

The Need for Glaucoma Management in Glaucoma Patients with Concurrent Obstructive Sleep Apnea: A Population-Based Cohort Study

 , , , ,
, , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
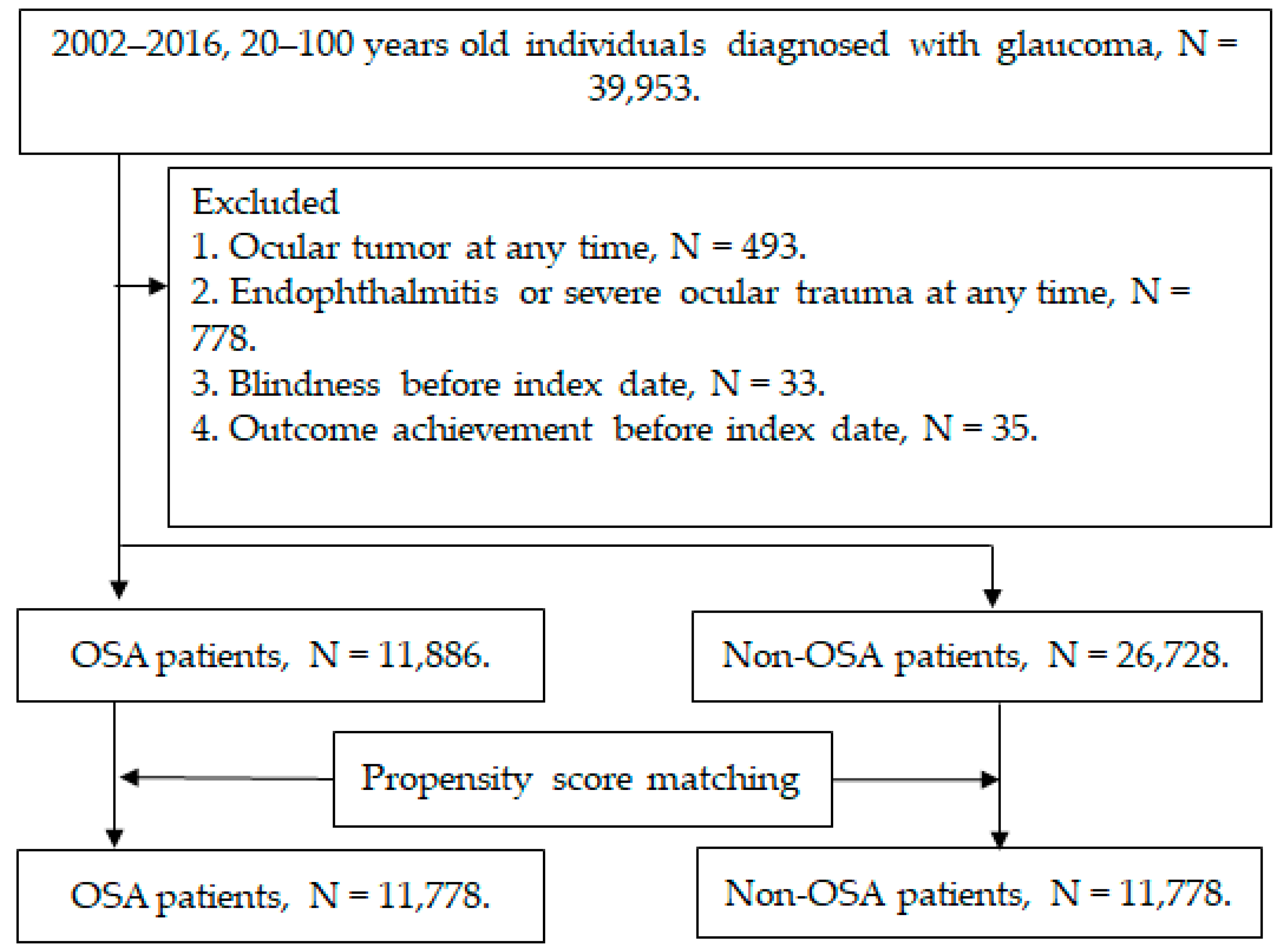
2.2. Patient Selection
2.3. Primary Outcome Measurement
2.4. Demographic Variables and Comorbidities
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weinreb, R.N.; Aung, T.; Medeiros, F.A. The pathophysiology and treatment of glaucoma: A review. JAMA 2014, 311, 1901–1911. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Lindsley, K.; Rouse, B.; Hong, H.; Shi, Q.; Friedman, D.S.; Wormald, R.; Dickersin, K. Comparative Effectiveness of First-Line Medications for Primary Open-Angle Glaucoma: A Systematic Review and Network Meta-analysis. Ophthalmology 2016, 123, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Soh, Z.; Yu, M.; Betzler, B.K.; Majithia, S.; Thakur, S.; Tham, Y.C.; Wong, T.Y.; Aung, T.; Friedman, D.S.; Cheng, C.Y. The Global Extent of Undetected Glaucoma in Adults: A Systematic Review and Meta-analysis. Ophthalmology 2021, 128, 1393–1404. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.D.; Khawaja, A.P.; Weizer, J.S. Glaucoma in Adults-Screening, Diagnosis, and Management: A Review. JAMA 2021, 325, 164–174. [Google Scholar] [CrossRef]
- Santos, M.; Hofmann, R.J. Ocular Manifestations of Obstructive Sleep Apnea. J. Clin. Sleep Med. 2017, 13, 1345–1348. [Google Scholar] [CrossRef]
- Quigley, H.A. Glaucoma. Lancet 2011, 377, 1367–1377. [Google Scholar] [CrossRef]
- McMonnies, C.W. Glaucoma history and risk factors. J. Optom. 2017, 10, 71–78. [Google Scholar] [CrossRef]
- Worley, A.; Grimmer-Somers, K. Risk factors for glaucoma: What do they really mean? Aust. J. Prim. Health 2011, 17, 233–239. [Google Scholar] [CrossRef]
- Martínez-Blanco, A.M.; Cantor, E.J.; Valencia-Peña, C. Prevalence and risk factors for primary angle-closure disease spectrum: The Colombian glaucoma study. Eur. J. Ophthalmol. 2021, 32, 942–950. [Google Scholar] [CrossRef]
- Resch, H.; Garhofer, G.; Fuchsjäger-Mayrl, G.; Hommer, A.; Schmetterer, L. Endothelial dysfunction in glaucoma. Acta Ophthalmol. 2009, 87, 4–12. [Google Scholar] [CrossRef]
- Salman, L.A.; Shulman, R.; Cohen, J.B. Obstructive Sleep Apnea, Hypertension, and Cardiovascular Risk: Epidemiology, Pathophysiology, and Management. Curr. Cardiol. Rep. 2020, 22, 6. [Google Scholar] [CrossRef]
