

Taxanes in the Treatment of Head and Neck Squamous Cell Carcinoma

Abstract
1. Introduction
2. Taxane in HNSCC Clinical Application
2.1. Locally Advanced HNSCC
2.2. R/M HNSCC
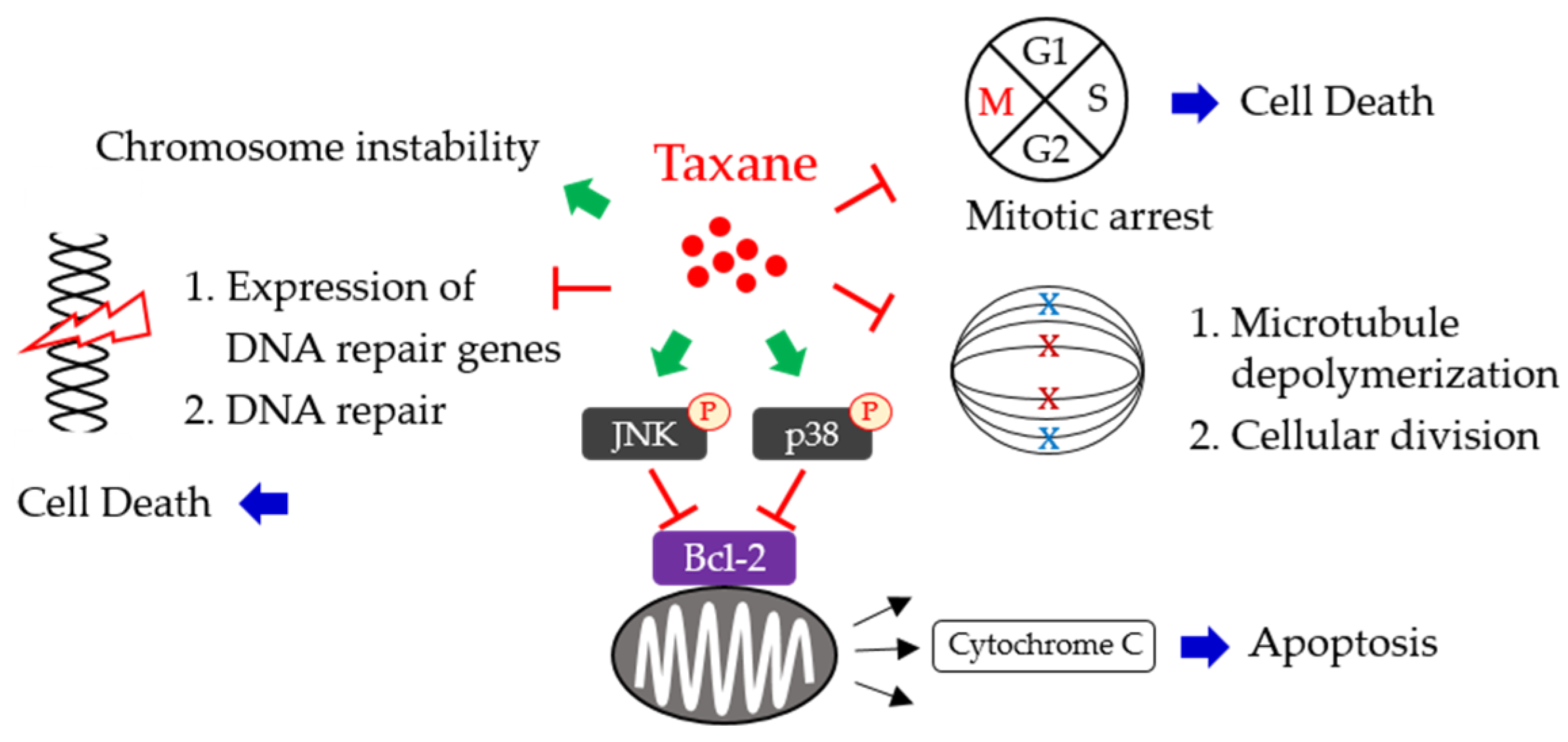
3. Molecular Mechanisms of Taxanes
3.1. Interfering the Function of Microtubules
3.2. Induction of Apoptosis
3.3. DNA Damage and DNA Repair Inhibition
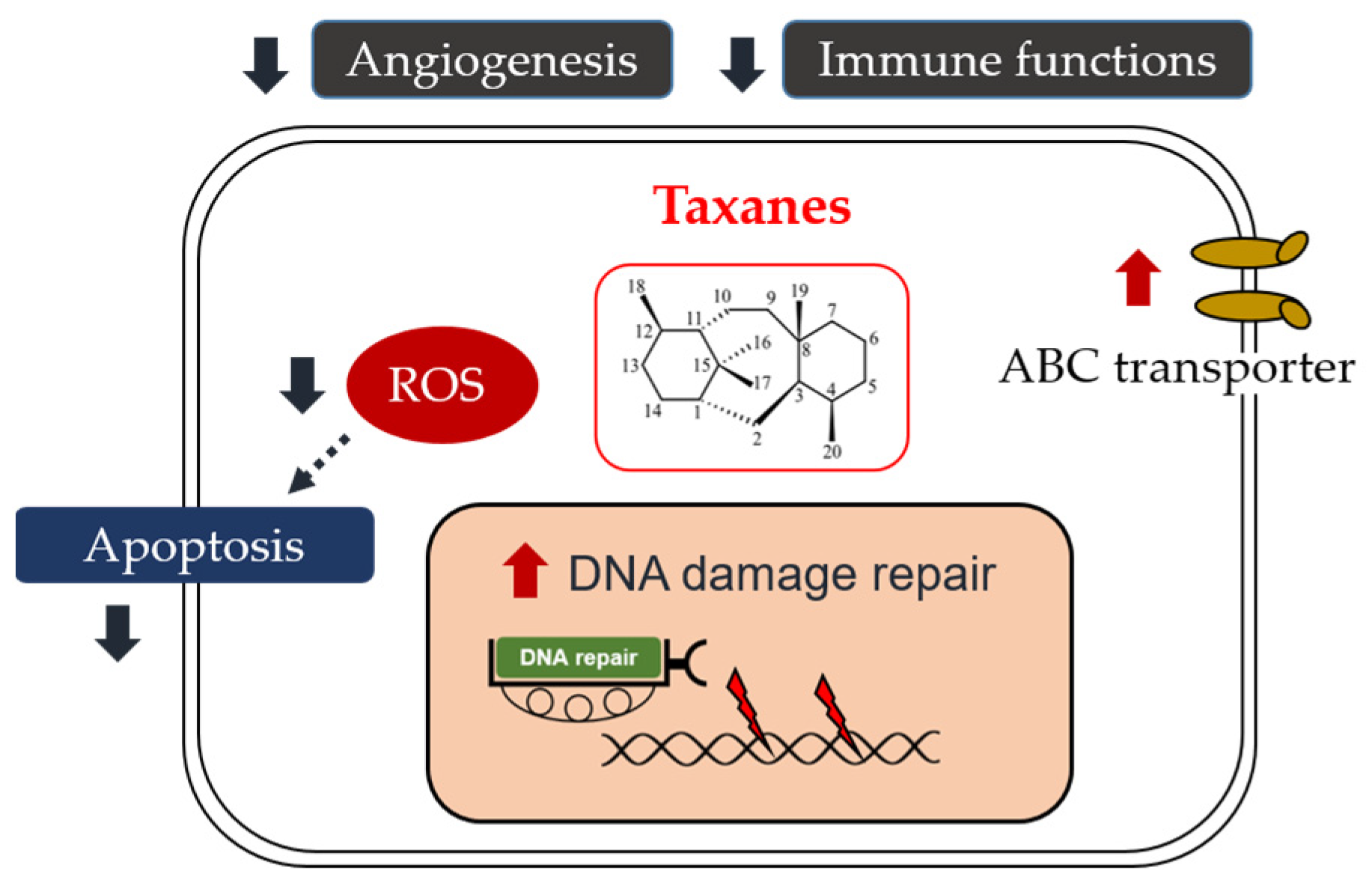
4. Taxane Resistance in HNSCC
4.1. Intrinsic Mechanisms
4.1.1. DNA/RNA Damage Repair
4.1.2. Drug Efflux
4.1.3. Apoptosis Inhibition
4.2. Extrinsic Mechanisms
4.2.1. Angiogenesis
4.2.2. The Interaction of Immune Therapy and Chemotherapy
4.2.3. Optimizing the Pharmacokinetics of Chemotherapy
5. Ongoing Clinical Trials
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and neck squamous cell carcinoma. Nat. Rev. Dis. Prim. 2020, 6, 92. [Google Scholar] [CrossRef]
- Leemans, C.R.; Snijders, P.J.F.; Brakenhoff, R.H. The molecular landscape of head and neck cancer. Nat. Rev. Cancer 2018, 18, 269–282. [Google Scholar] [CrossRef]
- Economopoulou, P.; de Bree, R.; Kotsantis, I.; Psyrri, A. Diagnostic Tumor Markers in Head and Neck Squamous Cell Carcinoma (HNSCC) in the Clinical Setting. Front. Oncol. 2019, 9, 827. [Google Scholar] [CrossRef]
- Chow, L.Q.M. Head and Neck Cancer. N. Engl. J. Med. 2020, 382, 60–72. [Google Scholar] [CrossRef] [PubMed]
- Gau, M.; Karabajakian, A.; Reverdy, T.; Neidhardt, E.M.; Fayette, J. Induction chemotherapy in head and neck cancers: Results and controversies. Oral Oncol. 2019, 95, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Wichmann, G.; Krüger, A.; Boehm, A.; Kolb, M.; Hofer, M.; Fischer, M.; Müller, S.; Purz, S.; Stumpp, P.; Sabri, O.; et al. Induction chemotherapy followed by radiotherapy for larynx preservation in advanced laryngeal and hypopharyngeal cancer: Outcome prediction after one cycle induction chemotherapy by a score based on clinical evaluation, computed tomography-based volumetry and 18F-FDG-PET/CT. Eur. J. Cancer 2017, 72, 144–155. [Google Scholar] [CrossRef]
- Hsieh, C.Y.; Lein, M.Y.; Yang, S.N.; Wang, Y.C.; Lin, Y.J.; Lin, C.Y.; Hua, C.H.; Tsai, M.H.; Lin, C.C. Dose-dense TPF induction chemotherapy for locally advanced head and neck cancer: A phase II study. BMC Cancer 2020, 20, 832. [Google Scholar] [CrossRef]
- Mosca, L.; Ilari, A.; Fazi, F.; Assaraf, Y.G.; Colotti, G. Taxanes in cancer treatment: Activity, chemoresistance and its overcoming. Drug Resist. Updat. 2021, 54, 100742. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.K.; Ryu, M.H.; Park, S.H.; Kim, J.G.; Kim, J.W.; Cho, S.H.; Park, Y.I.; Park, S.R.; Rha, S.Y.; Kang, M.J.; et al. Efficacy and safety findings from DREAM: A phase III study of DHP107 (oral paclitaxel) versus i.v. paclitaxel in patients with advanced gastric cancer after failure of first-line chemotherapy. Ann. Oncol. 2018, 29, 1220–1226. [Google Scholar] [CrossRef]
- Umanzor, G.; Cutler, D.L.; Barrios, F.J.; Vassallo, R.H.; Chivalan, M.A.; Bejarano, S.A.; Ramirez, J.R.; Fein, L.; Kramer, E.D.; Kowalyszyn, R.D.; et al. Oral paclitaxel with encequidar: The first orally administered paclitaxel shown to be superior to IV paclitaxel on confirmed response and survival with less neuropathy: A phase III clinical study in metastatic breast cancer (Abstract GS6-01). Cancer Res. 2020, 80 (Suppl. 4), GS6-01. [Google Scholar] [CrossRef]
- O’Shaughnessy, J.; Piccart, M.; Schwartzberg, L.S.; Cortes, J.; Harbeck, N.; Im, S.A.; Rugo, H.S.; Untch, M.; Yardley, D.A.; Bondarenko, I.; et al. CONTESSA: A multinational, multicenter, randomized, phase III registration study of tesetaxel plus a reduced dose of capecitabine in patients (pts) with HER2-, hormone receptor + (HR+) locally advanced or metastatic breast cancer (LA/MBC) who have previously received a taxane. J. Clin. Oncol. 2019, 37 (Suppl. 15), TPS1107. [Google Scholar] [CrossRef]
- Lei, L.; Wang, X.J.; Tang, S.C. Novel taxanes in development: Hopes or hypes? Crit. Rev. Oncol. Hematol. 2022, 176, 103727. [Google Scholar] [CrossRef]
- Churchill, C.D.; Klobukowski, M.; Tuszynski, J.A. Elucidating the mechanism of action of the clinically approved taxanes: A comprehensive comparison of local and allosteric effects. Chem. Biol. Drug Des. 2015, 86, 1253–1266. [Google Scholar] [CrossRef] [PubMed]
- Schiff, P.B.; Fant, J.; Horwitz, S.B. Promotion of microtubule assembly in vitro by taxol. Nature 1979, 277, 665–667. [Google Scholar] [CrossRef] [PubMed]
- Ramos, A.; Sadeghi, S.; Tabatabaeian, H. Battling Chemoresistance in Cancer: Root Causes and Strategies to Uproot Them. Int. J. Mol. Sci. 2021, 22, 9451. [Google Scholar] [CrossRef] [PubMed]
- Vermorken, J.B.; Remenar, E.; van Herpen, C.; Gorlia, T.; Mesia, R.; Degardin, M.; Stewart, J.S.; Jelic, S.; Betka, J.; Preiss, J.H.; et al. Cisplatin, fluorouracil, and docetaxel in unresectable head and neck cancer. N. Engl. J. Med. 2007, 357, 1695–1704. [Google Scholar] [CrossRef]
