Overview of Evidence in Prevention and Aetiology of Food Allergy: A Review of Systematic Reviews



Abstract
:1. Introduction
- (1)
- The direct effect of allergens introduced into infant and maternal diets at specific times and principally whether earlier introduction promotes the development of tolerance in a maturing immune system or the development of allergy;
- (2)
- The role of environmental microbiota in the normal education of the immune system, whereby it is thought that the normal immune system requires the presence of a diverse microbiota in early life for the development of tolerance and a western lifestyle limits exposure to these necessary microbiota (the hygiene hypothesis);
- (3)
- Other lifestyle factors including the effects of vitamin D and environmental pollution on the immune system.
2. Experimental Section
2.1. Eligibility Criteria
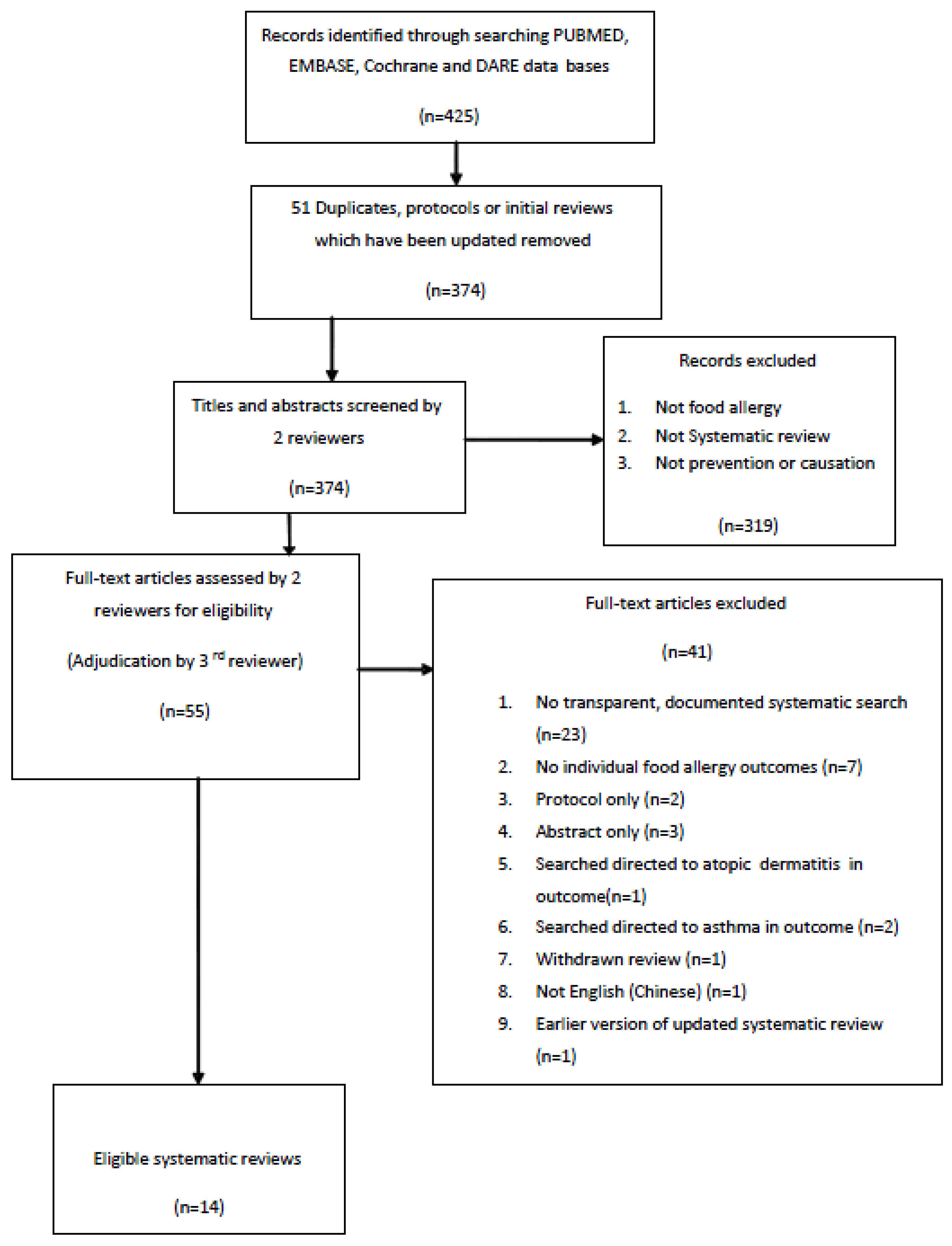
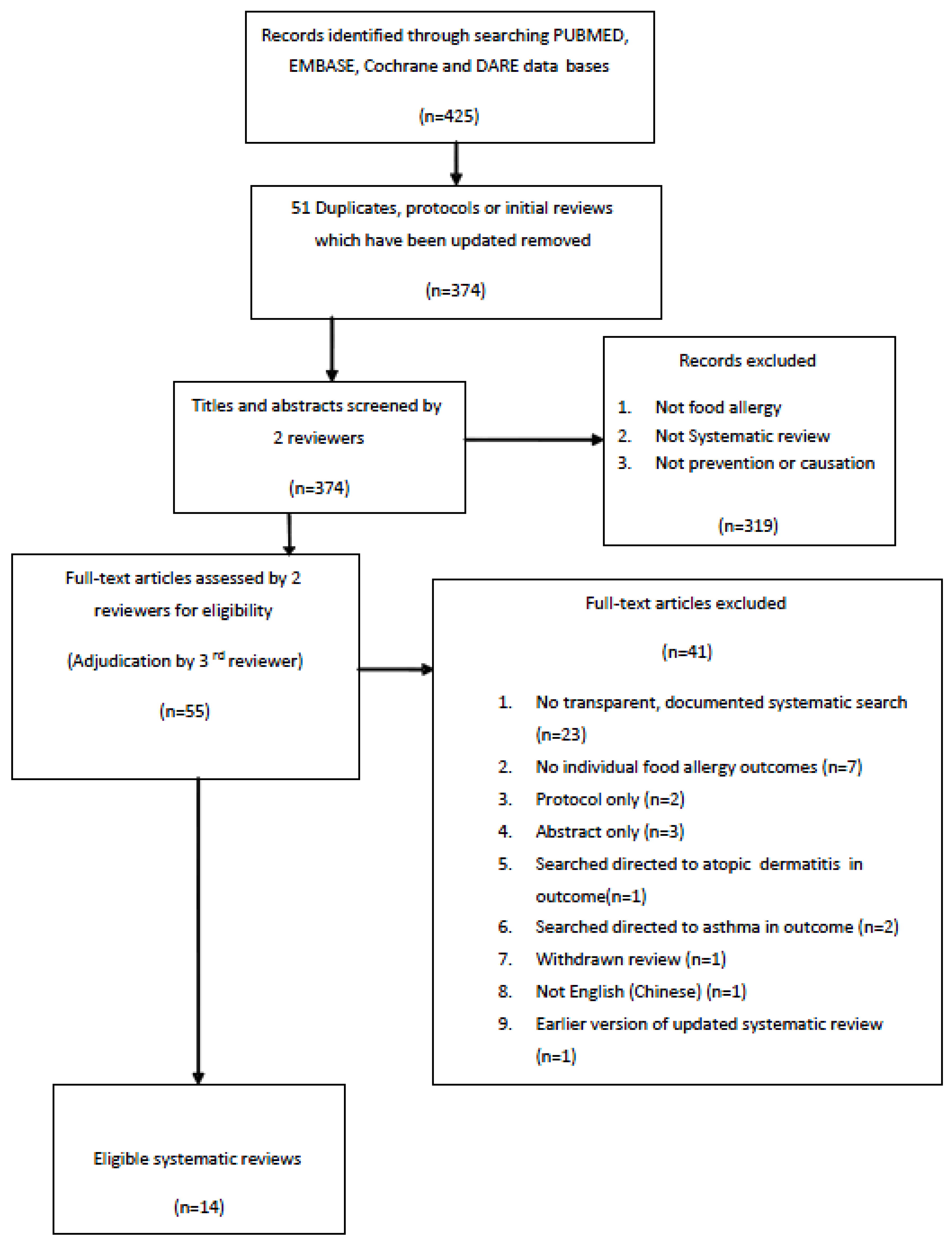
2.2. Search Strategy
2.3. Selection of Reviews
2.4. Assessment of the Quality of the Systematic Reviews
2.5. Analysis
3. Results and Discussion
3.1. Results
- (1)
- Formula (hydrolysed or soy) for the prevention of food allergy or food sensitization.
- (2)
- Maternal and infant diet and dietary supplements for the prevention of food allergy or food sensitization:
- Introduction of solids or allergenic solids in infants and/or mothers diet.
- Probiotics and omega-3 supplements to mother and infant.
- (3)
- Hygiene hypothesis related interventions:
- Infant immunisation and its impact on immune deviation and food allergy/food sensitization development.
- Delivery by caesarean section.
3.1.1. Formula for Prevention

{kind=link}
| First author (year) AMSTAR quality Meta-analysis (MA)+ or − | Designs of the studies included in each review and search dates | Intervention/s/comparisons | Population/s studied | Outcome/s measured | Main Results | Authors’ Conclusion/s |
|---|---|---|---|---|---|---|
| Szajewska (2010) [74] Quality: High (9) MA− | 1 RCT 1985–2010 | Partially hydrolysed 100% whey formula (pHF) vs. Standard infant formula (StF) | High Allergy risk Infants with at least 2 first degree relatives with allergy whose mothers decided not to breastfeed | Food Allergy (FA) at 6 months. Food Allergy—not defined in SR. Source papers—symptoms suggestive of cow’s milk allergy such as diarrhoea and colic. | RR 0.36, 95% CI (0.15, 0.89) (1 study (n = 67) | Results indicate that pHF is effective in prevention of symptoms of possible CMA compared to StF ☺ |
| Osborn (2006) [70] update (2009) * Quality: High (11) MA− | 1 RCT Search 1980–2006 Included only trials with greater than 80% follow up | Soy Formula vs. Cow’s milk formula | High Allergy risk Children with biparental history of allergic disease | Food Allergy Not defined in SR. Source papers—Not clear—GI symptoms and IgE characterized as Obvious, Probable or possible atopic disease Cow’s Milk protein intolerance (CMPI) Soy protein allergy (SPA) Cow’s milk allergy (CMA) | CMPI RR = 1.09 (0.45, 2.62) SPA RR = 3.26 (0.36, 29.17) CMA RR 1.09 (0.45, 4.86) All results from 1 study (n = 50) | Feeding with soy formula cannot be recommended for primary prevention for infants at high risk of allergy or food intolerance 😐 |
| Osborn (2006) * [71] Quality: High (11) MA− | 5 RCTs Updated search March 2009 Included only trials with greater than 80% follow up | Hydrolysed infant formula vs. human milk or cow’s milk formula AND Partially hydrolysed vs. extensively hydrolysed cow’s milk | High Allergy Risk (3 studies) 2 studies biparental atopy or uniparental atopy with raised cord IgE 1 study at least 1 first degree relative Population based (2 studies) Updated search March 2009 | Food Allergy/CMA1 study unknown 2 studies unblinded food elimination/challenge 2 studies used symptoms with specific IgE | 1. Short term studies (2): 1.1 Hydrolysed vs. human milk CMA RR 7.11, 0.35, 143.84 (n = 90) RR 0.87, 0.52, 1.46 (n = 3,559) Food Allergy RR 1.43, 0.38, 5.37 (n = 90) 1.2 Hydrolysed vs. cow’s milk CMA RR 5.13, 0.25, 103.43 (n = 90) RR 0.62, 0.38, 1.00 (n = 3,559) Food Allergy RR 1.37, 0.33, 5.71 (n = 90) 2. Long-term studies (3) 2.1 Hydrolysed vs. cows CMA RR 0.36, 0.15, 0.89 (n = 67) Food Allergy RR 1.82, 0.64, 5.16(n = 141) 2.2 Extensive vs. partial hydrolysed CMA RR 0.13, 0.01, 1.16 (n = 246) Food Allergy RR 0.43, 0.19, 0.99 (n = 341) | No evidence to support feeding with hydrolysed formula for prevention of allergy compared to breastfeeding. 