
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Crouser, E.D.; Maier, L.A.; Wilson, K.C.; Bonham, C.A.; Morgenthau, A.S.; Patterson, K.C.; Abston, E.; Bernstein, R.C.; Blankstein, R.; Chen, E.S.; et al. Diagnosis and Detection of Sarcoidosis. An Official American Thoracic Society Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2020, 201, e26–e51. [Google Scholar] [CrossRef] [PubMed]
- Franzen, D.P.; Brutsche, M.; Nilsson, J.; Böni, C.; Daccord, C.; Distler, O.; Elsener, D.; Funke-Chambour, M.; Gruner, C.; Hayward-Könnecke, H.; et al. Sarcoidosis—A multisystem disease. Swiss. Med. Wkly. 2022, 152, w30049. [Google Scholar] [CrossRef] [PubMed]
- Culver, D.A.; Judson, M.A. New advances in the management of pulmonary sarcoidosis. BMJ 2019, 367, l5553. [Google Scholar] [CrossRef] [PubMed]
- Drent, M.; Crouser, E.D.; Grunewald, J. Challenges of Sarcoidosis and Its Management. N. Engl. J. Med. 2021, 385, 1018–1032. [Google Scholar] [CrossRef]
- McDonnell, M.J.; Saleem, M.I.; Wall, D.; Gilmartin, J.J.; Rutherford, R.M.; O’Regan, A. Predictive value of C-reactive protein and clinically relevant baseline variables in sarcoidosis. Sarcoidosis. Vasc. Diffuse. Lung Dis. 2016, 33, 331–340. [Google Scholar]
- Zhou, Y.; Zhang, Y.; Zhao, M.; Li, Q.; Li, H. sIL-2R levels predict the spontaneous remission in sarcoidosis. Respir. Med. 2020, 171, 106115. [Google Scholar] [CrossRef]
- Belhomme, N.; Jouneau, S.; Bouzillé, G.; Decaux, O.; Lederlin, M.; Guillot, S.; Perlat, A.; Jégo, P. Role of serum immunoglobulins for predicting sarcoidosis outcome: A cohort study. PLoS ONE 2018, 13, e0193122. [Google Scholar] [CrossRef]
- Bergantini, L.; Bianchi, F.; Cameli, P.; Mazzei, M.A.; Fui, A.; Sestini, P.; Rottoli, P.; Bargagli, E. Prognostic Biomarkers of Sarcoidosis: A Comparative Study of Serum Chitotriosidase, ACE, Lysozyme, and KL-6. Dis. Markers. 2019, 2019, 8565423. [Google Scholar] [CrossRef]
- Ishiyama, M.; Soine, L.A.; Vesselle, H.J. Semi-quantitative metabolic values on FDG PET/CT including extracardiac sites of disease as a predictor of treatment course in patients with cardiac sarcoidosis. EJNMMI Res. 2017, 7, 67. [Google Scholar] [CrossRef]
- Benamore, R.; Kendrick, Y.R.; Repapi, E.; Helm, E.; Cole, S.L.; Taylor, S.; Ho, L.P. CTAS: A CT score to quantify disease activity in pulmonary sarcoidosis. Thorax 2016, 71, 1161–1163. [Google Scholar] [CrossRef]