- Patel, S.R. Obstructive Sleep Apnea. Ann. Intern. Med. 2019, 171, ITC81–ITC96. [Google Scholar] [CrossRef] [PubMed]
- Veasey, S.C.; Rosen, I.M. Obstructive Sleep Apnea in Adults. N. Engl. J. Med. 2019, 380, 1442–1449. [Google Scholar] [CrossRef]
- Lee, J.J.; Sundar, K.M. Evaluation and Management of Adults with Obstructive Sleep Apnea Syndrome. Lung 2021, 199, 87–101. [Google Scholar] [CrossRef] [PubMed]
- Cesareo, M.; Giannini, C.; Martucci, A.; Di Marino, M.; Pocobelli, G.; Aiello, F.; Mancino, R.; Nucci, C. Links between obstructive sleep apnea and glaucoma neurodegeneration. Prog. Brain Res. 2020, 257, 19–36. [Google Scholar] [CrossRef] [PubMed]
- Bahr, K.; Bopp, M.; Kewader, W.; Dootz, H.; Döge, J.; Huppertz, T.; Simon, P.; Prokosch-Willing, V.; Matthias, C.; Gouveris, H. Obstructive sleep apnea as a risk factor for primary open angle glaucoma and ocular hypertension in a monocentric pilot study. Respir. Res. 2020, 21, 258. [Google Scholar] [CrossRef]
- Jassim, A.H.; Fan, Y.; Pappenhagen, N.; Nsiah, N.Y.; Inman, D.M. Oxidative Stress and Hypoxia Modify Mitochondrial Homeostasis During Glaucoma. Antioxid. Redox Signal. 2021, 35, 1341–1357. [Google Scholar] [CrossRef]
- Düger, M.; Seyhan, E.C.; Günlüoğlu, M.Z.; Bolatkale, M.; Özgül, M.A.; Turan, D.; Uğur, E.; Ülfer, G. Does ischemia-modified albumin level predict severity of obstructive sleep apnea? Sleep Breath. 2021, 25, 65–73. [Google Scholar] [CrossRef]
- Labarca, G.; Gower, J.; Lamperti, L.; Dreyse, J.; Jorquera, J. Chronic intermittent hypoxia in obstructive sleep apnea: A narrative review from pathophysiological pathways to a precision clinical approach. Sleep Breath. 2020, 24, 751–760. [Google Scholar] [CrossRef]
- Mojon, D.S.; Hess, C.W.; Goldblum, D.; Fleischhauer, J.; Koerner, F.; Bassetti, C.; Mathis, J. High prevalence of glaucoma in patients with sleep apnea syndrome. Ophthalmology 1999, 106, 1009–1012. [Google Scholar] [CrossRef]
- Walsh, J.T.; Montplaisir, J. Familial glaucoma with sleep apnoea: A new syndrome? Thorax 1982, 37, 845–849. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.Y.; Su, W.W.; Liu, C.H.; Chen, H.S.; Wu, S.C.; Chang, S.H.L.; Chen, K.J.; Wu, W.C.; Chen, N.H.; Li, H.Y.; et al. Correlation between structural progression in glaucoma and obstructive sleep apnea. Eye 2019, 33, 1459–1465. [Google Scholar] [CrossRef] [PubMed]