😐 In high-risk infants unable to be breast fed limited evidence of allergy and CMA reduction. ☺ Need further trials |
| Hays (2005) [72] Quality: Low (2) MA− | RCTs 22 studies | Comparison of hydrolysed formulas with: breastfeeding, cow’s milk formula, soy formula or combinations | High Allergy Risk (22) Population based (1) | Atopy Not defined in SR. Source papers—seems largely based on objective measure in the presence of GI symptoms—open food challenge, DBPCFC, SPT IgE | High-risk infants demonstrate significant reductions in the cumulative incidence of atopic disease through the first 1 to 5 years of life compared with feeding CMF. (no pooled results) | Formulas seem effective but better measures food allergy needed to confirm ☺ |
| Schoetzau (2001) [73] Quality: Medium (5) MA− | RCTs Prospective Cohorts 3 studies up to 2001 ‡ | Comparison of hydrolysed formulas vs. cow’s milk formula | High Allergy Risk | Food allergy: based on strict, well-defined food elimination and challenge procedures including double-blind placebo controlled food challenge. | Food allergy 0.50 (0.04; 5.72) (1 study, n = 91) Sensitization to cow’s milk: (1 study, n = 91) 9 months 0.19 (0.02; 1.66) 18 Months 0.26 (0.05; 1.32) (1 study, n = 67) 6 months 0.07 (0.00; 1.29) 12 months 0.05 (0.00;1.01) | The lack of statistical power of these studies means that more studies will have to be conducted to determine the effect of hydrolysed formulas and allergy 😐 |
3.1.2. Maternal and Infant Diet and Dietary Supplements
| First Author (Year) AMSTAR Quality Meta-analysis MA (+or −) | Study Design/s included in review Search dates | Intervention/s and comparisons | Population/s studied | Outcome measures | Main results | Authors’ Conclusions |
|---|---|---|---|---|---|---|
| Klemens (2011) [79] Quality: Medium MA+ | RCT 3 studies 1950–2010 | Omega-3 (n-3 PUFA) supplementation during pregnancy and/or lactation vs. placebo (olive or soy oil) | High Allergy Risk & Population based | Egg Allergy; Skin prick test Food Allergy; Clinical diagnosis | Egg SPT up to 12 months reduced—OR 0.33 (0.16, 0.70) (187 children from 2 studies) Food Allergy up to 12 or 30 months—OR 0.46 (0.16, 1.38) (264 children from 3 studies) Supplementation started in pregnancy Food Allergy (2 studies on 200 children)—OR 0.34 (95% CI 0.10, 1.15) | n-3 PUFU protective against egg sensitization ☺ but no reduction in food allergy risk 😐 |
| Anandan (2009) [78] Quality: Medium MA+ | RCT 2 studies 1966–2008 | Omega-3 (n-3 PUFU) supplementation during pregnancy and/or lactation vs. placebo (olive oil) | High Allergy Risk & Population based | Food Allergy—Not defined in SR. Source papers—not clear in one study and clinical diagnosis in other. | Food Allergy up to 12 or 30 months RR 0.51 (0.10, 2.55) (148 children from 2 studies) | A non-significant risk reduction in those receiving n-3 PUFU supplements compared to placebo 😐 |
| Osborn (2007) * [67] Quality: High MA+ | 2 RCT & Quasi RCT 1966–2007 | Probiotics (various types and mixtures) vs. no probiotics given to infants | High Allergy Risk & Population based | Food Allergy History of immediate symptoms on food exposure and specific SPT Cow’s Milk Allergy DBPCFC (if suggestive symptoms, signs or SPT) | Food Allergy RR 1.54 (0.70, 3.37) (175 children from 1 high risk allergy study using Lactobacillus acidophilus) Cow’s Milk Allergy RR 0.41 (0.02, 9.84) (72 children from 1 population based study using Lactobacillus rhamanosus) | Insufficient evidence to recommend probiotics as a preventative measure for food allergy. 😐 |
