
Statistical Issues in Serial Killer Nurse Cases



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
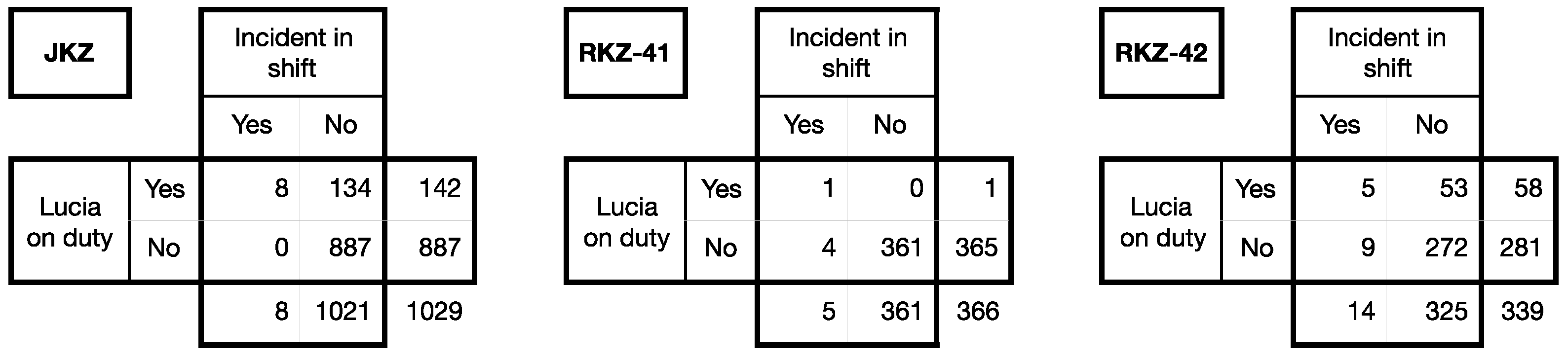
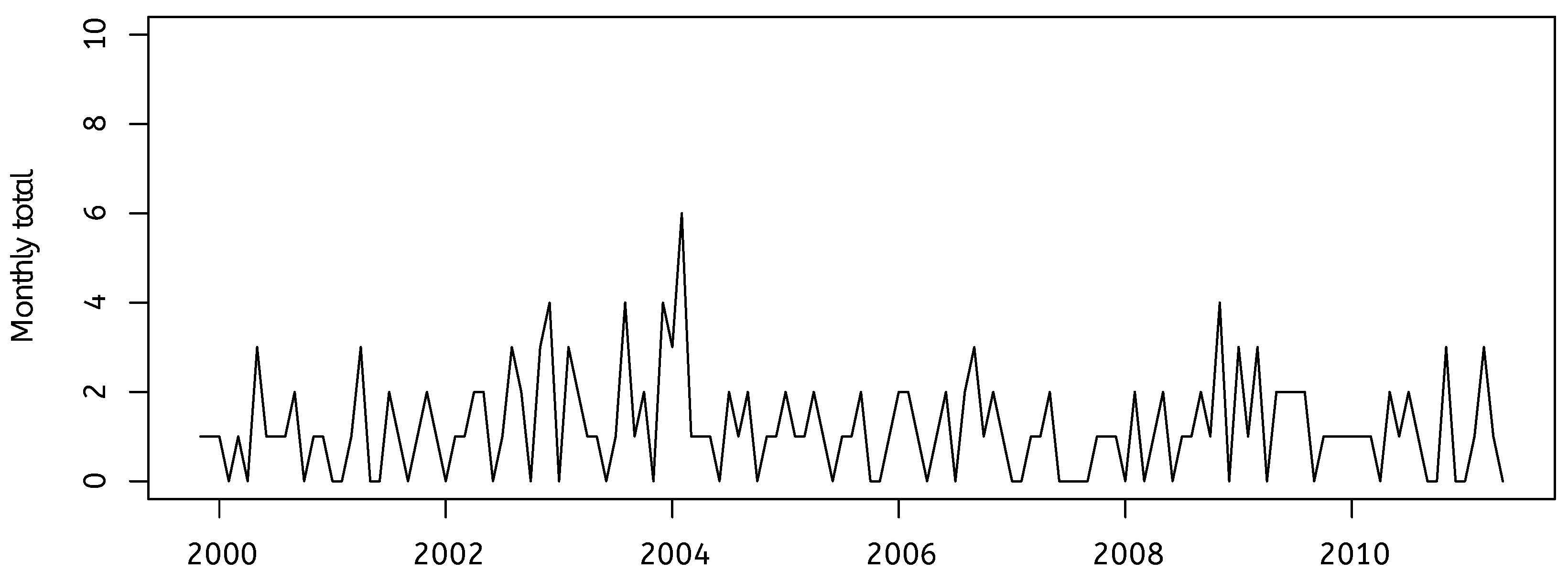
3. The Case of Lucia de Berk
4. The Case of Ben Geen
5. New Findings in the Ben Geen Case
6. Insights from Forensic Psychology and Criminology
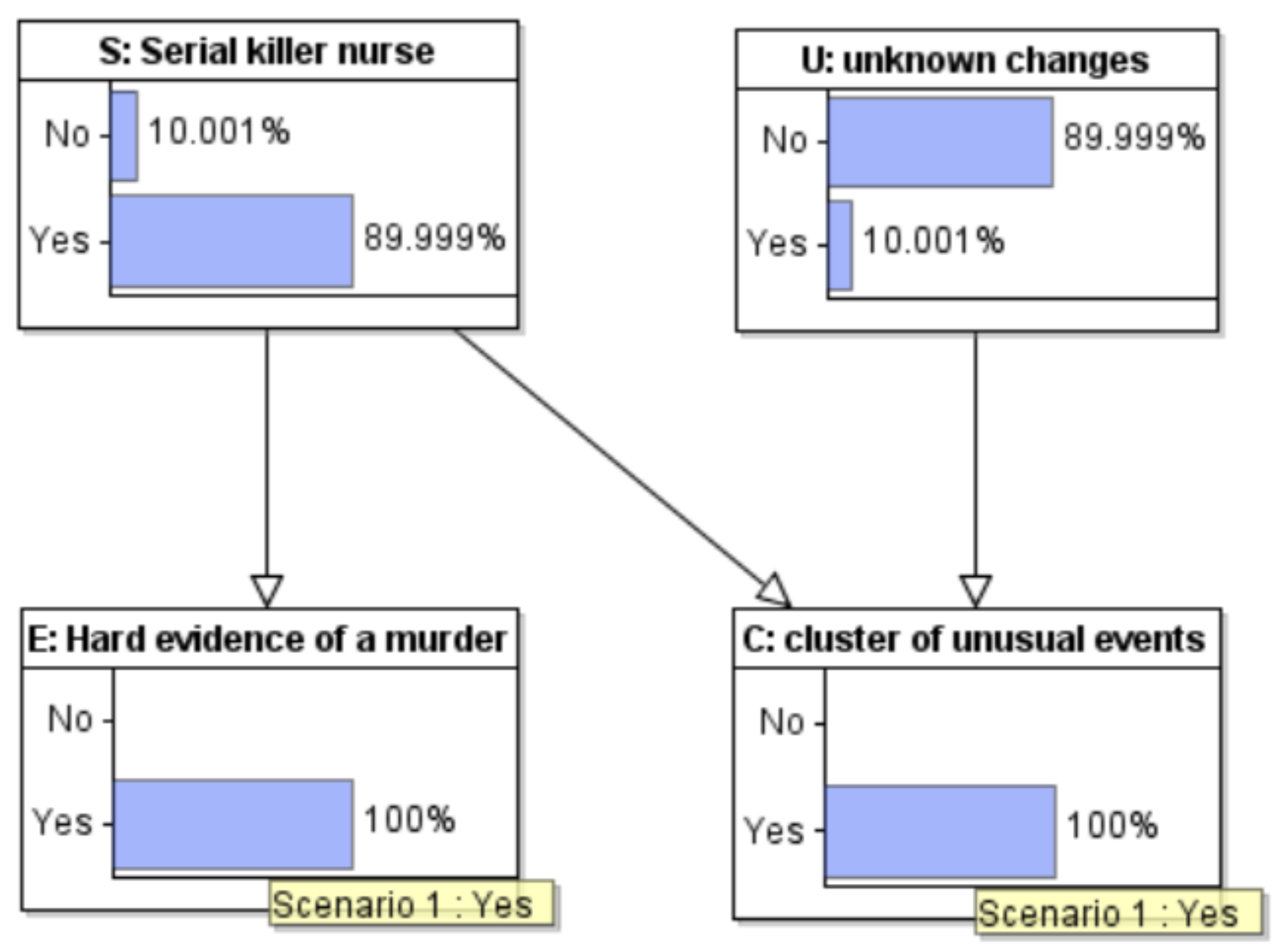
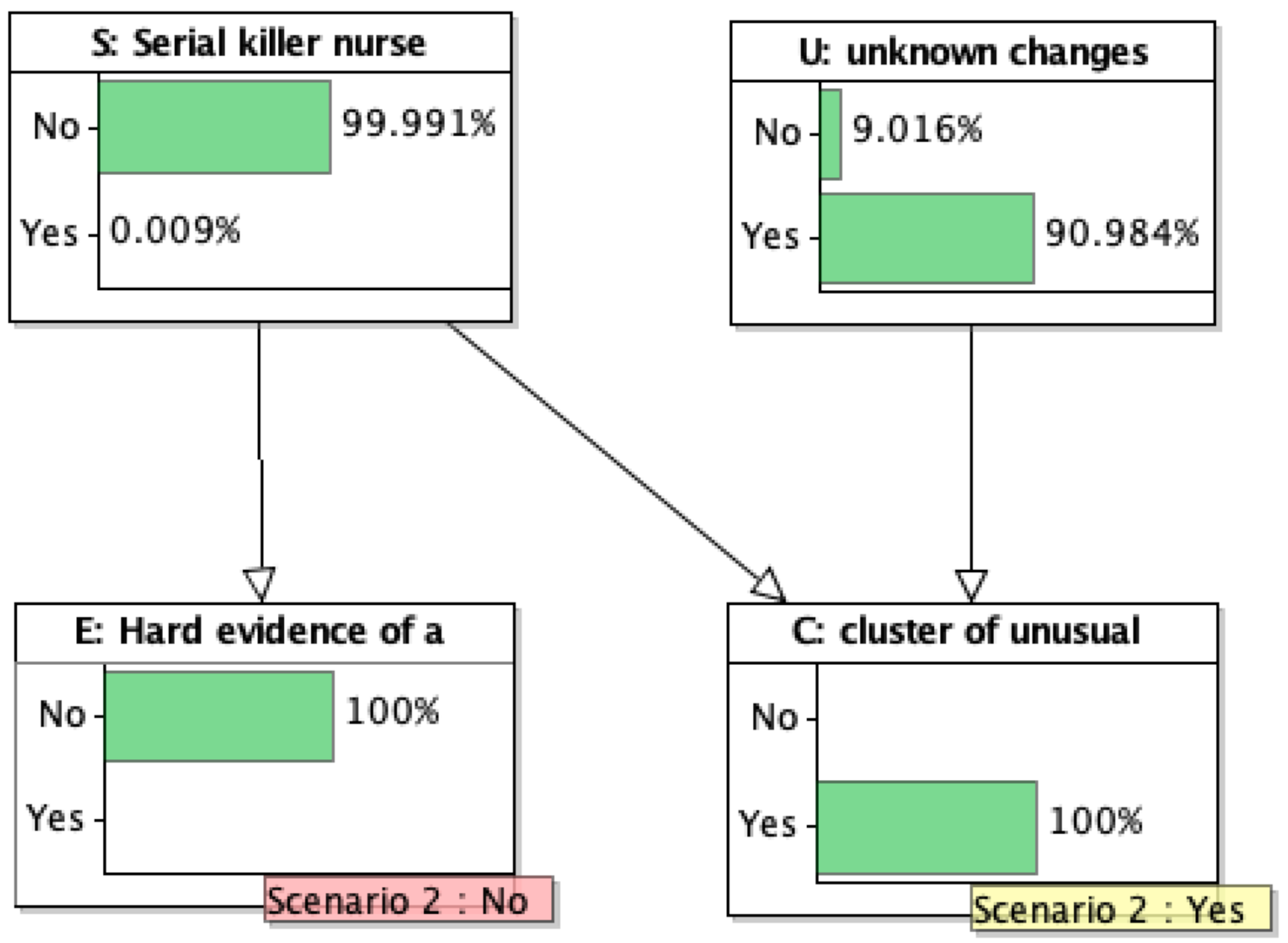
7. Bayesian Analysis of a Stylized Case
8. Confirmational Bias and Other Biases
The hospital’s illegal and unqualified investigation team was only looking for evidence to secure a conviction (Confirmation Bias) while discarding or ignoring evidence that proved Ben’s innocence. The hospital’s Serious Untoward Investigation Team initiated by Chief Nurse Brock in her capacity of Executive Lead for Governance consisted of several medical, nursing, and medical records staff who were all untrained in forensic investigative techniques, crime scene preservation and the taking of witness statements. The team carried out an unlawful and flawed investigation, the material from which was later presented to medical experts appointed by the prosecution as legitimate. The opinion of these medical experts was based on flawed evidence, which had been given to those experts without their knowledge of how that evidence had been obtained. Expert opinion given on the basis of ignorance of improperly obtained evidence invalidates that medical expert evidence. The judge and jury were not aware at the trial that the evidence had been unlawfully obtained, nor of the risks to justice associated with it.
