
Intestinal Ischemia: Unusual but Fearsome Complication of COVID-19 Infection

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Case 1
3.2. Case 2
3.3. Case 3
3.4. Case 4
3.5. Case 5
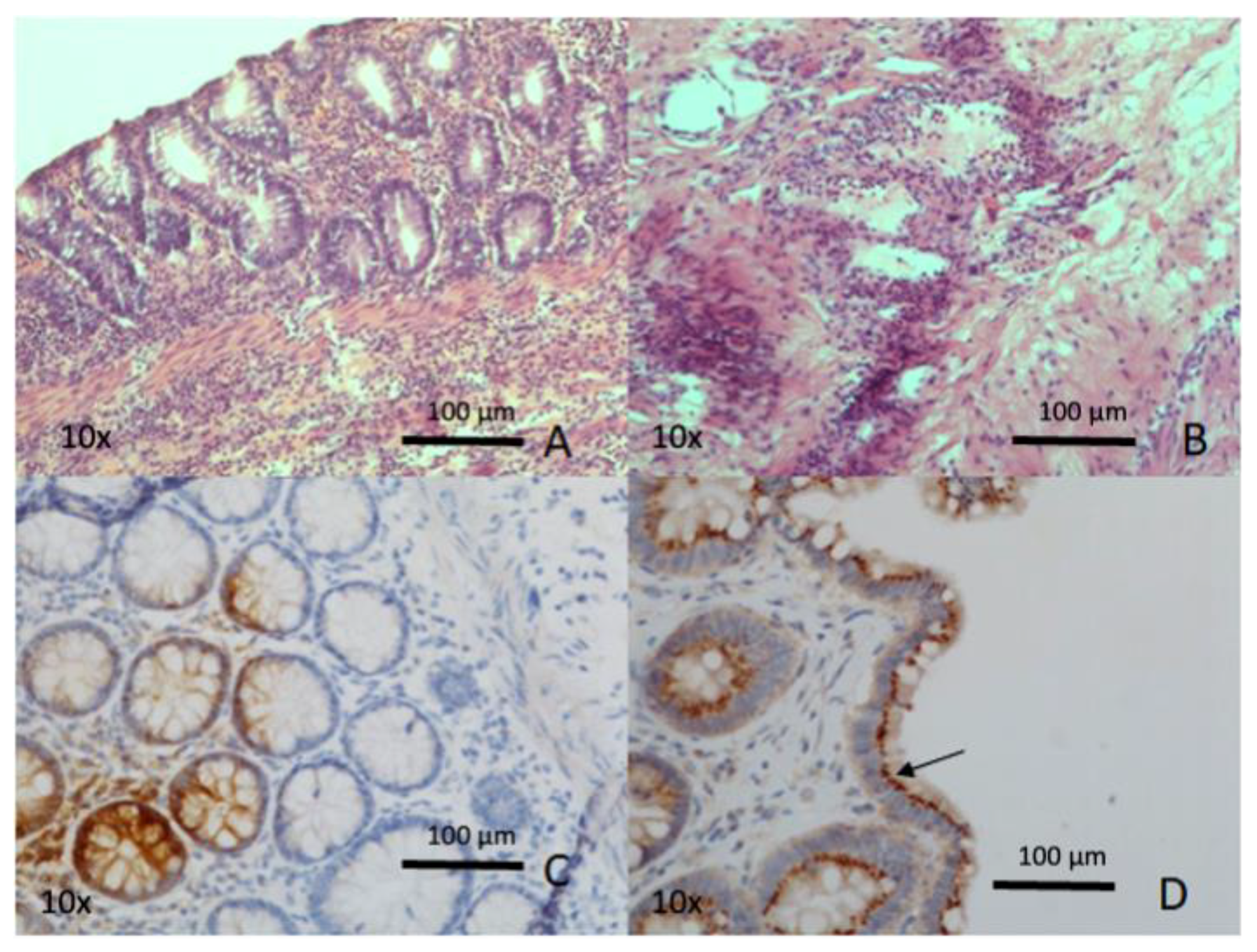
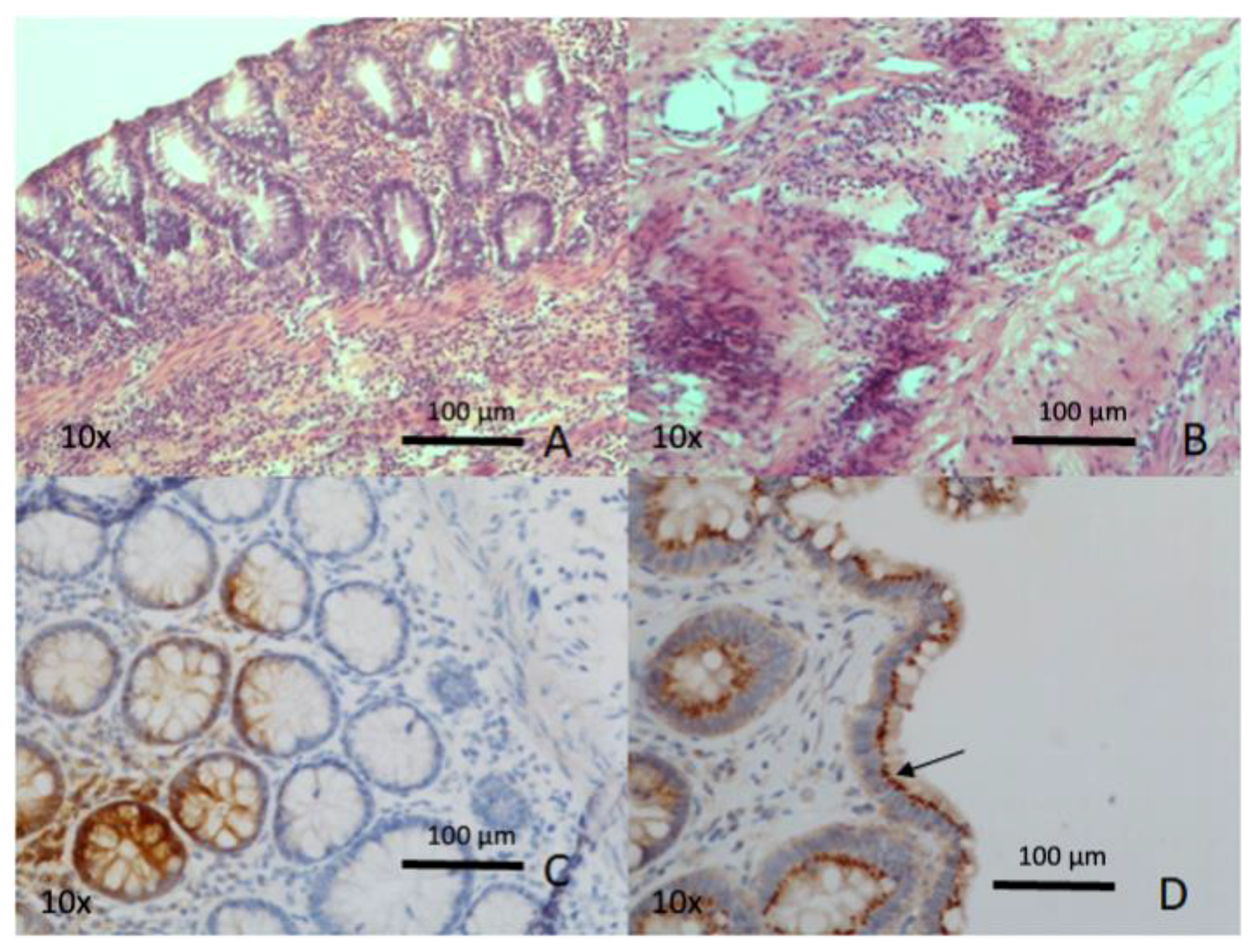
3.6. Immunohistochemical and Molecular SARS-CoV-2 Detection in Paraffin-Embedded Tissue
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cao, Y.; Cai, K.; Xiong, L. Coronavirus disease 2019: A new severe acute respiratory syndrome from Wuhan in China. Acta Virol. 2020, 64, 245–250. [Google Scholar] [CrossRef]
- Ignat, M.; Philouze, G.; Aussenac-Belle, L.; Faucher, V.; Collange, O.; Mutter, D.; Pessaux, P. Small bowel ischemia and SARS-CoV-2 infection: An underdiagnosed distinct clinical entity. Surgery 2020, 168, 14–16. [Google Scholar] [CrossRef]
- Pan, L.; Mu, M.; Yang, P.; Sun, Y.; Wang, R.; Yan, J.; Li, P.; Hu, B.; Wang, J.; Hu, C.; et al. Clinical Characteristics of COVID-19 Patients With Digestive Symptoms in Hubei, China: A Descriptive, Cross-Sectional, Multicenter Study. Am. J. Gastroenterol. 2020, 115, 766–773. [Google Scholar] [CrossRef] [PubMed]
- Kaliszewski, K.; Diakowska, D.; Nowak, Ł.; Tokarczyk, U.; Sroczyński, M.; Sępek, M.; Dudek, A.; Sutkowska-Stępień, K.; Kiliś-Pstrusińska, K.; Matera-Witkiewicz, A.; et al. Assessment of Gastrointestinal Symptoms and Dyspnea in Patients Hospitalized due to COVID-19: Contribution to Clinical Course and Mortality. J. Clin. Med. 2022, 11, 1821. [Google Scholar] [CrossRef] [PubMed]
- Mao, R.; Qiu, Y.; He, J.-S.; Tan, J.-Y.; Li, X.-H.; Liang, J.; Shen, J.; Zhu, L.-R.; Chen, Y.; Iacucci, M.; et al. Manifestations and prognosis of gastrointestinal and liver involvement in patients with COVID-19: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2020, 5, 667–678. [Google Scholar] [CrossRef]
