
Genetic Susceptibility of HLA Alleles to Non-Steroidal Anti-Inflammatory Drug Hypersensitivity in the Taiwanese Population

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. HLA Allele Typing
2.3. HLA Imputation for Genotype Data
2.4. Participants
2.5. Covariates
2.6. Statistical Analysis
3. Results
3.1. Characteristics of Participants
3.2. Allele Frequencies and Association between HLA Alleles and NSAID Allergy
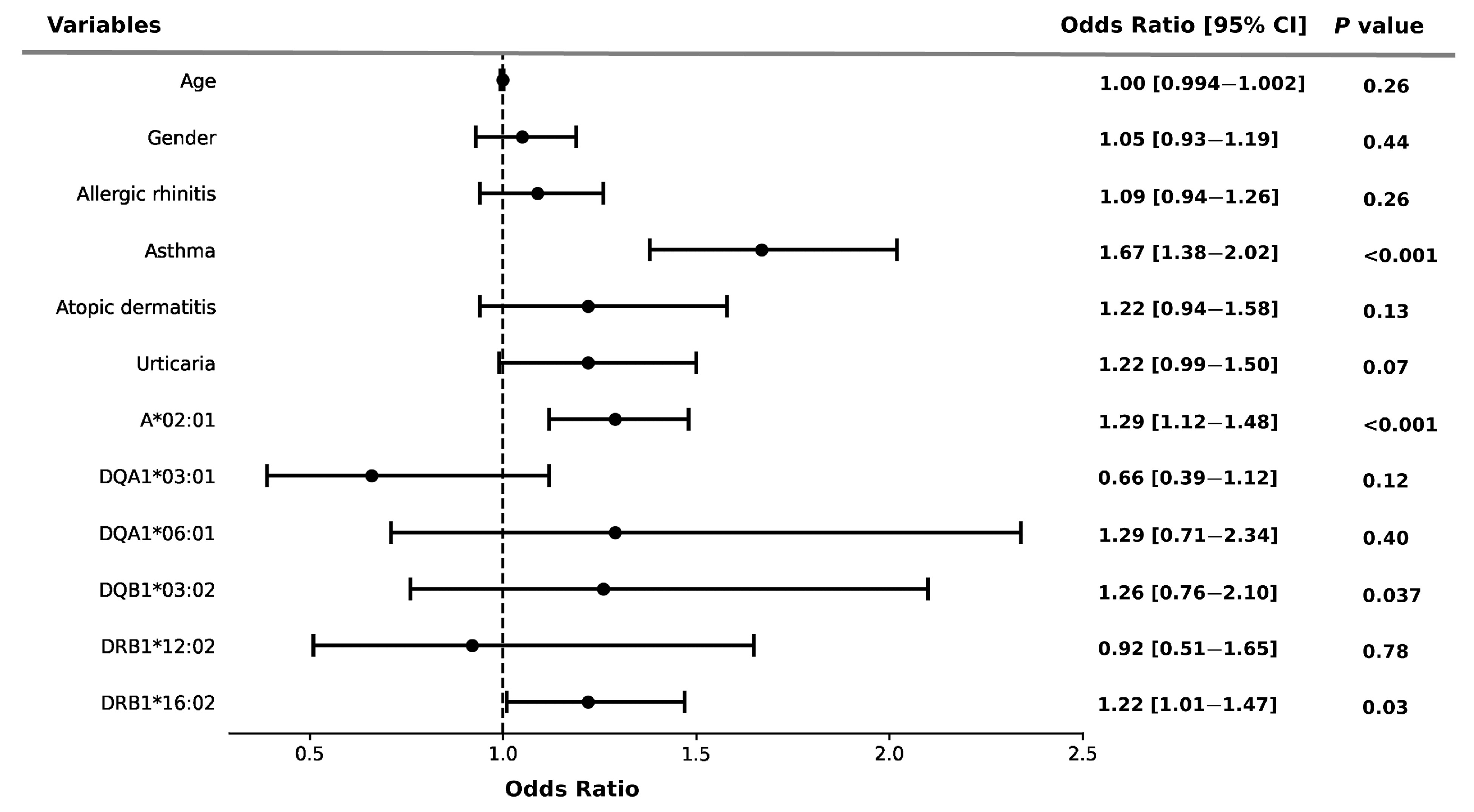
3.3. Association of HLA Alleles and Comorbidities with the Risk of NSAID Allergy
3.4. Distribution and Association of HLA Alleles with the Severity of Allergy
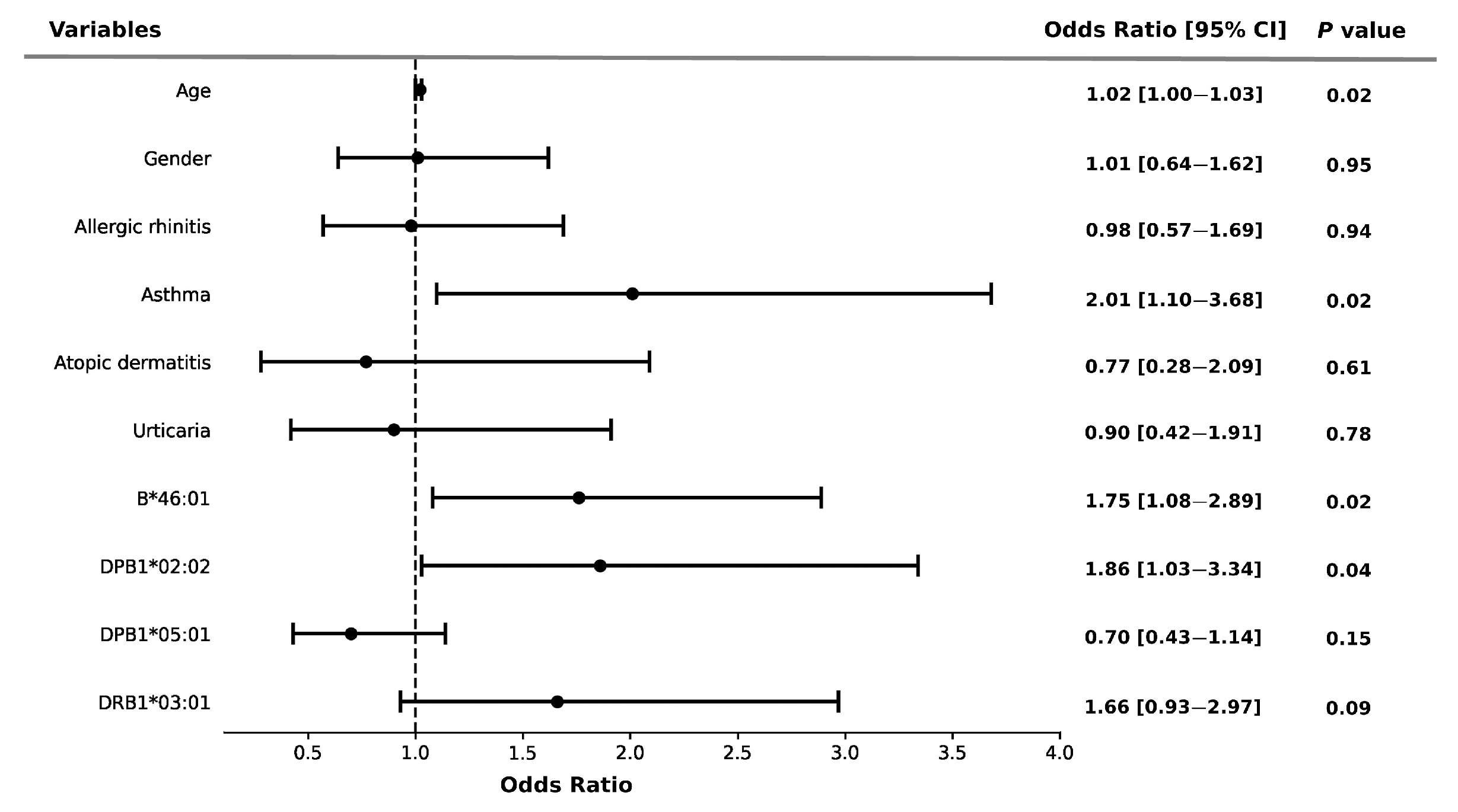
3.5. Association of HLA Alleles and Comorbidities with Severity of Allergy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | body max index |
| WBC | white blood cell |
| HgB | hemoglobin |
| PLT | platelet |
| GOT | glutamic-oxalacetic transaminase. |
| GPT | glutamyl pyruvic transaminase |
| HLA | Human leukocyte antigen |
| NSAIDs | Non-steroid anti-inflammatory drugs |
| ADR | adverse drug reactions |
| MHC | major histocompatibility complex |
| SJS | Stevens–Johnson syndrome |
| TEN | toxic epidermal necrolysis |
| AFs | allele frequencies |
| ICD-9-CM | International Classification of Diseases, Ninth Revision, Clinical Modification |
References
- Ong, C.K.; Lirk, P.; Tan, C.H.; Seymour, R.A. An evidence-based update on nonsteroidal anti-inflammatory drugs. Clin. Med. Res. 2007, 5, 19–34. [Google Scholar] [CrossRef] [PubMed]
- Bindu, S.; Mazumder, S.; Bandyopadhyay, U. Non-steroidal anti-inflammatory drugs (NSAIDs) and organ damage: A current perspective. Biochem. Pharmacol. 2020, 180, 114147. [Google Scholar] [CrossRef] [PubMed]
- Harirforoosh, S.; Asghar, W.; Jamali, F. Adverse effects of nonsteroidal antiinflammatory drugs: An update of gastrointestinal, cardiovascular and renal complications. J. Pharm. Pharm. Sci. 2013, 16, 821–847. [Google Scholar] [CrossRef] [PubMed]
- Yeung, W.Y.W.; Park, H.S. Update on the Management of Nonsteroidal Anti-Inflammatory Drug Hypersensitivity. Yonsei Med. J. 2020, 61, 4–14. [Google Scholar] [CrossRef]
- Hermans, M.A.W.; Otten, R.; Karim, A.F.; van Maaren, M.S. Nonsteroidal anti-inflammatory drug hypersensitivity: Not always an allergy! Neth. J. Med. 2018, 76, 52–59. [Google Scholar]
