The Impact of Family History of Allergy on Risk of Food Allergy: A Population-Based Study of Infants


 , ,
, ,  and
and
Abstract
:1. Introduction
2. Methods
2.1. HealthNuts Study Methods
2.2. Statistical Analysis
2.3. Sensitivity Analysis
3. Results
3.1. Prevalence of Family History of Allergy in the Population

{kind=link}
| Family member | |||||
|---|---|---|---|---|---|
| Mother (n = 5,276) | Father (n = 5,276) | Brother (n = 1,556) | Sister (n = 1,475) | Any family member (n = 5,276) | |
| Any allergy | 44.2 | 37.9 | 37.5 | 35.7 | 69.4 |
| Allergic rhinitis | 30.7 | 27.2 | 9.6 | 6.9 | 50.0 |
| Asthma | 14.9 | 13.5 | 14.0 | 10.5 | 30.7 |
| Eczema | 14.1 | 7.6 | 24.4 | 24.3 | 30.5 |
| Any food allergy | 5.6 | 3.6 | 7.9 | 7.7 | 13.0 |
| Peanut allergy | 0.6 | 0.6 | 3.1 | 2.5 | 2.8 |
| Egg allergy | 0.3 | 0.3 | 2.4 | 2.1 | 1.8 |
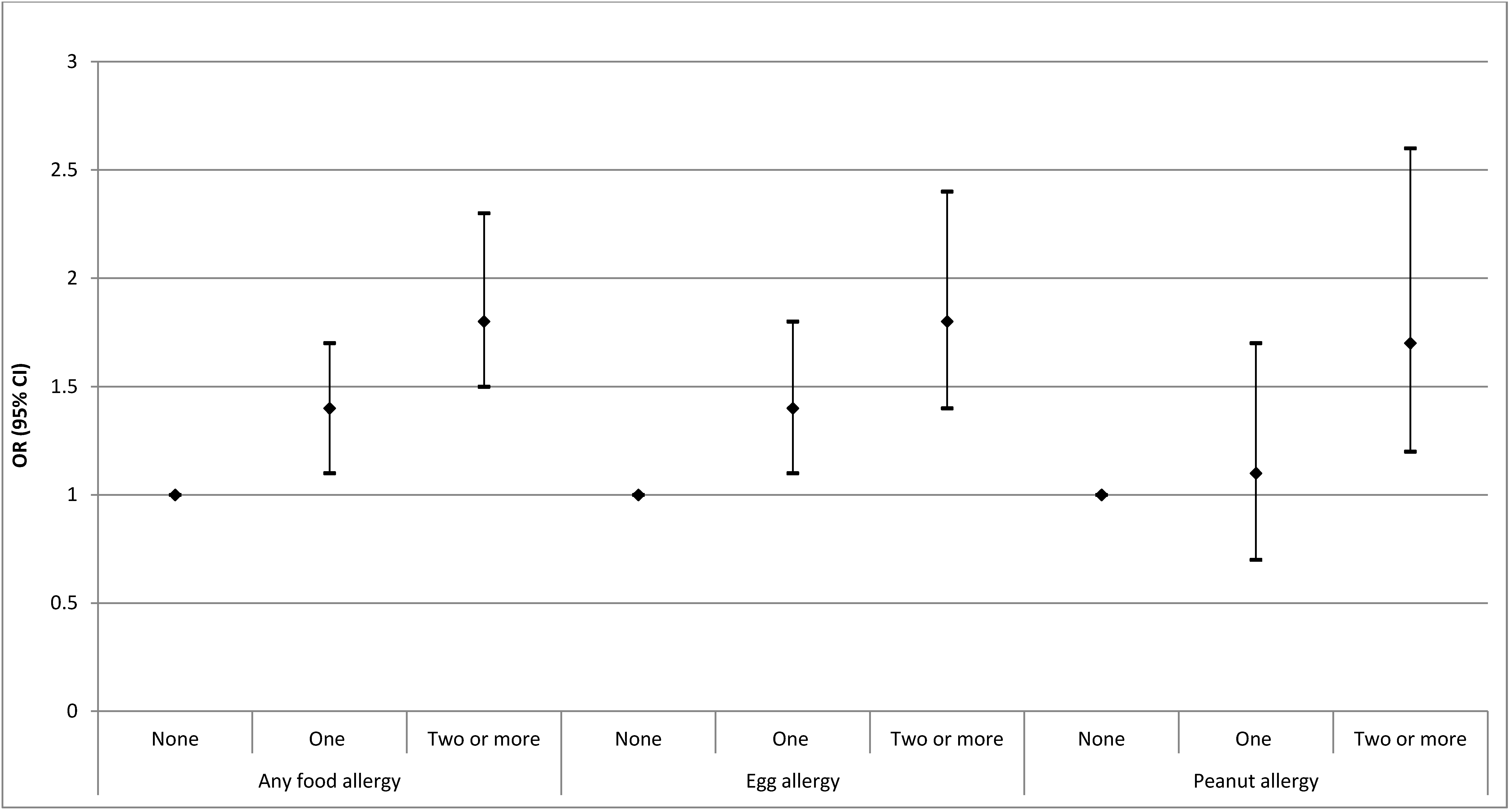
3.2. Risk of Food Allergy according to Number of Immediate Family Members with a History of Allergic Disease

3.3. Prevalence of Food Allergy according to Number of Immediate Family Members with Allergic Disease
3.4. Impact of Parental and Sibling Asthma, Allergic Rhinitis, Eczema and Food Allergy on Risk of Food Allergy in the Infant
| Does the infant have siblings? | Sibling history of allergy | Parent history of allergy | N | Any food allergy Prevalence (95% CI) | p value * | Egg allergy Prevalence (95% CI) | p value * | Peanut allergy Prevalence (95% CI) | p value * |
|---|---|---|---|---|---|---|---|---|---|
| No | - | None | 858 | 10.3 (8.2, 12.3) | - | 8.9 (7.0, 10.8) | - | 2.6 (1.5, 3.6) | - |
| No | - | One parent | 1,083 | 12.7 (10.8, 14.7) | 0.090 | 11.8 (9.9, 13.8) | 0.033 | 2.7 (1.7, 3.6) | 0.87 |
| No | - | Two parents | 482 | 16.0 (12.7, 19.3) | 0.002 | 13.9 (10.8, 17.0) | 0.005 | 4.0 (2.3, 5.7) | 0.14 |
| Yes | No | None | 648 | 5.6 (3.8, 7.3) | - | 4.6 (3.0, 6.2) | - | 2.2 (1.1, 3.4) | - |
| Yes | No | One parent | 650 | 7.8 (5.8, 9.9) | 0.10 | 6.4 (4.5, 8.2) | 0.15 | 2.9 (1.6, 4.1) | 0.47 |
| Yes | No | Two parents | 197 | 10.2 (5.9, 14.4) | 0.025 | 8.9 (4.9, 12.8) | 0.022 | 2.0 (0.04, 3.9) | 0.81 |
| Yes | Yes | None | 270 | 9.6 (6.1, 13.2) | - | 7.9 (4.7, 11.1) | - | 2.5 (0.7, 4.3) | - |
| Yes | Yes | One parent | 474 | 11.0 (8.1, 13.8) | 0.57 | 7.9 (5.5, 10.3) | 0.99 | 5.1 (3.1, 7.0) | 0.090 |
| Yes | Yes | Two parents | 225 | 20.0 (14.7, 25.3) | 0.001 | 19.1 (14.0, 24.3) | < 0.001 | 5.2 (2.3, 8.0) | 0.12 |