- Kraaijvanger, R.; Janssen Bonás, M.; Vorselaars, A.D.M.; Veltkamp, M. Biomarkers in the Diagnosis and Prognosis of Sarcoidosis: Current Use and Future Prospects. Front. Immunol. 2020, 11, 1443. [Google Scholar] [CrossRef] [PubMed]
- Grunewald, J.; Grutters, J.C.; Arkema, E.V.; Saketkoo, L.A.; Moller, D.R.; Müller-Quernheim, J. Publisher Correction: Sarcoidosis. Nat. Rev. Dis. Primers. 2019, 5, 49. [Google Scholar] [CrossRef] [PubMed]
- Kobak, S. Catch the rainbow: Prognostic factor of sarcoidosis. Lung India 2020, 37, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Judson, M.A. The ability to predict the clinical course of pulmonary sarcoidosis from data that is right in front of us. J. Bras. Pneumol. 2022, 48, e20220012. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Zou, L.; Wang, S.; Zeng, T.; Li, P.; Shen, Y.; Chen, L. Performance of Serum Angiotensin-Converting Enzyme in Diagnosing Sarcoidosis and Predicting the Active Status of Sarcoidosis: A Meta-Analysis. Biomolecules 2022, 12, 1400. [Google Scholar] [CrossRef]
- Malkova, A.; Zinchenko, Y.; Starshinova, A.; Kudlay, D.; Kudryavtsev, I.; Glushkova, A.; Yablonskiy, P.; Shoenfeld, Y. Sarcoidosis: Progression to the chronic stage and pathogenic based treatment (narrative review). Front. Med. 2022, 9, 963435. [Google Scholar] [CrossRef]
- Zhang, H.; Costabel, U.; Dai, H. The Role of Diverse Immune Cells in Sarcoidosis. Front. Immunol. 2021, 12, 788502. [Google Scholar] [CrossRef]
- Loke, W.S.J.; Herbert, C.; Thomas, P.S. Sarcoidosis: Immunopathogenesis and Immunological Markers. Int. J. Chronic. Dis. 2013, 2013, 928601. [Google Scholar] [CrossRef]
- Manika, K.; Domvri, K.; Kyriazis, G.; Kontakiotis, T.; Papakosta, D. BALF and blood NK- cells in different stages of pulmonary sarcoidosis. Sarcoidosis. Vasc. Diffuse. Lung Dis. 2021, 38, e2021039. [Google Scholar] [CrossRef]
- Aleksonienė, R.; Zeleckienė, I.; Matačiūnas, M.; Puronaitė, R.; Jurgauskienė, L.; Malickaitė, R.; Strumilienė, E.; Gruslys, V.; Zablockis, R.; Danila, E. Relationship between radiologic patterns, pulmonary function values and bronchoalveolar lavage fluid cells in newly diagnosed sarcoidosis. J. Thorac. Dis. 2017, 9, 88–95. [Google Scholar] [CrossRef]
- Aleksonienė, R.; Besusparis, J.; Gruslys, V.; Jurgauskienė, L.; Laurinavičienė, A.; Laurinavičius, A.; Malickaitė, R.; Norkūnienė, J.; Zablockis, R.; Žurauskas, E.; et al. CD31+, CD38+, CD44+, and CD103+ lymphocytes in peripheral blood, bronchoalveolar lavage fluid and lung biopsy tissue in sarcoid patients and controls. J. Thorac. Dis. 2021, 13, 2300–2318. [Google Scholar] [CrossRef] [PubMed]