- Gomes, E.R.; Demoly, P. Epidemiology of hypersensitivity drug reactions. Curr. Opin. Allergy Clin. Immunol. 2005, 5, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Thong, B.Y. Nonsteroidal anti-inflammatory drug hypersensitivity in the Asia-Pacific. Asia Pac. Allergy 2018, 8, e38. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Dhopeshwarkar, N.; Blumenthal, K.G.; Goss, F.; Topaz, M.; Slight, S.P.; Bates, D.W. Drug allergies documented in electronic health records of a large healthcare system. Allergy 2016, 71, 1305–1313. [Google Scholar] [CrossRef]
- Rajan, J.P.; Wineinger, N.E.; Stevenson, D.D.; White, A.A. Prevalence of aspirin-exacerbated respiratory disease among asthmatic patients: A meta-analysis of the literature. J. Allergy Clin. Immunol. 2015, 135, 676–681.e1. [Google Scholar] [CrossRef]
- Denninger, J.W.; Marletta, M.A. Guanylate cyclase and the ˙NO/cGMP signaling pathway. Biochim. Biophys. Acta 1999, 1411, 334–350. [Google Scholar] [CrossRef]
- Laukeviciene, A.; Ugincius, P.; Korotkich, I.; Lazauskas, R.; Kevelaitis, E. Anaphylaxis of small arteries: Putative role of nitric oxide and prostanoids. Medicina 2010, 46, 38–44. [Google Scholar] [CrossRef]
- Choo, S.Y. The HLA system: Genetics, immunology, clinical testing, and clinical implications. Yonsei Med. J. 2007, 48, 11–23. [Google Scholar] [CrossRef]
- Chang, C.C.; Too, C.L.; Murad, S.; Hussein, S.H. Association of HLA-B*1502 allele with carbamazepine-induced toxic epidermal necrolysis and Stevens-Johnson syndrome in the multi-ethnic Malaysian population. Int. J. Dermatol. 2011, 50, 221–224. [Google Scholar] [CrossRef]
- Ferrell, P.B., Jr.; McLeod, H.L. Carbamazepine, HLA-B*1502 and risk of Stevens-Johnson syndrome and toxic epidermal necrolysis: US FDA recommendations. Pharmacogenomics 2008, 9, 1543–1546. [Google Scholar] [CrossRef]
- Hung, S.I.; Chung, W.H.; Liou, L.B.; Chu, C.C.; Lin, M.; Huang, H.P.; Lin, Y.L.; Lan, J.L.; Yang, L.C.; Hong, H.S.; et al. HLA-B*5801 allele as a genetic marker for severe cutaneous adverse reactions caused by allopurinol. Proc. Natl. Acad. Sci. USA 2005, 102, 4134–4139. [Google Scholar] [CrossRef] [PubMed]
