
A Prediction Model for Tumor Recurrence in Stage II–III Colorectal Cancer Patients: From a Machine Learning Model to Genomic Profiling

 ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population and Histopathology
2.2. Data Collection
2.3. ML Models and Nomogram
2.4. Tumor Sequencing with a Targeted Gene Panel
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics and Histopathological Features of Patients with and without Cancer Recurrence
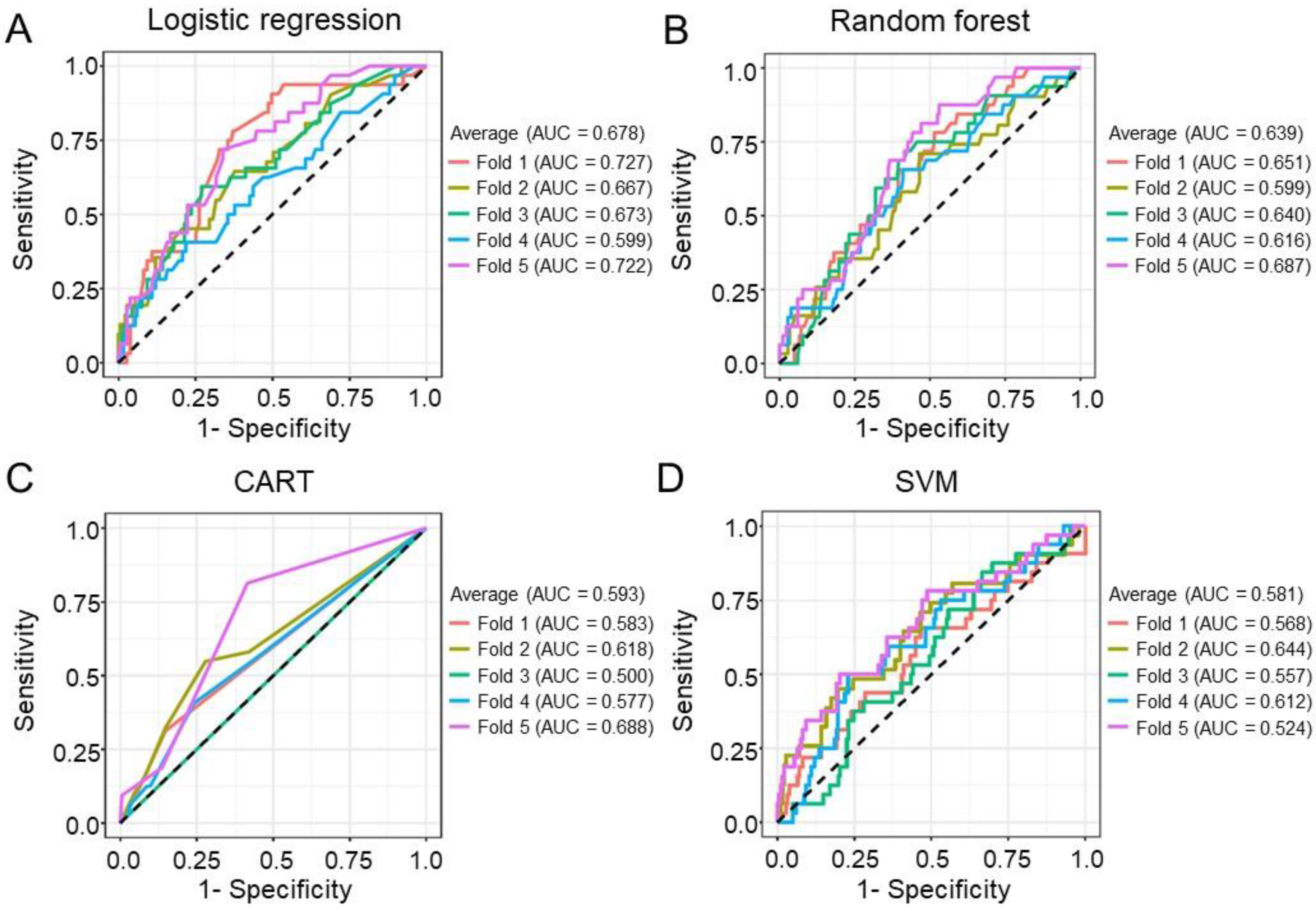
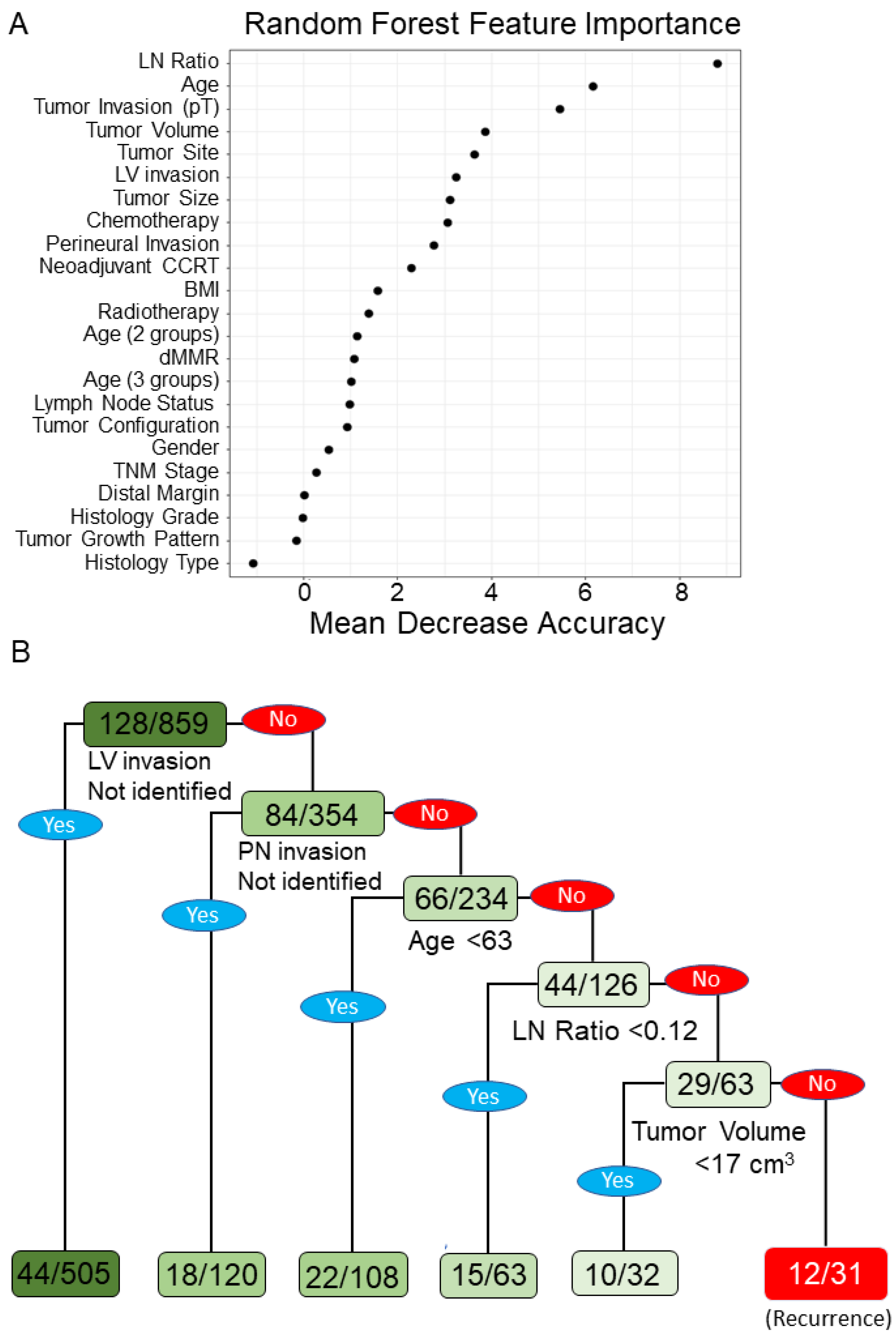
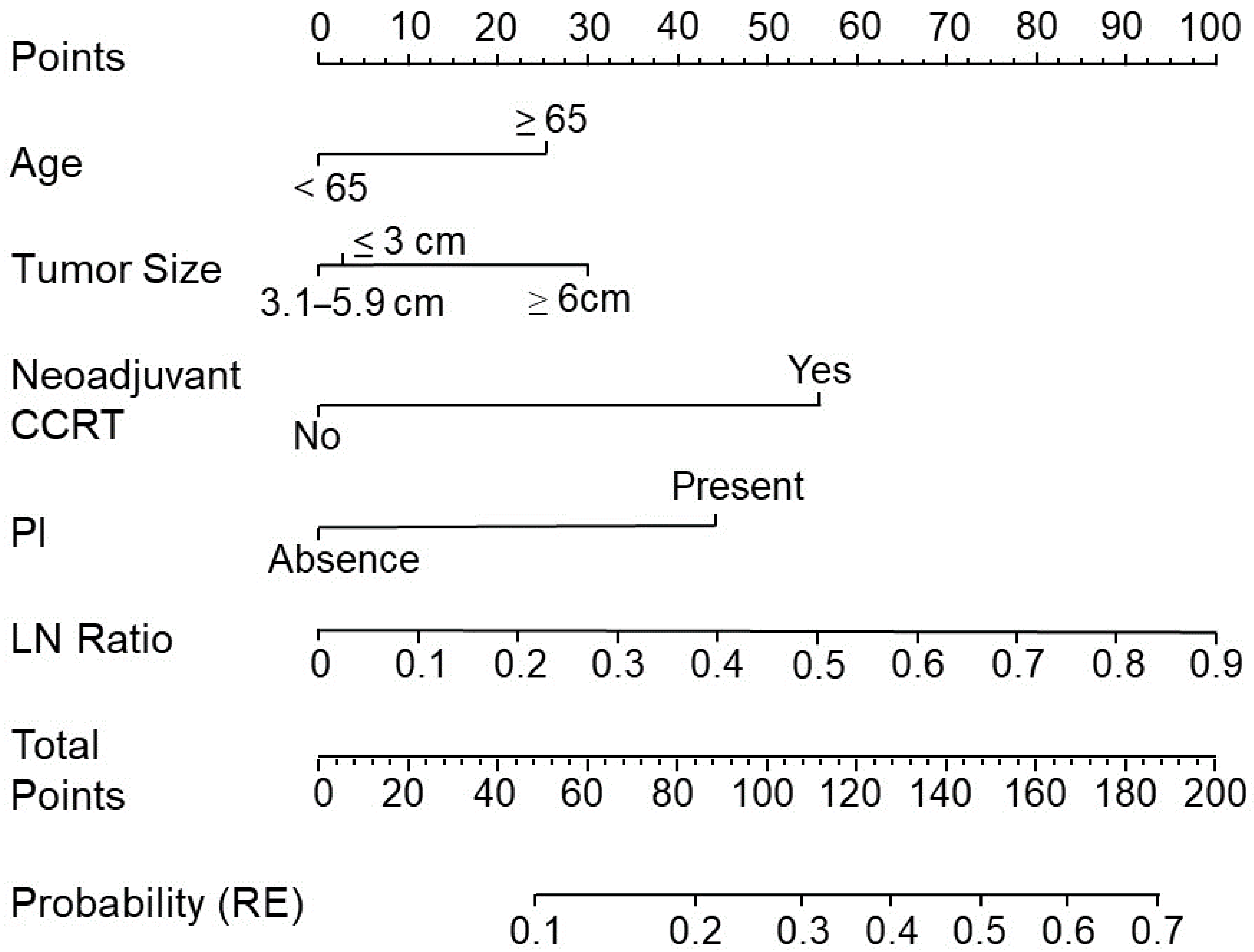
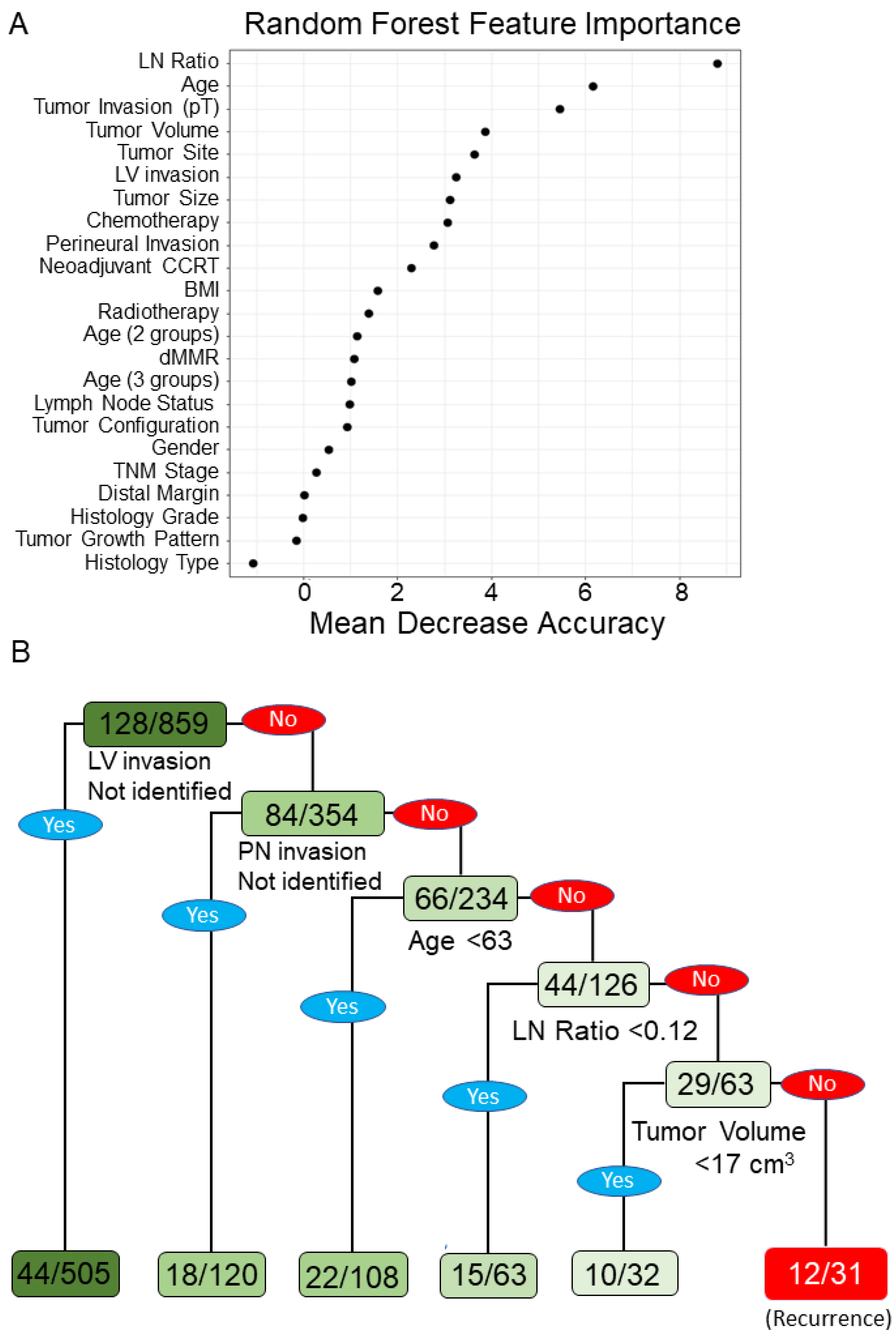
3.2. ML Model Performance for Assessing CRC Recurrence and Predictive Nomogram
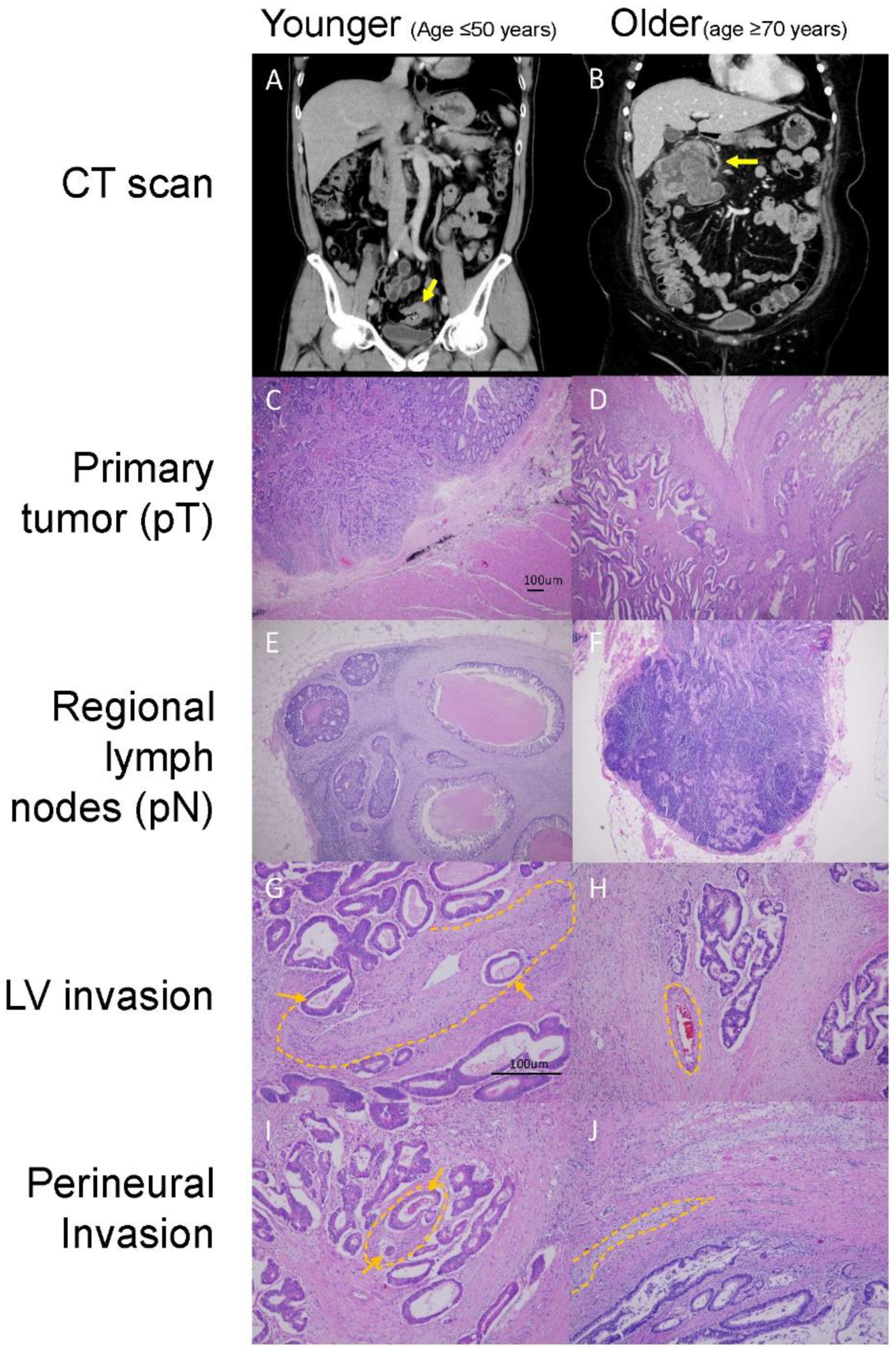