- Li, W.; Moore, M.J.; Vasilieva, N.; Sui, J.; Wong, S.K.; Berne, M.A.; Somasundaran, M.; Sullivan, J.L.; Luzuriaga, K.; Greenough, T.C.; et al. Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature 2003, 426, 450–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lukassen, S.; Chua, R.L.; Trefzer, T.; Kahn, N.C.; Schneider, M.A.; Muley, T.; Winter, H.; Meister, M.; Veith, C.; Boots, A.W.; et al. SARS-CoV-2 receptor ACE2 and TMPRSS2 are primarily expressed in bronchial transient secretory cells. EMBO J. 2020, 39, e105114. [Google Scholar] [CrossRef]
- Ashraf, U.M.; Abokor, A.A.; Edwards, J.M.; Waigi, E.W.; Royfman, R.S.; Hasan, S.A.-M.; Smedlund, K.B.; Hardy, A.M.G.; Chakravarti, R.; Koch, L.G. SARS-CoV-2, ACE2 expression, and systemic organ invasion. Physiol. Genom. 2021, 53, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Cholankeril, G.; Podboy, A.; Aivaliotis, V.I.; Tarlow, B.; Pham, E.A.; Spencer, S.P.; Kim, D.; Hsing, A.; Ahmed, A. High prevalence of concurrent gastrointestinal manifestations in patients with Severe Acute Respiratory Syndrome Coronavirus-2: Early experience from California. Gastroenterology 2020, 159, 775–777. [Google Scholar] [CrossRef] [PubMed]
- Bhayana, R.; Som, A.; Li, M.D.; Carey, D.E.; Anderson, M.A.; Blake, M.A.; Catalano, O.; Gee, M.S.; Hahn, P.F.; Harisinghani, M.; et al. Abdominal Imaging Findings in COVID-19: Preliminary Observations. Radiology 2020, 297, E207–E215. [Google Scholar] [CrossRef]
- Bryce, C.; Grimes, Z.; Pujadas, E.; Ahuja, S.; Beasley, M.B.; Albrecht, R.; Hernandez, T.; Stock, A.; Zhao, Z.; AlRasheed, M.R.; et al. Pathophysiology of SARS-CoV-2: The Mount Sinai COVID-19 autopsy experience. Mod. Pathol. 2021, 34, 1456–1467. [Google Scholar] [CrossRef] [PubMed]
- Xiao, F.; Tang, M.; Zheng, X.; Liu, Y.; Li, X.; Shan, H. Evidence for Gastrointestinal Infection of SARS-CoV-2. Gastroenterology 2020, 158, 1831–1833.e3. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Qu, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Alberca, G.G.F. Coronavirus disease-2019 and the intestinal tract: An overview. World J. Gastroenterol. 2021, 27, 1255–1266. [Google Scholar] [CrossRef]
- Saeed, U.; Sellevoll, H.B.; Young, V.S.; Sandbaek, G.; Glomsaker, T.; Mala, T. COVID-19 may present with acute abdominal pain. Br. J. Surg. 2020, 107, e186–e187. [Google Scholar] [CrossRef]