- Khalili, N. The Immunogenetics of Cutaneous Drug Reactions. Adv. Exp. Med. Biol. 2022, 1367, 411–431. [Google Scholar] [CrossRef] [PubMed]
- Quiralte, J.; Sánchez-García, F.; Torres, M.J.; Blanco, C.; Castillo, R.; Ortega, N.; de Castro, F.R.; Pérez-Aciego, P.; Carrillo, T. Association of HLA-DR11 with the anaphylactoid reaction caused by nonsteroidal anti-inflammatory drugs. J. Allergy Clin. Immunol. 1999, 103, 685–689. [Google Scholar] [CrossRef]
- Ghattaoraya, G.S.; Dundar, Y.; González-Galarza, F.F.; Maia, M.H.; Santos, E.J.; da Silva, A.L.; McCabe, A.; Middleton, D.; Alfirevic, A.; Dickson, R.; et al. A web resource for mining HLA associations with adverse drug reactions: HLA-ADR. Database 2016, 2016, baw069. [Google Scholar] [CrossRef] [PubMed]
- Dahmani, D.I.; Chila, N.; Abdelouahab, F.; Bouyoucef, H.; Bougrida, M.; Rouabah, L.; Nedjar, F. Association between HLA-class II genes and asthma susceptibility in a selected Constantine population. Pan Afr. Med. J. 2020, 35, 48. [Google Scholar] [CrossRef]
- Doğan, N.; Çildağ, S.; Yenisey, Ç.; Şentürk, T. The association between chronic spontaneous urticaria and HLA class I and class II antigen. Turk. J. Med. Sci. 2020, 50, 1231–1235. [Google Scholar] [CrossRef]
- Zheng, X.; Shen, J.; Cox, C.; Wakefield, J.C.; Ehm, M.G.; Nelson, M.R.; Weir, B.S. HIBAG--HLA genotype imputation with attribute bagging. Pharmacogenom. J. 2014, 14, 192–200. [Google Scholar] [CrossRef]
- Niggemann, B.; Beyer, K. Time for a new grading system for allergic reactions? Allergy 2016, 71, 135–136. [Google Scholar] [CrossRef]
- Asero, R. Single NSAID hypersensitivity is associated with atopic status. Eur. Ann. Allergy Clin. Immunol. 2015, 47, 48–53. [Google Scholar]
- Asero, R. Intolerance to nonsteroidal anti-inflammatory drugs might precede by years the onset of chronic urticaria. J. Allergy Clin. Immunol. 2003, 111, 1095–1098. [Google Scholar] [CrossRef]
- Li, J.; Hao, Y.; Li, W.; Lv, X.; Gao, P. HLA-G in asthma and its potential as an effective therapeutic agent. Allergol. Immunopathol. 2023, 51, 22–29. [Google Scholar] [CrossRef]
- Kontakioti, E.; Domvri, K.; Papakosta, D.; Daniilidis, M. HLA and asthma phenotypes/endotypes: A review. Hum. Immunol. 2014, 75, 930–939. [Google Scholar] [CrossRef]