3.3. Different Clinicopathological Features between Younger and Older Patients with CRC
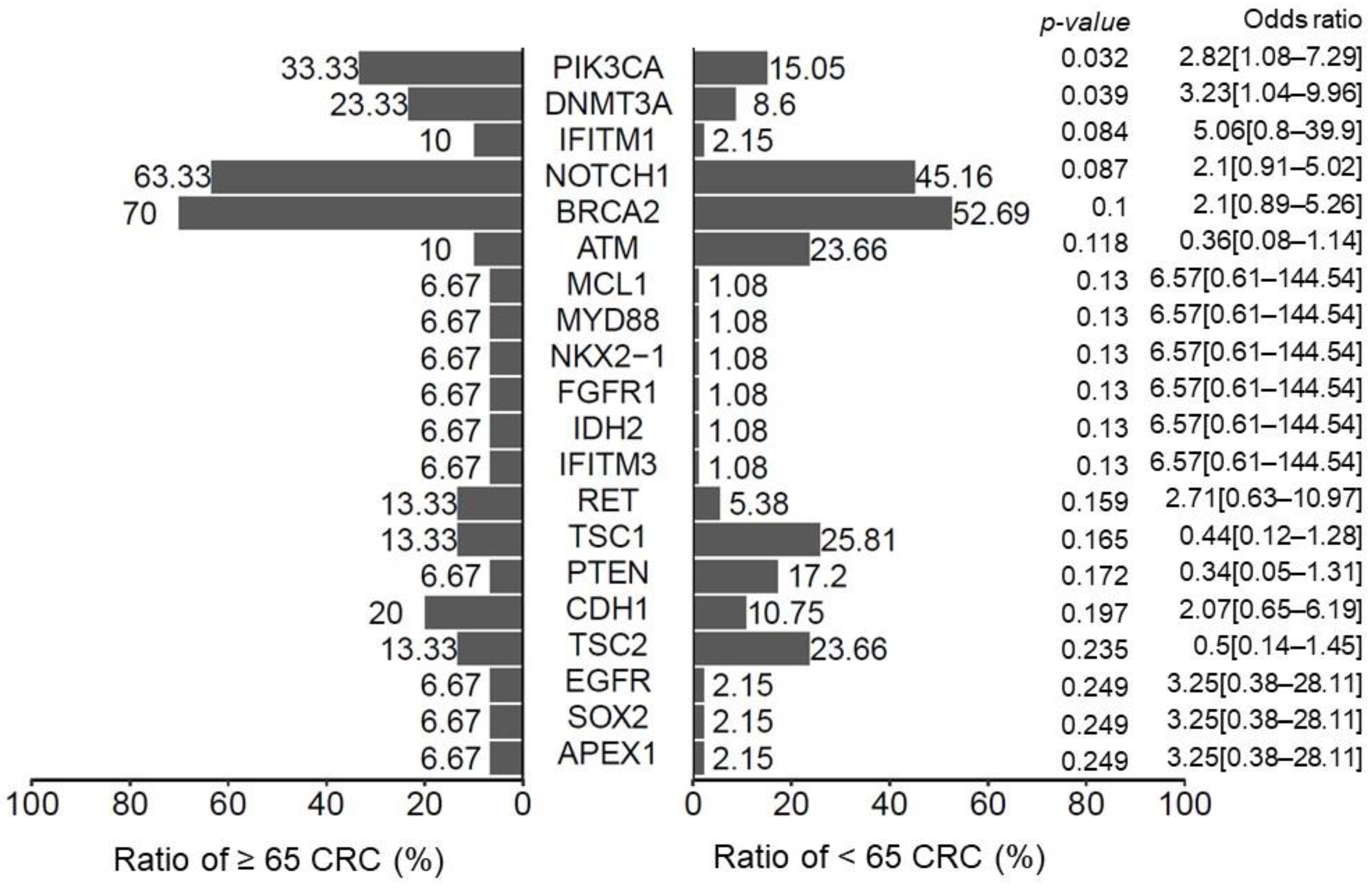
3.4. The Genomic Landscape in Older Patients with CRC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- HPA. 2020. Available online: https://www.hpa.gov.tw/Pages/Detail.aspx?nodeid=269&pid=13498 (accessed on 2 November 2021).