- Goyal, M.; Tiwari, U.S.; Jaseja, H. Pathophysiology of the comorbidity of glaucoma with obstructive sleep apnea: A postulation. Eur. J. Ophthalmol. 2021, 31, 2776–2780. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.C.; Hu, C.C.; Ho, J.D.; Chiu, H.W.; Lin, H.C. Obstructive sleep apnea and increased risk of glaucoma: A population-based matched-cohort study. Ophthalmology 2013, 120, 1559–1564. [Google Scholar] [CrossRef] [PubMed]
- Jordan, A.S.; McSharry, D.G.; Malhotra, A. Adult obstructive sleep apnoea. Lancet 2014, 383, 736–747. [Google Scholar] [CrossRef]
- Alotaibi, M.; Alsubaie, M.; Alharthi, A.; Alnabri, A.; Bormah, A.; Alafif, K.; Alhibshi, N. The Risk of Obstructive Sleep Apnea in Open-Angle Glaucoma Patients. Cureus 2021, 13, e18699. [Google Scholar] [CrossRef]
- Bagabas, N.; Ghazali, W.; Mukhtar, M.; AlQassas, I.; Merdad, R.; Maniyar, A.; Almarzouki, N.; Afreen, H.; Badeeb, O.; Wali, S. Prevalence of Glaucoma in Patients with Obstructive Sleep Apnea. J. Epidemiol. Glob. Health 2019, 9, 198–203. [Google Scholar] [CrossRef]
- Wu, A.; Khawaja, A.P.; Pasquale, L.R.; Stein, J.D. A review of systemic medications that may modulate the risk of glaucoma. Eye 2020, 34, 12–28. [Google Scholar] [CrossRef]
- Roberti, G.; Oddone, F.; Agnifili, L.; Katsanos, A.; Michelessi, M.; Mastropasqua, L.; Quaranta, L.; Riva, I.; Tanga, L.; Manni, G. Steroid-induced glaucoma: Epidemiology, pathophysiology, and clinical management. Surv. Ophthalmol. 2020, 65, 458–472. [Google Scholar] [CrossRef]
- Conlon, R.; Saheb, H.; Ahmed, I.I.K. Glaucoma treatment trends: A review. Can. J. Ophthalmol. 2017, 52, 114–124. [Google Scholar] [CrossRef]
- Quaranta, L.; Riva, I.; Gerardi, C.; Oddone, F.; Floriani, I.; Konstas, A.G. Quality of Life in Glaucoma: A Review of the Literature. Adv. Ther. 2016, 33, 959–981. [Google Scholar] [CrossRef] [PubMed]
- West, S.D.; Turnbull, C. Obstructive sleep apnoea. Eye 2018, 32, 889–903. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; He, X.; Li, Q.; Zhang, Y.; Hu, J.; Zong, R.; Zhuang, J.; Quantock, A.J.; Gao, Y.; Li, W.; et al. Obstructive Sleep Apnea Affects Lacrimal Gland Function. Investig. Ophthalmol. Vis. Sci. 2022, 63, 3. [Google Scholar] [CrossRef] [PubMed]