- Lakshmanan, S.; Toubia, N. Pneumatosis Intestinalis in COVID-19. Clin. Gastroenterol. Hepatol. 2021, 19, e99. [Google Scholar] [CrossRef]
- Cheung, S.; Quiwa, J.C.; Pillai, A.; Onwu, C.; Tharayil, Z.J.; Gupta, R. Superior mesenteric artery thrombosis and acute intestinal ischemia. Am. J. Case Rep. 2020, 21, e925753. [Google Scholar] [CrossRef]
- Panigada, M.; Bottino, N.; Tagliabue, P.; Grasselli, G.; Novembrino, C.; Chantarangkul, V.; Pesenti, A.; Peyvandi, F.; Tripodi, A. Hypercoagulability of COVID-19 patients in intensive care unit: A report of thromboelastography findings and other parameters of hemostasis. J. Thromb. Haemost. 2020, 18, 1738–1742. [Google Scholar] [CrossRef]
- Fransvea, P.; Costa, G.; Pepe, G.; La Greca, A.; Magalini, S.; Puccioni, C.; d’Agostino, L.; Altieri, G.; Borello, A.; Cozza, V.; et al. Acute intestinal ischemia in patients with COVID-19: Single-centre experience and literature review. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 1414–1429. [Google Scholar]
- Serban, D.; Tribus, L.C.; Vancea, G.; Stoian, A.P.; Dascalu, A.M.; Suceveanu, A.I.; Tanasescu, C.; Costea, A.C.; Tudosie, M.S.; Tudor, C.; et al. Acute Mesenteric Ischemia in COVID-19 Patients. J. Clin. Med. 2021, 11, 200. [Google Scholar] [CrossRef]
- Hassan, W.; Ramadan, H.K. COVID-19 and pneumatosis intestinalis: An early sign of intestinal ischemia. Dig. Liver Dis. 2021, 53, 289–290. [Google Scholar] [CrossRef] [PubMed]
- Horvat, N.; Pinto, P.V.A.; Araujo-Filho, J.D.A.B.; Santos, J.M.M.M.; Dias, A.B.; Miranda, J.A.; de Oliveira, C.V.; Barbosa, C.S.; Morais, T.C.; Assuncao-Jr, A.N.; et al. Abdominal gastrointestinal imaging findings on computed tomography in patients with COVID-19 and correlation with clinical outcomes. Eur. J. Radiol. Open 2021, 8, 100326. [Google Scholar] [CrossRef]
- Boraschi, P.; Giugliano, L.; Mercogliano, G.; Donati, F.; Romano, S.; Neri, E. Abdominal and gastrointestinalmanifestations in COVID 19 patients: Isimaginguseful? World J. Gastroenterol. 2021, 27, 4143–4159. [Google Scholar] [CrossRef]