- Osterman, E.; Glimelius, B. Recurrence Risk after Up-to-Date Colon Cancer Staging, Surgery, and Pathology: Analysis of the Entire Swedish Population. Dis. Colon Rectum 2018, 61, 1016–1025. [Google Scholar] [CrossRef]
- Osterman, E.; Hammarström, K.; Imam, I.; Osterlund, E.; Sjöblom, T.; Glimelius, B. Recurrence Risk after Radical Colorectal Cancer Surgery—Less Than before, but How High Is It? Cancers 2020, 12, 3308. [Google Scholar] [CrossRef]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Arain, M.A.; Chen, Y.-J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Farkas, L.; et al. Colon Cancer, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 329–359. [Google Scholar] [CrossRef]
- Enofe, N.; Morris, A.D.; Liu, Y.; Liang, W.; Wu, C.S.; Sullivan, P.S.; Balch, G.G.; Staley, C.A.; Gillespie, T.W.; Shaffer, V.O. Receipt of Adjuvant Chemotherapy in Stage II Colon Cancer and Overall Survival: A National Cancer Database Study. J. Surg. Res. 2020, 252, 69–79. [Google Scholar] [CrossRef]
- Papamichael, D.; Renfro, L.A.; Matthaiou, C.; Yothers, G.; Saltz, L.; Guthrie, K.A.; Van Cutsem, E.; Schmoll, H.J.; Labianca, R.; André, T.; et al. Validity of Adjuvant! Online in older patients with stage III colon cancer based on 2967 patients from the ACCENT database. J. Geriatr. Oncol. 2016, 7, 422–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, W.; He, Y.; Wang, Y.; Li, X.; Young, J.; Ioannidis, J.P.A.; Dunlop, M.G.; Theodoratou, E. Risk factors and risk prediction models for colorectal cancer metastasis and recurrence: An umbrella review of systematic reviews and meta-analyses of observational studies. BMC Med. 2020, 18, 172. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.-H.; Kim, J.M.; Kang, G.H.; Chang, H.J.; Kang, D.W.; Kim, J.H.; Bae, J.M.; Seo, A.N.; Park, H.S.; Kang, Y.K.; et al. Standardized Pathology Report for Colorectal Cancer, 2nd Edition. J. Pathol. Transl. Med. 2020, 54, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Sluijter, C.E.; van Workum, F.; Wiggers, T.; van de Water, C.; Visser, O.; van Slooten, H.J.; Overbeek, L.I.H.; Nagtegaal, I.D. Improvement of Care in Patients with Colorectal Cancer: Influence of the Introduction of Standardized Structured Reporting for Pathology. JCO Clin. Cancer Inform. 2019, 3, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Konishi, T.; Shimada, Y.; Hsu, M.; Wei, I.H.; Pappou, E.; Smith, J.J.; Nash, G.M.; Guillem, J.G.; Paty, P.B.; Garcia-Aguilar, J.; et al. Contemporary Validation of a Nomogram Predicting Colon Cancer Recurrence, Revealing All-Stage Improved Outcomes. JNCI Cancer Spectr. 2019, 3, pkz015. [Google Scholar] [CrossRef]
- He, Y.; Ong, Y.; Li, X.; Din, F.V.N.; Brown, E.; Timofeeva, M.; Wang, Z.; Farrington, S.M.; Campbell, H.; Dunlop, M.G.; et al. Performance of prediction models on survival outcomes of colorectal cancer with surgical resection: A systematic review and meta-analysis. Surg. Oncol. 2019, 29, 196–202. [Google Scholar] [CrossRef]
- Mitsala, A.; Tsalikidis, C.; Pitiakoudis, M.; Simopoulos, C.; Tsaroucha, A.K. Artificial Intelligence in Colorectal Cancer Screening, Diagnosis and Treatment. A New Era. Curr. Oncol. 2021, 28, 1581–1607. [Google Scholar] [CrossRef]
- Ting, W.C.; Lu, Y.A.; Ho, W.C.; Cheewakriangkrai, C.; Chang, H.R.; Lin, C.L. Machine Learning in Prediction of Second Primary Cancer and Recurrence in Colorectal Cancer. Int. J. Med. Sci. 2020, 17, 280–291. [Google Scholar] [CrossRef] [Green Version]
- Achilonu, O.J.; Fabian, J.; Bebington, B.; Singh, E.; Eijkemans, M.J.C.; Musenge, E. Predicting Colorectal Cancer Recurrence and Patient Survival Using Supervised Machine Learning Approach: A South African Population-Based Study. Front. Public Health 2021, 9, 694306. [Google Scholar] [CrossRef]
- Kourou, K.; Exarchos, T.P.; Exarchos, K.P.; Karamouzis, M.V.; Fotiadis, D.I. Machine learning applications in cancer prognosis and prediction. Comput. Struct. Biotechnol. J. 2015, 13, 8–17. [Google Scholar] [CrossRef] [Green Version]
- Irizarry, R.A. Introduction to Data Science: Data Analysis and Prediction Algorithms with R, 1st ed.; Taylor & Francis Group: Abingdon on Thames, UK, 2019. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing; R Core Team: Vienna, Austria, 2020; Available online: https://www.R-project.org/ (accessed on 2 December 2021).