- Posner, M.R.; Hershock, D.M.; Blajman, C.R.; Mickiewicz, E.; Winquist, E.; Gorbounova, V.; Tjulandin, S.; Shin, D.M.; Cullen, K.; Ervin, T.J.; et al. Cisplatin and fluorouracil alone or with docetaxel in head and neck cancer. N. Engl. J. Med. 2007, 357, 1705–1715. [Google Scholar] [CrossRef]
- Guigay, J.; Fayette, J.; Mesia, R.; Saada-Bouzid, E.; Lafond, C.; Geoffrois, L.; Martin, L.; Capitain, O.; Cupissol, D.; Castanie, H.; et al. TPExtreme randomized trial: Quality of Life (QoL) and survival according to second-line treatments in patients with recurrent/metastatic head and neck squamous cell carcinoma (R/M HNSCC). J. Clin. Oncol. 2020, 38 (Suppl. 15), 6507. [Google Scholar] [CrossRef]
- Saleh, K.; Daste, A.; Martin, N.; Pons-Tostivint, E.; Auperin, A.; Herrera-Gomez, R.G.; Baste-Rotllan, N.; Bidault, F.; Guigay, J.; Le Tourneau, C.; et al. Response to salvage chemotherapy after progression on immune checkpoint inhibitors in patients with recurrent and/or metastatic squamous cell carcinoma of the head and neck. Eur. J. Cancer 2019, 121, 123–129. [Google Scholar] [CrossRef]
- Jacinto, J.K.; Co, J.; Mejia, M.B.; Regala, E.E. The evidence on effectiveness of weekly vs. triweekly cisplatin concurrent with radiotherapy in locally advanced head and neck squamous cell carcinoma (HNSCC): A systematic review and meta-analysis. Br. J. Radiol. 2017, 90, 20170442. [Google Scholar] [CrossRef] [PubMed]
- Mody, M.D.; Rocco, J.W.; Yom, S.S.; Haddad, R.I.; Saba, N.F. Head and neck cancer. Lancet 2021, 398, 2289–2299. [Google Scholar] [CrossRef]
- Guigay, J.; Tahara, M.; Licitra, L.; Keilholz, U.; Friesland, S.; Witzler, P.; Mesía, R. The Evolving Role of Taxanes in Combination with Cetuximab for the Treatment of Recurrent and/or Metastatic Squamous Cell Carcinoma of the Head and Neck: Evidence, Advantages, and Future Directions. Front. Oncol. 2019, 9, 668. [Google Scholar] [CrossRef]
- Lai, J.I.; Chao, T.C.; Liu, C.Y.; Huang, C.C.; Tseng, L.M. A systemic review of taxanes and their side effects in metastatic breast cancer. Front. Oncol. 2022, 12, 940239. [Google Scholar] [CrossRef]
- Perl, G.; Ben-Aharon, I.; Popovtzer, A.; Stemmer, S.M.; Vidal, L. Addition of taxane to induction therapy in head and neck malignancies: A systematic review and meta-analysis of randomized controlled trials. Chemotherapy 2013, 59, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Grégoire, V.; Lefebvre, J.L.; Licitra, L.; Felip, E.; EHNS-ESMO-ESTRO Guidelines Working Group. Squamous cell carcinoma of the head and neck: EHNS-ESMO-ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2010, 21 (Suppl. 5), v184–v186. [Google Scholar] [CrossRef]
- Marur, S.; Forastiere, A.A. Head and Neck Squamous Cell Carcinoma: Update on Epidemiology, Diagnosis, and Treatment. Mayo Clin. Proc. 2016, 91, 386–396. [Google Scholar] [CrossRef] [PubMed]
- Pignon, J.P.; le Maître, A.; Maillard, E.; Bourhis, J.; MACH-NC Collaborative Group. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): An update on 93 randomised trials and 17,346 patients. Radiother. Oncol. 2009, 92, 4–14. [Google Scholar] [CrossRef]
- Hitt, R.; Grau, J.J.; López-Pousa, A.; Berrocal, A.; García-Girón, C.; Irigoyen, A.; Sastre, J.; Martínez-Trufero, J.; Brandariz Castelo, J.A.; Verger, E.; et al. A randomized phase III trial comparing induction chemotherapy followed by chemoradiotherapy versus chemoradiotherapy alone as treatment of unresectable head and neck cancer. Ann. Oncol. 2014, 25, 216–225. [Google Scholar] [CrossRef]
- Cohen, E.E.; Karrison, T.G.; Kocherginsky, M.; Mueller, J.; Egan, R.; Huang, C.H.; Brockstein, B.E.; Agulnik, M.B.; Mittal, B.B.; Yunus, F.; et al. Phase III randomized trial of induction chemotherapy in patients with N2 or N3 locally advanced head and neck cancer. J. Clin. Oncol. 2014, 32, 2735–2743. [Google Scholar] [CrossRef]
- Ghi, M.G.; Paccagnella, A.; Ferrari, D.; Foa, P.; Alterio, D.; Codecà, C.; Nolè, F.; Verri, E.; Orecchia, R.; Morelli, F.; et al. Induction TPF followed by concomitant treatment versus concomitant treatment alone in locally advanced head and neck cancer. A phase II–III trial. Ann. Oncol. 2017, 28, 2206–2212. [Google Scholar] [CrossRef] [PubMed]
- Haddad, R.I.; Posner, M.; Hitt, R.; Cohen, E.E.W.; Schulten, J.; Lefebvre, J.L.; Vermorken, J.B. Induction chemotherapy in locally advanced squamous cell carcinoma of the head and neck: Role, controversy, and future directions. Ann. Oncol. 2018, 29, 1130–1140. [Google Scholar] [CrossRef]
