Dietary and Physical Activity Behaviours in African Migrant Women Living in High Income Countries: A Systematic Review and Framework Synthesis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Identification
2.2. Inclusion and Exclusion Criteria
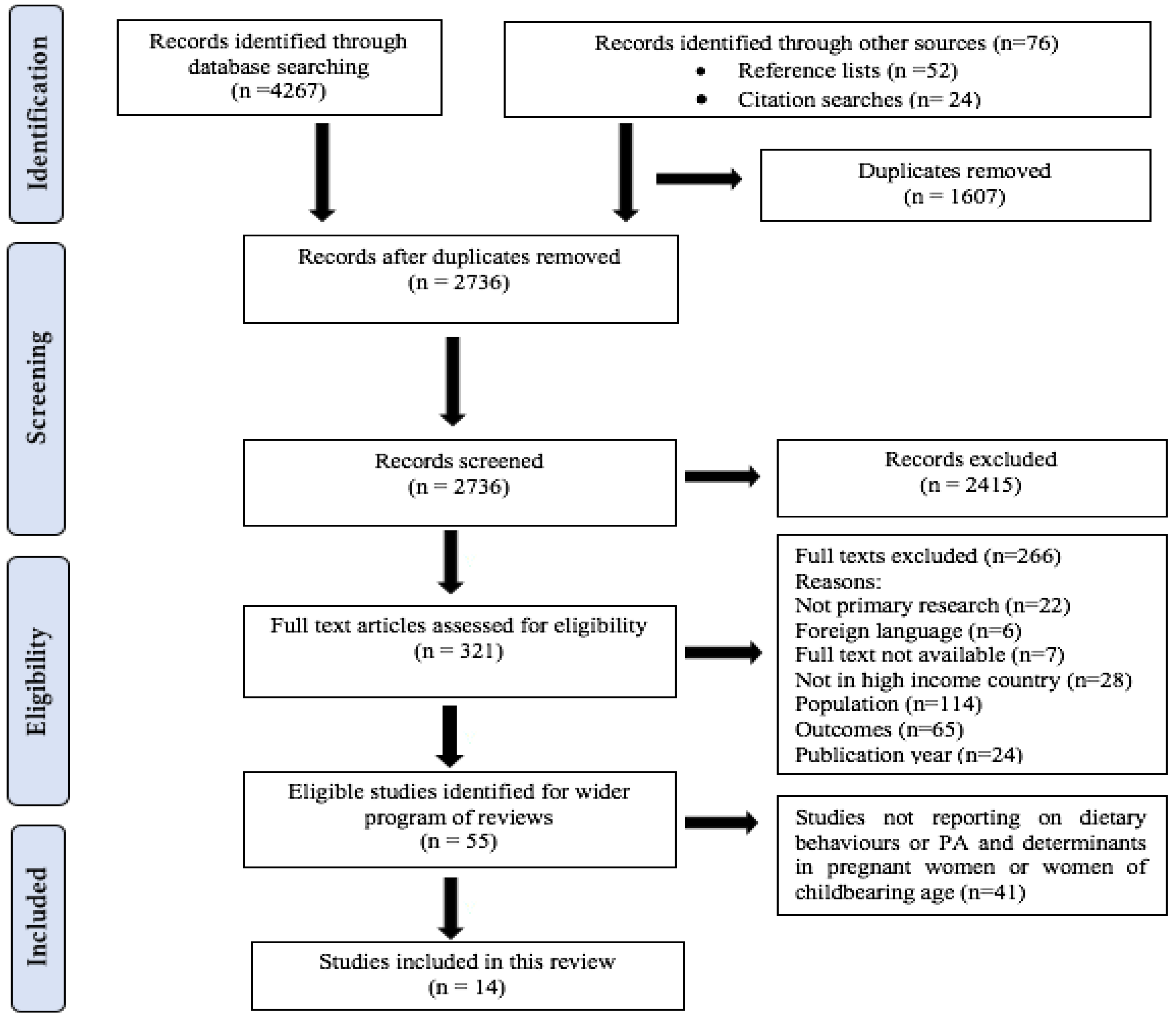
2.3. Study Selection and Screening
2.4. Data Extraction and Quality Assessment
2.5. Data Synthesis
3. Results
3.1. Description of Included Studies
3.2. Dietary Behaviours
3.2.1. Dietary Intakes
Energy and Macronutrient Intakes
Micronutrient Intakes
3.2.2. Dietary Patterns
3.2.3. Food Practices
Shopping and Cooking Practices
Eating Practices
3.3. Determinants of Dietary Behaviours
3.3.1. Sociodemographic Factors
3.3.2. Migration-related Factors
3.3.3. Culture and Religion
3.3.4. Pregnancy Status
3.3.5. Nutrition-Related Knowledge, Beliefs and Perceptions
3.3.6. Competing Priorities
3.4. PA Behaviours
3.5. Determinants of PA Behaviours
3.5.1. Sociodemographic Factors
3.5.2. Migration-Related Factors
3.5.3. Culture and Religion
3.5.4. PA-Related Knowledge, Beliefs and Perceptions
3.5.5. Competing Priorities
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
Medline Search Strategy
- africa*.mp. [mp = title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms]
- exp Africa/
- African Continental Ancestry Group/
- (foreign born adj6 black*).mp.
