






Correlation between Thyroid Responses and Inflammatory Cytokines in Critically Ill COVID-19 Patients

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Outcomes
2.3. Measurement of Thyroid Hormones
2.4. Measurement of Cytokines
2.5. Statistical Analysis
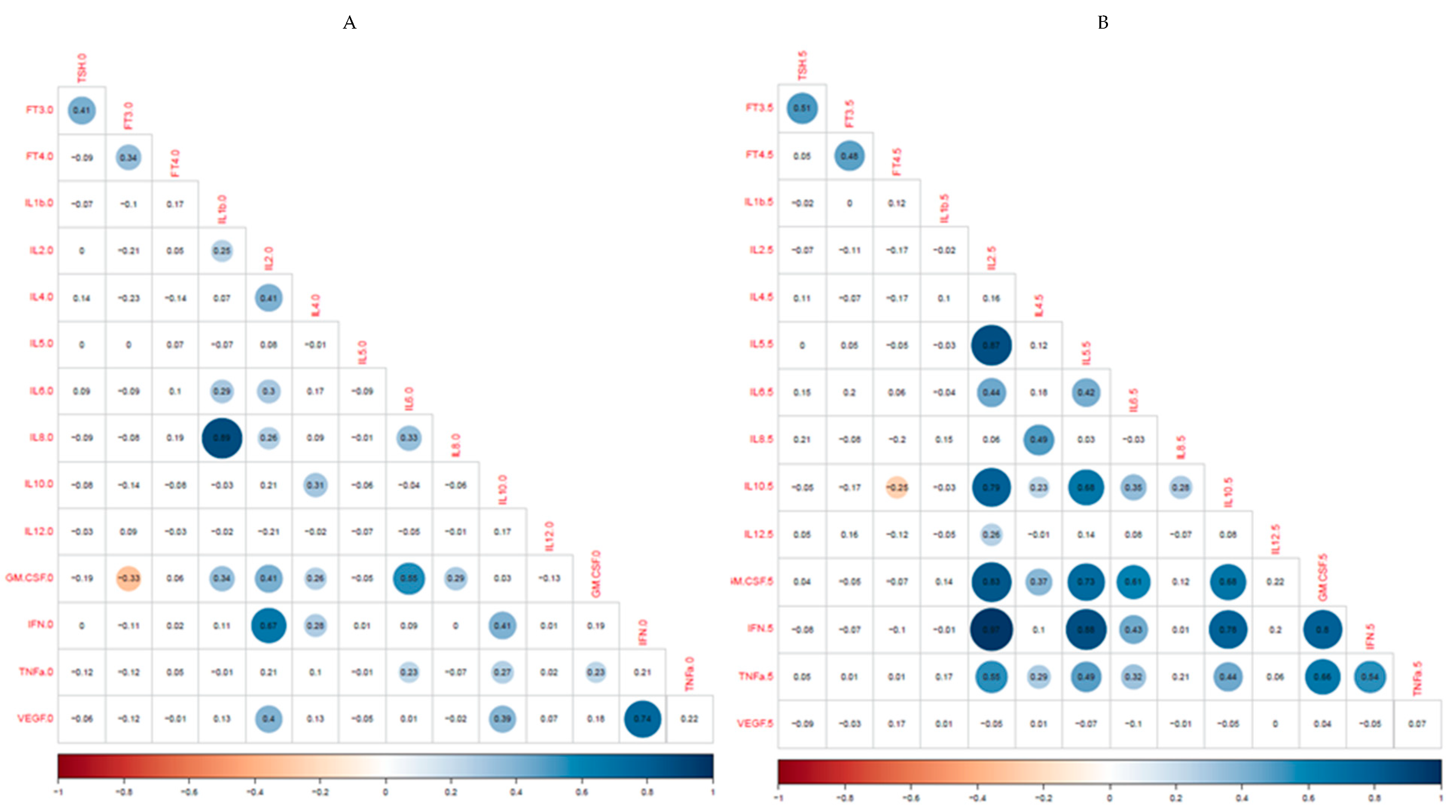
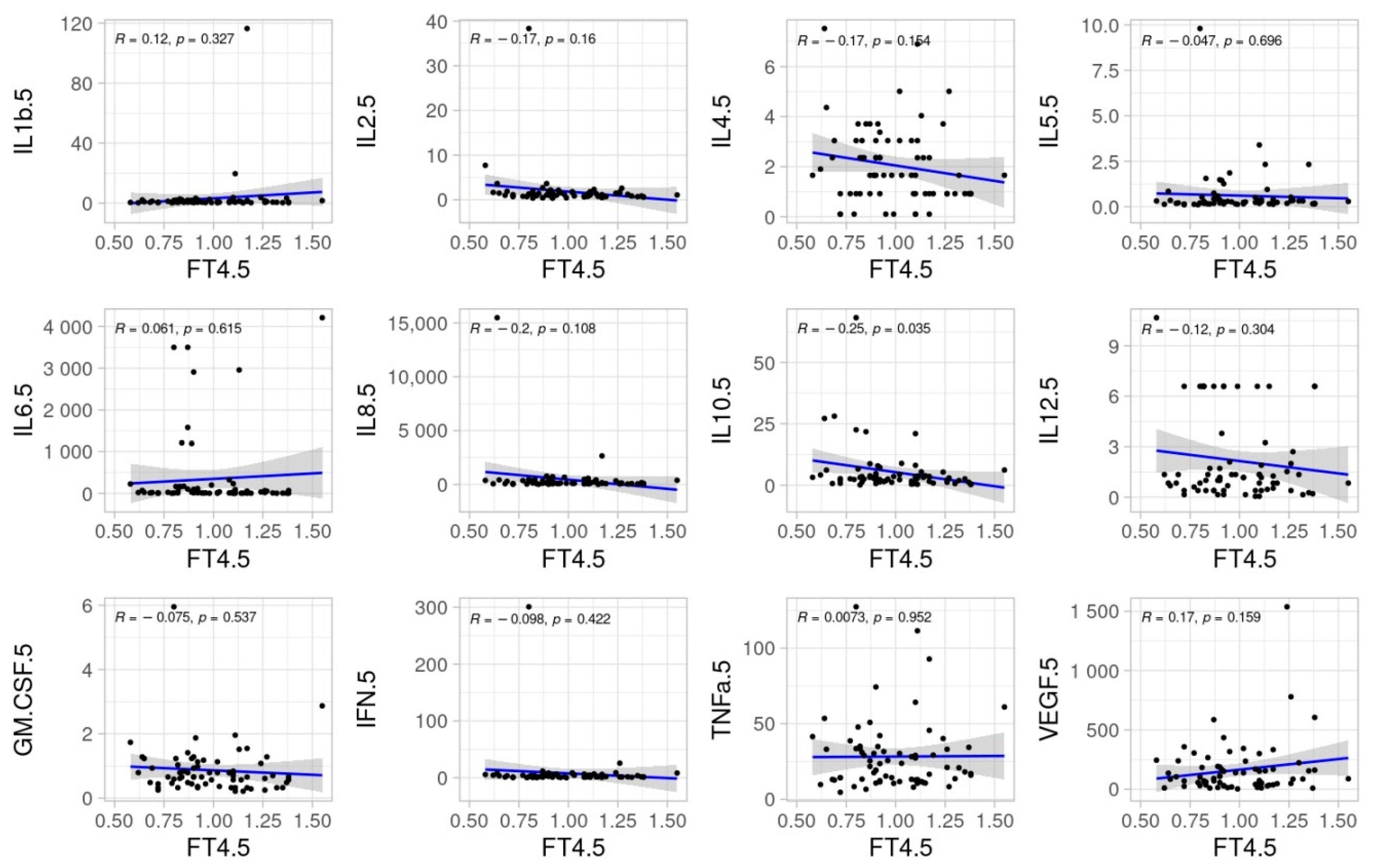
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roberts, C.M.; Levi, M.; McKee, M.; Schilling, R.; Lim, W.S.; Grocott, M.P.W. COVID-19: A complex multisystem disorder. Br. J. Anaesth. 2020, 125, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Mir, T.; Almas, T.; Kaur, J.; Faisaluddin, M.; Song, D.; Ullah, W.; Mamtani, S.; Rauf, H.; Yadav, S.; Latchana, S.; et al. Coronavirus disease 2019 (COVID-19): Multisystem review of pathophysiology. Ann. Med. Surg. 2021, 69, 102745. [Google Scholar] [CrossRef] [PubMed]
- Inaba, H.; Aizawa, T. Coronavirus Disease 2019 and the Thyroid - Progress and Perspectives. Front. Endocrinol. 2021, 12, 708333. [Google Scholar] [CrossRef] [PubMed]
- Mourouzis, I.; Apostolaki, V.; Trikas, A.; Kokkinos, L.; Alexandrou, N.; Avdikou, M.; Giannoulopoulou, M.; Vassi, A.; Tseti, I.; Pantos, C. The Potential of Thyroid Hormone Therapy in Severe COVID-19: Rationale and Preliminary Evidence. Int. J. Environ. Re.S Public Health 2022, 19, 8063. [Google Scholar] [CrossRef] [PubMed]
- Bellastella, G.; Cirillo, P.; Carbone, C.; Scappaticcio, L.; Maio, A.; Botta, G.; Tomasuolo, M.; Longo, M.; Pontillo, A.; Bellastella, A.; et al. Neuroimmunoendocrinology of SARS-CoV 2 Infection. Biomedicines 2022, 10, 2855. [Google Scholar] [CrossRef] [PubMed]
- Li, M.Y.; Li, L.; Zhang, Y.; Wang, X.S. Expression of the SARS-CoV-2 cell receptor gene ACE2 in a wide variety of human tissues. Infect. Dis. Poverty 2020, 9, 45. [Google Scholar] [CrossRef] [PubMed]
- Zou, R.; Wu, C.; Zhang, S.; Wang, G.; Zhang, Q.; Yu, B.; Wu, Y.; Dong, H.; Wu, G.; Wu, S.; et al. Euthyroid Sick Syndrome in Patients With COVID-19. Front. Endocrinol. 2020, 11, 566439. [Google Scholar] [CrossRef] [PubMed]