- Yano, R.; Konno, A.; Watanabe, K.; Tsukamoto, H.; Kayano, Y.; Ohnaka, H.; Goto, N.; Nakamura, T.; Masada, M. Pharmacoethnicity of docetaxel-induced severe neutropenia: Integrated analysis of published phase II and III trials. Int. J. Clin. Oncol. 2013, 18, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Okano, S.; Enokida, T.; Onoe, T.; Ota, Y.; Motegi, A.; Zenda, S.; Akimoto, T.; Tahara, M. Induction TPF chemotherapy followed by CRT with fractionated administration of cisplatin in patients with unresectable locally advanced head and neck cancer. Int. J. Clin. Oncol. 2019, 24, 789–797. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Q.; Fang, J.; Huang, Z.; Yang, Y.; Lian, M.; Liu, H.; Zhang, Y.; Ye, J.; Hui, X.; Wang, Y.; et al. A response prediction model for taxane, cisplatin, and 5-fluorouracil chemotherapy in hypopharyngeal carcinoma. Sci. Rep. 2018, 8, 12675. [Google Scholar] [CrossRef]
- Lau, A.; Yang, W.F.; Li, K.Y.; Su, Y.X. Systemic Therapy in Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma—A Systematic Review and Meta-Analysis. Crit. Rev. Oncol. Hematol. 2020, 153, 102984. [Google Scholar] [CrossRef]
- Guigay, J.; Aupérin, A.; Fayette, J.; Saada-Bouzid, E.; Lafond, C.; Taberna, M.; Geoffrois, L.; Martin, L.; Capitain, O.; Cupissol, D.; et al. Cetuximab, docetaxel, and cisplatin versus platinum, fluorouracil, and cetuximab as first-line treatment in patients with recurrent or metastatic head and neck squamous-cell carcinoma (GORTEC 2014-01 TPExtreme): A multicentre, open-label, randomised, phase 2 trial. Lancet Oncol. 2021, 22, 463–475. [Google Scholar] [CrossRef]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulières, D.; Tahara, M.; de Castro, G., Jr.; Psyrri, A.; Basté, N.; Neupane, P.; Bratland, Å.; et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised, open-label, phase 3 study. Lancet 2019, 394, 1915–1928. [Google Scholar] [CrossRef]
- Dzienis, M.R.; Cundom, J.E.; Fuentes, C.S.; Hansen, A.R.; Nordlinger, M.J.; Pastor, A.V.; Oppelt, P.; Neki, A.; Gregg, R.W.; Lima, I.P.F.; et al. Pembrolizumab (pembro) + carboplatin (carbo) + paclitaxel (pacli) as first-line (1L) therapy in recurrent/metastatic (R/M) head and neck squamous cell carcinoma (HNSCC): Phase VI KEYNOTE-B10 study. Ann. Oncol. 2022, 33 (Suppl. 7), S295–S322. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gümüş, M.; Mazières, J.; Hermes, B.; Çay Şenler, F.; Csőszi, T.; Fülöp, A.; et al. Pembrolizumab plus Chemotherapy for Squamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef]
- Fuereder, T.; Minichsdorfer, C.; Mittlboeck, M.; Wagner, C.; Heller, G.; Putz, E.M.; Oberndorfer, F.; Müllauer, L.; Aretin, M.B.; Czerny, C.; et al. Pembrolizumab plus docetaxel for the treatment of recurrent/metastatic head and neck cancer: A prospective phase I/II study. Oral Oncol. 2022, 124, 105634. [Google Scholar] [CrossRef]
- Huang, Y.; Sun, J.; Li, J.; Zhu, D.; Dong, M.; Dou, S.; Tang, Y.; Shi, W.; Sun, Q.; Zhao, T.; et al. Neoadjuvant immunochemotherapy for locally advanced resectable oral squamous cell carcinoma: A prospective single-arm trial (Illuminate Trial). Int. J. Surg. 2023, 109, 2220–2227. [Google Scholar] [CrossRef]
- Patil, V.M.; Noronha, V.; Menon, N.; Singh, A.; Ghosh-Laskar, S.; Budrukkar, A.; Bhattacharjee, A.; Swain, M.; Mathrudev, V.; Nawale, K.; et al. Results of Phase III Randomized Trial for Use of Docetaxel as a Radiosensitizer in Patients With Head and Neck Cancer, Unsuitable for Cisplatin-Based Chemoradiation. J. Clin. Oncol. 2023, 41, 2350–2361. [Google Scholar] [CrossRef] [PubMed]
- Hitt, R.; Mesía, R.; Lozano, A.; Iglesias Docampo, L.; Grau, J.J.; Taberna, M.; Rubió-Casadevall, J.; Martínez-Trufero, J.; Morillo, E.D.B.; García Girón, C.; et al. Randomized phase 3 noninferiority trial of radiotherapy and cisplatin vs radiotherapy and cetuximab after docetaxel-cisplatin-fluorouracil induction chemotherapy in patients with locally advanced unresectable head and neck cancer. Oral Oncol. 2022, 134, 106087. [Google Scholar] [CrossRef] [PubMed]
- Le, X.; Gleber-Netto, F.O.; Rubin, M.L.; Qing, Y.; Du, R.; Kies, M.; Blumenschein, G., Jr.; Lu, C.; Johnson, F.M.; Bell, D.; et al. Induction chemotherapy with or without erlotinib in patients with head and neck squamous cell carcinoma amenable for surgical resection. Clin. Cancer Res. 2022, 28, 2796–2806. [Google Scholar] [CrossRef]
- Martínez-Trufero, J.; Lozano Borbalas, A.; Pajares Bernad, I.; Taberna Sanz, M.; Ortega Izquierdo, E.; Cirauqui Cirauqui, B.; Rubió-Casadevall, J.; Plana Serrahima, M.; Ponce Ortega, J.M.; Planas Toledano, I.; et al. Sequential chemotherapy regimen of induction with panitumumab and paclitaxel followed by radiotherapy and panitumumab in patients with locally advanced head and neck cancer unfit for platinum derivatives. The phase II, PANTERA/TTCC-2010-06 study. Clin. Transl. Oncol. 2021, 23, 1666–1677. [Google Scholar] [CrossRef] [PubMed]
- Keil, F.; Hartl, M.; Altorjai, G.; Berghold, A.; Riedl, R.; Pecherstorfer, M.; Mayrbäurl, B.; De Vries, A.; Schuster, J.; Hackl, J.; et al. Docetaxel, cisplatin and 5-FU compared with docetaxel, cisplatin and cetuximab as induction chemotherapy in advanced squamous cell carcinoma of the head and neck: Results of a randomised phase II AGMT trial. Eur. J. Cancer 2021, 151, 201–210. [Google Scholar] [CrossRef]