- ethnic minorit*.mp.
- 1 or 2 or 3 or 4 or 5
- “Emigrants and Immigrants”/
- migrant*.mp.
- immigrant*.mp.
- emigrant*.mp.
- 7 or 8 or 9 or 10
- exp Women/
- Mothers/
- exp Child/
- infant/ or infant, newborn/
- (baby or babies).mp. [mp = title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms]
- toddler*.mp.
- offspring.mp.
- young child*.mp.
- kindergarten.mp.
- preschool*.mp.
- pre-school*.mp.
- 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22
- exp Obesity/
- exp Overweight/
- bodyweight.mp.
- body weight changes/ or weight gain/
- maternal obesity.mp.
- obes*.mp.
- adiposity.mp.
- body fat*.mp.
- fat mass.mp.
- exp Body Composition/
- body mass index/ or body size/
- weight.mp.
- (obes* adj6 pregnan*).mp.
- (weight adj6 pregnan*).mp.
- (bmi adj6 pregnan*).mp.
- (obes* adj6 prepregnan*).mp.
- (obes* adj6 pre-pregnan*).mp.
- (weight adj6 prepregnan*).mp.
- (weight adj6 pre-pregnan*).mp.
- (bmi adj6 prepregnan*).mp.
- (bmi adj6 pre-pregnan*).mp.
- Eating or diet or food or intake
- Exercise or activity or PA
- Pediatric Obesity/
- Fetal Macrosomia/
- large for gestational age.mp.
- weight for height.mp.
- infant nutrition.mp.
- (child* adj2 nutrition).mp.
- infant feeding.mp.
- (child* adj2 feeding).mp.
- exp Breast Feeding/
- complimentary feeding.mp.
- exclusive breastfeeding.mp.