| Kramer (2012) * [80] Quality: High MA+ | 3 RCT & Quasi RCT 6 July 2012 | Maternal dietary antigen avoidance diet (different regimens) during third trimester of pregnancy (2 studies, n = 383) , and pregnancy and lactation (1 study n = 497) | High Allergy risk | Sensitization Skin prick tests for cow’s milk, egg and peanut allergy at ages 6 months, 1, 2 and 7 years | Many SPTs showed no evidence of association. Those of note: Avoidance during pregnancy: Infant egg sensitization at 6 mo RR 0.58 (0.32, 1.05) in 2 studies (n = 340) Avoidance during pregnancy and lactation Child egg sensitization at 2 years RR 1.91 (1.03, 3.53) in 1 study (n = 497) Child milk sensitization at 2 years RR 4.30 (0.94, 19.67) in 1 study (n = 473) | No significant effect of maternal antigen avoidance on skin prick tests in infant or child 😐 |
| Thompson (2010) [82] AMSTAR Quality: Medium MA− | 2 RCTs, 2 case controls 1999–2008 | Mother’s exposure to peanut (more or less than once per week) Childs exposure to peanut RCT—Exclusion diets | High Allergy risk & population based CC—2 studies of total 48 peanut allergic and 228 controls RCT—2 studies of total 685 full-term newborns | Sensitization or clinical peanutallergy Peanut-specific skin prick tests and peanut-specific IgE. Also DBPCFC was used to measure peanut allergy | Due to heterogeneous nature and the small number of studies pooling results was not possible, None of the individual results reported by any of the studies showed any significant association between peanut consumption and food allergy or sensitization | Maternal exposure or introduction time of peanuts in a child’s life appears to have no effect on peanut allergy 😐 |
| Tarini (2006) [81] AMSTAR Quality: Low MA− | 1 Prospective cohort study 1966–2005 | Exclusive breastfeeding for 6 months (n = 70) vs. introduction solids at 3 months(n = 65) | High Allergy risk | Food allergy—defined as: history of skin rash or heavy vomiting after ingestion of food by 1 year At 5 years food allergy was defined as the above plus positive skin prick test | 37% of infants fed solids at 3 months of age had a history of food allergy up to the age of 1 compared to 7% who were fed breast milk exclusively (p < 0.001) At 5 years no difference between the two groups | Early solid feeding appears to have no association with food allergy 1 year result due to poor definition of food allergy 😐 |
- Timing of solids and allergenic solids for prevention and maternal exposure to allergens.Three systematic reviews assessed the role of ingested allergenic foods in mothers and children’s diets and all reached similar conclusions [80,81,82]. One review synthesized the information from three Randomized Controlled Trials (RCTS) concerning the influence of maternal diet during pregnancy and lactation on sensitization in infants and children, finding no relationship between the avoidance of allergenic foods in the maternal diet and sensitization in the child [80]. A second review incorporated two RCTs and two case control studies assessing the role of peanut ingestion in mothers and children, finding no increase in the risk of peanut allergy or sensitization associated with either child or maternal peanut intake [82]. The third review included one cohort study of 135 children and found no difference in the risk of food allergy at the age of 5 years (symptoms plus positive SPT) when comparing infants exclusively breast fed for the first 6 months, to breast fed infants who had solids introduced at 3 months [81]. None of these reviews contributed any evidence concerning whether introducing foods under the cover of breast feeding had an impact on sensitization and food allergy.