- Oppelt, P.; Ley, J.; Daly, M.; Rich, J.; Paniello, R.; Jackson, R.S.; Pipkorn, P.; Liu, J.; Gay, H.; Palka, K.; et al. nab-Paclitaxel and cisplatin followed by cisplatin and radiation (Arm 1) and nab-paclitaxel followed by cetuximab and radiation (Arm 2) for locally advanced head and neck squamous-cell carcinoma: A multicenter, non-randomized phase 2 trial. Med. Oncol. 2021, 38, 35. [Google Scholar] [CrossRef] [PubMed]
- Fayette, J.; Cropet, C.; Gautier, J.; Toullec, C.; Burgy, M.; Bruyas, A.; Sire, C.; Lagrange, A.; Clatot, F.; Calderon, B.; et al. Results of the multicenter phase II FRAIL-IMMUNE trial evaluating the efficacy and safety of durvalumab combined with weekly paclitaxel carboplatin in first-line in patients (pts) with recurrent/metastatic squamous cell carcinoma of the head and neck (R/M SCCHN) not eligible for cisplatin-based therapies. J. Clin. Oncol. 2023, 41 (Suppl. 16), 6003. [Google Scholar] [CrossRef]
- Adkins, D.; Ley, J.; Atiq, O.; Powell, S.; Spanos, W.C.; Gitau, M.; Rigden, C.; Palka, K.; Liu, J.; Oppelt, P. Nanoparticle albumin-bound paclitaxel with cetuximab and carboplatin as first-line therapy for recurrent or metastatic head and neck cancer: A single-arm, multicenter, phase 2 trial. Oral Oncol. 2021, 115, 105173. [Google Scholar] [CrossRef]
- Bacus, S.S.; Gudkov, A.V.; Lowe, M.; Lyass, L.; Yung, Y.; Komarov, A.P.; Keyomarsi, K.; Yarden, Y.; Seger, R. Taxol-induced apoptosis depends on MAP kinase pathways (ERK and p38) and is independent of p53. Oncogene 2001, 20, 147–155. [Google Scholar] [CrossRef]
- Gurbi, B.; Brauswetter, D.; Varga, A.; Gyulavári, P.; Pénzes, K.; Murányi, J.; Zámbó, V.; Birtalan, E.; Krenács, T.; Becker, D.L.; et al. The Potential Impact of Connexin 43 Expression on Bcl-2 Protein Level and Taxane Sensitivity in Head and Neck Cancers—In Vitro Studies. Cancers 2019, 11, 1848. [Google Scholar] [CrossRef] [PubMed]
- Selimovic, D.; Hassan, M.; Haikel, Y.; Hengge, U.R. Taxol-induced mitochondrial stress in melanoma cells is mediated by activation of c-Jun N-terminal kinase (JNK) and p38 pathways via uncoupling protein 2. Cell. Signal. 2008, 20, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.Y.; Lin, C.C.; Huang, Y.W.; Chen, J.H.; Tsou, Y.A.; Chang, L.C.; Fan, C.C.; Lin, C.Y.; Chang, W.C. Macrophage secretory IL-1β promotes docetaxel resistance in head and neck squamous carcinoma via SOD2/CAT-ICAM1 signaling. JCI Insight 2022, 7, e157285. [Google Scholar] [CrossRef] [PubMed]
- Hung, C.H.; Chan, S.H.; Chu, P.M.; Tsai, K.L. Docetaxel Facilitates Endothelial Dysfunction through Oxidative Stress via Modulation of Protein Kinase C Beta: The Protective Effects of Sotrastaurin. Toxicol. Sci. 2015, 145, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Pan, Z.; Gollahon, L. Taxol directly induces endoplasmic reticulum-associated calcium changes that promote apoptosis in breast cancer cells. Breast J. 2011, 17, 56–70. [Google Scholar] [CrossRef] [PubMed]
- Pan, Z.; Avila, A.; Gollahon, L. Paclitaxel induces apoptosis in breast cancer cells through different calcium—Regulating mechanisms depending on external calcium conditions. Int. J. Mol. Sci. 2014, 15, 2672–2694. [Google Scholar] [CrossRef]
- Swanton, C.; Nicke, B.; Schuett, M.; Eklund, A.C.; Ng, C.; Li, Q.; Hardcastle, T.; Lee, A.; Roy, R.; East, P.; et al. Chromosomal instability determines taxane response. Proc. Natl. Acad. Sci. USA 2009, 106, 8671–8676. [Google Scholar] [CrossRef] [PubMed]
- Carter, S.L.; Eklund, A.C.; Kohane, I.S.; Harris, L.N.; Szallasi, Z. A signature of chromosomal instability inferred from gene expression profiles predicts clinical outcome in multiple human cancers. Nat. Genet. 2006, 38, 1043–1048. [Google Scholar] [CrossRef]
- Jean, S.; Li, J.; Katsaros, D.; Wubbenhorst, B.; Maxwell, K.N.; Fishbein, L.; McLane, M.W.; Benedetto, C.; Canuto, E.M.; Mitra, N.; et al. Paclitaxel is necessary for improved survival in epithelial ovarian cancers with homologous recombination gene mutations. Oncotarget 2016, 7, 48577–48585. [Google Scholar] [CrossRef][Green Version]
- Busatto, F.F.; Viero, V.P.; Schaefer, B.T.; Saffi, J. Cell growth analysis and nucleotide excision repair modulation in breast cancer cells submitted to a protocol using doxorubicin and paclitaxel. Life Sci. 2021, 268, 118990. [Google Scholar] [CrossRef]
- Burcher, K.M.; Faucheux, A.T.; Lantz, J.W.; Wilson, H.L.; Abreu, A.; Salafian, K.; Patel, M.J.; Song, A.H.; Petro, R.M.; Lycan, T., Jr.; et al. Prevalence of DNA Repair Gene Mutations in Blood and Tumor Tissue and Impact on Prognosis and Treatment in HNSCC. Cancers 2021, 13, 3118. [Google Scholar] [CrossRef] [PubMed]