- 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 or 41 or 42 or 43 or 44 or 45 or 46 or 47 or 48 or 49 or 50 or 51 or 52 or 53 or 54 or 55 or 56 or 57
- Knowledge or beliefs or perceptions
- Behaviour* or behavior* or attitude* or habit*
- Determinant* or factor* or influence*
- 59 or 60 or 61
- 6 and 11 and 23 and 56 and 62
References
- Stephenson, J.; Heslehurst, N.; Hall, J.; Schoenaker, D.A.; Hutchinson, J.; Cade, J.E.; Kumaran, K. Before the beginning: Nutrition and lifestyle in the preconception period and its importance for future health. Lancet 2018, 391, 1830–1841. [Google Scholar] [CrossRef]
- Ho, A.; Flynn, A.C.; Pasupathy, D. Nutrition in pregnancy. Obstet. Gynaecol. Reprod. Med. 2016, 26, 259–264. [Google Scholar] [CrossRef]
- Merchant, K.M.; Kurz, K.M. Women’s Nutrition through the Life Cycle: Social and Biological Vulnerabilities. In The Health of Women; Routledge: New York, NY, USA, 2018; pp. 63–90. [Google Scholar]
- Picciano, M.F. Pregnancy and Lactation: Physiological Adjustments, Nutritional Requirements and the Role of Dietary Supplements. J. Nutr. 2003, 133, 1997S–2002S. [Google Scholar] [CrossRef] [PubMed]
- Morrison, J.L.; Regnault, T.R. Nutrition in pregnancy: Optimising maternal diet and fetal adaptations to altered nutrient supply. Nutrients 2016, 8, 342. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Good Maternal Nutrition the Best Start in Life; World Health Organization: Copenhagen, Denmark, 2016; ISBN 978 9289051545. [Google Scholar]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010; pp. 34–58. [Google Scholar]
- da Silva, S.G.; Ricardo, L.I.; Evenson, K.R.; Hallal, P.C. Leisure-time physical activity in pregnancy and maternal-child health: A systematic review and meta-analysis of randomized controlled trials and cohort studies. Sports Med. 2017, 47, 295–317. [Google Scholar] [CrossRef] [PubMed]
- Domenjoz, I.; Kayser, B.; Boulvain, M. Effect of physical activity during pregnancy on mode of delivery. Am. J. Obstet. Gynecol. 2014, 211, 401. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; Duffey, K.; Gordon-Larsen, P. Environmental influences on food choice, physical activity and energy balance. Physiol. Behav. 2005, 86, 603–613. [Google Scholar] [CrossRef] [PubMed]
- Short, S.E.; Mollborn, S. Social determinants and health behaviors: Conceptual frames and empirical advances. Curr. Opin. Psychol. 2015, 5, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Hiza, H.A.; Casavale, K.O.; Guenther, P.M.; Davis, C.A. Diet quality of americans differs by age, sex, race/ethnicity, income, and education level. J. Acad. Nutr. Diet. 2013, 113, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Krige, S.M.; Mahomoodally, F.M.; Subratty, A.H.; Ramasawmy, D. Relationship between socio-demographic factors and eating practices in a multicultural society. Food Nutr. Sci. 2012, 3, 286. [Google Scholar] [CrossRef]
- Park, S.Y.; Murphy, S.P.; Wilkens, L.R.; Yamamoto, J.F.; Sharma, S.; Hankin, J.H.; Henderson, B.E.; Kolonel, L.N. Dietary patterns using the Food Guide Pyramid groups are associated with sociodemographic and lifestyle factors: The multiethnic cohort study. J. Nutr. 2005, 135, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Satia, J.A. Dietary acculturation and the nutrition transition: An overview. Appl. Physiol. Nutr. Metab. 2010, 35, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Osei-Kwasi, H.A.; Powell, K.; Nicolaou, M.; Holdsworth, M. The influence of migration on dietary practices of Ghanaians living in the United Kingdom: A qualitative study. Ann. Hum. Biol. 2017, 44, 454–463. [Google Scholar] [CrossRef] [PubMed]
- Osei-Kwasi, H.A. Systematic mapping review of the factors influencing dietary behaviour in ethnic minority groups living in Europe: A DEDIPAC study. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 85. [Google Scholar] [CrossRef] [PubMed]
- Alyousif, Z.; Mathews, A.E. Impact of migration on diet, physical activity, and body weight among international students moving from the Gulf Countries to the United States. Case Rep. J. 2018, 2, 7. [Google Scholar]