- Dietary supplements for prevention (omega 3 and pre/probiotics).There were two reviews of RCTs for early life oral interventions using omega-3 polyunsaturated fatty acids (3-PUFA), which were of intermediate quality [78,79]. Both these reviews included the same two original studies [83,84] except that the more recent review incorporated a third study [85]. Both reviews found no association of 3-PUFA supplementation with the risk of food allergy defined as a clinical diagnosis. The more recent review [79] however found a reduced risk for egg sensitization in infancy for those supplemented with 3-PUFA (OR 0.33 (95% CI 0.16, 0.70)) from two studies n = 187.One high quality systematic review which summarized RCTs on probiotic supplementation [67], found no association between supplementation and the risk of food allergy, defined by symptoms on food exposure with positive specific SPT (1 study, n = 175) or cow’s milk allergy, defined using double blind placebo controlled food challenge (1 study, n = 72). These results however were based on only 247 children from two different studies in which different lactobacillus species were used.
3.1.3. Hygiene Hypothesis Related Interventions
| First Author (Year) AMSTAR Quality Meta-analysis MA (+ or −) | Study Designs included in review & search dates | Population/s studied and numbers | Intervention/s and comparisons | Outcome measures | Main results | Authors’ Conclusions |
|---|---|---|---|---|---|---|
| Arnoldussen (2011) [86] Quality: Medium MA− | 1 Randomized prospective single blind study 1 Retrospective Cohort study No search dates stated | High allergy risk RCT- BCG = 62 Placebo = 59 Cohort- Atopic hereditary children 216 cases, 358 controls | BCG vaccination | Food allergy: Symptoms of allergy (skin reactions, wheezing, vomiting, or diarrhoea) on more than one occasion after ingestion or contact with a particular type of food or allergen (1 study) Symptoms of feeding induced vomiting diarrhoea or abdominal pain (1 study) | Results not pooled because outcomes were judged to be too heterogeneous on clinical grounds Neither study individually showed a significant association with food allergy | No protective effect of BCG vaccination on the development of food allergy 😐 |
| Bager (2008) [87] Quality: Medium MA+ | 6 Cohort studies Between 1966 & 1 May 2007 | 32,565 children aged 0–17 Populations not defined | Delivery by C-section | Food Allergy/Atopy: Hospital admission for food anaphylaxis or epipen prescription (age 0–6) (1 study) Physician diagnosis (age 8–17) (1 study) Parent or self report to foods or drugs (age 3–17) (1 study) Parent or self report to egg, fish or nuts (age 1–2) (1 study) Raised specific IgE to food (age 1–2) (2 studies) | Food allergy or Food atopy OR 1.32 (95% CI 1.12, 1.55) (6 studies (n = 32,565)) | C-section may be associated with increases risk of food allergy. ☹ Results may have been affected by publication bias. |
| Koplin (2008) [88] Quality: Medium MA− | 3 Prospective Cohorts 1 Retrospective cohort Published before July 2007 | Population based (3) and High Allergy risk (1) 15,121 children | Delivery by C-Section | Food Allergy: Symptoms of food allergy Sensitization: IgE antigen-specific levels | Results were not pooled due to small number of papers included in study | C-section may result in an increased risk of IgE-mediated sensitization ☹ |
Infant Immunisation
Caesarean Section
3.2. Discussion
3.2.1. Infant Formulas
3.2.2. Diet and Dietary Supplements
3.2.3. Hygiene Hypothesis Related Interventions
3.2.4. Major Limitations of Included Systematic Reviews
4. Conclusions
Acknowledgments
Conflicts of Interest
References
- Pumphrey, R.S.; Gowland, M.H. Further fatal allergic reactions to food in the United Kingdom, 1999–2006. J. Allergy Clin. Immunol. 2007, 119, 1018–1019. [Google Scholar] [CrossRef]
- Yocum, M.W.; Butterfield, J.H.; Klein, J.S.; Volcheck, G.W.; Schroeder, D.R.; Silverstein, M.D. Epidemiology of anaphylaxis in Olmsted County: A population-based study. J. Allergy Clin. Immunol. 1999, 104, 452–456. [Google Scholar] [CrossRef]
- Poulos, L.M.; Waters, A.M.; Correll, P.K.; Loblay, R.H.; Marks, G.B. Trends in hospitalizations for anaphylaxis, angioedema, and urticaria in Australia, 1993–1994 to 2004–2005. J. Allergy Clin. Immunol. 2007, 120, 878–884. [Google Scholar] [CrossRef]
- Liew, W.K.; Williamson, E.; Tang, M.L. Anaphylaxis fatalities and admissions in Australia. J. Allergy Clin. Immunol. 2009, 123, 434–442. [Google Scholar] [CrossRef]
- Osborne, N.J.; Koplin, J.J.; Martin, P.E.; Gurrin, L.C.; Lowe, A.J.; Matheson, M.C.; Ponsonby, A.L.; Wake, M.; Tang, M.L.; Dharmage, S.C.; et al. Prevalence of challenge-proven IgE-mediated food allergy using population-based sampling and predetermined challenge criteria in infants. J. Allergy Clin. Immunol. 2011, 127, 668–676. [Google Scholar] [CrossRef]
- Rona, R.J.; Keil, T.; Summers, C.; Gislason, D.; Zuidmeer, L.; Sodergren, E.; Sigurdardottir, S.T.; Lindner, T.; Goldhahn, K.; Dahlstrom, J.; et al. The prevalence of food allergy: A meta-analysis. J. Allergy Clin. Immunol. 2007, 120, 638–646. [Google Scholar] [CrossRef]