- Cury, S.S.; Miranda, P.M.; Marchi, F.A.; Canto, L.M.D.; Chulam, T.C.; Petersen, A.H.; Aagaard, M.M.; Pinto, C.A.L.; Kowalski, L.P.; Rogatto, S.R. Germline variants in DNA repair genes are associated with young-onset head and neck cancer. Oral Oncol. 2021, 122, 105545. [Google Scholar] [CrossRef] [PubMed]
- Prochnow, S.; Wilczak, W.; Bosch, V.; Clauditz, T.S.; Muenscher, A. ERCC1, XPF and XPA—Locoregional differences and prognostic value of DNA repair protein expression in patients with head and neck squamous cell carcinoma. Clin. Oral Investig. 2019, 23, 3319–3329. [Google Scholar] [CrossRef]
- Psyrri, A.; Gkotzamanidou, M.; Papaxoinis, G.; Krikoni, L.; Economopoulou, P.; Kotsantis, I.; Anastasiou, M.; Souliotis, V.L. The DNA damage response network in the treatment of head and neck squamous cell carcinoma. ESMO Open 2021, 6, 100075. [Google Scholar] [CrossRef]
- Hsieh, C.Y.; Chang, W.C.; Lin, C.C.; Chen, J.H.; Lin, C.Y.; Liu, C.H.; Lin, C.; Hung, M.C. Combination treatment of arsenic trioxide and osimertinib in recurrent and metastatic head and neck squamous cell carcinoma. Am. J. Cancer Res. 2022, 12, 5049–5061. [Google Scholar]
- De Vos, M.; Schreiber, V.; Dantzer, F. The diverse roles and clinical relevance of PARPs in DNA damage repair: Current state of the art. Biochem. Pharmacol. 2012, 84, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Pascal, J.M. The comings and goings of PARP-1 in response to DNA damage. DNA Repair 2018, 71, 177–182. [Google Scholar] [CrossRef]
- Moutafi, M.; Economopoulou, P.; Rimm, D.; Psyrri, A. PARP inhibitors in head and neck cancer: Molecular mechanisms, preclinical and clinical data. Oral Oncol. 2021, 117, 105292. [Google Scholar] [CrossRef]
- Glorieux, M.; Dok, R.; Nuyts, S. Novel DNA targeted therapies for head and neck cancers: Clinical potential and biomarkers. Oncotarget 2017, 8, 81662–81678. [Google Scholar] [CrossRef]
- de Haan, R.; van Werkhoven, E.; van den Heuvel, M.M.; Peulen, H.M.U.; Sonke, G.S.; Elkhuizen, P.; van den Brekel, M.W.M.; Tesselaar, M.E.T.; Vens, C.; Schellens, J.H.M.; et al. Study protocols of three parallel phase 1 trials combining radical radiotherapy with the PARP inhibitor olaparib. BMC Cancer 2019, 19, 901. [Google Scholar] [CrossRef]
- Jelinek, M.J.; Foster, N.R.; Zoroufy, A.J.; Schwartz, G.K.; Munster, P.N.; Seiwert, T.Y.; de Souza, J.A.; Vokes, E.E. A phase I trial adding poly(ADP-ribose) polymerase inhibitor veliparib to induction carboplatin-paclitaxel in patients with head and neck squamous cell carcinoma: Alliance A091101. Oral Oncol. 2021, 114, 105171. [Google Scholar] [CrossRef]
- Méndez, E.; Rodriguez, C.P.; Kao, M.C.; Raju, S.; Diab, A.; Harbison, R.A.; Konnick, E.Q.; Mugundu, G.M.; Santana-Davila, R.; Martins, R.; et al. A Phase I Clinical Trial of AZD1775 in Combination with Neoadjuvant Weekly Docetaxel and Cisplatin before Definitive Therapy in Head and Neck Squamous Cell Carcinoma. Clin. Cancer Res. 2018, 24, 2740–2748. [Google Scholar] [CrossRef] [PubMed]
- Portugal, J.; Mansilla, S.; Bataller, M. Mechanisms of drug-induced mitotic catastrophe in cancer cells. Curr. Pharm. Des. 2010, 16, 69–78. [Google Scholar] [CrossRef]
- Kao, M.; Green, C.; Sidorova, J.; Méndez, E. Strategies for Targeted Therapy in Head and Neck Squamous Cell Carcinoma Using WEE1 Inhibitor AZD1775. JAMA Otolaryngol. Head Neck Surg. 2017, 143, 631–633. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Liao, J.; Lapidus, R.G.; Fan, X.; Mehra, R.; Cullen, K.J.; Dan, H. Targeting Wee1 kinase to suppress proliferation and survival of cisplatin-resistant head and neck squamous cell carcinoma. Cancer Chemother. Pharmacol. 2022, 89, 469–478. [Google Scholar] [CrossRef]
- Mohammad, I.S.; He, W.; Yin, L. Understanding of human ATP binding cassette superfamily and novel multidrug resistance modulators to overcome MDR. Biomed. Pharmacother. 2018, 100, 335–348. [Google Scholar] [CrossRef] [PubMed]
- Xiao, H.; Zheng, Y.; Ma, L.; Tian, L.; Sun, Q. Clinically-Relevant ABC Transporter for Anti-Cancer Drug Resistance. Front. Pharmacol. 2021, 12, 648407. [Google Scholar] [CrossRef]
- Callaghan, R.; Luk, F.; Bebawy, M. Inhibition of the multidrug resistance P-glycoprotein: Time for a change of strategy? Drug Metab. Dispos. 2014, 42, 623–631. [Google Scholar] [CrossRef]
- Dechsupa, N.; Khamto, N.; Chawapun, P.; Siriphong, S.; Innuan, P.; Suwan, A.; Luangsuep, T.; Photilimthana, N.; Maita, W.; Thanacharttanatchaya, R.; et al. Pentagalloyl Glucose-Targeted Inhibition of P-Glycoprotein and Re-Sensitization of Multidrug-Resistant Leukemic Cells (K562/ADR) to Doxorubicin: In Silico and Functional Studies. Pharmaceuticals 2023, 16, 1192. [Google Scholar] [CrossRef]
- Chen, Q.H. Crosstalk between Microtubule Stabilizing Agents and Prostate Cancer. Cancers 2023, 15, 3308. [Google Scholar] [CrossRef] [PubMed]