- Fietze, I.; Laharnar, N.; Obst, A.; Ewert, R.; Felix, S.B.; Garcia, C.; Gläser, S.; Glos, M.; Schmidt, C.O.; Stubbe, B.; et al. Prevalence and association analysis of obstructive sleep apnea with gender and age differences—Results of SHIP-Trend. J. Sleep Res. 2019, 28, e12770. [Google Scholar] [CrossRef] [PubMed]
- Bonsignore, M.R.; Saaresranta, T.; Riha, R.L. Sex differences in obstructive sleep apnoea. Eur. Respir. Rev. 2019, 28, 190030. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.W.; Friedman, M.; Lin, H.C.; Chang, H.W.; Wilson, M.; Lin, M.C. Normal tension glaucoma in patients with obstructive sleep apnea/hypopnea syndrome. J. Glaucoma 2011, 20, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Bilgin, G. Normal-tension glaucoma and obstructive sleep apnea syndrome: A prospective study. BMC Ophthalmol. 2014, 14, 27. [Google Scholar] [CrossRef]
- Sergi, M.; Salerno, D.E.; Rizzi, M.; Blini, M.; Andreoli, A.; Messenio, D.; Pecis, M.; Bertoni, G. Prevalence of normal tension glaucoma in obstructive sleep apnea syndrome patients. J. Glaucoma 2007, 16, 42–46. [Google Scholar] [CrossRef]
- Arnaud, C.; Bochaton, T.; Pépin, J.L.; Belaidi, E. Obstructive sleep apnoea and cardiovascular consequences: Pathophysiological mechanisms. Arch. Cardiovasc. Dis. 2020, 113, 350–358. [Google Scholar] [CrossRef]
- Gaballa, S.A.; Kompella, U.B.; Elgarhy, O.; Alqahtani, A.M.; Pierscionek, B.; Alany, R.G.; Abdelkader, H. Corticosteroids in ophthalmology: Drug delivery innovations, pharmacology, clinical applications, and future perspectives. Drug Deliv. Transl. Res. 2021, 11, 866–893. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Non-OSA N = 11,778 | OSA N = 11,778 | ASD |
|---|---|---|---|
| Year of index | 0.0000 | ||
| 2001–2006 | 2820 (23.94%) | 2781 (23.61%) | |
| 2007–2011 | 3858 (32.76%) | 3917 (33.26%) | |
| 2012–2017 | 5100 (43.30%) | 5080 (43.13%) | |
| Age at index | 0.0000 | ||
| <40 | 612 (5.20%) | 637 (5.41%) | |
| 40–49 | 1172 (9.95%) | 1160 (9.85%) | |
| 50–59 | 2418 (20.53%) | 2435 (20.67%) | |
| 60–69 | 3348 (28.43%) | 3310 (28.10%) | |
| 70–79 | 2952 (25.06%) | 2923 (24.82%) | |
| ≧80 | 1276 (10.83%) | 1313 (11.15%) | |
| Sex | 0.0007 | ||
| Male | 4545 (38.59%) | 4549 (38.62%) | |
| Female | 7233 (61.41%) | 7229 (61.38%) | |
| Urbanization | 0.0376 | ||
| Urban | 7450 (63.25%) | 7371 (62.58%) | |
| Sub-urban | 3207 (27.23%) | 3274 (27.80%) | |
| Rural | 1121 (9.52%) | 1133 (9.62%) | |
| Education level | 0.0238 | ||