- Kattan, M.W. Nomograms. Introduction. Semin Urol. Oncol. 2002, 20, 79–81. [Google Scholar] [PubMed]
- Wang, K.; Li, M.; Hakonarson, H. ANNOVAR: Functional annotation of genetic variants from next-generation sequencing data. Nucleic Acids Res. 2010, 38, e164. [Google Scholar] [CrossRef] [PubMed]
- Tsai, Y.Y.; Lee, W.J. An imagined future community: Taiwan Biobank, Taiwanese genome, and nation-building. BioSocieties 2021, 16, 88–115. [Google Scholar] [CrossRef]
- Fluss, R.; Faraggi, D.; Reiser, B. Estimation of the Youden Index and its associated cutoff point. Biom. J. 2005, 47, 458–472. [Google Scholar] [CrossRef] [Green Version]
- Polikar, R. Ensemble based systems in decision making. IEEE Circuits Syst. Mag. 2006, 6, 21–45. [Google Scholar] [CrossRef]
- McKay, A.; Donaleshen, J.; Helewa, R.M.; Park, J.; Wirtzfeld, D.; Hochman, D.; Singh, H.; Turner, D. Does young age influence the prognosis of colorectal cancer: A population-based analysis. World J. Surg. Oncol. 2014, 12, 370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouvier, A.M.; Launoy, G.; Bouvier, V.; Rollot, F.; Manfredi, S.; Faivre, J.; Cottet, V.; Jooste, V. Incidence and patterns of late recurrences in colon cancer patients. Int. J. Cancer 2015, 137, 2133–2138. [Google Scholar] [CrossRef]
- Zare-Bandamiri, M.; Fararouei, M.; Zohourinia, S.; Daneshi, N.; Dianatinasab, M. Risk Factors Predicting Colorectal Cancer Recurrence Following Initial Treatment: A 5-Year Cohort Study. Asian Pac. J. Cancer Prev. 2017, 18, 2465–2470. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Li, Q.; He, D.; Chen, Y.; Li, J. Tumor size improves the accuracy of the prognostic prediction of T4a stage colon cancer. Sci. Rep. 2021, 11, 16264. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Chiang, S.-F.; Sahoo, P.K.; Mohapatra, S.K.; You, J.-F.; Onthoni, D.D.; Hung, H.-Y.; Chiang, J.-M.; Huang, Y.; Tsai, W.-S. Prediction of Colon Cancer Stages and Survival Period with Machine Learning Approach. Cancers 2019, 11, 2007. [Google Scholar] [CrossRef] [Green Version]
- Xu, Y.; Ju, L.; Tong, J.; Zhou, C.-M.; Yang, J.-J. Machine Learning Algorithms for Predicting the Recurrence of Stage IV Colorectal Cancer After Tumor Resection. Sci. Rep. 2020, 10, 2519. [Google Scholar] [CrossRef]
- Tsikitis, V.L.; Larson, D.W.; Huebner, M.; Lohse, C.M.; Thompson, P.A. Predictors of recurrence free survival for patients with stage II and III colon cancer. BMC Cancer 2014, 14, 336. [Google Scholar] [CrossRef] [Green Version]
- Hoshino, N.; Hasegawa, S.; Hida, K.; Kawada, K.; Ganeko, R.; Sugihara, K.; Sakai, Y. Nomogram for predicting recurrence in stage II colorectal cancer. Acta Oncol. 2016, 55, 1414–1417. [Google Scholar] [CrossRef] [Green Version]
- Renfro, L.A.; Grothey, A.; Xue, Y.; Saltz, L.B.; André, T.; Twelves, C.; Labianca, R.; Allegra, C.J.; Alberts, S.R.; Loprinzi, C.L.; et al. ACCENT-based web calculators to predict recurrence and overall survival in stage III colon cancer. J. Natl. Cancer Inst. 2014, 106, dju333. [Google Scholar] [CrossRef] [Green Version]
- Saso, K.; Myoshi, N.; Fujino, S.; Takenaka, Y.; Takahashi, Y.; Nishimura, J.; Yasui, M.; Ohue, M.; Tokuoka, M.; Ide, Y.; et al. A novel prognostic prediction model for recurrence in patients with stage II colon cancer after curative resection. Mol. Clin. Oncol. 2018, 9, 697–701. [Google Scholar] [CrossRef] [Green Version]
- Weiser, M.R.; Landmann, R.G.; Kattan, M.W.; Gonen, M.; Shia, J.; Chou, J.; Paty, P.B.; Guillem, J.G.; Temple, L.K.; Schrag, D.; et al. Individualized prediction of colon cancer recurrence using a nomogram. J. Clin. Oncol. 2008, 26, 380–385. [Google Scholar] [CrossRef]
- Balachandran, V.P.; Gonen, M.; Smith, J.J.; DeMatteo, R.P. Nomograms in oncology: More than meets the eye. Lancet Oncol. 2015, 16, e173–e180. [Google Scholar] [CrossRef] [Green Version]
- Lemini, R.; Attwood, K.; Pecenka, S.; Grego, J.; Spaulding, A.C.; Nurkin, S.; Colibaseanu, D.T.; Gabriel, E. Stage II-III colon cancer: A comparison of survival calculators. J. Gastrointest. Oncol. 2018, 9, 1091–1098. [Google Scholar] [CrossRef]
- Valentini, V.; van Stiphout, R.G.; Lammering, G.; Gambacorta, M.A.; Barba, M.C.; Bebenek, M.; Bonnetain, F.; Bosset, J.F.; Bujko, K.; Cionini, L.; et al. Nomograms for predicting local recurrence, distant metastases, and overall survival for patients with locally advanced rectal cancer on the basis of European randomized clinical trials. J. Clin. Oncol. 2011, 29, 3163–3172. [Google Scholar] [CrossRef] [PubMed]
- Alabi, R.O.; Mäkitie, A.A.; Pirinen, M.; Elmusrati, M.; Leivo, I.; Almangush, A. Comparison of nomogram with machine learning techniques for prediction of overall survival in patients with tongue cancer. Int. J. Med. Inform. 2021, 145, 104313. [Google Scholar] [CrossRef] [PubMed]
- Hong, K.D.; Lee, S.I.; Moon, H.Y. Lymph node ratio as determined by the 7th edition of the American Joint Committee on Cancer staging system predicts survival in stage III colon cancer. J. Surg. Oncol. 2011, 103, 406–410. [Google Scholar] [CrossRef]
- Chin, C.C.; Wang, J.Y.; Yeh, C.Y.; Kuo, Y.H.; Huang, W.S.; Yeh, C.H. Metastatic lymph node ratio is a more precise predictor of prognosis than number of lymph node metastases in stage III colon cancer. Int. J. Color. Dis. 2009, 24, 1297–1302. [Google Scholar] [CrossRef] [PubMed]
- Jakob, M.O.; Guller, U.; Ochsner, A.; Oertli, D.; Zuber, M.; Viehl, C.T. Lymph node ratio is inferior to pN-stage in predicting outcome in colon cancer patients with high numbers of analyzed lymph nodes. BMC Surg. 2018, 18, 81. [Google Scholar] [CrossRef]