- Burks, A.W.; Tang, M.; Sicherer, S.; Muraro, A.; Eigenmann, P.A.; Ebisawa, M.; Fiocchi, A.; Chiang, W.; Beyer, K.; Wood, R.; et al. ICON: Food allergy. J. Allergy Clin. Immunol. 2012, 129, 906–920. [Google Scholar]
- Ho, M.H.; Wong, W.H.; Heine, R.G.; Hosking, C.S.; Hill, D.J.; Allen, K.J. Early clinical predictors of remission of peanut allergy in children. J. Allergy Clin. Immunol. 2008, 121, 731–736. [Google Scholar] [CrossRef]
- Allen, K.J.; Dharmage, S.C. The role of food allergy in the atopic march. Clin. Exp. Allergy 2010, 40, 1439–4141. [Google Scholar] [CrossRef]
- Sicherer, S.H.; Furlong, T.J.; Maes, H.H.; Desnick, R.J.; Sampson, H.A.; Gelb, B.D. Genetics of peanut allergy: A twin study. J. Allergy Clin. Immunol. 2000, 106, 53–56. [Google Scholar] [CrossRef]
- Zuidmeer, L.; Goldhahn, K.; Rona, R.J.; Gislason, D.; Madsen, C.; Summers, C.; Sodergren, E.; Dahlstrom, J.; Lindner, T.; Sigurdardottir, S.T.; et al. The prevalence of plant food allergies: A systematic review. J. Allergy Clin. Immunol. 2008, 121, 1210–1218. [Google Scholar]
- Chafen, J.J.; Newberry, S.J.; Riedl, M.A.; Bravata, D.M.; Maglione, M.; Suttorp, M.J.; Sundaram, V.; Paige, N.M.; Towfigh, A.; Hulley, B.J.; et al. Diagnosing and managing common food allergies: A systematic review. JAMA 2010, 303, 1848–1856. [Google Scholar]
- Mulla, Z.D.; Simon, M.R. Hospitalizations for anaphylaxis in Florida: Epidemiologic analysis of a population-based dataset. Int. Arch. Allergy Immunol. 2007, 144, 128–136. [Google Scholar]
- Mullins, R.J.; Clark, S.; Camargo, C.A., Jr. Socio-economic status, geographic remoteness and childhood food allergy and anaphylaxis in Australia. Clin. Exp. Allergy 2010, 40, 1523–1532. [Google Scholar]
- Asher, M.I.; Montefort, S.; Björkstén, B.; Lai, C.K.W.; Strachan, D.P.; Weiland, S.K.; Williams, H.; the ISAAC PhaseThree Study Group. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC phases one and three repeat multicountry cross-sectional surveys. Lancet 2006, 368, 733–743. [Google Scholar]
- Cataldo, F.; Accomando, S.; Fragapane, M.L.; Montaperto, D. Are food intolerances and allergies increasing in immigrant children coming from developing countries? Pediatr. Allergy Immunol. 2006, 17, 364–369. [Google Scholar] [CrossRef]
- Boyce, J.A.; Assa’ad, A.; Burks, A.W.; Jones, S.M.; Sampson, H.A.; Wood, R.A.; Plaut, M.; Cooper, S.F.; Fenton, M.J.; Arshad, S.H.; et al. Guidelines for the diagnosis and management of food allergy in the United States: Report of the NIAID-sponsored expert panel. J. Allergy Clin. Immunol. 2010, 126, S1–S58. [Google Scholar] [CrossRef]
- Young, E.; Stoneham, M.D.; Petruckevitch, A.; Barton, J.; Rona, R. A population study of food intolerance. Lancet 1994, 343, 1127–1130. [Google Scholar] [CrossRef]
- Celik-Bilgili, S.; Mehl, A.; Verstege, A.; Staden, U.; Nocon, M.; Beyer, K.; Niggemann, B. The predictive value of specific immunoglobulin E levels in serum for the outcome of oral food challenges. Clin. Exp. Allergy 2005, 35, 268–273. [Google Scholar] [CrossRef]
- Becker, L.; Oxman, A. Chapter 22: Overviews of Reviews. Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J., Green, S., Eds.; The Cochrane Collaboration: Melbourne, Australia, 2011. Available online: www.cochrane-handbook.org (accessed on 25 October 2013).
- Pieper, D.; Buechter, R.; Jerinic, P.; Eikermann, M. Overviews of reviews often have limited rigor: A systematic review. J. Clin. Epidemiol. 2012, 65, 1267–1273. [Google Scholar] [CrossRef]
- Shea, B.J.; Hamel, C.; Wells, G.A.; Bouter, L.M.; Kristjansson, E.; Grimshaw, J.; Henry, D.A.; Boers, M. AMSTAR is a reliable and valid measurement tool to assess the methodological quality of systematic reviews. J. Clin. Epidemiol. 2009, 62, 1013–1020. [Google Scholar] [CrossRef]
- Shea, B.J.; Bouter, L.M.; Peterson, J.; Boers, M.; Andersson, N.; Ortiz, Z.; Ramsay, T.; Bai, A.; Shukla, V.K.; Grimshaw, J.M. External validation of a measurement tool to assess systematic reviews (AMSTAR). PLoS One 2007, 2, e1350. [Google Scholar] [CrossRef]
- Shea, B.; Dube, C.; Moher, D. Assessing the Quality of Reports of Systematic Reviews: The QUOROM Statement Compared to Other Tools. In Systematic Reviews in Health Care: Meta-Analysis in Context; BMJ Publishing Group: London, UK, 2001; pp. 122–139. [Google Scholar]
- Sacks, H.; Berrier, J.; Reitman, D.; Ancona-Berk, V.; Chalmers, T. Meta-analyses of randomized controlled trials. N. Engl. J. Med. 1987, 316, 450–455. [Google Scholar] [CrossRef]
- Shea, B.; Grimshaw, J.; Wells, G.; Boers, M.; Andersson, N.; Hamel, C.; Porter, A.; Tugwell, P.; Moher, D.; Bouter, L. Development of AMSTAR: A measurement tool to assess the methodological quality of systematic reviews. BMC Med. Res. Methodol. 2007, 7, 10. [Google Scholar] [CrossRef]
- Smith, V.; Devane, D.; Begley, C.M.; Clarke, M. Methodology in conducting a systematic review of systematic reviews of healthcare interventions. BMC Med. Res. Methodol. 2011, 11, 15. [Google Scholar] [CrossRef]
- Grimshaw, J.; Hill, S.; Lowe, D.; Kaufman, C.; Mayhew, A.; Fiander, M.; Taylor, M.; Worswick, J.; Wu, J. Canadian Agency for Drugs and Technologies in Health, Methods for Development. Available online: http://www.cadth.ca/en/resources/rx-for-change/methods-for-development (accessed on 25 June 2013).