| Elementary school or below | 5783 (49.10%) | 5894 (50.04%) | |
| Junior high school | 1694 (14.38%) | 1703 (14.46%) | |
| Senior high school | 3268 (27.75%) | 3177 (26.97%) | |
| University or above | 1033 (8.77%) | 1004 (8.52%) | |
| Co-morbidities | |||
| Hypertension | 5613 (47.66%) | 5578 (47.36%) | 0.0060 |
| DM | 3083 (26.18%) | 3084 (26.18%) | 0.0002 |
| Ischemic heart diseases | 1385 (11.76%) | 1440 (12.23%) | 0.0144 |
| Hemodialysis | 151 (1.28%) | 154 (1.31%) | 0.0023 |
| Cerebrovascular disease | 1173 (9.96%) | 1240 (10.53%) | 0.0188 |
| Uveitis | 402 (3.41%) | 433 (3.68%) | 0.0142 |
| Cataract | 5302 (45.02%) | 5320 (45.17%) | 0.0031 |
| Refractive error | 393 (3.34%) | 487 (4.13%) | 0.0421 |
| Steroid use | |||
| Prednisolone | 1844 (15.66%) | 2343 (19.89%) | 0.1110 |
| Methylprednisolone | 563 (4.78%) | 777 (6.60%) | 0.0785 |
| Hydrocortisone | 264 (2.24%) | 343 (2.91%) | 0.0423 |
| Triamcinolone | 642 (5.45%) | 879 (7.46%) | 0.0819 |
| Dexamethasone | 1468 (12.46%) | 1665 (14.14%) | 0.0493 |
| OSA-related surgeries | 2537 (21.54%) |
| Event | Non-OSA n = 11,778 | OSA n = 11,778 |
|---|---|---|
| Laser trabeculoplasty | ||
| Follow up person months | 928,868 | 907,452 |
| New case | 69 | 67 |
| Incidence rate #(95% CI) | 0.740 (0.590–0.940) | 0.740 (0.580–0.940) |
| Crude relative risk (95% CI) | Reference | 0.979 (0.700–1.371) |
| AHR (95% CI) | Reference | 0.978 (0.698–1.371) |
| Trabeculectomy and tube shunt surgery | ||
| Follow up person months | 917,540 | 899,247 |
| New case | 239 | 182 |
| Incidence rate #(95% CI) | 2.600 (2.290–2.960) | 2.020 (1.750–2.340) |
| Crude relative risk (95% CI) | Reference | 0.774 (0.655–0.914) |
| AHR (95% CI) | Reference | 0.855 (0.720–1.016) |
| Cyclodestructive procedure | ||
| Follow up person months | 930,462 | 908,072 |
| New case | 64 | 60 |
| Incidence rate#(95% CI) | 0.690 (0.540–0.880) | 0.660 (0.510–0.850) |
| Crude Relative risk (95% CI) | Reference | 0.944 (0.664–1.343) |
| AHR (95% CI) | Reference | 0.927 (0.651–1.320) |
| Eyeball removal | ||
| Follow up person months | 933754 | 910816 |
| New case | 6 | 8 |
| Incidence rate #(95% CI) | 0.060 (0.030–0.140) | 0.090 (0.040–0.180) |
| Crude Relative risk (95% CI) | Reference | 1.343 (0.466–3.872) |
| AHR (95% CI) | Reference | 1.284 (0.442–3.725) |
| Parameters | Laser Trabeculoplasty | Trabeculectomy and Tube Shunt Surgery | Cyclodestructive Procedure |