- Wieland, M.L.; Weis, J.A.; Palmer, T.; Goodson, M.; Loth, S.; Omer, F.; Abbenyi, A.; Krucker, K.; Edens, K.; Sia, I.G. Physical activity and nutrition among immigrant and refugee women: A community-based participatory research approach. Women’s Health Issues 2012, 22, e225–e232. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, S.A.; Ruben, J.D.; Narayan, K.V. Health of foreign-born people in the United States: A review. Health Place 2008, 14, 623–635. [Google Scholar] [CrossRef] [PubMed]
- Sanou, D.; O’Reilly, E.; Ngnie-Teta, I.; Batal, M.; Mondain, N.; Andrew, C.; Newbold, B.K.; Bourgeault, I.L. Acculturation and nutritional health of immigrants in Canada: A scoping review. J. Immigr. Mino. Health 2014, 16, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Goulao, B.; Santos, O.; do Carmo, I. The impact of migration on body weight: A review. Cad. Saude Publ. 2015, 31, 229–245. [Google Scholar] [CrossRef]
- Gilbert, P.A.; Khokhar, S. Changing Dietary habits of ethnic groups in Europe and implications for health. Nutr. Rev. 2008, 66, 203–215. [Google Scholar]
- Oza-Frank, R.; Venkat Narayan, K.M. Effect of length of residence on overweight by region of birth and age at arrival among US immigrants. Public Health Nutr. 2010, 13, 868–875. [Google Scholar] [CrossRef] [PubMed]
- Ross, S.E.T.; Larson, N.; Graham, D.J.; Neumark-Sztainer, D. Longitudinal changes in physical activity and sedentary behavior from adolescence to adulthood: Comparing US–born and foreign-born populations. J. Phys. Act. Health 2014, 11, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Higgins, V.; Dale, A. Ethnic Differences in Physical Activity and Obesity. In Ethnicity and Integration; Springer: Dordrecht, The Netherlands, 2010; pp. 203–224. [Google Scholar]
- Saffer, H.; Dave, D.; Grossman, M.; Ann Leung, L. Racial, ethnic, and gender differences in physical activity. J. Hum. Cap. 2013, 7, 378–410. [Google Scholar] [CrossRef] [PubMed]
- Dogra, S.; Meisner, B.A.; Ardern, C.I. Variation in mode of physical activity by ethnicity and time since immigration: A cross-sectional analysis. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 75. [Google Scholar] [CrossRef] [PubMed]
- Kukaswadia, A.; Pickett, W.; Janssen, I. Time since immigration and ethnicity as predictors of physical activity among Canadian youth: A cross-sectional study. PLoS ONE 2014, 9, e89509. [Google Scholar] [CrossRef] [PubMed]
- Gagnon, A.J.; Zimbeck, M.; Zeitlin, J.; Collaboration, R. Migration to western industrialised countries and perinatal health: A systematic review. Soc. Sci. Med. 2009, 69, 934–946. [Google Scholar] [CrossRef] [PubMed]
- Malin, M.; Gissler, M. Maternal care and birth outcomes among ethnic minority women in Finland. BMC Public Health 2009, 9, 84. [Google Scholar] [CrossRef] [PubMed]
- Zanconato, G.; Iacovella, C.; Parazzini, F.; Bergamini, V.; Franchi, M. Pregnancy outcome of migrant women delivering in a public institution in northern Italy. Gynecol. Obstet. Investig. 2011, 72, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Ekéus, C.; Cnattingius, S.; Essén, B.; Hjern, A. Stillbirth among foreign-born women in Sweden. J. Public Health 2011, 21, 788–792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swann, C.; Carmona, C.; Ryan, M.; Raynor, M.; Baris, E.; Dunsdon, S.; Kelly, M.P. Health systems and health-related behaviour change: A review of primary and secondary evidence. Natl. Inst. Health Clin. Excell. 2010. Available online: https://www.nice.org.uk/media/default/About/what-we-do/NICE-guidance/NICE-guidelines/Public-health-guidelines/Additional-publications/Special-report-health-systems-and-health-related-behaviour-change.pdf (accessed on 28 June 2018).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Zlotnik, H. International Migration in Africa: An Analysis Based on Estimates of the Migrant Stock. Migr. Inf. Source 2004. Available online: https://www.migrationpolicy.org/article/international-migration-africa-analysis-based-estimates-migrant-stock (accessed on 23 June 2018).
