Evidence of Associations Between Feto-Maternal Vitamin D Status, Cord Parathyroid Hormone and Bone-Specific Alkaline Phosphatase, and Newborn Whole Body Bone Mineral Content

Abstract
:1. Introduction
2. Subjects and Methods
3. Statistical Analysis
4. Results

{kind=link}
| Cord 25(OH)D 1 | Maternal PTH 1 | Cord PTH 1 | Cord BALP 1 | Unadjusted WBBMC | Adjusted WBBMC 2 | |
|---|---|---|---|---|---|---|
| Maternal 25(OH)D | 0.78 | −0.44 | −0.19 | −0.26 | NS | 0.21 |
| <0.0001 | <0.0001 | 0.09 | 0.02 | 0.06 | ||
| Cord 25(OH)D 1 | - | −0.43 | −0.24 | −0.34 | NS | 0.23 |
| <0.0001 | 0.03 | 0.002 | 0.04 | |||
| Maternal PTH 1 | - | NS | 0.21 | NS | NS | |
| 0.07 | ||||||
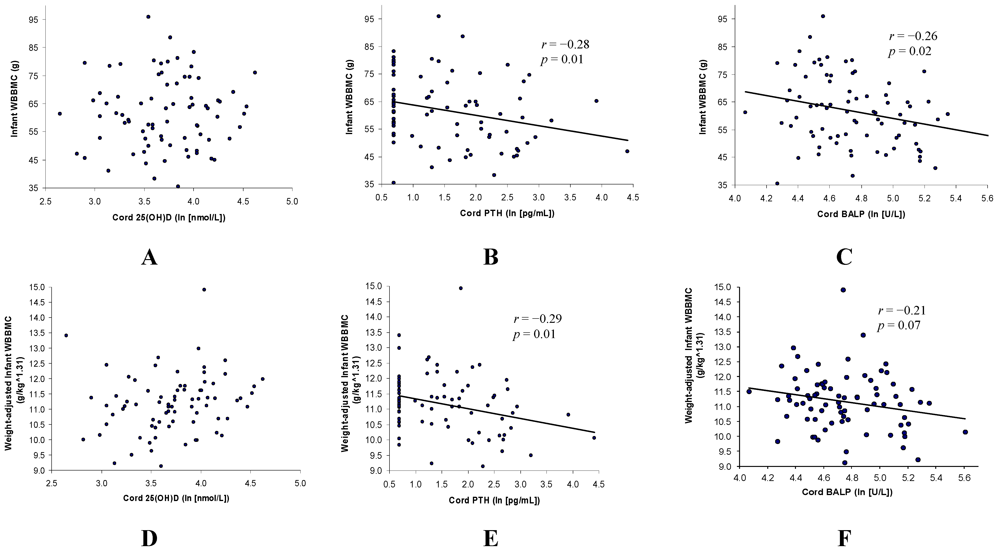
| Cord PTH 1 | - | 0.27 | −0.28 | −0.29 | ||
| 0.02 | 0.01 | 0.01 | ||||
| Cord BALP 1 | - | −0.26 | −0.21 | |||
| 0.02 | 0.07 |

| African American (n = 40) | Non–African American (n = 40) | p–value | |||
|---|---|---|---|---|---|
| Mean (SD) 1 | Range | Mean (SD) 1 | Range | ||
| Gestational age at birth (weeks) | 39.7 (1.6) | 37.1–42.0 | 39.4 (1.1) | 37.1–41.3 | NS |
| Birth weight (g) | 3429 (512) | 2372–4532 | 3419 (526) | 2290–4460 | NS |
| Age at DXA scan (days) | 12.8 (3.4) | 8–21 | 13.4 (3.5) | 9–21 | NS |
| Maternal parity | 2.1 (1.2) | 1–5 | 1.8 (0.8) | 1–3 | NS |
| Maternal age (years) | 25.4 (5.2) | 18–39 | 28.3 (5.6) | 18–38 | 0.02 |
| Maternal BMI (kg/m2) 1 | 32.2 (29.6, 35.0) | 18.8–49.9 | 30.9 (28.3, 33.7) | 20.5–66.0 | NS |
| Maternal total vitamin D intake (IU/days) | 698 (246) | 0–1326 | 684 (253) | 184–1316 | NS |
| Maternal 25(OH)D (nmol/L) | 69.1 (26.1) | 33.5–118.5 | 82.3 (30.3) | 20.8–151.7 | 0.04 |
| Cord 25(OH)D 1,2 (nmol/L) | 36.0 (31.7, 40.8) | 16.7–87.5 | 48.2 (41.4, 56.1) | 14.1–157.5 | 0.004 |
| Maternal PTH (pg/mL) 1 | 29.4 (24.9, 34.8) | 9.5–66.1 | 29.3 (23.6, 36.4) | 6.2–102.0 | NS |
| Cord PTH (pg/mL) 1,2 | 6.1 (4.6, 8.0) | 2.0–50.7 | 3.7 (2.8, 4.7) | 2.0–82.5 | 0.009 |
| Cord BALP (U/L) 1 | 123.9 (112.2, 137.1) | 71.4–272.5 | 107.7 (98.4, 117.9) | 58.3–197.8 | 0.04 |
| WBBMC (g) | 61.3 (13.1) | 38.3–95.9 | 61.9 (12.1) | 35.4–83.3 | NS |
| WBBMC (g per (kg^1.31)) | 10.9 (0.9) | 9.1–12.7 | 11.4 (1.0) | 8.9–14.9 | 0.06 |
| N | % | n | % | p–value | |
| Sex | NS | ||||
| Male | 22 | 55 | 18 | 45 | |