|---|---|---|---|
| Age | |||
| Age < 60 | 0.899 (0.559–1.446) | 0.966 (0.751–1.242) | 0.836 (0.494–1.414) |
| Age ≥ 60 | 1.043 (0.720–1.511) | 0.774 (0.611–0.998)* | 0.856 (0.588–1.247) |
| Sex | |||
| Male | 1.070 (0.696–1.644) | 0.833 (0.650–1.068) | 0.721 (0.461–1.129) |
| Female | 0.924 (0.622–1.374) | 0.883 (0.694–1.125) | 1.032 (0.671–1.588) |
| Glaucoma subtype | |||
| OAG | 1.066 (0.596–1.907) | 1.114 (0.749–1.656) | 0.970 (0.464–2.029) |
| NTG | 7.095 (0.665–9.719) | 1.180 (0.262–5.322) | NA |
| ACG | 0.925 (0.532–1.609) | 0.731 (0.514–1.038) | 0.697 (0.381–1.274) |
| OSA years | |||
| OSA < 1 year | 1.489 (0.826–2.685) | 1.322 (0.937–1.864) | 0.502 (0.186–1.359) |
| OSA 1–2 years | 1.413 (0.765–2.610) | 0.977 (0.653–1.461) | 0.659 (0.270–1.609) |
| OSA > 2 years | 0.832 (0.590–1.173) | 0.752 (0.614–1.022) | 0.940 (0.677–1.305) |
| OSA-related surgeries | |||
| With any surgery | 1.047 (0.766–1.431) | 0.824 (0.674–1.008) | 0.829 (0.753–1.147) |
| Without surgery | 0.724 (0.547–1.357) | 0.883 (0.729–1.070) | 0.899 (0.666–1.260) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.-Y.; Chien, H.-W.; Huang, J.-Y.; Yen, C.-H.; Chen, H.-C.; Hwang, Y.-S.; Chang, C.-K.; Yang, S.-F. The Need for Glaucoma Management in Glaucoma Patients with Concurrent Obstructive Sleep Apnea: A Population-Based Cohort Study. Biomedicines 2023, 11, 187. https://doi.org/10.3390/biomedicines11010187
Lee C-Y, Chien H-W, Huang J-Y, Yen C-H, Chen H-C, Hwang Y-S, Chang C-K, Yang S-F. The Need for Glaucoma Management in Glaucoma Patients with Concurrent Obstructive Sleep Apnea: A Population-Based Cohort Study. Biomedicines. 2023; 11(1):187. https://doi.org/10.3390/biomedicines11010187
Chicago/Turabian StyleLee, Chia-Yi, Hsiang-Wen Chien, Jing-Yang Huang, Chieh-Hung Yen, Hung-Chi Chen, Yih-Shiou Hwang, Chao-Kai Chang, and Shun-Fa Yang. 2023. "The Need for Glaucoma Management in Glaucoma Patients with Concurrent Obstructive Sleep Apnea: A Population-Based Cohort Study" Biomedicines 11, no. 1: 187. https://doi.org/10.3390/biomedicines11010187
APA StyleLee, C.-Y., Chien, H.-W., Huang, J.-Y., Yen, C.-H., Chen, H.-C., Hwang, Y.-S., Chang, C.-K., & Yang, S.-F. (2023). The Need for Glaucoma Management in Glaucoma Patients with Concurrent Obstructive Sleep Apnea: A Population-Based Cohort Study. Biomedicines, 11(1), 187. https://doi.org/10.3390/biomedicines11010187