- Al-Muhsen, S.; Clarke, A.E.; Kagan, R.S. Peanut allergy: An overview. CMAJ 2003, 168, 1279–1285. [Google Scholar]
- Halken, S. Prevention of allergic disease in childhood: Clinical and epidemiological aspects of primary and secondary allergy prevention. Pediatr. Allergy Immunol. 2004, 15, 9–32. [Google Scholar]
- Kramer, M.S. Breastfeeding and allergy: The evidence. Ann. Nutr. Metab. 2011, 59, 20–26. [Google Scholar] [CrossRef]
- Passalacqua, G.; Compalati, E.; Schiappoli, M.; Senna, G. Complementary and alternative medicine for the treatment and diagnosis of asthma and allergic diseases. Monaldi Arch. Chest Dis. 2005, 63, 47–54. [Google Scholar]
- Zuppa, A.A.; Cota, F.; Barberi, S.; de Luca, D.; Visintini, F.; Tortorolo, G. Alimentary strategies in the neonatal period in the prevention of allergies. Pediatr. Med. Chir. 2002, 24, 45–52. [Google Scholar]
- Alexander, D.D.; Cabana, M.D. Partially hydrolyzed 100% whey protein infant formula and reduced risk of atopic dermatitis: A meta-analysis. J. Pediatr. Gastroenterol. Nutr. 2010, 50, 422–430. [Google Scholar]
- Ardern, K. Tartrazine Exclusion for Allergic Asthma. In Cochrane Database of Systematic Reviews; John Wiley & Sons, Ltd.: New York, NY, USA, 2001. [Google Scholar]
- Bahna, S.L. Hypoallergenic formulas: Optimal choices for treatment versus prevention. Ann. Allergy Asthma Immunol. 2008, 101, 453–459. [Google Scholar] [CrossRef]
- Chouraqui, J.P.; Dupont, C.; Bocquet, A.; Bresson, J.L.; Briend, A.; Darmaun, D.; Frelut, M.L.; Ghisolfi, J.; Girardet, J.P.; Goulet, O.; et al. Feeding during the first months of life and prevention of allergy. Arch. Pediatr. 2008, 15, 431–442. [Google Scholar] [CrossRef]
- De Greef, E.; Hauser, B.; Devreker, T.; Veereman-Wauters, G.; Vandenplas, Y. Diagnosis and management of cow’s milk protein allergy in infants. World J. Pediatr. 2012, 8, 19–24. [Google Scholar] [CrossRef]
- Du Toit, G.; Lack, G. Can food allergy be prevented? The current evidence. Pediatr. Clin. North Am. 2011, 58, 481–509. [Google Scholar] [CrossRef]
- Ebo, D.G.; Stevens, W.J. IgE-mediated food allergy—Extensive review of the literature. Acta Clin. Belg. 2001, 56, 234–247. [Google Scholar]
- Friedman, N.J.; Zeiger, R.S. The role of breast-feeding in the development of allergies and asthma. J. Allergy Clin. Immunol. 2005, 115, 1238–1248. [Google Scholar] [CrossRef]
- Goldin, B.R.; Gorbach, S.L. Clinical indications for probiotics: An overview. Clin. Infect. Dis. 2008, 46, S96–S100. [Google Scholar] [CrossRef]
- Gotua, M.; Lomidze, N.; Dolidze, N.; Gotua, T. IgE-mediated food hypersensitivity disorders. Georgian Med. News 2008, 157, 39–44. [Google Scholar]
- Hill, D.J.; Hosking, C.S. Infantile colic and food hypersensitivity. J. Pediatr. Gastroenterol. Nutr. 2000, 30, S67–S76. [Google Scholar] [CrossRef]
- Host, A.; Halken, S.; Muraro, A.; Dreborg, S.; Niggemann, B.; Aalberse, R.; Arshad, S.H.; von Berg, A.; Carlsen, K.H.; Duschen, K.; et al. Dietary prevention of allergic diseases in infants and small children. Pediatr. Allergy Immunol. 2008, 19, 1–4. [Google Scholar]
- Kamdar, T.; Bryce, P.J. Immunotherapy in food allergy. Immunotherapy 2010, 2, 329–338. [Google Scholar] [CrossRef]
- Kummeling, I.; Thijs, C.; Penders, J. Early life antibiotic use and risk of allergy and asthma-A systematic review and meta—analysis of reverse causation and confounding-by-indication. Euro. J. Allergy Clin. Immunol. 2010, 65, 189–190. [Google Scholar]
- Liu, A.H. Hygiene theory and allergy and asthma prevention. Paediatr. Perinat. Epidemiol. 2007, 21, 2–7. [Google Scholar] [CrossRef]
- Matheson, M.C.; Allen, K.J.; Tang, M.L. Understanding the evidence for and against the role of breastfeeding in allergy prevention. Clin. Exp. Allergy 2012, 42, 827–851. [Google Scholar]
- Ring, J.; Mohrenschlager, M. Allergy to peanut oil—Clinically relevant? J. Eur. Acad. Dermatol. Venereol. 2007, 21, 452–455. [Google Scholar]
- Seidman, E.G.; Singer, S. Therapeutic modalities for cow’s milk allergy. Ann. Allergy Asthma Immunol. 2003, 90, 104–111. [Google Scholar] [CrossRef]
- Szajewska, H. Extensive and partial protein hydrolysate preterm formulas. J. Pediatr. Gastroenterol. Nutr. 2007, 45, S183–S187. [Google Scholar] [CrossRef]
- Virkud, Y.V.; Vickery, B.P. Advances in immunotherapy for food allergy. Discov. Med. 2012, 14, 159–165. [Google Scholar]
- Cantani, A. The growing genetic links and the early onset of atopic diseases in children stress the unique role of the atopic march: A meta-analysis. J. Investig. Allergol. Clin. Immunol. 1999, 9, 314–320. [Google Scholar]
- Ortolani, C.; Pastorello, E.A.; Farioli, L.; Ispano, M.; Pravettoni, V.; Berti, C.; Incorvaia, C.; Zanussi, C. IgE-mediated allergy from vegetable allergens. Ann. Allergy 1993, 71, 470–476. [Google Scholar]
- Baumgartner, M.; Brown, C.A.; Exl, B.M.; Secretin, M.C.; van’t Hof, M.; Haschke, F. Controlled Trials Investigating the Use of One Partially Hydrolyzed Whey Formula for Dietary Prevention of Atopic Manifestations until 60 Months of Age: An Overview Using Meta-Analytical Techniques (Structured Abstract). In Nutrition Research; Database of Abstracts of Reviews of Effects (DARE): New York, NY, USA, 1998; pp. 1425–1442. [Google Scholar]
- Muche-Borowski, C.; Kopp, M.; Reese, I.; Sitter, H.; Werfel, T.; Schafer, T. Allergy prevention. J. Dtsch. Dermatol. Ges. 2010, 8, 718–724. [Google Scholar]
- Osborn David, A.; Sinn John, K.H. Prebiotics in Infants for Prevention of Allergy. In Cochrane Database of Systematic Reviews; John Wiley & Sons, Ltd.: New York, NY, USA, 2013. [Google Scholar]
- Penders, J.; Stobberingh, E.E.; van den Brandt, P.A.; Thijs, C. The role of the intestinal microbiota in the development of atopic disorders. Allergy 2007, 62, 1223–1236. [Google Scholar] [CrossRef]
- Van den Oord, R.A.; Sheikh, A. Filaggrin gene defects and risk of developing allergic sensitisation and allergic disorders: Systematic review and meta-analysis. BMJ 2009, 339, b2433. [Google Scholar] [CrossRef]
- Gunaratne Anoja, W.; Makrides, M.; Collins Carmel, T. Maternal Prenatal and/or Postnatal n-3 Fish Oil Supplementation for Preventing Allergies in Early Childhood. In Cochrane Database of Systematic Reviews; John Wiley & Sons, Ltd.: New York, NY, USA, 2012. [Google Scholar]
- Klemens, C.; Berman, D.; Mozurkewich, E. A meta-analysis of perinatal omega-3 fatty acid supplementation on inflammatory markers, allergy, atopy, and asthma in infancy and childhood. Am. J. Obstetr. Gynecol. 2010, 201. [Google Scholar] [CrossRef]
- Lamotte, C.; Preda, C.; Iliescu, C. Specific Oral Immunotherapy for Food Allergy in Children: A Systematic Review and Meta-Analysis of Randomized Control Trials. In Proceedings of the 17th Annual Meeting of French Society of Pharmacology and Therapeutics, Lille, France, 22–24 April 2013.