- Costabel, U.; Hunninghake, G.W. ATS/ERS/WASOG statement on sarcoidosis. Sarcoidosis Statement Committee. American Thoracic Society. European Respiratory Society. World Association for Sarcoidosis and Other Granulomatous Disorders. Eur. Respir. J. 1999, 14, 735–737. [Google Scholar] [CrossRef] [PubMed]
- Erdal, B.S.; Crouser, E.D.; Yildiz, V.; King, M.A.; Patterson, A.T.; Knopp, M.V.; Clymer, B.D. Quantitative computerized two-point correlation analysis of lung CT scans correlates with pulmonary function in pulmonary sarcoidosis. Chest 2012, 142, 1589–1597. [Google Scholar] [CrossRef] [PubMed]
- Simmering, J.; Stapleton, E.M.; Polgreen, P.M.; Kuntz, J.; Gerke, A.K. Patterns of medication use and imaging following initial diagnosis of sarcoidosis. Respir. Med. 2021, 189, 106622. [Google Scholar] [CrossRef] [PubMed]
- Akram, M.J.; Khalid, U.; Abu Bakar, M.; Butt, F.M.; Ashraf, M.B. Sarcoidosis: Epidemiology, characteristics, and outcomes over 10 years—A single-center study in Pakistan. Expert. Rev. Respir. Med. 2022, 16, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Casal, A.; Suárez-Antelo, J.; Soto-Feijóo, R.; Ferreiro, L.; Rodríguez-Núñez, N.; Lama, A.; Riveiro, V.; Toubes, M.E.; Lourido, T.; Ricoy, J.; et al. Sarcoidosis. Disease progression based on radiological and functional course: Predictive factors. Heart Lung 2022, 56, 62–69. [Google Scholar] [CrossRef]
- Schimmelpennink, M.C.; Meek, D.B.; Vorselaars, A.D.M.; Langezaal, L.C.M.; van Moorsel, C.H.M.; van der Vis, J.J.; Veltkamp, M.; Grutters, J.C. Characterization of the PF-ILD phenotype in patients with advanced pulmonary sarcoidosis. Respir. Res. 2022, 23, 169. [Google Scholar] [CrossRef]
- Bonham, C.A.; Strek, M.E.; Patterson, K.C. From granuloma to fibrosis: Sarcoidosis associated pulmonary fibrosis. Curr. Opin. Pulm. Med. 2016, 22, 484–491. [Google Scholar] [CrossRef]
- Schenkel, A.R.; Chew, T.W.; Chlipala, E.; Harbord, M.W.N.; Muller, W.A. Different susceptibilities of PECAM-deficient mouse strains to spontaneous idiopathic pneumonitis. Exp. Mol. Pathol. 2006, 81, 23–30. [Google Scholar] [CrossRef]
- Marelli-Berg, F.M.; Clement, M.; Mauro, C.; Caligiuri, G. An immunologist’s guide to CD31 function in T-cells. J. Cell Sci. 2013, 126, 2343–2352. [Google Scholar] [CrossRef]