| Female | 18 | 45 | 22 | 55 | |
| Race | N/A | ||||
| African American | 40 | 100 | 0 | – | |
| Hispanic | 0 | – | 12 | 30 | |
| Asian | 0 | – | 8 | 20 | |
| Caucasian | 0 | – | 4 | 10 | |
| Mixed/Other | 0 | – | 16 | 40 | |
| Maternal vitamin D supplementation | NS | ||||
| <400 IU/day | 7 | 17.5 | 11 | 27.5 | |
| ≥400 IU/day | 33 | 82.5 | 29 | 72.5 | |
| Feeding | NS | ||||
| Exclusively breast fed | 11 | 27.5 | 19 | 47.5 | |
| Exclusively formula fed | 13 | 32.5 | 6 | 15.0 | |
| Mixed | 16 | 40.00 | 15 | 37.5 | |
5. Discussion
6. Conclusion
Conflict of Interest
Acknowledgements
References
- Prentice, A. Milk intake, calcium and vitamin D in pregnancy and lactation: Effects on maternal, fetal and infant bone in low- and high-income countries. Nestle Nutr. Workshop Ser. Pediatr. Program. 2011, 67, 1–15. [Google Scholar] [CrossRef]
- Sahota, O.; Masud, T.; San, P.; Hosking, D.J. Vitamin D insufficiency increases bone turnover markers and enhances bone loss at the hip in patients with established vertebral osteoporosis. Clin. Endocrinol. (Oxf.) 1999, 51, 217–221. [Google Scholar] [CrossRef]
- Jones, G.; Dwyer, T.; Hynes, K.L.; Parameswaran, V.; Greenaway, T.M. Vitamin D insufficiency in adolescent males in Southern Tasmania: Prevalence, determinants, and relationship to bone turnover marker. Osteoporos Int. 2005, 16, 636–641. [Google Scholar] [CrossRef]
- Walker, V.P.; Modlin, R.L. The Vitamin D Connection to Pediatric Infections and Immune Function. Pediatr. Res. 2009, 65, 106–113. [Google Scholar] [CrossRef]
- Bringhurst, F.R.; Strewler, G.J. Renal and Skeletal Actions of Parathyroid Hormone (PTH) and PTH-Related Protein. In Principles of Bone Biology; Bilezikian, J.P., Raisz, L.G., Rodan, G.A., Eds.; Academic Press: San Diego, CA, USA, 2002; pp. 483–514. [Google Scholar]
- Mitchell, D.M.; Juppner, H. Regulation of calcium homeostasis and bone metabolism in the fetus and neonate. Curr. Opin. Endocrinol. Diabetes Obes. 2010, 17, 25–30. [Google Scholar]
- Sulaiman, R.A.; Sharratt, C.L.; Lee, P.W.; Skinner, A.; Griffiths, M.J.; Webster, C.; Ford, C.; Anderson, J.; Gama, R. Ethnic differences in umbilical cord blood vitamin D and parathyroid hormone—South Asians compared to Whites born in the UK. J. Matern. Fetal Neonatal Med. 2010, 23, 1315–1317. [Google Scholar] [CrossRef]