- National Heart, Lung, and Blood Institute. Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies; National Institutes of Health, Department of Health and Human Services: Bethesda, MD, USA, 2014. Available online: http://www.nhlbi.nih.gov/health-pro/guidelines/in-develop/cardiovascular-risk-reduction/tools/co-hort (accessed on 28 June 2018).
- Singh, J. Critical appraisal skills programme. J. Pharmacol. Pharmacother. 2013, 4, 76. [Google Scholar] [CrossRef]
- Barnett-Page, E.; Thomas, J. Methods for the synthesis of qualitative research: A critical review. BMC Med. Res. Methodol. 2009, 9, 59. [Google Scholar] [CrossRef] [PubMed]
- Dixon-Woods, M. Using framework-based synthesis for conducting reviews of qualitative Studies. BMC Med. 2011, 9, 39. [Google Scholar] [CrossRef] [PubMed]
- Dassanayake, J.; Dharmage, S.C.; Gurrin, L.; Sundararajan, V.; Payne, W.R. Are Australian immigrants at a risk of being physically inactive? Int. J. Behav. Nutr. Phys. Act. 2011, 8, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casali, M.E.; Borsari, L.; Marchesi, I.; Borella, P.; Bargellini, A. Lifestyle and food habits changes after migration: A focus on immigrant women in modena (Italy). Ann. Igi. Med. Prev. Comunità 2015, 27, 748–759. [Google Scholar]
- Dominguez, L.J.; Galioto, A.; Pineo, A.; Ferlisi, A.; Vernuccio, L.; Belvedere, M.; Costanza, G.; Putignano, E.; Barbagallo, M. Blood pressure and cardiovascular risk profiles of Africans who migrate to a western country. Ethn. Dis. 2008, 18, 512–518. [Google Scholar] [PubMed]
- Lindsay, K.L.; Gibney, E.R.; McNulty, B.A.; McAuliffe, F.M. Pregnant immigrant Nigerian women: An exploration of dietary intakes. Public Health 2014, 128, 647–653. [Google Scholar] [CrossRef] [PubMed]
- Regev-Tobias, H.; Reifen, R.; Endevelt, R.; Havkin, O.; Cohen, E.; Stern, G.; Stark, A. Dietary acculturation and increasing rates of obesity in Ethiopian women Living in Israel. Nutrition 2012, 28, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Smith, N.R.; Kelly, Y.J.; Nazroo, J.Y. The effects of acculturation on obesity rates in ethnic minorities in England: Evidence from the health survey for England. Eur. J. Public Health 2012, 22, 508–513. [Google Scholar] [CrossRef] [PubMed]
- Renzaho, A.M.N.; Gibbons, C.; Swinbum, B.; Jolley, D.; Burns, C. Obesity and undernutrition in sub-saharan African immigrant and refugee children in Victoria, Australia. Asia Pac. J. Clin. Nutr. 2006, 15, 482–490. [Google Scholar] [PubMed]
- Gil, A.; Vioque, J.; Torija, E. Usual diet in Bubis, A rural immigrant population of African origin in Madrid. J. Hum. Nutr. Diet. 2005, 18, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Roville-Sausse, F. Growth rates of children of subsaharan African ancestry born to immigrant parents and of French children in Paris. Am. J. Hum. Biol. 1998, 10, 757–763. [Google Scholar] [CrossRef]
- Delisle, H.F.; Vioque, J.; Gil, A. Dietary patterns and quality in West-African Immigrants in Madrid. Nutr. J. 2009, 8, 3. [Google Scholar] [CrossRef] [PubMed]
- Persson, G.; Mahmud, A.J.; Hansson, E.E.; Strandberg, E.L. Somali women’s view of physical activity—A focus group study. BMC Women’s Health 2014, 101, e1198–e1199. [Google Scholar] [CrossRef] [PubMed]