| Does the infant have siblings? | Sibling history of allergy | Parent history of allergy | N | Prevalence of food allergy among responders (95% CI) | Prevalence of food allergy, using sampling weights (95% CI) |
|---|---|---|---|---|---|
| No | - | None | 858 | 10.3 (8.2, 12.3) | 9.6 (7.5, 11.6) |
| No | - | One parent | 1,083 | 12.7 (10.8, 14.7) | 12.1 (10.1, 14.1) |
| No | - | Two parents | 482 | 16.0 (12.7, 19.3) | 14.6 (11.3, 17.9) |
| Yes | No | None | 689 | 5.6 (3.8, 7.3) | 5.0 (3.3, 6.8) |
| Yes | No | One parent | 684 | 7.8 (5.8, 9.9) | 7.6 (5.4, 9.7) |
| Yes | No | Two parents | 213 | 10.2 (5.9, 14.4) | 9.0 (4.9, 13.1) |
| Yes | Yes | None | 297 | 9.6 (6.1, 13.2) | 10.0 (6.3, 13.8) |
| Yes | Yes | One parent | 513 | 11.0 (8.1, 13.8) | 10.9 (7.9, 13.8) |
| Yes | Yes | Two parents | 251 | 20.0 (14.7, 25.3) | 18.0 (12.7, 23.4) |
| Egg allergy | Peanut allergy | |||||||
|---|---|---|---|---|---|---|---|---|
| Crude multivariable model * | Adjusted for confounders † | Crude multivariable model * | Adjusted for confounders † | |||||
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Maternal allergy | ||||||||
| Food Allergy (n = 297) | 0.76 (0.50, 1.16) | 0.21 | 0.65 (0.41, 1.04) | 0.075 | 0.46 (0.18, 1.14) | 0.092 | 0.35 (0.12, 0.97) | 0.044 |
| Eczema (n = 742) | 1.65 (1.28, 2.12) | <0.001 | 1.57 (1.20, 2.04) | 0.001 | 1.31 (0.85, 2.03) | 0.22 | 1.27 (0.81, 2.00) | 0.30 |
| Allergic rhinitis alone (n = 1,167) | 1.22 (0.97, 1.55) | 0.088 | 1.27 (0.99, 1.63) | 0.052 | 1.18 (0.79, 1.77) | 0.42 | 1.26 (0.83, 1.92) | 0.28 |
| Asthma alone (n = 377) | 1.41 (0.98, 2.03) | 0.066 | 1.54 (1.05, 2.26) | 0.027 | 1.33 (0.71, 2.51) | 0.37 | 1.48 (0.76, 2.86) | 0.25 |
| Allergic rhinitis + asthma (n = 450) | 1.23 (0.87, 1.73) | 0.24 | 1.30 (0.91, 1.86) | 0.15 | 1.97 (1.18, 3.28) | 0.009 | 2.35 (1.39, 3.96) | 0.001 |
| Paternal allergy | ||||||||
| Food Allergy (n = 192) | 0.89 (0.53, 1.50) | 0.67 | 0.77 (0.44, 1.36) | 0.37 | 0.87 (0.35, 2.18) | 0.77 | 0.72 (0.26, 2.01) | 0.54 |
| Eczema (n = 401) | 1.52 (1.10, 2.09) | 0.011 | 1.35 (0.96, 1.90) | 0.086 | 0.82 (0.43, 1.56) | 0.55 | 0.76 (0.39, 1.49) | 0.42 |
| Allergic rhinitis alone (n = 1,047) | 1.20 (0.94, 1.52) | 0.14 | 1.21 (0.94, 1.56) | 0.13 | 1.28 (0.86, 1.91) | 0.23 | 1.28 (0.85, 1.93) | 0.25 |
| Asthma alone (n = 326) | 1.09 (0.73, 1.63) | 0.67 | 1.21 (0.80, 1.82) | 0.37 | 0.71 (0.31, 1.64) | 0.42 | 0.77 (0.33, 1.79) | 0.54 |