- Joshi, A.; Patil, V.; Noronha, V.; Dhumal, S.; Pande, N.; Chandrasekharan, A.; Turkar, S.; Dsouza, H.; Shrirangwar, S.; Mahajan, A.; et al. Results of a phase II randomized controlled clinical trial comparing efficacy of Cabazitaxel versus Docetaxel as second line or above therapy in recurrent head and neck cancer. Oral Oncol. 2017, 75, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Nightingale, G.; Ryu, J. Cabazitaxel (jevtana): A novel agent for metastatic castration-resistant prostate cancer. Pharm. Ther. 2012, 37, 440–448. [Google Scholar]
- Mody, M.D.; Gill, H.S.; Saba, N.F. The Evolving and Future Role of Taxanes in Squamous Cell Carcinomas of the Head and Neck: A Review. JAMA Otolaryngol. Head Neck Surg. 2016, 142, 898–905. [Google Scholar] [CrossRef]
- Swiecicki, P.; Yilmaz, E.; Rosenberg, A.J.; Fujisawa, T.; Yang Bruce, J.; Meng, C.; Wozniak, M.; Wang, L.; Rao Gorla, S.; Lyn Geiger, J. Enfortumab vedotin in the previously treated advanced head and neck cancer (HNC) cohort of EV-202. J. Clin. Oncol. 2023, 41 (Suppl. 16), 6017. [Google Scholar] [CrossRef]
- Shao, T.; Chen, T.; Chen, Y.; Liu, X.; Chen, Y.L.; Wang, Q.; Zhu, T.; Guo, M.; Li, H.; Ju, D.; et al. Construction of paclitaxel-based antibody—Drug conjugates with a PEGylated linker to achieve superior therapeutic index. Signal Transduct. Target. Ther. 2020, 5, 132. [Google Scholar] [CrossRef]
- Evans, N.; Grygorash, R.; Williams, P.; Kyle, A.; Kantner, T.; Pathak, R.; Sheng, X.; Simoes, F.; Makwana, H.; Resende, R.; et al. Incorporation of Hydrophilic Macrocycles Into Drug-Linker Reagents Produces Antibody-Drug Conjugates With Enhanced in vivo Performance. Front. Pharmacol. 2022, 13, 764540. [Google Scholar] [CrossRef]
- Domanitskaya, N.; Wangari-Talbot, J.; Jacobs, J.; Peiffer, E.; Mahdaviyeh, Y.; Paulose, C.; Malofeeva, E.; Foster, K.; Cai, K.Q.; Zhou, Y.; et al. Abcc10 status affects mammary tumour growth, metastasis, and docetaxel treatment response. Br. J. Cancer 2014, 111, 696–707. [Google Scholar] [CrossRef]
- Liu, Y.; Li, G.; Liu, C.; Tang, Y.; Zhang, S. RSF1 regulates the proliferation and paclitaxel resistance via modulating NF-κB signaling pathway in nasopharyngeal carcinoma. J. Cancer 2017, 8, 354–362. [Google Scholar] [CrossRef][Green Version]
- Kansal, V.; Kinney, B.L.C.; Uppada, S.; Saba, N.F.; Stokes, W.A.; Buchwald, Z.S.; Schmitt, N.C. The expanding role of IAP antagonists for the treatment of head and neck cancer. Cancer Med. 2023, 12, 13958–13965. [Google Scholar] [CrossRef]
- Gomez-Roca, C.; Even, C.; Le Tourneau, C.; Basté, N.; Delord, J.P.; Sarini, J.; Vergez, S.; Temam, S.; Hoffmann, C.; Rochaix, P.; et al. Exploratory window-of-opportunity trial to investigate the tumor pharmacokinetics/pharmacodynamics of the IAP antagonist Debio 1143 in patients with head and neck cancer. Clin. Transl. Sci. 2022, 15, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Sazonova, E.V.; Kopeina, G.S.; Imyanitov, E.N.; Zhivotovsky, B. Platinum drugs and taxanes: Can we overcome resistance? Cell Death Discov. 2021, 7, 155. [Google Scholar] [CrossRef] [PubMed]
- Dogan, E.; Kara, H.G.; Kosova, B.; Cetintas, V.B. Targeting Apoptosis to Overcome Chemotherapy Resistance. In Metastasis; Exon Publications: Brisbane, Australia, 2022; Chapter 12, pp. 163–180. [Google Scholar] [CrossRef]
- Ariffin, A.B.; Forde, P.F.; Jahangeer, S.; Soden, D.M.; Hinchion, J. Releasing pressure in tumors: What do we know so far and where do we go from here? A review. Cancer Res. 2014, 74, 2655–2662. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.; Zhang, Q.; Luo, W. Angiogenesis inhibitors as therapeutic agents in cancer: Challenges and future directions. Eur. J. Pharmacol. 2016, 793, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Hata, K.; Osaki, M.; Dhar, D.K.; Nakayama, K.; Fujiwaki, R.; Ito, H.; Nagasue, N.; Miyazaki, K. Evaluation of the antiangiogenic effect of Taxol in a human epithelial ovarian carcinoma cell line. Cancer Chemother. Pharmacol. 2004, 53, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Loo, W.T.; Fong, J.H.; Cheung, M.N.; Chow, L.W. The efficacy of Paclitaxel on solid tumour analysed by ATP bioluminescence assay and VEGF expression: A translational research study. Biomed. Pharmacother. 2005, 59 (Suppl. 2), S337–S339. [Google Scholar] [CrossRef]
- Heydar, H.; Mansouri, K.; Norooznezhad, M.; Norooznezhad, F.; Mohamadnia, A.; Bahrami, N. Bevacizumab Inhibits Angiogenic Cytokines in Head and Neck Squamous Cell Carcinoma: From Gene to the Protein. Int. J. Hematol. Oncol. Stem Cell Res. 2018, 12, 136–141. [Google Scholar]
- Hoang, T.; Huang, S.; Armstrong, E.; Eickhoff, J.C.; Harari, P.M. Enhancement of radiation response with bevacizumab. J. Exp. Clin. Cancer Res. 2012, 31, 37. [Google Scholar] [CrossRef]