- Lishnevsky, M.; Young, L.C.; Woods, S.J.; Groshong, S.D.; Basaraba, R.J.; Gilchrist, J.M.; Higgins, D.M.; Gonzalez-Juarrero, M.; Bass, T.A.; Muller, W.A.; et al. Microhemorrhage is an early event in the pulmonary fibrotic disease of PECAM-1 deficient FVB/n mice. Exp. Mol. Pathol. 2014, 97, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Guedes, A.G.; Jude, J.A.; Paulin, J.; Rivero-Nava, L.; Kita, H.; Lund, F.E.; Kannan, M.S. Airway responsiveness in CD38-deficient mice in allergic airway disease: Studies with bone marrow chimeras. Am. J. Physiol. Lung Cell Mol. Physiol. 2015, 308, L485–L493. [Google Scholar] [CrossRef] [PubMed]
- Newman, D.K.; Fu, G.; McOlash, L.; Schauder, D.; Newman, P.J.; Cui, W.; Rao, S.; Johnson, B.D.; Gershan, J.A.; Riese, M.J. PECAM-1 (CD31) expression in naïve and memory, but not acutely activated, CD8+ T cells. J. Leukoc. Biol. 2018, 104, 883–893. [Google Scholar] [CrossRef]
- Kudryavtsev, I.; Serebriakova, M.; Starshinova, A.; Zinchenko, Y.; Basantsova, N.; Malkova, A.; Soprun, L.; Churilov, L.P.; Toubi, E.; Yablonskiy, P.; et al. Imbalance in B cell and T Follicular Helper Cell Subsets in Pulmonary Sarcoidosis. Sci. Rep. 2020, 10, 1059. [Google Scholar] [CrossRef] [PubMed]
- Ziora, D.; Jastrzębski, D.; Adamek, M.; Czuba, Z.; Kozielski, J.J.; Grzanka, A.; Kasperska-Zajac, A. Circulating concentration of markers of angiogenic activity in patients with sarcoidosis and idiopathic pulmonary fibrosis. BMC Pulm. Med. 2015, 15, 113. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, Y.; Van Seventer, G.A.; Siraganian, R.; Wahl, L.; Shaw, S. Dual role of the CD44 molecule in T cell adhesion and activation. J. Immunol. 1989, 143, 2457–2463. [Google Scholar] [CrossRef]
- Goodison, S.; Urquidi, V.; Tarin, D. CD44 cell adhesion molecules. Mol. Pathol. 1999, 52, 189–196. [Google Scholar] [CrossRef]
- Rivera, N.V.; Hagemann-Jensen, M.; Ferreira, M.A.R.; Kullberg, S.; Eklund, A.; Martin, N.G.; Padyukov, L.; Grunewald, J. Common variants of T-cells contribute differently to phenotypic variation in sarcoidosis. Sci. Rep. 2017, 7, 5623. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, X.; Long, M.; Yuan, M.; Yin, J.; Luo, W.; Wang, S.; Cai, Y.; Jiang, W.; Chao, J. Macrophage-derived GPNMB trapped by fibrotic extracellular matrix promotes pulmonary fibrosis. Commun. Biol. 2023, 6, 136. [Google Scholar] [CrossRef]
- Culty, M.; O’Mara, T.E.; Underhill, C.B.; Yeager, H., Jr.; Swartz, R.P. Hyaluronan receptor (CD44) expression and function in human peripheral blood monocytes and alveolar macrophages. J. Leukoc. Biol. 1994, 56, 605–611. [Google Scholar] [CrossRef]