- Nurmatov, U.; Devereux, G.; Sheikh, A. Establishing the Effectiveness, Cost-Effectiveness and Safety of Oral and Sublingual Immunotherapy for Food Allergy: A Systematic Review and Meta-Analysis of Intervention Studies. In Proceedings of the 22nd World Allergy Congress, Cancun, Mexico, 4–8 December 2011.
- Schindler, T.; Gladman, L.; Sinn John, K.H.; Osborn David, A. Polyunsaturated Fatty Acid Supplementation in Infancy for the Prevention of Allergy and Food Hypersensitivity. In Cochrane Database of Systematic Reviews; John Wiley & Sons, Ltd.: New York, NY, USA, 2012. [Google Scholar]
- Ducharme, F.; Scarlett, J. Cow’s Milk Protein Avoidance and Development of Childhood Wheeze in Children with a Family History of Atopy. In Cochrane Database of Systematic Reviews; John Wiley & Sons, Ltd.: New York, NY, USA, 2007. [Google Scholar]
- Osborn David, A.; Sinn John, K.H. Probiotics in Infants for Prevention of Allergic Disease and Food Hypersensitivity. In Cochrane Database of Systematic Reviews; John Wiley & Sons, Ltd.: New York, NY, USA, 2007. [Google Scholar]
- Tang, L.J.; Chen, J.; Shen, Y. Meta-analysis of probiotics preventing allergic diseases in infants. Zhonghua Er Ke Za Zhi 2012, 50, 504–509. [Google Scholar]
- Dretzke, J.; Song, F. Provocation-Neutralisation Testing and Therapy for Food Allergy (Provisional Abstract); Database of Abstracts of Reviews of Effects: New York, NY, USA, 2004; p. 105. [Google Scholar]
- Osborn David, A.; Sinn John, K.H. Soy Formula for Prevention of Allergy and Food Intolerance in Infants; Cochrane Database of Systematic Reviews: New York, NY, USA, 2006. [Google Scholar]
- Osborn David, A.; Sinn John, K.H. Formulas Containing Hydrolysed Protein for Prevention of Allergy and Food Intolerance in Infants; Cochrane Database of Systematic Reviews: New York, NY, USA, 2006. [Google Scholar]
- Hays, T.; Wood, R.A. A systematic review of the role of hydrolyzed infant formulas in allergy prevention. Arch. Pediatr. Adolesc. Med. 2005, 159, 810–816. [Google Scholar] [CrossRef]
- Schoetzau, A.; Gehring, U.; Wichmann, H.E. Prospective cohort studies using hydrolysed formulas for allergy prevention in atopy-prone newborns: A systematic review. Eur. J. Pediatr. 2001, 160, 323–332. [Google Scholar] [CrossRef]
- Szajewska, H.; Horvath, A. Meta-analysis of the evidence for a partially hydrolyzed 100% whey formula for the prevention of allergic diseases. Curr. Med. Res. Opin. 2010, 26, 423–437. [Google Scholar] [CrossRef]
- Vandenplas, Y.; Hauser, B.; Borre, C.; Clybouw, C.; Mahler, T.; Hachimi-Idrissi, S.; Deraeve, L.; Malfroot, A.; Dab, I. The long-term effect of a partial whey hydrolysate formula on the prophylaxis of atopic disease. Eur. J. Pediatr. 1995, 154, 488–494. [Google Scholar] [CrossRef]
- Saarinen, K.M.; Juntunen-Backman, K.; Jarvenpaa, A.L.; Kuitunen, P.; Lope, L.; Renlund, M.; Siivola, M.; Savilahti, E. Supplementary feeding in maternity hospitals and the risk of cow’s milk allergy: A prospective study of 6209 infants. J. Allergy Clin. Immunol. 1999, 104, 457–461. [Google Scholar] [CrossRef]
- White, C. Three journals raise doubts on validity of Canadian studies. BMJ 2004, 328, 67. [Google Scholar] [CrossRef]
- Anandan, C.; Nurmatov, U.; Sheikh, A. Omega 3 and 6 oils for primary prevention of allergic disease: Systematic review and meta-analysis. Allergy 2009, 64, 840–848. [Google Scholar] [CrossRef]
- Klemens, C.M.; Berman, D.R.; Mozurkewich, E.L. The effect of perinatal omega-3 fatty acid supplementation on inflammatory markers and allergic diseases: A systematic review. BJOG 2011, 118, 916–925. [Google Scholar] [CrossRef]
- Kramer, M.S.; Kakuma, R. Maternal Dietary Antigen Avoidance during Pregnancy or Lactation, or Both, for Preventing or Treating Atopic Disease in the Child. In Cochrane Database of Systematic Reviews; John Wiley & Sons, Ltd.: New York, NY, USA, 2012. [Google Scholar]
- Tarini, B.A.; Carroll, A.E.; Sox, C.M.; Christakis, D.A. Systematic review of the relationship between early introduction of solid foods to infants and the development of allergic disease. Arch. Pediatr. Adolesc. Med. 2006, 160, 502–507. [Google Scholar] [CrossRef]
- Thompson, R.L.; Miles, L.M.; Lunn, J.; Devereux, G.; Dearman, R.J.; Strid, J.; Buttriss, J.L. Peanut sensitisation and allergy: Influence of early life exposure to peanuts. Br. J. Nutr. 2010, 103, 1278–1286. [Google Scholar] [CrossRef]
- Dunstan, J.A.; Mori, T.A.; Barden, A.; Beilin, L.J.; Taylor, A.L.; Holt, P.G.; Prescott, S.L. Fish oil supplementation in pregnancy modifies neonatal allergen-specific immune responses and clinical outcomes in infants at high risk of atopy: A randomized, controlled trial. J. Allergy Clin. Immunol. 2003, 112, 1178–1184. [Google Scholar] [CrossRef]
- Lauritzen, L.; Kjaer, T.M.; Fruekilde, M.B.; Michaelsen, K.F.; Frokiaer, H. Fish oil supplementation of lactating mothers affects cytokine production in 2 1/2-year-old children. Lipids 2005, 40, 669–676. [Google Scholar] [CrossRef]