- Quintanilha, M.; Mayan, M.J.; Thompson, J.; Bell, R.C. Contrasting “back home” and “here”: How Northeast African migrant women perceive and experience health during pregnancy and postpartum in Canada. Int. J. Equity Health 2016, 15, 80. [Google Scholar] [CrossRef] [PubMed]
- Garnweidner, L.M.; Terragni, L.; Pettersen, K.S.; Mosdol, A. Perceptions of the host country’s food culture among female immigrants from Africa and Asia: Aspects relevant for cultural sensitivity in nutrition communication. J. Nutr. Educ. Behav. 2012, 44, 335–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicolaou, M.; Benjelloun, S.; Stronks, K.; van Dam, R.; Seidell, J.; Doak, C. Influences on body weight of female moroccan migrants in the Netherlands: A qualitative study. Health Place 2012, 18, 883–891. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Essential Nutrition Actions: Improving Maternal, Newborn, Infant and Young Child Health and Nutrition; World Health Organization: Geneva, Switzerland, 2013; p. 2. [Google Scholar]
- Marangoni, F.; Cetin, I.; Verduci, E.; Canzone, G.; Giovannini, M.; Scollo, P.; Corsello, G.; Poli, A. Maternal diet and nutrient requirements in pregnancy and breastfeeding. An Italian consensus document. Nutrients 2016, 8, 629. [Google Scholar] [CrossRef] [PubMed]
- Black, R.E. Micronutrients in Pregnancy. Br. J. Nutr. 2001, 85, S193–S197. [Google Scholar] [CrossRef] [PubMed]
- Duley, L. Pre-eclampsia and the hypertensive disorders of Pregnancy. Br. Med. Bull. 2003, 67, 161–176. [Google Scholar] [CrossRef] [PubMed]
- Kumar, B.N.; Holmboe-Ottesen, G.; Lien, N.; Wandel, M. Ethnic differences in body mass index and associated factors of adolescents from minorities in Oslo, Norway: A cross-sectional study. Public Health Nutr. 2004, 7, 999–1008. [Google Scholar] [CrossRef] [PubMed]
- Satia, J.A.; Patterson, R.E.; Kristal, A.R.; Hislop, T.G.; Yasui, Y.; Taylor, V.M. Development of scales to measure dietary acculturation among Chinese-Americans and Chinese-Canadians. J. Am. Diet. Assoc. 2001, 101, 548–553. [Google Scholar] [CrossRef]
- Leung, G.; Stanner, S. Diets of minority ethnic groups in the UK: Influence on chronic disease risk and implications for prevention. Nutr. Bull. 2011, 36, 161–198. [Google Scholar] [CrossRef]
- Popkin, B.M.; Adair, L.S.; Ng, S.W. Global nutrition transition and the pandemic of obesity in developing countries. Nutr. Rev. 2012, 70, 3–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez-Cueto, F.; Verbeke, W.; Lachat, C.; Remaut-De Winter, A.M. Changes in dietary habits following temporal migration. The case of international students in Belgium. Appetite 2009, 52, 83–88. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Host Country | Study Type | Participants’ Regions (Countries) of Origin and Sample Size | Participant Ages (Years) | Duration of Residence in HIC (Years) | Outcome(s) Measured | Study Quality |
|---|---|---|---|---|---|---|---|
| Persson et al., 2014 [51] | Sweden | Qualitative | East Africa (Somalia), n = 26 | 17–67 | Mean 11.56 (Range 1–23) | Determinants of PA behaviours | Good |
| Quintanilha et al., 2016 [52] 1 | Canada | Qualitative | North East Africa (Eritrea, Ethiopia, Somalia), n = 80 | NR | NR | Determinants of dietary behaviours Determinants of PA behaviours | Fair |