| Allergic rhinitis + asthma (n = 388) | 1.21 (0.85, 1.72) | 0.29 | 1.14 (0.79, 1.67) | 0.48 | 1.90 (1.13, 3.21) | 0.016 | 1.77 (1.01, 3.09) | 0.045 |
| Siblings | ||||||||
| Food Allergy (n = 240) | 1.68 (1.08, 2.62) | 0.023 | 1.25 (0.77, 2.05) | 0.36 | 0.97 (0.45, 2.10) | 0.94 | 0.78 (0.34, 1.79) | 0.56 |
| Eczema (n = 740) | 1.31 (0.94, 1.83) | 0.11 | 1.26 (0.89, 1.78) | 0.20 | 1.34 (0.81, 2.19) | 0.25 | 1.23 (0.73, 2.06) | 0.44 |
| Allergic rhinitis alone (n = 157) | 1.93 (1.15, 3.24) | 0.013 | 2.45 (1.45, 4.17) | 0.001 | 1.42 (0.62, 3.23) | 0.41 | 1.65 (0.71, 3.82) | 0.24 |
| Asthma alone (n = 302) | 1.44 (0.94, 2.22) | 0.095 | 1.56 (1.00, 2.43) | 0.051 | 1.52 (0.82, 2.81) | 0.19 | 1.59 (0.85, 3.00) | 0.15 |
| Allergic rhinitis + asthma (n = 78) | 1.34 (0.61, 2.97) | 0.47 | 1.66 (0.74, 3.71) | 0.21 | 0.32 (0.04, 2.43) | 0.27 | 0.35 (0.05, 2.65) | 0.31 |
4. Discussion
5. Conclusions
Acknowledgments
Conflicts of Interest
References
- Prescott, S.; Allen, K.J. Food allergy: Riding the second wave of the allergy epidemic. Pediatr. Allergy Immunol. 2011, 22, 155–160. [Google Scholar] [CrossRef]
- Tsai, H.-J.; Kumar, R.; Pongracic, J.; Liu, X.; Story, R.; Yu, Y.; Caruso, D.; Costello, J.; Schroeder, A.; Fang, Y.; et al. Familial aggregation of food allergy and sensitization to food allergens: A family-based study. Clin. Exp. Allergy 2009, 39, 101–109. [Google Scholar] [CrossRef]
- Sicherer, S.H.; Furlong, T.J.; Maes, H.H.; Desnick, R.J.; Sampson, H.A.; Gelb, B.D. Genetics of peanut allergy: A twin study. J. Allergy Clin. Immunol. 2000, 106, 53–56. [Google Scholar] [CrossRef]
- Osborne, N.J.; Koplin, J.J.; Martin, P.E.; Gurrin, L.C.; Thiele, L.; Tang, M.L.; Ponsonby, A.-L.; Dharmage, S.C.; Allen, K.J.; for the HealthNuts Study Investigators. The HealthNuts population-based study of paediatric food allergy: Validity, safety and acceptability. Clin. Exp. Allergy 2010, 40, 1516–1522. [Google Scholar] [CrossRef]
- Koplin, J.J.; Tang, M.L.K.; Martin, P.E.; Osborne, N.J.; Lowe, A.J.; Ponsonby, A.-L.; Robinson, M.N.; Tey, D.; Thiele, L.; Hill, D.J.; et al. Predetermined challenge eligibility and cessation criteria for oral food challenges in the HealthNuts population-based study of infants. J. Allergy Clin. Immunol. 2012, 129, 1145–1147. [Google Scholar] [CrossRef]
- Koplin, J.J.; Dharmage, S.C.; Ponsonby, A.-L.; Tang, M.L.K.; Lowe, A.J.; Gurrin, L.C.; Osborne, N.J.; Martin, P.E.; Robinson, M.N.; Wake, M.; et al. Environmental and demographic risk factors for egg allergy in a population-based study of infants. Allergy 2012, 67, 1415–1422. [Google Scholar] [CrossRef]