- Gleisner, A.L.; Mogal, H.; Dodson, R.; Efron, J.; Gearhart, S.; Wick, E.; Lidor, A.; Herman, J.M.; Pawlik, T.M. Nodal status, number of lymph nodes examined, and lymph node ratio: What defines prognosis after resection of colon adenocarcinoma? J. Am. Coll. Surg. 2013, 217, 1090–1100. [Google Scholar] [CrossRef] [PubMed]
- Zanghì, A.; Cavallaro, A.; Lo Menzo, E.; Curella Botta, S.; Lo Bianco, S.; Di Vita, M.; Cardì, F.; Cappellani, A. Is there a relationship between length of resection and lymph-node ratio in colorectal cancer? Gastroenterol. Rep. 2020, 9, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Trepanier, M.; Erkan, A.; Kouyoumdjian, A.; Nassif, G.; Albert, M.; Monson, J.; Lee, L. Examining the relationship between lymph node harvest and survival in patients undergoing colectomy for colon adenocarcinoma. Surgery 2019, 166, 639–647. [Google Scholar] [CrossRef]
- Zhang, M.-R.; Xie, T.-H.; Chi, J.-L.; Li, Y.; Yang, L.; Yu, Y.-Y.; Sun, X.-F.; Zhou, Z.-G. Prognostic role of the lymph node ratio in node positive colorectal cancer: A meta-analysis. Oncotarget 2016, 7, 72898–72907. [Google Scholar] [CrossRef]
- Merchant, S.J.; Nanji, S.; Brennan, K.; Karim, S.; Patel, S.V.; Biagi, J.J.; Booth, C.M. Management of stage III colon cancer in the elderly: Practice patterns and outcomes in the general population. Cancer 2017, 123, 2840–2849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilleron, S.; Gower, H.; Janssen-Heijnen, M.; Signal, V.C.; Gurney, J.K.; Morris, E.J.; Cunningham, R.; Sarfati, D. Patterns of age disparities in colon and lung cancer survival: A systematic narrative literature review. BMJ Open 2021, 11, e044239. [Google Scholar] [CrossRef]
- Mima, K.; Kurashige, J.; Miyanari, N.; Morito, A.; Yumoto, S.; Matsumoto, T.; Kosumi, K.; Inoue, M.; Mizumoto, T.; Kubota, T.; et al. Advanced Age Is a Risk Factor for Recurrence After Resection in Stage II Colorectal Cancer. In Vivo 2020, 34, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.; Shaik, M.; Johnston, G.; Saha, S.K.; Berbiglia, L.; Hicks, M.; Gernand, J.; Grewal, S.; Arora, M.; Wiese, D. Tumor size predicts long-term survival in colon cancer: An analysis of the National Cancer Data Base. Am. J. Surg. 2015, 209, 570–574. [Google Scholar] [CrossRef]
- Wang, Q.; Shi, Y.-L.; Zhou, K.; Wang, L.-L.; Yan, Z.-X.; Liu, Y.-L.; Xu, L.-L.; Zhao, S.-W.; Chu, H.-L.; Shi, T.-T.; et al. PIK3CA mutations confer resistance to first-line chemotherapy in colorectal cancer. Cell Death Dis. 2018, 9, 739. [Google Scholar] [CrossRef]
- Day, F.L.; Jorissen, R.N.; Lipton, L.; Mouradov, D.; Sakthianandeswaren, A.; Christie, M.; Li, S.; Tsui, C.; Tie, J.; Desai, J.; et al. PIK3CA and PTEN gene and exon mutation-specific clinicopathologic and molecular associations in colorectal cancer. Clin. Cancer Res. 2013, 19, 3285–3296. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Yang, C.; Wu, C.; Cui, W.; Wang, L. DNA Methyltransferases in Cancer: Biology, Paradox, Aberrations, and Targeted Therapy. Cancers 2020, 12, 2123. [Google Scholar] [CrossRef]
- Cervena, K.; Siskova, A.; Buchler, T.; Vodicka, P.; Vymetalkova, V. Methylation-Based Therapies for Colorectal Cancer. Cells 2020, 9, 1540. [Google Scholar] [CrossRef] [PubMed]
- Tian, X.; Zhu, X.; Yan, T.; Yu, C.; Shen, C.; Hu, Y.; Hong, J.; Chen, H.; Fang, J.Y. Recurrence-associated gene signature optimizes recurrence-free survival prediction of colorectal cancer. Mol. Oncol. 2017, 11, 1544–1560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, J.; Wang, Z.; Chen, W.; Ding, Y.; Wang, H.; Huang, H.; Huang, W.; Cai, S. Integration of genetic signature and TNM staging system for predicting the relapse of locally advanced colorectal cancer. Int. J. Color. Dis. 2010, 25, 1277–1285. [Google Scholar] [CrossRef] [PubMed]
- Lindor, N.M.; Burgart, L.J.; Leontovich, O.; Goldberg, R.M.; Cunningham, J.M.; Sargent, D.J.; Walsh-Vockley, C.; Petersen, G.M.; Walsh, M.D.; Leggett, B.A.; et al. Immunohistochemistry versus microsatellite instability testing in phenotyping colorectal tumors. J. Clin. Oncol. 2002, 20, 1043–1048. [Google Scholar] [CrossRef] [PubMed]
- Ribic, C.M.; Sargent, D.J.; Moore, M.J.; Thibodeau, S.N.; French, A.J.; Goldberg, R.M.; Hamilton, S.R.; Laurent-Puig, P.; Gryfe, R.; Shepherd, L.E.; et al. Tumor microsatellite-instability status as a predictor of benefit from fluorouracil-based adjuvant chemotherapy for colon cancer. N. Engl. J. Med. 2003, 349, 247–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lanza, G.; Gafà, R.; Santini, A.; Maestri, I.; Guerzoni, L.; Cavazzini, L. Immunohistochemical test for MLH1 and MSH2 expression predicts clinical outcome in stage II and III colorectal cancer patients. J. Clin. Oncol. 2006, 24, 2359–2367. [Google Scholar] [CrossRef] [PubMed]
- Jover, R.; Zapater, P.; Castells, A.; Llor, X.; Andreu, M.; Cubiella, J.; Balaguer, F.; Sempere, L.; Xicola, R.M.; Bujanda, L.; et al. The efficacy of adjuvant chemotherapy with 5-fluorouracil in colorectal cancer depends on the mismatch repair status. Eur. J. Cancer 2009, 45, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.; Taieb, J.; Fiskum, J.; Yothers, G.; Goldberg, R.; Yoshino, T.; Alberts, S.; Allegra, C.; de Gramont, A.; Seitz, J.F.; et al. Microsatellite Instability in Patients with Stage III Colon Cancer Receiving Fluoropyrimidine With or Without Oxaliplatin: An ACCENT Pooled Analysis of 12 Adjuvant Trials. J. Clin. Oncol. 2021, 39, 642–651. [Google Scholar] [CrossRef]