- Kovacs, C.S.; Kronenberg, H.M. Maternal-fetal calcium and bone metabolism during pregnancy, puerperium, and lactation. Endocr. Rev. 1997, 18, 832–872. [Google Scholar] [CrossRef]
- Miao, D.; He, B.; Karaplis, A.C.; Goltzman, D. Parathyroid hormone is essential for normal fetal bone formation. J. Clin. Invest. 2002, 109, 1173–1182. [Google Scholar]
- Risteli, J.; Kauppila, S.; Jukkola, A.; Marjoniemi, E.; Melkko, J.; Risteli, L. Biomarkers of bone formation. In Biomarkers of Disease: An Evidence-Based Approach; Trull, A.K., Demers, L.M., Holt, D.W., Johnston, A., Tredger, J.M., Price, C.P., Eds.; Cambridge University Press: Cambridge, UK, 2002; pp. 115–121. [Google Scholar]
- Calero, J.A.; Munoz, M.T.; Argente, J.; Traba, M.L.; Mendez-Davila, C.; Garcia-Moreno, C.; de la Piedra, C. A variation in Bone Alkaline Phosphatase levels that correlates positively with bone loss and normal levels of aminoterminal propeptide of collagen I in girls with anorexia nervosa. Clin. Chim. Acta 1999, 285, 121–129. [Google Scholar]
- Crofton, P.M.; Shrivastava, A.; Wade, J.C.; Stephen, R.; Kelnar, C.J.; Lyon, A.J.; McIntosh, N. Bone and collagen markers in preterm infants: relationship with growth and bone mineral content over the first 10 weeks of life. Pediatr. Res. 1999, 46, 581–587. [Google Scholar] [CrossRef]
- Ikeuchi, K.; Umesaki, N. Factors affecting bone mineral density of young women and predictive factors of low bone mineral density. Clin. Exp. Obstet. Gynecol. 2009, 36, 87–90. [Google Scholar]
- Viljakainen, H.T.; Saarnio, E.; Hytinantti, T.; Miettinen, M.; Surcel, H.; Makitie, O.; Andersson, S.; Laitinen, K.; Lamberg-Allardt, C. Maternal vitamin D status determines bone variables in the newborn. J. Clin. Endocrinol. Metab. 2010, 95, 1749–1757. [Google Scholar]
- Mahon, P.; Harvey, N.; Crozier, S.; Inskip, H.; Robinson, S.; Arden, N.; Swaminathan, R.; Cooper, C.; Godfrey, K. Low maternal vitamin D status and fetal bone development: Cohort study. J. Bone Miner. Res. 2010, 25, 14–19. [Google Scholar] [CrossRef]
- USDA National nutrient database for standard reference. Available online: http://www.nal.usda.gov/fnic/foodcomp/search (accessed on 20 January 2010).