- Gao, W.; Guo, W.; Guo, Y.; Shi, M.; Dong, G.; Wang, G.; Ge, Q.; Zhu, J.; Zhouet, X. Thyroid hormone concentrations in severely or critically ill patients with COVID-19. J. Endocrinol. Investig. 2021, 44, 1031–1040. [Google Scholar] [CrossRef] [PubMed]
- Ballesteros Vizoso, M.A.; Castilla, A.F.; Barceló, A.; Raurich, J.M.; Argente Del Castillo, P.; Morell-García, D.; Velasco, J.; Pérez-Bárcena, J.; Llompart-Pou, J.A. Thyroid Disfunction in Critically Ill COVID-19 Patients. Relationship with In-Hospital Mortality. J. Clin. Med. 2021, 10, 5057. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Li, X.; Dai, Y.; Zhang, J. The Association Between COVID-19 and Thyroxine Levels: A Meta-Analysis. Front. Endocrinol. 2022, 12, 779692. [Google Scholar] [CrossRef] [PubMed]
- McElvaney, O.J.; McEvoy, N.L.; McElvaney, O.F.; Carroll, T.P.; Murphy, M.P.; Dunlea, D.M.; Ní Choileáin, O.; Clarke, J.; O’Connor, E.; Hogan, G.; et al. Characterization of the Inflammatory Response to Severe COVID-19 Illness. Am. J. Respir. Crit. Care Med. 2020, 202, 812–821. [Google Scholar] [CrossRef] [PubMed]
- Del Valle, D.M.; Kim-Schulze, S.; Huang, H.H.; Beckmann, N.D.; Nirenberg, S.; Wang, B.; Lavin, Y.; Swartz, T.H.; Madduri, D.; Stock, A.; et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nat. Med. 2020, 26, 1636–1643. [Google Scholar] [CrossRef] [PubMed]
- Dhar, S.K.; Vishnupriyan, K.; Damodar, S.; Gujar, S.; Das, M. IL-6 and IL-10 as predictors of disease severity in COVID-19 patients: Results from meta-analysis and regression. Heliyon 2021, 7, e06155. [Google Scholar] [CrossRef] [PubMed]
- Clausen, C.L.; Rasmussen, Å.K.; Johannsen, T.H.; Hilsted, L.M.; Skakkebæk, N.E.; Szecsi, P.B.; Pedersen, L.; Benfield, T.; Juul, A. Thyroid function in COVID-19 and the association with cytokine levels and mortality. Endocr. Connect. 2021, 10, 1234–1242. [Google Scholar] [CrossRef] [PubMed]