| Dassanayake et al., 2011 [41] | Australia | Quantitative | North Africa, Other Africa (countries not specified), n = 122 Comparison group—Australia (n = 6460) | NR | NR | PA behaviours | Good |
| Delisle et al., 2009 [50] | Spain | Quantitative | West Africa (countries not specified), n = 130 | <30–≥45 | <6–>11 | Dietary behaviours PA behaviours | Good |
| Garnweidner et al., 2012 [53] | Norway | Qualitative | North Africa (Algeria, Egypt, Morocco); North East Africa (Somalia), n = 7 | 25–60 | 2–35 (50% population <10 years) | Dietary behaviours Determinants of dietary behaviours | Good |
| Casali et al., 2015 [42] 1 | Italy | Quantitative | North Africa and Sub-Saharan Africa (countries not specified), n = 66 | Mean (SD) 31.8 (7.3) | NR | Dietary behaviours | Fair |
| Dominguez et al., 2008 [43] | Italy | Quantitative | Sub-Saharan Africa (Ivory Coast, Ghana, Nigeria, Mali, Benin), n = 23 | Mean (SD) 29.9 (8.3) | NR | PA behaviours | Good |
| Lindsay et al., 2014 [44] 1 | Ireland | Quantitative | West Africa (Nigeria), n = 52 | Mean (SD) 32 (6.3) | Mean (SD) 7.5 (3.2) | Dietary behaviours | Fair |
| Regev et al., 2012 [45] | Israel | Quantitative | North East Africa (Ethiopia), n = 53 | Mean (SD) 32.0 (6.0) | Mean (SD) 13.8 (5.8) 13.8 ± 5.8 | Dietary behaviours Determinants of dietary behaviours PA behaviours Determinants of PA behaviours | Good |
| Smith et al., 2011 [46] | England | Quantitative | Black African (region or countries not specified), n = 587 | 16–34 | NR | Dietary behaviours PA behaviours | Fair |
| Nicolaou et al., 2012 [54] | Netherlands | Qualitative | North Africa (Morocco), n = 22 | 27–59 | <10–≥21 | Determinants of dietary behaviours Determinants of PA behaviours | Good |
| Renzaho 2006 [47] | Australia | Quantitative | Sub-Saharan Africa (countries not specified), n = 111 | NR | Dietary behaviours Determinants of dietary behaviours | Good | |
| Gil et al., 2005 [48] | Spain | Quantitative | West Africa (countries not specified), n = 130 | <30–≥45 | Mean (SD) 8.2 (6.9) | Dietary behaviours PA behaviours | Fair |
| Roville-Sausse 1998 [49] 1 | France | Quantitative | Sub-Saharan Africa (Senegal, Mali, Niger), n = 129 | 18–41 | <10 | Dietary behaviours Determinants of dietary behaviours | Fair |
| Author | Host Country | Population Countries of Origin | Dietary Outcomes Measured | Data Collection Methods |
|---|---|---|---|---|
| Delisle et al., 2009 | Spain | West Africa (countries not specified), n = 130 No comparison group | Dietary patterns after migration | Interviews, FFQ |
| Garnweidner et al., 2012 | Norway | North Africa (Algeria, Egypt, Morocco); North East Africa (Somalia), n = 7 No comparison group | Dietary patterns after migration, determinants of dietary behaviours | Interviews |
| .Casali et al., 2015 1 | Italy | North Africa and Sub-Saharan Africa (countries not specified), n = 66 Comparison groups (Non-African): Central and Eastern Europe (n = 24) | Dietary patterns after migration, comparison of food group consumption patterns with non-African ethnic groups | Interviews, Questionnaires |