- de Onis, M.; Onyango, A.W.; Van den Broeck, J.; Chumlea, W.C.; Martorell, R. Measurement and standardization protocols for anthropometry used in the construction of a new international growth reference. Food Nutr. Bull. 2004, 25, S27–S36. [Google Scholar]
- Dror, D.K.; Allen, L.H. Vitamin D inadequacy in pregnancy: Biology, outcomes, and intervention. Nutr. Rev. 2010, 68, 465–477. [Google Scholar] [CrossRef]
- Koo, W.W.; Bush, A.J.; Walters, J.; Carlson, S.E. Postnatal development of bone mineral status during infancy. J. Am. Coll. Nutr. 1998, 17, 65–70. [Google Scholar]
- Bodnar, L.M.; Catov, J.M.; Zmuda, J.M.; Cooper, M.E.; Parrott, M.S.; Roberts, J.M.; Marazita, M.L.; Simhan, H.N. Maternal serum 25-hydroxyvitamin D concentrations are associated with small-for-gestational age births in white women. J. Nutr. 2010, 140, 999–1006. [Google Scholar] [CrossRef]
- Swamy, G.K.; Garrett, M.E.; Miranda, M.L.; Ashley-Koch, A.E. Maternal vitamin D receptor genetic variation contributes to infant birthweight among black mothers. Am. J. Med. Genet. A 2011, 155, 1264–1271. [Google Scholar] [CrossRef]
- Ross, A.C.; Taylor, C.L.; Yaktine, A.L.; Del Valle, H.B. Dietary Reference Intakes for Calcium and Vitamin D; Institute of Medicine: Washington, DC, USA, 2010. [Google Scholar]
- Gopalakrishnan, R.; Ouyang, H.; Somerman, M.J.; McCauley, L.K.; Franceschi, R.T. Matrix gamma-carboxyglutamic acid protein is a key regulator of PTH-mediated inhibition of mineralization in MC3T3-E1 osteoblast-like cells. Endocrinology 2001, 142, 4379–4388. [Google Scholar]
- Gopalakrishnan, R.; Suttamanatwong, S.; Carlson, A.E.; Franceschi, R.T. Role of matrix Gla protein in parathyroid hormone inhibition of osteoblast mineralization. Cells Tissues Organs 2005, 181, 166–175. [Google Scholar]
- Schinke, T.; McKee, M.D.; Karsenty, G. Extracellular matrix calcification: where is the action? Nat. Genet. 1999, 21, 150–151. [Google Scholar] [CrossRef]
- Parfitt, A.M.; Qiu, S.; Rao, D.S. The mineralization index—A new approach to the histomorphometric appraisal of osteomalacia. Bone 2004, 35, 320–325. [Google Scholar] [CrossRef]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Dror, D.K.; King, J.C.; Fung, E.B.; Loan, M.D.V.; Gertz, E.R.; Allen, L.H. Evidence of Associations Between Feto-Maternal Vitamin D Status, Cord Parathyroid Hormone and Bone-Specific Alkaline Phosphatase, and Newborn Whole Body Bone Mineral Content. Nutrients 2012, 4, 68-77. https://doi.org/10.3390/nu4020068
Dror DK, King JC, Fung EB, Loan MDV, Gertz ER, Allen LH. Evidence of Associations Between Feto-Maternal Vitamin D Status, Cord Parathyroid Hormone and Bone-Specific Alkaline Phosphatase, and Newborn Whole Body Bone Mineral Content. Nutrients. 2012; 4(2):68-77. https://doi.org/10.3390/nu4020068
Chicago/Turabian StyleDror, Daphna K., Janet C. King, Ellen B. Fung, Marta D. Van Loan, Erik R. Gertz, and Lindsay H. Allen. 2012. "Evidence of Associations Between Feto-Maternal Vitamin D Status, Cord Parathyroid Hormone and Bone-Specific Alkaline Phosphatase, and Newborn Whole Body Bone Mineral Content" Nutrients 4, no. 2: 68-77. https://doi.org/10.3390/nu4020068