- Lania, A.; Sandri, M.T.; Cellini, M.; Mirani, M.; Lavezzi, E.; Mazziotti, G. Thyrotoxicosis in patients with COVID-19: The THYRCOV study. Eur. J. Endocrinol. 2020, 183, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Lei, J.; Li, Z. Thyroid function changes and COVID-19 severity: Egg or chicken? Endocrine 2022, 78, 436–440. [Google Scholar] [CrossRef] [PubMed]
- Świątkowska-Stodulska, R.; Berlińska, A.; Puchalska-Reglińska, E. Thyroid Function, Inflammatory Response, and Glucocorticoids in COVID-19. Front. Endocrinol. 2022, 13, 939842. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Zhang, H.; Dauphars, D.J.; He, Y.W. A Potential Role of Interleukin 10 in COVID-19 Pathogenesis. Trends Immunol. 2021, 42, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Liu, L.; Zhang, D.; Xu, J.; Dai, H.; Tang, N.; Su, X.; Cao, B. SARS-CoV-2 and viral sepsis: Observations and hypotheses. Lancet 2020, 395, 1517–1520. [Google Scholar] [CrossRef] [PubMed]
- Pinski, A.N.; Steffen, T.L.; Zulu, M.Z.; George, S.L.; Dickson, A.; Tifrea, D.; Maroney, K.J.; Tedeschi, N.; Zhang, Y.; Scheuermann, R.H.; et al. Corticosteroid treatment in COVID-19 modulates host inflammatory responses and transcriptional signatures of immune dysregulation. J. Leukoc. Biol. 2021, 110, 1225–1239. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N: 78 | |
|---|---|
| Female, n (%) | 23 (29.5%) |
| Age (years) | 62.1 (12.4) |
| SAPS II | 40.6 (14.2) |
| APACHE II | 18.0 (8.0) |
| Admission SOFA | 5.4 (2.5) |
| Comorbidities, n (%) | |
| Hypertension | 43 (55.1%) |
| Diabetes mellitus | 20 (25.6%) |
| Dyslipidemia | 37 (47.4%) |
| COPD | 10 (12.8%) |
| Chronic kidney disease | 9 (11.5%) |
| Chronic cardiac disease | 12 (15.4%) |
| Malignancy (active) | 9 (11.5%) |
| Prior treatment, n (%) | |
| Beta-blockers | 13 (16.6%) |
| ACE inhibitors | 17 (21.8%) |
| ARBs | 19 (24.3%) |
| Statins | 30 (38.4%) |
| Treatment in the ICU |
| Steroids: 78 (100%) |
| Remdesivir: 11 (14.1%) |
| Tocilizumab: 15 (9.2%) |
| Prophylactic heparin: 43 (55.1%) |