9. Conclusions
Justice systems are sometimes called upon to evaluate cases in which health care professionals are suspected of killing their patients illegally. These cases are difficult to evaluate because they involve at least two levels of uncertainty. Commonly in a murder case, it is clear that a homicide has occurred, and investigators must resolve uncertainty about who is responsible. In the cases we examine here there is also uncertainty about whether homicide has occurred. Investigators need to consider whether the deaths that prompted the investigation could plausibly have occurred for reasons other than homicide, in addition to considering whether, if homicide was indeed the cause, the person under suspicion is responsible. In this report, the RSS provides advice and guidance on the investigation and evaluation of such cases. This report was prompted by concerns about the statistical challenges such cases pose for the legal system. The cases often turn, in part, on statistical evidence that is difficult for lay people and even legal professionals to evaluate. Furthermore, the statistical evidence may be distorted by biases, hidden or apparent, in the investigative process that render it misleading. In this report, the RSS provides advice and guidance on how to conduct investigations in such cases, with a particular focus on minimizing the kinds of biases that could distort statistical evidence arising from the investigation. This report also provides guidance on how to recognize and take account of such biases when evaluating statistical evidence and more broadly on how to understand the strengths and limitations of such evidence and give it proper weight. This report is designed specifically to help all professionals involved in investigating such cases and those who evaluate such cases in the legal system, including expert witnesses. It will also be of interest to scholars and legal professionals who are interested in the role of statistics in evidentiary proof, and more generally to anyone interested in improving criminal investigations.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Dotto, Francesco, Richard D. Gill, and Julia Mortera. 2022. Statistical Analyses in the case of an Italian nurse accused of murdering patients. arXiv arXiv:2202.08895. To appear in Law, Probability and Risk. [Google Scholar]
- Dror, Itiel, and David Charlton. 2006. Why experts make errors. Journal of Forensic Identification 56: 600. Available online: https://www.researchgate.net/publication/248440075_Why_Experts_Make_Errors (accessed on 1 August 2022).
- Dror, Itiel E., Ruth M. Morgan, Carolyn Rando, and Sherry Nakhaeizadeh. 2017. Letter to the editor—The bias snowball and the bias cascade effects: Two distinct biases that may impact forensic decision making. Journal of Forensic Sciences 62: 832–33. [Google Scholar] [CrossRef] [PubMed]
- Elffers, Henk. 2002a. Distribution of Incidents of Resuscitation and Death in the Juliana Kinderziekenhuis and the Rode Kruisziekenhuis. (Unofficial English Translation of Dutch Original). Available online: https://www.math.leidenuniv.nl/~gill/Elffers1eng.pdf (accessed on 1 August 2022).
- Elffers, Henk. 2002b. Elaborated Analysis. Distribution of Incidents of Resuscitation and Death at the Juliana Kinderziekenhuis and the Rode Kruisziekenhuis. (Unofficial English Translation of Dutch Original). Available online: https://www.math.leidenuniv.nl/~gill/Elffers2eng.pdf (accessed on 1 August 2022).