- d’Alessandro, M.; Carleo, A.; Cameli, P.; Bergantini, L.; Perrone, A.; Vietri, L.; Lanzarone, N.; Vagaggini, C.; Sestini, P.; Bargagli, E. BAL biomarkers’ panel for differential diagnosis of interstitial lung diseases. Clin. Exp. Med. 2020, 20, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Sung, S.S.; Fu, S.M.; Rose, C.E., Jr.; Gaskin, F.; Ju, S.T.; Beaty, S.R. A major lung CD103 (alphaE)-beta7 integrin-positive epithelial dendritic cell population expressing Langerin and tight junction proteins. J. Immunol. 2006, 176, 2161–2172. [Google Scholar] [CrossRef] [PubMed]
- Beauchamp, N.M.; Yammani, R.D.; Alexander-Miller, M.A. CD8 marks a subpopulation of lung-derived dendritic cells with differential responsiveness to viral infection and toll-like receptor stimulation. J. Virol. 2012, 86, 10640–10650. [Google Scholar] [CrossRef]
- Laidlaw, B.J.; Zhang, N.; Marshall, H.D.; Staron, M.M.; Guan, T.; Hu, Y.; Cauley, L.S.; Craft, J.; Kaech, S.M. CD4+ T cell help guides formation of CD103+ lung-resident memory CD8+ T cells during influenza viral infection. Immunity 2014, 41, 633–645. [Google Scholar] [CrossRef] [PubMed]
- Bernatchez, E.; Gold, M.J.; Langlois, A.; Lemay, A.M.; Brassard, J.; Flamand, N.; Marsolais, D.; McNagny, K.M.; Blanchet, M.R. Pulmonary CD103 expression regulates airway inflammation in asthma. Am. J. Physiol. Lung Cell Mol. Physiol. 2015, 308, L816–L826. [Google Scholar] [CrossRef]
- McMaster, S.R.; Wein, A.N.; Dunbar, P.R.; Hayward, S.L.; Cartwright, E.K.; Denning, T.L.; Kohlmeier, J.E. Pulmonary antigen encounter regulates the establishment of tissue-resident CD8 memory T cells in the lung airways and parenchyma. Mucosal. Immunol. 2018, 11, 1071–1078. [Google Scholar] [CrossRef]
- Wu, H.; Liao, W.; Li, Q.; Long, H.; Yin, H.; Zhao, M.; Chan, V.; Lau, C.S.; Lu, Q. Pathogenic role of tissue-resident memory T cells in autoimmune diseases. Autoimmun. Rev. 2018, 17, 906–911. [Google Scholar] [CrossRef]
- d’Alessandro, M.; Gangi, S.; Cavallaro, D.; Bergantini, L.; Mezzasalma, F.; Cattelan, S.; Baglioni, S.; Abbritti, M.; Cameli, P.; Bargagli, E. CD103 Expression on Regulatory and Follicular T Cells in Lymph Nodes, Bronchoalveolar Lavage Fluid and Peripheral Blood of Sarcoidosis Patients. Life 2022, 12, 762. [Google Scholar] [CrossRef]
- Helmers, R.A.; Dayton, C.S.; Floerchinger, C.; Hunninghake, G.W. Bronchoalveolar lavage in interstitial lung disease: Effect of volume of fluid infused. J. Appl. Physiol 1989, 67, 1443–1446. [Google Scholar] [CrossRef]