- Norsa, L.; Bonaffini, P.A.; Indriolo, A.; Valle, C.; Sonzogni, A.; Sironi, S. Poor Outcome of Intestinal Ischemic Manifestations of COVID-19. Gastroenterology 2020, 159, 1595–1597.e1. [Google Scholar] [CrossRef]
- Farina, D.; Rondi, P.; Botturi, E.; Renzulli, M.; Borghesi, A.; Guelfi, D.; Ravanelli, M. Gastrointestinal: Bowel ischemia in asuspected coronavirus disease (COVID-19) patient. J. Gastroenterol. Hepatol. 2021, 36, 41. [Google Scholar] [CrossRef]
- Kielty, J.; Duggan, W.P.; O’Dwyer, M. Extensive pneumatosis intestinalis and portal venous gas mimicking mesenteric ischaemia in a patient with SARS-CoV-2. Ann. R. Coll. Surg. Engl. 2020, 102, e145–e147. [Google Scholar] [CrossRef]
- Aiello, P.; Johnson, S.; Ramos Mercado, A.; Hussein, S. Pneumatosis intestinalis in a patient with COVID-19. BMJ Case Rep. 2020, 13, e237564. [Google Scholar] [CrossRef]
- Meini, S.; Zini, C.; Passaleva, M.T.; Frullini, A.; Fusco, F.; Carpi, R.; Piani, F. Pneumatosisintestinalis in COVID-19. BMJ Open Gastroenterol. 2020, 7, e000434. [Google Scholar] [CrossRef]
- Zamboni, P.; Bortolotti, D.; Occhionorelli, S.; Traina, L.; Neri, L.M.; Rizzo, R.; Gafà, R.; Passaro, A. Bowel ischemia as onset of COVID-19 in otherwise asymptomatic patients with persistently negative swab. J. Intern. Med. 2021, 291, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Norsa, L.; Valle, C.; Morotti, D.; Bonaffini, P.A.; Indriolo, A.; Sonzogni, A. Intestinal ischemia in the COVID-19 era. Dig. Liver Dis. 2020, 52, 1090–1091. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Jiang, X.; Zhang, Z.; Huang, S.; Zhang, Z.; Fang, Z.; Gu, Z.; Gao, L.; Shi, H.; Mai, L.; et al. Gastrointestinal symptoms of 95 cases with SARS-CoV-2 infection. Gut 2020, 69, 997–1001. [Google Scholar] [CrossRef] [PubMed]
- Beyerstedt, S.; Casaro, E.B.; Rangel, É.B. COVID-19: Angiotensin-converting enzyme 2 (ACE2) expression and tissue susceptibility to SARS-CoV-2 infection. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 905–919. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| CASE 1 | CASE 2 | CASE 3 | CASE 4 | CASE 5 | |