- Argiris, A.; Li, S.; Savvides, P.; Ohr, J.P.; Gilbert, J.; Levine, M.A.; Chakravarti, A.; Haigentz, M., Jr.; Saba, N.F.; Ikpeazu, C.V.; et al. Phase III Randomized Trial of Chemotherapy With or Without Bevacizumab in Patients With Recurrent or Metastatic Head and Neck Cancer. J. Clin. Oncol. 2019, 37, 3266–3274. [Google Scholar] [CrossRef]
- Yao, M.; Galanopoulos, N.; Lavertu, P.; Fu, P.; Gibson, M.; Argiris, A.; Rezaee, R.; Zender, C.; Wasman, J.; Machtay, M.; et al. Phase II study of bevacizumab in combination with docetaxel and radiation in locally advanced squamous cell carcinoma of the head and neck. Head Neck 2015, 37, 1665–1671. [Google Scholar] [CrossRef]
- Salama, J.K.; Haraf, D.J.; Stenson, K.M.; Blair, E.A.; Witt, M.E.; Williams, R.; Kunnavakkam, R.; Cohen, E.E.; Seiwert, T.; Vokes, E.E. A randomized phase II study of 5-fluorouracil, hydroxyurea, and twice-daily radiotherapy compared with bevacizumab plus 5-fluorouracil, hydroxyurea, and twice-daily radiotherapy for intermediate-stage and T4N0-1 head and neck cancers. Ann. Oncol. 2011, 22, 2304–2309. [Google Scholar] [CrossRef] [PubMed]
- Elser, C.; Siu, L.L.; Winquist, E.; Agulnik, M.; Pond, G.R.; Chin, S.F.; Francis, P.; Cheiken, R.; Elting, J.; McNabola, A.; et al. Phase II trial of sorafenib in patients with recurrent or metastatic squamous cell carcinoma of the head and neck or nasopharyngeal carcinoma. J. Clin. Oncol. 2007, 25, 3766–3773. [Google Scholar] [CrossRef] [PubMed]
- Cooney, M.M.; Tserng, K.Y.; Makar, V.; McPeak, R.J.; Ingalls, S.T.; Dowlati, A.; Overmoyer, B.; McCrae, K.; Ksenich, P.; Lavertu, P.; et al. A phase IB clinical and pharmacokinetic study of the angiogenesis inhibitor SU5416 and paclitaxel in recurrent or metastatic carcinoma of the head and neck. Cancer Chemother. Pharmacol. 2005, 55, 295–300. [Google Scholar] [CrossRef]
- Limaye, S.; Riley, S.; Zhao, S.; O’Neill, A.; Posner, M.; Adkins, D.; Jaffa, Z.; Clark, J.; Haddad, R. A randomized phase II study of docetaxel with or without vandetanib in recurrent or metastatic squamous cell carcinoma of head and neck (SCCHN). Oral Oncol. 2013, 49, 835–841. [Google Scholar] [CrossRef]
- Seidel, J.A.; Otsuka, A.; Kabashima, K. Anti-PD-1 and Anti-CTLA-4 Therapies in Cancer: Mechanisms of Action, Efficacy, and Limitations. Front. Oncol. 2018, 8, 86. [Google Scholar] [CrossRef] [PubMed]
- Sakai, A.; Ebisumoto, K.; Iijima, H.; Yamauchi, M.; Teramura, T.; Yamazaki, A.; Watanabe, T.; Inagi, T.; Maki, D.; Okami, K. Chemotherapy following immune checkpoint inhibitors in recurrent or metastatic head and neck squamous cell carcinoma: Clinical effectiveness and influence of inflammatory and nutritional factors. Discov. Oncol. 2023, 14, 158. [Google Scholar] [CrossRef]
- Wanderley, C.W.; Colón, D.F.; Luiz, J.P.M.; Oliveira, F.F.; Viacava, P.R.; Leite, C.A.; Pereira, J.A.; Silva, C.M.; Silva, C.R.; Silva, R.L.; et al. Paclitaxel Reduces Tumor Growth by Reprogramming Tumor-Associated Macrophages to an M1 Profile in a TLR4-Dependent Manner. Cancer Res. 2018, 78, 5891–5900. [Google Scholar] [CrossRef]
- Reinisch, M.; Ataseven, B.; Kümmel, S. Neoadjuvant Dose-Dense and Dose-Intensified Chemotherapy in Breast Cancer—Review of the Literature. Breast Care 2016, 11, 13–20. [Google Scholar] [CrossRef]
- Lyman, G.H.; Barron, R.L.; Natoli, J.L.; Miller, R.M. Systematic review of efficacy of dose-dense versus non-dose-dense chemotherapy in breast cancer, non-Hodgkin lymphoma, and non-small cell lung cancer. Crit. Rev. Oncol. Hematol. 2012, 81, 296–308. [Google Scholar] [CrossRef]
- Fayette, J.; Fontaine-Delaruelle, C.; Ambrun, A.; Daveau, C.; Poupart, M.; Ramade, A.; Zrounba, P.; Neidhardt, E.M.; Péron, J.; Diallo, A.; et al. Neoadjuvant modified TPF (docetaxel, cisplatin, fluorouracil) for patients unfit to standard TPF in locally advanced head and neck squamous cell carcinoma: A study of 48 patients. Oncotarget 2016, 7, 37297–37304. [Google Scholar] [CrossRef]
- Anantharamu, S.; Jacob, L.A.; Dasappa, L.; Babu, M.C.S.; Lokesh, K.N.; Rudresha, A.H.; Lakkavalli Krishnappa, R.; Saldanha, S.C. A prospective comparative study on biweekly docetaxel, cisplatin, 5-fluorouracil, leucovorin (TPFL) versus triweekly TPF as an induction chemotherapy in locally advanced squamous cell carcinoma of head and neck. Ann. Oncol. 2022, 33, S850. [Google Scholar] [CrossRef]
- Guiard, E.; Clatot, F.; Even, C.; Perréard, M.; Abdeddaim, C.; Johnson, A.; Vauléon, E.; Rambeau, A. Impact of previous nivolumab treatment on the response to taxanes in patients with recurrent/metastatic head and neck squamous cell carcinoma. Eur. J. Cancer 2021, 159, 125–132. [Google Scholar] [CrossRef]
- Daste, A.; De-Mones, E.; Cochin, V.; Dupin, C.; Digue, L.; Ravaud, A.; Domblides, C. Progression beyond nivolumab: Stop or repeat? Dramatic responses with salvage chemotherapy. Oral Oncol. 2018, 81, 116–118. [Google Scholar] [CrossRef]
- Sukari, A.; Nagasaka, M.; Abdallah, N. Responses in patients receiving sequential paclitaxel post progression on PD1 inhibitors. Oral Oncol. 2018, 80, 100–102. [Google Scholar] [CrossRef] [PubMed]