- Nishimura, K.; Itoh, H.; Kitaichi, M.; Nagai, S.; Izumi, T. Pulmonary sarcoidosis: Correlation of CT and histopathologic findings. Radiology 1994, 189, 105–109. [Google Scholar] [CrossRef]
- Criado, E.; Sánchez, M.; Ramírez, J.; Arguis, P.; de Caralt, T.M.; Perea, R.J.; Xaubet, A. Pulmonary sarcoidosis: Typical and atypical manifestations at high-resolution CT with pathologic correlation. Radiographics 2010, 30, 1567–1586. [Google Scholar] [CrossRef] [PubMed]
- Keijsers, R.G.; van den Heuvel, D.A.; Grutters, J.C. Imaging the inflammatory activity of sarcoidosis. Eur. Respir. J. 2013, 41, 743–751. [Google Scholar] [CrossRef] [PubMed]
- Distefano, G.; Vancheri, A.; Palermo, M.; Tiralongo, F.; Foti, P.V.; Mauro, L.A.; Vancheri, C.; Basile, A.; Palmucci, S. Morphological Patterns of Sarcoidosis and Clinical Outcome: Retrospective Analysis through a Multidisciplinary Approach. Diagnostics 2020, 10, 212. [Google Scholar] [CrossRef] [PubMed]
- Polverosi, R.; Russo, R.; Coran, A.; Battista, A.; Agostini, C.; Pomerri, F.; Giraudo, C. Typical and atypical pattern of pulmonary sarcoidosis at high-resolution CT: Relation to clinical evolution and therapeutic procedures. Radiol. Med. 2014, 119, 384–392. [Google Scholar] [CrossRef]
- Duan, J.; Xu, Y.; Zhu, H.; Zhang, H.; Sun, S.; Sun, H.; Wang, W.; Xie, S. Relationship between CT activity score with lung function and the serum angiotensin converting enzyme in pulmonary sarcoidosis on chest HRCT. Medicine 2018, 97, e12205. [Google Scholar] [CrossRef]
- Silva, A.L.; Melo, N.; Caetano Mota, P.; Lima, B.; Pereira, J.M.; Cunha, R.; Guimarães, S.; Souto-Moura, C.; Morais, A. Pulmonary Sarcoidosis: Prognostic Factors at Diagnosis in Patients from North of Portugal. Reumatol. Clin. 2020, 16, 468–472. [Google Scholar] [CrossRef]
- Kirkil, G.; Lower, E.E.; Baughman, R.P. Predictors of Mortality in Pulmonary Sarcoidosis. Chest 2018, 153, 105–113. [Google Scholar] [CrossRef]
- Danila, E.; Jurgauskiene, L.; Malickaite, R. BAL fluid cells and pulmonary function in different radiographic stages of newly diagnosed sarcoidosis. Adv. Med. Sci. 2008, 53, 228–233. [Google Scholar] [CrossRef]
- Danila, E.; Zurauskas, E.; Loskutoviene, G.; Zablockis, R.; Nargela, R.; Birzietyte, V.; Valentinaviciene, G. Significance of bronchoscopic lung biopsy in clinical practice. Adv. Med. Sci. 2008, 53, 11–16. [Google Scholar] [CrossRef]