- Lugli, A.; Kirsch, R.; Ajioka, Y.; Bosman, F.; Cathomas, G.; Dawson, H.; El Zimaity, H.; Fléjou, J.F.; Hansen, T.P.; Hartmann, A.; et al. Recommendations for reporting tumor budding in colorectal cancer based on the International Tumor Budding Consensus Conference (ITBCC) 2016. Mod. Pathol. 2017, 30, 1299–1311. [Google Scholar] [CrossRef] [PubMed]
- Van Wyk, H.C.; Park, J.H.; Edwards, J.; Horgan, P.G.; McMillan, D.C.; Going, J.J. The relationship between tumour budding, the tumour microenvironment and survival in patients with primary operable colorectal cancer. Br. J. Cancer 2016, 115, 156–163. [Google Scholar] [CrossRef] [Green Version]
- Van Wyk, H.C.; Roseweir, A.; Alexander, P.; Park, J.H.; Horgan, P.G.; McMillan, D.C.; Edwards, J. The Relationship Between Tumor Budding, Tumor Microenvironment, and Survival in Patients with Primary Operable Colorectal Cancer. Ann. Surg. Oncol. 2019, 26, 4397–4404. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Overall (N = 1073) | Recurrence | p-Value | |
|---|---|---|---|---|
| Yes (n = 159) | No (n = 914) | |||
| Sex | 0.062 | |||
| Male | 616 (57.4%) | 102 (64.2%) | 514 (56.2%) | |
| Female | 457 (42.6%) | 57 (35.8%) | 400 (43.8%) | |
| Age (years) | 65.39 (12.88) | 65.86 (12.97) | 65.31 (12.87) | 0.432 |
| BMI | 23.80 (3.70) | 23.87 (3.79) | 23.78 (3.69) | 0.992 |
| Radiotherapy | 0.288 | |||
| No | 786 (73.3%) | 111 (69.8%) | 675 (73.9%) | |
| Yes | 287 (26.7%) | 48 (30.2%) | 239 (26.1%) | |
| Chemotherapy | 0.003 | |||
| No | 138 (12.9%) | 9 (5.7%) | 129 (14.1%) | |
| Yes | 935 (87.1%) | 150 (94.3%) | 785 (85.9%) | |
| Tumor site | 0.466 | |||
| Right side colon | 322 (30.3%) | 42 (26.6%) | 280 (30.9%) | |
| Left side colon | 464 (43.7%) | 70 (44.3%) | 394 (43.5%) | |
| Rectum | 277 (26.1%) | 46 (29.1%) | 231 (25.5%) | |
| Tumor configuration | 0.008 | |||
| Endophytic | 733 (69.3%) | 123 (78.3%) | 610 (67.8%) | |
| Exophytic | 324 (30.7%) | 34 (21.7%) | 290 (32.2%) | |
| Tumor size | 0.189 | |||
| ≤3 cm | 270 (25.9%) | 39 (25.3%) | 231 (26.0%) | |
| 3.1–5.9 cm | 489 (46.8%) | 64 (41.6%) | 425 (47.8%) | |
| ≥6 cm | 285 (27.3%) | 51 (33.1%) | 234 (26.3%) | |
| Tumor volume | 42.13 (111.09) | 59.89 (148.86) | 39.09 (103.07) | 0.066 |
| Histologic grade | 0.084 | |||
| Poorly diff. | 48 (4.6%) | 11 (7.1%) | 37 (4.2%) | |
| Moderately diff. | 868 (83.0%) | 132 (84.6%) | 736 (82.7%) | |
| Well-diff. | 130 (12.4%) | 13 (8.3%) | 117 (13.1%) | |
| TNM stage * | <0.001 | |||
| II | 528 (49.2%) | 56 (35.2%) | 472 (51.6%) | |
| III | 545 (50.8%) | 103 (64.8%) | 442 (48.4%) | |
| Tumor invasion stage (pT) | <0.001 | |||
| 1–2 | 75 (7.0%) | 6 (3.8%) | 69 (7.6%) | |
| 3 | 858 (80.6%) | 115 (73.2%) | 743 (81.9%) | |
| 4 | 131 (12.3%) | 36 (22.9%) | 95 (10.5%) | |
| Lymph nodes status (pN) | <0.001 | |||
| 0 | 488 (49.3%) | 53 (35.3%) | 435 (51.8%) | |
| 1 | 343 (34.7%) | 54 (36.0%) | 289 (34.4%) | |
| 2 | 158 (16.0%) | 43 (28.7%) | 115 (13.7%) | |
| LN metastasis numbers | 1.74 (3.37) | 3.16 (4.58) | 1.50 (3.05) | <0.001 |
| Total harvested LNs | 20.02 (9.26) | 19.35 (8.35) | 20.14 (9.41) | 0.749 |
| LN ratio | 0.09 (0.15) | 0.16 (0.21) | 0.08 (0.14) | <0.001 |
| Distal margin | 0.159 | |||
| Uninvolved | 1061 (99.5%) | 155 (98.7%) | 906 (99.7%) | |
| Involved | 5 (0.5%) | 2 (1.3%) | 3 (0.3%) | |
| Circumferential margin | 0.075 | |||
| Uninvolved | 309 (91.2%) | 56 (90.3%) | 253 (91.3%) | |
| Involved | 13 (3.8%) | 5 (8.1%) | 8 (2.9%) | |
| Cannot be assessed | 17 (5.0%) | 1 (1.6%) | 16 (5.8%) | |
| Lymphovascular invasion | <0.001 | |||
| Absence | 624 (58.2%) | 57 (35.8%) | 567 (62.1%) | |
| Present | 448 (41.8%) | 102 (64.2%) | 346 (37.9%) | |
| Perineural invasion | <0.001 | |||
| Absence | 571 (53.3%) | 53 (33.3%) | 518 (56.7%) | |
| Present | 501 (46.7%) | 106 (66.7%) | 395 (43.3%) | |
| Tumor growth pattern | 0.083 | |||
| Infiltrating | 969 (90.6%) | 150 (94.3%) | 819 (90.0%) | |
| Pushing | 100 (9.4%) | 9 (5.7%) | 91 (10.0%) | |
| Tumor budding | 0.004 | |||
| Absent | 342 (81.4%) | 20 (62.5%) | 322 (83%) | |
| Present | 78 (18.6%) | 12 (37.5%) | 66 (17%) | |
| TRG | 0.312 | |||
| 1–2 | 15 (12.5%) | 5 (19.2%) | 10 (10.6%) | |
| 3–5 | 105 (87.5%) | 21 (80.8%) | 84 (89.4%) | |
| Neoadjuvant CCRT | 0.025 | |||
| No | 953 (88.8%) | 133 (83.6%) | 820 (89.7%) | |
| Yes | 120 (11.2%) | 26 (16.4%) | 94 (10.3%) | |
| dMMR | 0.932 | |||
| Deficient | 35 (10.1%) | 3 (9.7%) | 32 (10.2%) | |
| Proficient | 311 (89.9%) | 28 (90.3%) | 283 (89.8%) | |
| BRAF_V600E_Stain | >0.999 | |||
| Negative | 101 (85.6%) | 12 (85.7%) | 89 (85.6%) | |
| Positive | 17 (14.4%) | 2 (14.3%) | 15 (14.4%) | |
| Alive | <0.001 | |||
| Yes | 912 (85.0%) | 86 (54.1%) | 826 (90.4%) | |
| No | 161 (15.0%) | 73 (45.9%) | 88 (9.6%) | |
| Characteristic * | Univariable Analysis | Multivariable Analysis | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Age (years) | ||||||
| <65 vs. ≥65 | 1.24 | 0.85–1.81 | 0.273 | 1.70 | 1.12–2.61 | 0.014 |
| Tumor size | ||||||
| 1 vs. 2 (3.1–5.9 cm) | 0.88 | 0.55–1.44 | 0.612 | 0.94 | 0.56–1.60 | 0.808 |
| 1 vs. 3 (≥6 cm) | 1.21 | 0.73–2.03 | 0.466 | 1.79 | 1.01–3.22 | 0.047 |
| Lymph node ratio | 16.9 | 5.93–48.1 | <0.001 | 10.8 | 3.51–33.2 | <0.001 |
| Perineural invasion | ||||||
| No vs. Present | 2.37 | 1.61–3.52 | <0.001 | 2.51 | 1.63–3.91 | <0.001 |
| Neoadjuvant CCRT | ||||||
| No vs. Yes | 2.12 | 1.25–3.47 | 0.004 | 3.34 | 1.80–6.12 | <0.001 |
| Characteristic * | Univariable Analysis | Multivariable Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age (years) | ||||||
| <65 vs. ≥65 | 1.25 | 0.91–1.71 | 0.164 | 1.74 | 1.24–2.44 | 0.001 |
| Tumor size | ||||||
| 1 vs. 2 (3.1–5.9 cm) | 0.87 | 0.59–1.30 | 0.500 | 0.92 | 0.61–1.41 | 0.711 |