- Sánchez-Borges, M.; Caballero-Fonseca, F.; Capriles-Hulett, A. Cofactors and comorbidities in patients with aspirin/NSAID hypersensitivity. Allergol. Immunopathol. 2017, 45, 573–578. [Google Scholar] [CrossRef]
- Saper, V.E.; Ombrello, M.J.; Tremoulet, A.H.; Montero-Martin, G.; Prahalad, S.; Canna, S.; Shimizu, C.; Deutsch, G.; Tan, S.Y.; Remmers, E.F.; et al. Severe delayed hypersensitivity reactions to IL-1 and IL-6 inhibitors link to common HLA-DRB1*15 alleles. Ann. Rheum. Dis. 2022, 81, 406–415. [Google Scholar] [CrossRef] [PubMed]
- Redwood, A.J.; Pavlos, R.K.; White, K.D.; Phillips, E.J. HLAs: Key regulators of T-cell-mediated drug hypersensitivity. HLA 2018, 91, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S.; Becquemont, L. HLA-associated drug hypersensitivity and the prediction of adverse drug reactions. Pharmacogenomics 2017, 18, 1441–1457. [Google Scholar] [CrossRef] [PubMed]
- Pacor, M.L.; Di Lorenzo, G.; Mansueto, P.; Martinelli, N.; Esposito-Pellitteri, M.; Pradella, P.; Uxa, L.; Di Fede, G.; Rini, G.; Corrocher, R. Relationship between human leucocyte antigen class I and class II and chronic idiopathic urticaria associated with aspirin and/or NSAIDs hypersensitivity. Mediat. Inflamm. 2006, 2006, 62489. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Choi, J.H.; Lee, K.W.; Kim, S.H.; Shin, E.S.; Oh, H.B.; Suh, C.H.; Nahm, D.H.; Park, H.S. The human leucocyte antigen-DRB1*1302-DQB1*0609-DPB1*0201 haplotype may be a strong genetic marker for aspirin-induced urticaria. Clin. Exp. Allergy 2005, 35, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Dekker, J.W.; Nizankowska, E.; Schmitz-Schumann, M.; Pile, K.; Bochenek, G.; Dyczek, A.; Cookson, W.O.; Szczeklik, A. Aspirin-induced asthma and HLA-DRB1 and HLA-DPB1 genotypes. Clin. Exp. Allergy 1997, 27, 574–577. [Google Scholar] [CrossRef] [PubMed]
- Esmaeilzadeh, H.; Nabavi, M.; Amirzargar, A.A.; Aryan, Z.; Arshi, S.; Bemanian, M.H.; Fallahpour, M.; Mortazavi, N.; Rezaei, N. HLA-DRB and HLA-DQ genetic variability in patients with aspirin-exacerbated respiratory disease. Am. J. Rhinol. Allergy 2015, 29, e63–e69. [Google Scholar] [CrossRef]
- Trinh, H.K.T.; Pham, L.D.; Le, K.M.; Park, H.S. Pharmacogenomics of Hypersensitivity to Non-steroidal Anti-inflammatory Drugs. Front. Genet. 2021, 12, 647257. [Google Scholar] [CrossRef]