- Danila, E.; Zurauskas, E. Diagnostic value of epithelioid cell granulomas in bronchoscopic biopsies. Intern. Med. 2008, 47, 2121–2126. [Google Scholar] [CrossRef]
- Danila, E.; Jurgauskiene, L.; Norkuniene, J.; Malickaite, R. BAL fluid cells in newly diagnosed pulmonary sarcoidosis with different clinical activity. Ups. J. Med. Sci. 2009, 114, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Danila, E.; Norkūniene, J.; Jurgauskiene, L.; Malickaite, R. Diagnostic role of BAL fluid CD4/CD8 ratio in different radiographic and clinical forms of pulmonary sarcoidosis. Clin. Respir. J. 2009, 3, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Pocienė, I.; Gauronskaitė, R.; Galkauskas, D.; Mainelis, A.; Gruslys, V.; Danila, E. Age as a Risk Factor in the Occurrence of Complications during or after Bronchoscopic Lung Biopsy. Geriatrics 2022, 7, 34. [Google Scholar] [CrossRef] [PubMed]
- Ozyilmaz, E.; Ozturk, O.G.; Durmaz, A.; Othman Hasan, O.; Guzelbaba, B.; Seydaoglu, G.; Kuleci, S.; Hanta, I.; Erken, E.; Kocabas, A. Early prediction of sarcoidosis prognosis with HLA typing: A 5 year follow-up study. Sarcoidosis. Vasc. Diffuse. Lung Dis. 2018, 35, 184–191. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Demographics | Sarcoidosis Patients (n = 71) |
|---|---|
| Sex (male/female) | 38/33 |
| Age (years) | 37 (21–68) |
| Löfgren syndrome (yes/no) | 27/44 |
| Smoker (yes/never) | 25/46 |
| FVC, % pred | 104 ± 15 |
| FEV1, % pred | 97 ± 13 |
| FEV1/FVC, % | 79 ± 6 |
| TLC, % pred | 99 ± 12 |
| VC, % pred | 106 ± 14 |
| RV, % pred | 90 ± 21 |
| DLCO, % pred | 76 ± 11 |
| BALF total cells count, ×106/mL | 375 ± 192 |
| BALF macrophages, % | 60.8 ± 19.2 |
| BALF lymphocytes, % | 38.4 ± 19.2 |
| BALF neutrophils, % | 0.5 ± 0.8 |
| BALF eosinophils, % | 0.2 ± 0.3 |
| BALF CD4, % | 69.9 ± 17.7 |
| BALF CD8, % | 18.8 ± 13.3 |
| BALF CD4+/CD8+ | 6.1 ± 4.8 |
| Cells | Blood (n = 71) | BALF (n = 71) |
|---|---|---|
| CD4+, % | 41.1 ± 8.5 | 69.9 ± 17.7 |
| CD8+, % | 27.1 ± 9.0 | 18.8 ± 13.3 |
| CD4+/CD8+ | 1.7 ± 0.7 | 6.1 ± 4.8 |
| CD31+CD4+, % | 12.5 ± 6.5 | 5.9 ± 4.5 |
| CD38+CD4+, % | 23.4 ± 9.1 | 24.0 ± 14.1 |
| CD44+CD4+, % | 45.6 ± 9.9 | 75.7 ± 13.4 |
| CD103+CD4+, % | 2.3 ± 6.9 | 8.7 ± 8.2 |
| CD31+CD8+, % | 19.1 ± 7.7 | 10.1 ± 8.5 |
| CD38+CD8+, % | 20.3 ± 7.4 | 5.9 ± 6.5 |
| CD44+CD8+, % | 38.8 ± 11.1 | 20.9 ± 12.5 |
| CD103+CD8+, % | 3.7 ± 4.7 | 13.3 ± 11.3 |
| Cells | Sarcoidosis (n = 35) |
|---|---|
| CD4+, total | 7375 ± 8391 |
| CD8+, total | 3873 ± 7067 |
| CD38+, total | 2803.4 ± 5167 |
| CD44+, total | 10,322 ± 8094 |