| 1 vs. 3 (≥6 cm) | 1.19 | 0.79–1.81 | 0.406 | 1.82 | 1.16–2.85 | 0.010 |
| Lymph node ratio | 10.1 | 4.95–20.6 | <0.001 | 6.82 | 3.20–14.5 | <0.001 |
| Perineural invasion | ||||||
| No vs. Present | 2.73 | 1.96–3.80 | <0.001 | 2.90 | 2.03–4.16 | <0.001 |
| Neoadjuvant CCRT | ||||||
| No vs. Yes | 1.68 | 1.10–2.55 | 0.016 | 2.35 | 1.46–3.81 | <0.001 |
| Characteristic | Age (Years) | p-Value | ||
|---|---|---|---|---|
| ≤50 (n = 150) | 51–69 (n = 470) | ≥70 (n = 453) | ||
| Sex | 0.003 | |||
| Male | 80 (53.3%) | 297 (63.2%) | 239 (52.8%) | |
| Female | 70 (46.7%) | 173 (36.8%) | 214 (47.2%) | |
| Age (years) | 43.47 (5.81) | 60.72 (5.20) | 77.49 (5.02) | <0.001 |
| BMI | 24.00 (3.94) | 24.03 (3.77) | 23.49 (3.52) | 0.206 |
| Radiotherapy | <0.001 | |||
| No | 97 (64.7%) | 314 (66.8%) | 375 (82.8%) | |
| Yes | 53 (35.3%) | 156 (33.2%) | 78 (17.2%) | |
| Chemotherapy | <0.001 | |||
| No | 10 (6.7%) | 33 (7.0%) | 95 (21.0%) | |
| Yes | 140 (93.3%) | 437 (93.0%) | 358 (79.0%) | |
| Tumor site | 0.002 | |||
| Right side colon | 37 (24.7%) | 126 (26.9%) | 159 (35.7%) | |
| Left side colon | 63 (42.0%) | 208 (44.4%) | 193 (43.4%) | |
| Rectum | 50 (33.3%) | 134 (28.6%) | 93 (20.9%) | |
| Tumor configuration | 0.549 | |||
| Endophytic | 113 (75.3%) | 322 (69.4%) | 298 (67.3%) | |
| Exophytic | 37 (24.7%) | 142 (30.6%) | 145 (32.7%) | |
| Tumor size | 0.008 | |||
| ≤3 cm | 42 (28.6%) | 140 (30.3%) | 88 (20.2%) | |
| 3.1–5.9 cm | 70 (47.6%) | 207 (44.8%) | 212 (48.7%) | |
| ≥6 cm | 35 (23.8%) | 115 (24.9%) | 135 (31.0%) | |
| Tumor volume | 38.80 (81.50) | 35.99 (67.57) | 49.62 (149.17) | 0.049 |
| Histology grade | 0.812 | |||
| Poorly diff. | 9 (6.1%) | 20 (4.4%) | 19 (4.3%) | |
| Moderately diff. | 124 (83.8%) | 380 (82.8%) | 364 (82.9%) | |
| Well-diff. | 15 (10.1%) | 59 (12.9%) | 56 (12.8%) | |
| TNM stage * | <0.001 | |||
| II | 59 (39.3%) | 217 (46.2%) | 252 (55.6%) | |
| III | 91 (60.7%) | 253 (53.8%) | 201 (44.4%) | |
| Tumor invasion stage (pT) | 0.040 | |||
| 1–2 | 10 (6.8%) | 44 (9.5%) | 21 (4.6%) | |
| 3 | 115 (77.7%) | 369 (79.5%) | 374 (82.7%) | |
| 4 | 23 (15.5%) | 51 (11.0%) | 57 (12.6%) | |
| LN status (pN) | 0.005 | |||
| 0 | 53 (40.2%) | 197 (45.7%) | 238 (55.9%) | |
| 1 | 54 (40.9%) | 156 (36.2%) | 133 (31.2%) | |
| 2 | 25 (18.9%) | 78 (18.1%) | 55 (12.9%) | |
| LN metastasis numbers | 2.26 (4.05) | 1.80 (3.03) | 1.51 (3.44) | 0.001 |
| Total harvested LNs | 21.62 (10.40) | 19.89 (9.54) | 19.63 (8.49) | 0.207 |
| LN ratio | 0.10 (0.16) | 0.10 (0.16) | 0.08 (0.14) | 0.004 |
| Distal margin | >0.999 | |||
| Uninvolved | 149 (100.0%) | 466 (99.4%) | 446 (99.6%) | |
| Involved | 0 (0.0%) | 3 (0.6%) | 2 (0.4%) | |
| Circumferential margin | 0.412 | |||
| Uninvolved | 54 (96.4%) | 140 (88.1%) | 115 (92.7%) | |
| Involved | 1 (1.8%) | 9 (5.7%) | 3 (2.4%) | |
| Cannot be assessed | 1 (1.8%) | 10 (6.3%) | 6 (4.8%) | |
| Lymphovascular invasion | 0.212 | |||
| Absence | 78 (52.0%) | 274 (58.3%) | 272 (60.2%) | |
| Present | 72 (48.0%) | 196 (41.7%) | 180 (39.8%) | |
| Perineural invasion | 0.018 | |||
| Absence | 65 (43.3%) | 250 (53.2%) | 256 (56.6%) | |
| Present | 85 (56.7%) | 220 (46.8%) | 196 (43.4%) | |
| Growth pattern at tumor periphery | 0.273 | |||
| Infiltrating | 141 (94.0%) | 424 (90.6%) | 404 (89.6%) | |
| Pushing | 9 (6.0%) | 44 (9.4%) | 47 (10.4%) | |
| Tumor budding | 0.568 | |||
| Absence | 59 (83.1%) | 144 (79.1%) | 139 (83.2%) | |
| Present | 12 (16.9%) | 38 (20.9%) | 28 (16.8%) | |
| TRG | 0.765 | |||
| 1–2 | 5 (16.1%) | 7 (11.5%) | 3 (10.7%) | |
| 3–5 | 26 (83.9%) | 54 (88.5%) | 25 (89.3%) | |
| Neoadjuvant CCRT | <0.001 | |||
| No | 119 (79.3%) | 409 (87.0%) | 425 (93.8%) | |
| Yes | 31 (20.7%) | 61 (13.0%) | 28 (6.2%) | |
| dMMR | 0.488 | |||
| Deficient | 9 (14.3%) | 14 (9.2%) | 12 (9.2%) | |
| Proficient | 54 (85.7%) | 138 (90.8%) | 119 (90.8%) | |
| BRAF_V600E_stain | 0.076 | |||
| Negative | 23 (100.0%) | 42 (82.4%) | 36 (81.8%) | |
| Positive | 0 (0.0%) | 9 (17.6%) | 8 (18.2%) | |
| Recurrence | 0.698 | |||
| No | 129 (86.0%) | 404 (86.0%) | 381 (84.1%) | |
| Yes | 21 (14.0%) | 66 (14.0%) | 72 (15.9%) | |
| Alive | <0.001 | |||
| Yes | 137 (91.3%) | 425 (90.4%) | 350 (77.3%) | |
| No | 13 (8.7%) | 45 (9.6%) | 103 (22.7%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, P.-C.; Yeh, Y.-M.; Lin, B.-W.; Chan, R.-H.; Su, P.-F.; Liu, Y.-C.; Lee, C.-T.; Chen, S.-H.; Lin, P.-C. A Prediction Model for Tumor Recurrence in Stage II–III Colorectal Cancer Patients: From a Machine Learning Model to Genomic Profiling. Biomedicines 2022, 10, 340. https://doi.org/10.3390/biomedicines10020340
Chen P-C, Yeh Y-M, Lin B-W, Chan R-H, Su P-F, Liu Y-C, Lee C-T, Chen S-H, Lin P-C. A Prediction Model for Tumor Recurrence in Stage II–III Colorectal Cancer Patients: From a Machine Learning Model to Genomic Profiling. Biomedicines. 2022; 10(2):340. https://doi.org/10.3390/biomedicines10020340
Chicago/Turabian StyleChen, Po-Chuan, Yu-Min Yeh, Bo-Wen Lin, Ren-Hao Chan, Pei-Fang Su, Yi-Chia Liu, Chung-Ta Lee, Shang-Hung Chen, and Peng-Chan Lin. 2022. "A Prediction Model for Tumor Recurrence in Stage II–III Colorectal Cancer Patients: From a Machine Learning Model to Genomic Profiling" Biomedicines 10, no. 2: 340. https://doi.org/10.3390/biomedicines10020340
APA StyleChen, P.-C., Yeh, Y.-M., Lin, B.-W., Chan, R.-H., Su, P.-F., Liu, Y.-C., Lee, C.-T., Chen, S.-H., & Lin, P.-C. (2022). A Prediction Model for Tumor Recurrence in Stage II–III Colorectal Cancer Patients: From a Machine Learning Model to Genomic Profiling. Biomedicines, 10(2), 340. https://doi.org/10.3390/biomedicines10020340