- Plaza-Serón, M.D.C.; García-Martín, E.; Agúndez, J.A.; Ayuso, P. Hypersensitivity reactions to nonsteroidal anti-inflammatory drugs: An update on pharmacogenetics studies. Pharmacogenomics 2018, 19, 1069–1086. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Park, H.S. Genetic markers for differentiating aspirin-hypersensitivity. Yonsei Med. J. 2006, 47, 15–21. [Google Scholar] [CrossRef]
- Murdaca, G.; Contini, P.; Negrini, S.; Ciprandi, G.; Puppo, F. Immunoregulatory Role of HLA-G in Allergic Diseases. J. Immunol. Res. 2016, 2016, 6865758. [Google Scholar] [CrossRef]
- Mosaad, Y.M. Clinical Role of Human Leukocyte Antigen in Health and Disease. Scand. J. Immunol. 2015, 82, 283–306. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | Total n = 13,387 | NSAID Allergy n = 1217 | Control n = 12,170 | p Value | |||
|---|---|---|---|---|---|---|---|
| n | (%) | n | (%) | n | (%) | ||
| Age, years a | 56 ± 16 | 55 ± 16 | 56 ± 16 | 0.46 | |||
| Sex (n, %) b | |||||||
| female | 8527 | (63.7) | 772 | (63.4) | 7755 | (63.7) | |
| male | 4860 | (36.3) | 445 | (36.6) | 4415 | (36.3) | 0.87 |
| BMI a | 25.1 ± 4.7 | 24.9 ± 4.6 | 25.1 ± 4.7 | 0.34 | |||
| WBC a | 7317 ± 2278 | 7228 ± 2176 | 7326 ± 2288 | 0.16 | |||
| Hemoglobin (HgB) a | 12.9 ± 1.7 | 13.1 ± 1.7 | 12.9 ± 1.8 | 0.001 | |||
| PLT a | 248 ± 68 | 252 ± 703,580 | 248 ± 68 | 0.06 | |||
| Creatinine a | 1.22 ± 1.54 | 1.05 ± 1.06 | 1.23 ± 1.58 | <0.001 | |||
| GOT a | 28 ± 20 | 28 ± 20 | 28 ± 20 | 0.93 | |||
| GPT a | 28 ± 20 | 28 ± 19 | 28 ± 20 | 0.52 | |||
| IgE a | 223 ± 641 | 307 ± 611 | 212 ± 644 | 0.02 | |||
| Eosinophils a | 276 ± 3283 | 235 ± 267 | 281 ± 3488 | 0.87 | |||
| Tryptase a | 5.81 ± 5.84 | 2.27 ± 0.88 | 7.23 ± 6.41 | 0.16 | |||
| Comorbidity (n, %) b | |||||||
| Allergic rhinitis | <0.001 | ||||||
| No | 10,583 | (79.1) | 917 | (75.3) | 9666 | (79.4) | |
| Yes | 2804 | (20.9) | 300 | (24.7) | 2504 | (20.6) | |
| Asthma | <0.001 | ||||||
| No | 12,247 | (91.5) | 1055 | (86.7) | 11,192 | (92) | |
| Yes | 1140 | (8.5) | 162 | (13.3) | 978 | (8) | |
| Atopic dermatitis | 0.02 | ||||||
| No | 12,778 | (95.5) | 1145 | (94.1) | 11,633 | (95.6) | |
| Yes | 609 | (4.5) | 72 | (5.9) | 537 | (4.4) | |