- Denaro, N.; Merlano, M.C. Unexpected response with palliative conventional therapy in head and neck squamous cell carcinoma after anti-programmed death-1 progression. Head Neck 2019, 41, E42–E47. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| A. Locally Advanced HNSCC | ||||||||
|---|---|---|---|---|---|---|---|---|
| Patient Number | Major Adverse Event (AE) | |||||||
| Trial Design | Arms | Combined Agents | AE | N (%) | Grade | Reference | ||
| Open-label, Single-center | 1 | Toripalimab + Paclitaxel/Cisplatin | 20 | Baldness | 20 (100) | 1–2 | [42] | |
| Randomized, Open-label, Multi-center | 2 | RT ± Docetaxel | 356 | Odynophagia | 177 (98.9) | 3–5 | [43] | |
| Randomized, Open-label, Multi-center | 2 | TPF, cisplatin + RT ± Cetuximab + RT | 519 | Mucositis | 161 (79.7) | 2–3 | [44] | |
| Randomized, Single-center | 2 | Cisplatin/Carboplatin, Docetaxel + Erlotinib vs. placebo | 100 | Fatigue | 40 (77) | 1–2 | [45] | |
| Open-label, Multi-center | 1 | Panitumumab (Pb) + Paclitaxel, followed Bio-RT + Pb | 51 | Skin toxicity | 29 (56.9) | 3–4 | [46] | |
| Randomized, Open-label, Multi-center | 2 | TPF or TPC, followed RT + Cetuximab | 100 | GI disorders | 23 (23) | 3–5 | [47] | |
| Non-randomized, Single-center | 2 | Nanoparticle albumin-bound Paclitaxel, RT/Cisplatin vs. RT/Cetuximab | 79 | Fatigue | 44 (55.7) | 1–2 | [48] | |
| B. R/M HNSCC | ||||||||
| Patient Number | Major Adverse Event (AE) | |||||||
| Trial Design | Arms | Combined Agents | AE | N (%) | Grade | Reference | ||
| Open-label, Multi-center | 1 | Pembrolizumab + Paclitaxel + carboplatin | 92 | Neutropenia | 52 (57) | 1–3 | [39] | |
| Open-label, Multi-center | 1 | durvalumab combined with weekly paclitaxel carboplatin | 64 | no disclosure | [49] | |||
| Open-label, Single-center | 1 | Pembrolizumab plus docetaxel | 22 | Neutropenia | 3 (13.6) | 3–5 | [41] | |
| Open-label, Multi-center | 1 | Nab-paclitaxel+ cetuximab+carboplatin | 74 | Neutropenia | 25 (34) | 3–5 | [50] | |
| Agent | NCT Identifier | Phase | Study Design | Population |
|---|---|---|---|---|
| Paclitaxel | ||||
| NCT04338399 | III | Buparlisib and Paclitaxel vs. Paclitaxel | R/M HNSCC post PD-1 or PD-L1 inhibitor | |
| NCT05420948 | II | 1.Pembrolizumab alone | Circulating tumor DNA Response-Adaptive Pulsed Chemotherapy in R/M HNSCC | |
| 2.Pembrolizumab+Paclitaxel+Carboplatin | ||||
| NCT02270814 | II | Nab-Paclitaxel, Platinum, Cetuximab | Incurable HNSCC (R/M + unresectable HNSCC) | |
| NCT04282109 | II | Nivolumab/Paclitaxel | Cisplatin refractory R/M HNSCC | |
| NCT04278092 | II | Cetuximab + Paclitaxel | R/M HNSCC post first line Pembrolizumab | |
| NCT04831320 | II | Nivolumab/Bab-Paclitaxel | R/M HNSCC post PD-1 or PD-L1 inhibitor | |
| NCT03440437 | I/II | FS118 + Paclitaxel (expansion cohort) | R/M HNSCC post PD-1 or PD-L1 inhibitor | |
| NCT05283226 | II | Oral NRC-2694-A + Paclitaxel | R/M HNSCC post PD-1 or PD-L1 inhibitor | |
| NCT04858269 | II | Pembrolizumab + weekly CT (Paclitaxel + Carboplatin) | R/M HNSCC first line | |
| NCT05758389 | II | Tislelizumab, Paclitaxel (albumin-bound type), Cisplatin, 5-FU | Neoadjuvant CT for newly diagnosed resectable advanced HNSCC | |
| NCT04826679 | II | Camrelizumab, Nab-Paclitaxel, Cisplatin | Neoadjuvant CT for newly diagnosed resectable advanced HNSCC | |
| NCT05459129 | I/II | Atezolizumab + Tiragolumab + Carboplatin + Paclitaxel | Neoadjuvant CT for newly diagnosed resectable advanced HNSCC | |
| Docetaxel | ||||
| NCT05057247 | II | Duvelisib Plus Docetaxel | R/M HNSCC post PD-1 inhibitors | |
| NCT05252429 | II | Pembrolizumab/Docetaxel | R/M HNSCC first line | |
| NCT05376553 | II | Cemiplimab + Docetaxel/Cisplatin | Induction setting for LAHNSCC | |
| NCT04722523 | II | Cemiplimab/Cetuximab/Docetaxel/platinum | Resectable LAHNSCC Neoadjuvant | |
| NCT05726370 | II | Pembrolizumab/Platinum/Docetaxel | Resectable R/M HNSCC first line Neoadjuvant |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsieh, C.-Y.; Lin, C.-C.; Chang, W.-C. Taxanes in the Treatment of Head and Neck Squamous Cell Carcinoma. Biomedicines 2023, 11, 2887. https://doi.org/10.3390/biomedicines11112887
Hsieh C-Y, Lin C-C, Chang W-C. Taxanes in the Treatment of Head and Neck Squamous Cell Carcinoma. Biomedicines. 2023; 11(11):2887. https://doi.org/10.3390/biomedicines11112887
Chicago/Turabian StyleHsieh, Ching-Yun, Ching-Chan Lin, and Wei-Chao Chang. 2023. "Taxanes in the Treatment of Head and Neck Squamous Cell Carcinoma" Biomedicines 11, no. 11: 2887. https://doi.org/10.3390/biomedicines11112887
APA StyleHsieh, C.-Y., Lin, C.-C., & Chang, W.-C. (2023). Taxanes in the Treatment of Head and Neck Squamous Cell Carcinoma. Biomedicines, 11(11), 2887. https://doi.org/10.3390/biomedicines11112887