- Furuhjelm, C.; Warstedt, K.; Larsson, J.; Fredriksson, M.; Bottcher, M.F.; Falth-Magnusson, K.; Duchen, K. Fish oil supplementation in pregnancy and lactation may decrease the risk of infant allergy. Acta Paediatr. 2009, 98, 1461–1467. [Google Scholar] [CrossRef]
- Arnoldussen, D.L.; Linehan, M.; Sheikh, A. BCG vaccination and allergy: A systematic review and meta-analysis. J. Allergy Clin. Immunol. 2011, 127, 246–253. [Google Scholar] [CrossRef]
- Bager, P.; Wohlfahrt, J.; Westergaard, T. Caesarean delivery and risk of atopy and allergic disease: Meta-analyses. Clin. Exp. Allergy 2008, 38, 634–642. [Google Scholar] [CrossRef]
- Koplin, J.; Allen, K.; Gurrin, L.; Osborne, N.; Tang, M.L.; Dharmage, S. Is caesarean delivery associated with sensitization to food allergens and IgE-mediated food allergy: A systematic review. Pediatr. Allergy Immunol. 2008, 19, 682–687. [Google Scholar] [CrossRef]
- Eggesbo, M.; Botten, G.; Stigum, H.; Nafstad, P.; Magnus, P. Is delivery by cesarean section a risk factor for food allergy? J. Allergy Clin. Immunol. 2003, 112, 420–426. [Google Scholar] [CrossRef]
- Laubereau, B.; Filipiak-Pittroff, B.; von Berg, A.; Grubl, A.; Reinhardt, D.; Wichmann, H.E.; Koletzko, S. Caesarean section and gastrointestinal symptoms, atopic dermatitis, and sensitisation during the first year of life. Arch. Dis. Child. 2004, 89, 993–997. [Google Scholar] [CrossRef]
- Negele, K.; Heinrich, J.; Borte, M.; von Berg, A.; Schaaf, B.; Lehmann, I.; Wichmann, H.E.; Bolte, G. Mode of delivery and development of atopic disease during the first 2 years of life. Pediatr. Allergy Immunol. 2004, 15, 48–54. [Google Scholar] [CrossRef]
- Renz-Polster, H.; David, M.R.; Buist, A.S.; Vollmer, W.M.; O’Connor, E.A.; Frazier, E.A.; Wall, M.A. Caesarean section delivery and the risk of allergic disorders in childhood. Clin. Exp. Allergy 2005, 35, 1466–1472. [Google Scholar] [CrossRef]
- Liem, J.J.; Kozyrskyj, A.L.; Huq, S.I.; Becker, A.B. The risk of developing food allergy in premature or low-birth-weight children. J. Allergy Clin. Immunol. 2007, 119, 1203–1209. [Google Scholar] [CrossRef]
- Salam, M.T.; Margolis, H.G.; McConnell, R.; McGregor, J.A.; Avol, E.L.; Gilliland, F.D. Mode of delivery is associated with asthma and allergy occurrences in children. Ann. Epidemiol. 2006, 16, 341–346. [Google Scholar] [CrossRef]
- Kjellman, N.I.; Johansson, S.G. Soy versus cow’s milk in infants with a biparental history of atopic disease: Development of atopic disease and immunoglobulins from birth to 4 years of age. Clin. Allergy 1979, 9, 347–358. [Google Scholar] [CrossRef]
- Biondi-Zoccai, G.; Lotrionte, M.; Landoni, G.; Modena, M.G. The rough guide to systematic reviews and meta-analyses. HSR Proc. Intensive Care Cardiovasc. Anesth. 2011, 3, 161–173. [Google Scholar]
Appendix
A1. Search Strategy for the Various Databases
A1.1. Breakdown of Strategy
A1.1.1. Food Allergy Terms
A1.1.2. Systematic Review Terms
A2. Search Strategy in PubMed
A3. Search Strategy in EMBase
| Search # | Search Terms |
| 8 | 7 and 6 |
| 7 | Food hypersensitivity {Including Related Terms} |
| 6 | 1 or 2 or 3 or 4 or 5 |
| 5 | meta analysis {Including Related Terms} |
| 4 | Research * (integrati * or overview *) {Including Related Terms} |
| 3 | quantitative (review * or overview * or synthes *) {Including Related Terms} |
| 2 | Methodologic * (review * OR overview *) {Including Related Terms} |
| 1 | Systematic * (review * OR overview *) {Including Related Terms} |
A4. Search Strategy in COCHRANE Database
A5. Search Strategy in DARE
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Lodge, C.J.; Allen, K.J.; Lowe, A.J.; Dharmage, S.C. Overview of Evidence in Prevention and Aetiology of Food Allergy: A Review of Systematic Reviews. Int. J. Environ. Res. Public Health 2013, 10, 5781-5806. https://doi.org/10.3390/ijerph10115781
Lodge CJ, Allen KJ, Lowe AJ, Dharmage SC. Overview of Evidence in Prevention and Aetiology of Food Allergy: A Review of Systematic Reviews. International Journal of Environmental Research and Public Health. 2013; 10(11):5781-5806. https://doi.org/10.3390/ijerph10115781
Chicago/Turabian StyleLodge, Caroline J., Katrina J. Allen, Adrian J. Lowe, and Shyamali C. Dharmage. 2013. "Overview of Evidence in Prevention and Aetiology of Food Allergy: A Review of Systematic Reviews" International Journal of Environmental Research and Public Health 10, no. 11: 5781-5806. https://doi.org/10.3390/ijerph10115781
APA StyleLodge, C. J., Allen, K. J., Lowe, A. J., & Dharmage, S. C. (2013). Overview of Evidence in Prevention and Aetiology of Food Allergy: A Review of Systematic Reviews. International Journal of Environmental Research and Public Health, 10(11), 5781-5806. https://doi.org/10.3390/ijerph10115781