- Hopper, J.L.; Bui, Q.M.; Erbas, B.; Matheson, M.C.; Gurrin, L.C.; Burgess, J.A.; Lowe, A.J.; Jenkins, M.A.; Abramson, M.J.; Walters, E.H.; et al. Does eczema in infancy cause hay fever, asthma, or both in childhood? Insights from a novel regression model of sibling data. J. Allergy Clin. Immunol. 2012, 130, 1117–1122.e1. [Google Scholar] [CrossRef]
- Koplin, J.J.; Osborne, N.J.; Wake, M.; Martin, P.E.; Gurrin, L.C.; Robinson, M.N.; Tey, D.; Slaa, M.; Thiele, L.; Miles, L.; et al. Can early introduction of egg prevent egg allergy in infants? A population-based study. J. Allergy Clin. Immunol. 2010, 126, 807–813. [Google Scholar] [CrossRef]
- Osborne, N.J.; Koplin, J.J.; Martin, P.E.; Gurrin, L.C.; Lowe, A.J.; Matheson, M.C.; Ponsonby, A.-L.; Wake, M.; Tang, M.L.K.; Dharmage, S.C.; et al. Prevalence of challenge-proven IgE-mediated food allergy using population-based sampling and predetermined challenge criteria in infants. J. Allergy Clin. Immunol. 2011, 127, 668–676.e2. [Google Scholar] [CrossRef]
- Little, R.J.A.; Rubin, J. Statistical Analysis with Missing Data, 2nd ed.; John Wiley & Sons Inc: Hoboken, NJ, USA, 2002. [Google Scholar]
- Allen, K.J.; Koplin, J.J.; Ponsonby, A.L.; Gurrin, L.C.; Wake, M.; Vuillermin, P.; Martin, P.; Matheson, M.; Lowe, A.; Robinson, M.; et al. Vitamin D insufficiency is associated with challenge-proven food allergy in infants. J. Allergy Clin. Immunol. 2013, 131, 1109–1116.e6. [Google Scholar] [CrossRef]
- Martin, P.E.; Koplin, J.J.; Eckert, J.K.; Lowe, A.J.; Ponsonby, A.-L.; Osborne, N.J.; Gurrin, L.C.; Robinson, M.N.; Hill, D.J.; Tang, M.L.K.; et al. The prevalence and socio-demographic risk factors of clinical eczema in infancy: A population-based observational study. Clin. Exp. Allergy 2013, 43, 642–651. [Google Scholar]
- Kim, J.; Chang, E.; Han, Y.; Ahn, K.; Lee, S.-I. The incidence and risk factors of immediate type food allergy during the first year of life in Korean infants: A birth cohort study. Pediatr. Allergy Immunol. 2011, 22, 715–719. [Google Scholar] [CrossRef]
- Lao-araya, M.; Trakultivakorn, M. Prevalence of food allergy among preschool children in northern Thailand. Pediatr. Int. 2012, 54, 238–243. [Google Scholar] [CrossRef]