- Fenton, Norman, Martin Neil, and Daniel Berger. 2016. Bayes and the Law. Annual Review of Statistics and Its Application 3: 51–77. Available online: http://www.eecs.qmul.ac.uk/~norman/papers/bayes_and_the_law_revised_FINAL.pdf (accessed on 1 August 2022). [CrossRef]
- Fienberg, Stephen E., and David H. Kaye. 1991. Legal and Statistical Aspects of Some Mysterious Clusters. Journal of the Royal Statistical Society A 154: 61–74. Available online: https://ssrn.com/abstract=2777146 (accessed on 1 August 2022). [CrossRef]
- Forrest, Alexander R. W. 1995. Nurses who systematically harm their patients. Medical Law International 1: 411–21. [Google Scholar] [CrossRef]
- Gill, Richard D. 2014. Rarity of respiratory arrest in ED? arXiv arXiv:1407.2731. [Google Scholar]
- Gill, Richard D., Piet Groeneboom, and Peter De Jong. 2018. Elementary Statistics on Trial (the case of Lucia de Berk). Chance 31: 9–15. [Google Scholar] [CrossRef]
- Peter Green, Richard D. Gill, Neil Mackenzie, Julia Mortera, and William Thompson. 2022. Healthcare Serial Killer or Coincidence? Statistical Issues in Investigation of Suspected Medical Misconduct. London: Royal Statistical Society, To appear, September 2022. [Google Scholar]
- Hesketh, Wendy. 2012. The police-health profession’s protocol: A review. The Police Journal 85: 203–20. [Google Scholar] [CrossRef]
- Ibs, Inga Catharina. 2016. Applications of Bayesian Networks in Legal Reasoning. Bachelor’s thesis, University of Osnabrück, Osnabrück, Germany. Available online: https://www.researchgate.net/publication/311667346_Applications_of_Bayesian_Networks_In_Legal_Reasoning (accessed on 1 August 2022).
- Kassin, Saul M., Itiel E. Dror, and Jeff Kukucka. 2013. The Forensic Confirmation Bias: Problems, Perspectives, and Proposed Solutions. Journal of Applied Research in Memory and Cognition 2: 42–52. [Google Scholar] [CrossRef]
- Lagnado, David A. 2021. Explaining the Evidence: How the Mind Investigates the World. Cambridge: Cambridge University Press. [Google Scholar]
- Nickerson, Raymond S. 1998. Confirmation bias: A ubiquitous phenomenon in many guises. Review of General Psychology 2: 175–220. [Google Scholar] [CrossRef]
- Pennington, Nancy, and Reid Hastie. 1986. Evidence evaluation in complex decision making. Journal of Personality and Social Psychology 51: 242–58. [Google Scholar] [CrossRef]
- Pennington, Nancy, and Reid Hastie. 1992. Explaining the evidence: Tests of the Story Model for juror decision making. Journal of Personality and Social Psychology 62: 189–206. [Google Scholar] [CrossRef]
- Sackett, David L. 1979. Bias in analytical research. Journal of Chronic Diseases 32: 51–63. [Google Scholar] [CrossRef]
- Scherr, Kyle C., Allison D. Redlich, and Saul M. Kassin. 2013. Cumulative disadvantage: A psychological framework for understanding how innocence can lead to confession, wrongful conviction, and beyond. Perspectives on Psychological Science 15: 353–83. [Google Scholar] [CrossRef] [PubMed]
- Yardley, Elizabeth, and David Wilson. 2014. In Search of the ‘Angels of Death’: Conceptualising the Contemporary Nurse Healthcare Serial Killer. Journal of Investigative Psychology and Offender Profiling 13: 39–55. [Google Scholar] [CrossRef]
| 1 | Authors of the booklet are Professor Peter Green FRS, Emeritus Professor of Statistics, University of Bristol, and Distinguished Professor, University of Technology, Sydney (chairman); Professor Richard Gill, Emeritus Professor of Statistics, Leiden University; Neil Mackenzie QC, Arnot Manderson Advocates, Edinburgh; Professor Julia Mortera, Professor of Statistics, Università Roma Tre; Professor William Thompson, Professor Emeritus of Criminology, Law, and Society; Psychology and Social Behavior; and Law, University of California, Irvine. One of the appendices was provided by Professor Jane Hutton, Professor of Medical Statistics, University of Warwick. |





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gill, R.D.; Fenton, N.; Lagnado, D. Statistical Issues in Serial Killer Nurse Cases. Laws 2022, 11, 65. https://doi.org/10.3390/laws11050065
Gill RD, Fenton N, Lagnado D. Statistical Issues in Serial Killer Nurse Cases. Laws. 2022; 11(5):65. https://doi.org/10.3390/laws11050065
Chicago/Turabian StyleGill, Richard D., Norman Fenton, and David Lagnado. 2022. "Statistical Issues in Serial Killer Nurse Cases" Laws 11, no. 5: 65. https://doi.org/10.3390/laws11050065
APA StyleGill, R. D., Fenton, N., & Lagnado, D. (2022). Statistical Issues in Serial Killer Nurse Cases. Laws, 11(5), 65. https://doi.org/10.3390/laws11050065