| CD103+, total | 1532 ± 1589 |
| CD4+, % | 19.1 ± 11.7 |
| CD8+, % | 8.1 ± 6.3 |
| CD38+, % | 6.0 ± 6.2 |
| CD44+, % | 27.2 ± 10.3 |
| CD103+, % | 4.3 ± 3.0 |
| CD4+ density, mm2 | 705 ± 519 |
| CD8+ density, mm2 | 315 ± 269 |
| CD38+ density, mm2 | 235 ± 266 |
| CD44+ density, mm2 | 1002 ± 502 |
| CD103+ density, mm2 | 158 ± 118 |
| Collagen, % | 20.2 ± 7.4 |
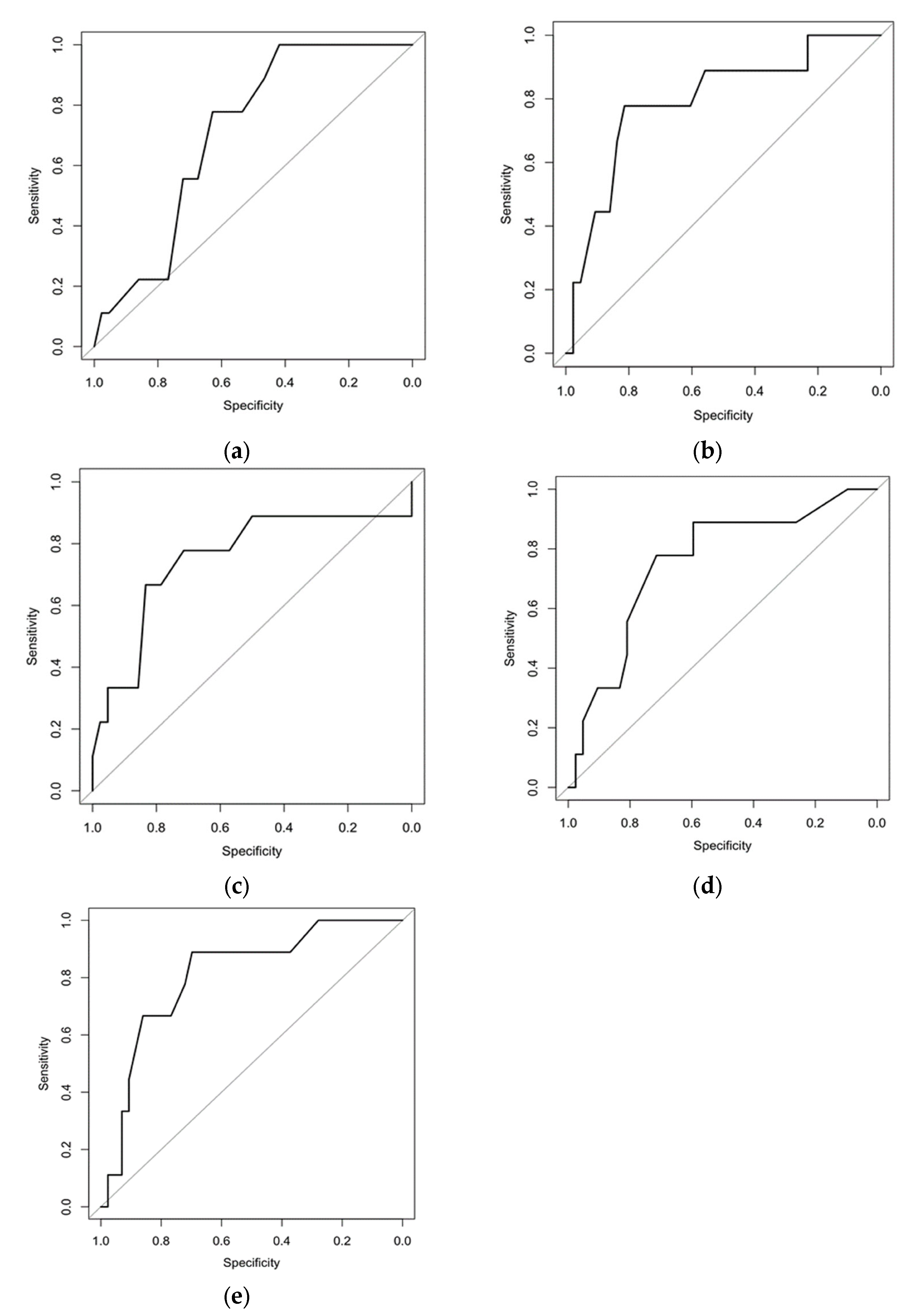
| Criteria | Cut-Off | Sp | Sn | AUC | AUC (CI 95%) | OR | CI 95% | p Value |
|---|---|---|---|---|---|---|---|---|
| CD4+CD31+ blood, % | ≤14.5 | 0.419 | 1.000 | 0.708 | 0.555; 0.861 | 13.78 | 0.75; 252.06 | 0.020 |
| CD4+CD44+ blood, % | ≤37.5 | 0.814 | 0.778 | 0.795 | 0.622; 0.968 | 15.31 | 2.66; 88.04 | <0.001 |
| CD8+CD31+ BALF, % | ≥13.5 | 0.833 | 0.667 | 0.751 | 0.536; 0.967 | 10.00 | 2.01; 49.83 | 0.010 |
| CD8+CD103+ BALF, % | ≥15.5 | 0.714 | 0.778 | 0.754 | 0.574; 0.933 | 8.75 | 1.59; 48.29 | 0.010 |
| Number of lung nodules | ≥15.0 | 0.698 | 0.889 | 0.810 | 0.658; 0.962 | 18.46 | 2.09; 163.05 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Danila, E.; Aleksonienė, R.; Besusparis, J.; Gruslys, V.; Jurgauskienė, L.; Laurinavičienė, A.; Laurinavičius, A.; Mainelis, A.; Zablockis, R.; Zeleckienė, I.; et al. Lymphocyte Subsets and Pulmonary Nodules to Predict the Progression of Sarcoidosis. Biomedicines 2023, 11, 1437. https://doi.org/10.3390/biomedicines11051437
Danila E, Aleksonienė R, Besusparis J, Gruslys V, Jurgauskienė L, Laurinavičienė A, Laurinavičius A, Mainelis A, Zablockis R, Zeleckienė I, et al. Lymphocyte Subsets and Pulmonary Nodules to Predict the Progression of Sarcoidosis. Biomedicines. 2023; 11(5):1437. https://doi.org/10.3390/biomedicines11051437
Chicago/Turabian StyleDanila, Edvardas, Regina Aleksonienė, Justinas Besusparis, Vygantas Gruslys, Laimutė Jurgauskienė, Aida Laurinavičienė, Arvydas Laurinavičius, Antanas Mainelis, Rolandas Zablockis, Ingrida Zeleckienė, and et al. 2023. "Lymphocyte Subsets and Pulmonary Nodules to Predict the Progression of Sarcoidosis" Biomedicines 11, no. 5: 1437. https://doi.org/10.3390/biomedicines11051437
APA StyleDanila, E., Aleksonienė, R., Besusparis, J., Gruslys, V., Jurgauskienė, L., Laurinavičienė, A., Laurinavičius, A., Mainelis, A., Zablockis, R., Zeleckienė, I., Žurauskas, E., & Malickaitė, R. (2023). Lymphocyte Subsets and Pulmonary Nodules to Predict the Progression of Sarcoidosis. Biomedicines, 11(5), 1437. https://doi.org/10.3390/biomedicines11051437