| Urticaria | 0.01 | ||||||
| No | 12,375 | (92.4) | 1101 | (90.5) | 11,274 | (92.6) | |
| Yes | 1012 | (7.6) | 116 | (9.5) | 896 | (7.4) | |
| Autoimmune | 0.65 | ||||||
| No | 10,219 | (76.3) | 936 | (76.9) | 9283 | (76.3) | |
| Yes | 3168 | (23.7) | 281 | (23.1) | 2887 | (23.7) | |
| Variables | NSAID Allergy | Control | p Value a,c | Risk of NSAID Allergy | ||||
|---|---|---|---|---|---|---|---|---|
| n = 2434 (Alleles) | n = 24,340 (Alleles) | |||||||
| n | (%) | n | (%) | OR (95% CI) | p Value b,c | |||
| A*02:01 | No | 2146 | (88.2) | 21,958 | (90.2) | |||
| Yes | 288 | (11.8) | 2382 | (9.8) | 0.002 * | 1.29 (1.12–1.48) | <0.001 * | |
| A*34:01 | No | 2430 | (99.8) | 24,336 | (99.9) | |||
| Yes | 4 | (0.2) | 4 | (0.0) | <0.001 * | 9.90 (2.47–39.7) | 0.001 * | |
| DQA1*03:01 | No | 2286 | (93.9) | 22,517 | (92.5) | |||
| Yes | 148 | (6.1) | 1823 | (7.5) | 0.013 | 0.79 (0.66–0.95) | 0.011 | |
| DQA1*06:01 | No | 2174 | (89.3) | 22,165 | (91.1) | |||
| Yes | (10.7) | 2175 | (8.9) | 0.005 * | 1.19 (1.03–1.39) | 0.020 | ||
| DQB1*03:02 | No | 2268 | (93.2) | 22,367 | (91.9) | |||
| Yes | 166 | (6.8) | 1973 | (8.1) | 0.028 | 0.82 (0.69–0.98) | 0.027 | |
| DRB1*12:02 | No | 2161 | (88.8) | 22,017 | (90.5) | |||
| Yes | 273 | (11.2) | 2323 | (9.5) | 0.009 * | 1.17 (1.01–1.36) | 0.032 | |
| DRB1*16:02 | No | 2285 | (93.9) | 23,101 | (94.9) | |||
| Yes | 149 | (6.1) | 1239 | (5.1) | 0.032 | 1.21 (1.01–1.46) | 0.038 | |
| Variables | Total n = 746 | Severe Allergy n = 94 | Mild Allergy n = 652 | p Value | |||
|---|---|---|---|---|---|---|---|
| n | (%) | n | (%) | n | (%) | ||
| Age, years a | 54 ± 15 | 57 ± 17 | 53 ± 15 | 0.01 | |||
| Sex (n, %) b | |||||||
| female | 485 | (65.0) | 60 | (63.8) | 425 | (65.2) | |
| male | 261 | (35.0) | 34 | (36.2) | 227 | (34.8) | 0.89 |
| BMI a | 25.0 ± 4.6 | 24.9 ± 3.8 | 25.0 ± 4.7 | 0.84 | |||
| Allergic rhinitis b | |||||||
| No | 542 | (72.7) | 66 | (70.2) | 476 | (73.0) | |
| Yes | 204 | (27.3) | 28 | (29.8) | 176 | (27.0) | 0.66 |
| Asthma b | |||||||
| No | 638 | (85.5) | 72 | (76.6) | 566 | (86.8) | |
| Yes | 108 | (14.5) | 22 | (23.4) | 86 | (13.2) | 0.01 |
| Atopic dermatitis b | |||||||
| No | 703 | (94.2) | 89 | (94.7) | 614 | (94.2) | |
| Yes | 43 | (5.8) | 5 | (5.3) | 38 | (5.8) | 1.00 |