| Age (years) | 74 | 69 | 77 | 75 | 72 |
| Gender (male/female) | M | M | M | M | M |
| Comorbidities | Arterial hypertension, ischemic heart disease in treatment with ASA, HCV+ | Arterial hypertension, previous subdural hematoma | Arterial hypertension, smoking, type 2DM, COPD, chronic ischemic heart disease, previous pulmonary embolism, and ischemic stroke | Double acute myocardial ischemia treated with double endovascular stenting, atrial fibrillation under oral anticoagulation therapy, and gastric ulcer | Arterial hypertension, post-ischemic dilated heart disease, COPD permanent atrial fibrillation, dyslipidemia |
| Previous abdominal surgery | NO | NO | YES (Hartmann’s resection for sigmoid diverticular perforation) | YES (Appendectomy) | NO |
| COVID-19 respiratory infection (yes/not) | YES | YES | YES | YES | YES |
| Clinical presentation | Acute abdominal distention | Diffuse severe abdominal pain | Acute abdominal pain with peritonitis | Diffuse acute abdominal pain | Hemoptysis |
| CT findings | Initial sign of pneumatosis of the cecum | Pneumoperitoneum with “enlargement” of the distal portion of the duodenum | Diffuse pneumoperitoneum | Small, covered perforation at the jejunum-ileal passage, with pneumatosis of the mesentery | Peritoneal fluid, initial pneumatosis of the mesenteric fan and of the duodenal-jejunal flexure wall |
| CASE 1 | CASE 2 | CASE 3 | CASE 4 | CASE 5 | |
|---|---|---|---|---|---|
| Surgery | Laparotomic ileocecal resection with temporary abdominal closure (NPWT) Second look: terminal ileostomy, colonic mucous fistula, and definitive abdominal wall closure | Laparotomic jejunal resection of perforated diverticulum and anastomosis | Laparotomic right hemicolectomy with terminal ileostomy and mucous fistula | Laparotomic resection of perforated jejunal loop at about 30 cm from Treitz’s level and anastomosis | Laparotomic suture of duodenal ulcer, multiple jejunal resections and packing Second look: hemostasis of retroperitoneal bleeding, abdominal packing, and skin closure III look: gastroentero-anastomosis, cholecystectomy with placement of transcystic biliary drain, intestinal patch repair of duodenal fistula, and abdominal wall closure. Peritoneal toilet, suture of the dehiscence of the patch at Treitz’s level, and Foley catheter duodenostomy |