- Pyrhonen, K.; Hiltunen, L.; Kaila, M.; Nayha, S.; Laara, E. Heredity of food allergies in an unselected child population: An epidemiological survey from Finland. Pediatr. Allergy Immunol. 2011, 22, e124–e132. [Google Scholar] [CrossRef]
- Lack, G.; Fox, D.; Northstone, K.; Golding, J. Factors associated with the development of peanut allergy in childhood. N. Engl. J. Med. 2003, 348, 977–985. [Google Scholar] [CrossRef]
- Goldberg, M.; Eisenberg, E.; Elizur, A.; Rajuan, N.; Rachmiel, M.; Cohen, A.; Zadik-Mnuhin, G.; Katz, Y. Role of parental atopy in cow’s milk allergy: A population-based study. Ann. allergy, asthma & immunol. 2013, 110, 279–283. [Google Scholar]
- Longo, G.; Berti, I.; Burks, A.W.; Krauss, B.; Barbi, E. IgE-mediated food allergy in children. Lancet 2013. [Google Scholar] [CrossRef]
- Dang, T.D.; Tang, M.L.K.; Koplin, J.J.; Licciardi, P.V.; Eckert, J.K.; Tan, T.; Gurrin, L.C.; Ponsonby, A.-L.; Dharmage, S.C.; Allen, K.J. Characterization of plasma cytokines in an infant population cohort of challenge-proven food allergy. Allergy 2013. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Koplin, J.J.; Allen, K.J.; Gurrin, L.C.; Peters, R.L.; Lowe, A.J.; Tang, M.L.K.; Dharmage, S.C.; Team, T.H.S. The Impact of Family History of Allergy on Risk of Food Allergy: A Population-Based Study of Infants. Int. J. Environ. Res. Public Health 2013, 10, 5364-5377. https://doi.org/10.3390/ijerph10115364
Koplin JJ, Allen KJ, Gurrin LC, Peters RL, Lowe AJ, Tang MLK, Dharmage SC, Team THS. The Impact of Family History of Allergy on Risk of Food Allergy: A Population-Based Study of Infants. International Journal of Environmental Research and Public Health. 2013; 10(11):5364-5377. https://doi.org/10.3390/ijerph10115364
Chicago/Turabian StyleKoplin, Jennifer J., Katrina J. Allen, Lyle C. Gurrin, Rachel L. Peters, Adrian J. Lowe, Mimi L. K. Tang, Shyamali C. Dharmage, and The HealthNuts Study Team. 2013. "The Impact of Family History of Allergy on Risk of Food Allergy: A Population-Based Study of Infants" International Journal of Environmental Research and Public Health 10, no. 11: 5364-5377. https://doi.org/10.3390/ijerph10115364
APA StyleKoplin, J. J., Allen, K. J., Gurrin, L. C., Peters, R. L., Lowe, A. J., Tang, M. L. K., Dharmage, S. C., & Team, T. H. S. (2013). The Impact of Family History of Allergy on Risk of Food Allergy: A Population-Based Study of Infants. International Journal of Environmental Research and Public Health, 10(11), 5364-5377. https://doi.org/10.3390/ijerph10115364