| Urticaria b | |||||||
| No | 668 | (89.5) | 85 | (90.4) | 583 | (89.4) | |
| Yes | 78 | (10.5) | 9 | (9.6) | 69 | (10.6) | 0.91 |
| Autoimmune b | |||||||
| No | 562 | (75.3) | 75 | (79.8) | 487 | (74.7) | |
| Yes | 184 | (24.7) | 19 | (20.2) | 165 | (25.3) | 0.35 |
| Variables | Severe Allergy | Mild Allergy | p Value a,c | Risk of Severe Allergy | ||||
|---|---|---|---|---|---|---|---|---|
| n = 188 (Alleles) | n = 1304 (Alleles) | |||||||
| n | (%) | n | (%) | OR (95% CI) | p Value b,c | |||
| B*46:01 | No | 154 | (81.9) | 1154 | (88.5) | |||
| Yes | 34 | (18.1) | 150 | (11.5) | 0.014 * | 1.68 (1.04–2.71) | 0.035 | |
| DPB1*02:02 | No | 168 | (89.4) | 1225 | (93.9) | |||
| Yes | 20 | (10.6) | 79 | (6.1) | 0.0280 | 1.95 (1.11–3.42) | 0.020 | |
| DPB1*05:01 | No | 112 | (59.6) | 671 | (51.5) | |||
| Yes | 76 | (40.4) | 633 | (48.5) | 0.0450 | 0.62 (0.39–0.99) | 0.045 | |
| DRB1*03:01 | No | 168 | (89.4) | 1220 | (93.6) | |||
| Yes | 20 | (10.6) | 84 | (6.4) | 0.0500 | 1.73 (0.99–3.02) | 0.054 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, S.-L.; Lai, C.-H.; Lin, G.-C.; Chen, Y.-M.; Lee, M.-H.; Hsu, H.-S.; Chen, I.-C. Genetic Susceptibility of HLA Alleles to Non-Steroidal Anti-Inflammatory Drug Hypersensitivity in the Taiwanese Population. Biomedicines 2023, 11, 3273. https://doi.org/10.3390/biomedicines11123273
Chang S-L, Lai C-H, Lin G-C, Chen Y-M, Lee M-H, Hsu H-S, Chen I-C. Genetic Susceptibility of HLA Alleles to Non-Steroidal Anti-Inflammatory Drug Hypersensitivity in the Taiwanese Population. Biomedicines. 2023; 11(12):3273. https://doi.org/10.3390/biomedicines11123273
Chicago/Turabian StyleChang, Szu-Ling, Chih-Hung Lai, Guan-Cheng Lin, Yi-Ming Chen, Mei-Hsuan Lee, Han-Shui Hsu, and I-Chieh Chen. 2023. "Genetic Susceptibility of HLA Alleles to Non-Steroidal Anti-Inflammatory Drug Hypersensitivity in the Taiwanese Population" Biomedicines 11, no. 12: 3273. https://doi.org/10.3390/biomedicines11123273
APA StyleChang, S.-L., Lai, C.-H., Lin, G.-C., Chen, Y.-M., Lee, M.-H., Hsu, H.-S., & Chen, I.-C. (2023). Genetic Susceptibility of HLA Alleles to Non-Steroidal Anti-Inflammatory Drug Hypersensitivity in the Taiwanese Population. Biomedicines, 11(12), 3273. https://doi.org/10.3390/biomedicines11123273