| Complications | Respiratory complications, tracheostomy | NO | NO | NO | Septic shock |
| Mortality | NO | NO | NO | NO | YES |
| Histology | Mucosal ischemic necrosis with fibrin thrombi of small vessel and pneumatosis | Mucosal edema with fibrin thrombi of small vessel and pneumatosis | Mucosal erosion and microhemorrage with fibrin thrombi of small vessel and pneumatosis | Mucosal edema and microhemorrage with fibrin thrombi of small vessel | Mucosal widespread ischemic necrosis and ulceration with fibrin thrombi of small vessel |
| PCR per SARS-CoV-2 (specimen) | negative | negative | positive | negative | negative |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strambi, S.; Proietti, A.; Galatioto, C.; Coccolini, F.; Cremonini, C.; Musetti, S.; Basolo, F.; Chiarugi, M.; Tartaglia, D. Intestinal Ischemia: Unusual but Fearsome Complication of COVID-19 Infection. Biomedicines 2022, 10, 1010. https://doi.org/10.3390/biomedicines10051010
Strambi S, Proietti A, Galatioto C, Coccolini F, Cremonini C, Musetti S, Basolo F, Chiarugi M, Tartaglia D. Intestinal Ischemia: Unusual but Fearsome Complication of COVID-19 Infection. Biomedicines. 2022; 10(5):1010. https://doi.org/10.3390/biomedicines10051010
Chicago/Turabian StyleStrambi, Silvia, Agnese Proietti, Christian Galatioto, Federico Coccolini, Camilla Cremonini, Serena Musetti, Fulvio Basolo, Massimo Chiarugi, and Dario Tartaglia. 2022. "Intestinal Ischemia: Unusual but Fearsome Complication of COVID-19 Infection" Biomedicines 10, no. 5: 1010. https://doi.org/10.3390/biomedicines10051010
APA StyleStrambi, S., Proietti, A., Galatioto, C., Coccolini, F., Cremonini, C., Musetti, S., Basolo, F., Chiarugi, M., & Tartaglia, D. (2022). Intestinal Ischemia: Unusual but Fearsome Complication of COVID-19 Infection. Biomedicines, 10(5), 1010. https://doi.org/10.3390/biomedicines10051010