| Intermediate dose heparin: 28 (35.9%) |
| Full anticoagulation: 7 (8.9%) |
| Mechanical ventilation: 67 (85.9%) |
| V-V ECMO: 5 (6.4%) |
| Outcomes |
| ICU LOS (days): 31.1 (31.5) |
| In-hospital LOS (days): 46.1 (38.7) |
| In-hospital Mortality: 23 (29.5%) |
| Variable | OR (95% CI) | p Value |
|---|---|---|
| Age | 1.11 (1.02–1.23) | 0.034 |
| SOFA | 1.49 (0.98–2.46) | 0.081 |
| PaO2/FiO2 | 0.96 (0.91–0.99) | 0.018 |
| IL-10 (day 5) | 1.23 (1.05–1.63) | 0.040 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Figueras Castilla, A.; Ballesteros Vizoso, M.A.; Iglesias Coma, A.; Barceló, A.; Barea-Mendoza, J.A.; Argente del Castillo, P.; Guardiola, B.; Pérez-Bárcena, J.; Llompart-Pou, J.A. Correlation between Thyroid Responses and Inflammatory Cytokines in Critically Ill COVID-19 Patients. Biomedicines 2023, 11, 26. https://doi.org/10.3390/biomedicines11010026
Figueras Castilla A, Ballesteros Vizoso MA, Iglesias Coma A, Barceló A, Barea-Mendoza JA, Argente del Castillo P, Guardiola B, Pérez-Bárcena J, Llompart-Pou JA. Correlation between Thyroid Responses and Inflammatory Cytokines in Critically Ill COVID-19 Patients. Biomedicines. 2023; 11(1):26. https://doi.org/10.3390/biomedicines11010026
Chicago/Turabian StyleFigueras Castilla, Albert, María A. Ballesteros Vizoso, Amanda Iglesias Coma, Antonia Barceló, Jesús A. Barea-Mendoza, Paula Argente del Castillo, Begoña Guardiola, Jon Pérez-Bárcena, and Juan A. Llompart-Pou. 2023. "Correlation between Thyroid Responses and Inflammatory Cytokines in Critically Ill COVID-19 Patients" Biomedicines 11, no. 1: 26. https://doi.org/10.3390/biomedicines11010026
APA StyleFigueras Castilla, A., Ballesteros Vizoso, M. A., Iglesias Coma, A., Barceló, A., Barea-Mendoza, J. A., Argente del Castillo, P., Guardiola, B., Pérez-Bárcena, J., & Llompart-Pou, J. A. (2023). Correlation between Thyroid Responses and Inflammatory Cytokines in Critically Ill COVID-19 Patients. Biomedicines, 11(1), 26. https://doi.org/10.3390/biomedicines11010026