| Quintanilha et al., 2016 [52] 1 | Canada | North East Africa (Eritrea, Ethiopia, Oromo, Somalia), n = 80 No comparison group | Determinants of dietary behaviours | FGD |
| Lindsay et al., 2014 [44] 1 | Ireland | West Africa (Nigeria), n = 52 No comparison group | Dietary intakes | Interviews, 24 h recall |
| Regev et al., 2012 [45] | Israel | North East Africa (Ethiopia), n = 53 No comparison group | Dietary patterns after migration, determinants of dietary behaviours | Interviews, 24 h recall |
| Smith et al., 2011 [46] | England | Black African (region or countries not specified), n = 587 Comparison group White Irish, n = 466 | Comparison of food group consumption patterns with non-African ethnic groups | Survey, Questionnaires |
| Nicolaou et al., 2012 [54] | Netherlands | North Africa (Morocco), n = 22 No comparison group | Determinants of dietary behaviours | FGD |
| Renzaho 2006 [47] | Australia | Sub-Saharan Africa (countries not specified), n = 111 No comparison group | Dietary patterns and food practices after migration, determinants of dietary behaviours | Interviews |
| Gil et al., 2005 [48] | Spain | West Africa (countries not specified), n = 130 No comparison group | Dietary intakes | Interviews, FFQ |
| Roville-Sausse 1998 [49] 1 | France | Sub-Saharan Africa (Senegal, Mali, Niger), n = 129 No comparison group | Dietary patterns and food practices after migration, determinants of dietary behaviours | Not reported |
| Energy and Macronutrient | Reported Intakes | WHO Recommended Intakes | |||||
|---|---|---|---|---|---|---|---|
| Mean (SD)—Pregnant Women [44] | Mean (SD)—Women of Childbearing Age [45,48] | %TE Pregnant Women [44] | %TE Women of Childbearing Age [45] | Mean Intake in Pregnancy | Mean Intake in Women of Childbearing Age | %TE 2 (both Pregnant Women and Women of Childbearing Age) | |
| Energy (Kcal) | 2393 (784) | NR | 51.9 | N/A | 2750 1 | N/A | N/A |
| Carbohydrate (g) | NR | 163.2 (63.6) 273.6 (67.0) | 19.4 | 65 | N/A | 130 | 55–75 |
| Protein (g) | NR | 33.8 (16.1) 107.2 (24.6) | 33.3 | 13.5 | N/A | 46 | 10–15 |
| Total fat (g) | NR | 25.3 (10.2) 85.7 (22.7) | 447.4 | 22.8 | N/A | <70 | 15–30 |
| Cholesterol (mg) | NR | 66 447.4 | NR | 66 | N/A | <300 mg/day | <300 mg/day |
| Dietary fibre (g) | 20.0 (9.8) | 8.6 (4.4) 21.3 (6.0) | NR | NR | 28 | 25 | N/A |
| Micronutrient | Mean Intakes | WHO Recommended Intakes | ||
|---|---|---|---|---|
| Mean (SD) Pregnant Women | Mean (SD) Women of Childbearing Age | Mean Intakes in Pregnancy [6] | Mean Intakes in Women of Childbearing Age | |
| Vitamin A (μg) [44,48] | 1448 (1886) [44] | 878.2 (944) [48] | 800 | 500 |
| Vitamin B12 (μg) [44,45] | 6.8 (5.2) [44] | 0.75 (0.66) [45] | 2.6 | 2.4 |
| Vitamin C (mg) [44,45,48] | 224.6 (130.4) [44] | 175.3 (92.3) [48] 70 (51) [45] | 55 | 45 |
| Vitamin D (μg) [44] | 5.1 (6.5) [44] | NR | 5 | N/A |
| Vitamin E (mg) [48] | NR | 14.0 (4.1) [48] | N/A | 7.5 |
| Calcium (mg) [44,45,48] | 726.6 (425.8) [44] | 1074 (344) [48] 277 (152) [45] | 1500–2000 | 1000 |
| Selenium (μg) [44] | 77.9 (37.0) [44] | NR | 30 | N/A |
| Sodium (mg) [44,48] | 4646 (2130) [44] | 4266 (1250) [48] | <2000 | <2000 |
| Folate (μg) [44,45] | 308.4 (141.9) [44] | 129 (58) [45] | 600 | 400 |
| Iron (mg) [44,45,48] | 14.0 (5.8) [44] | 18.2 (3.9) [48] 12.8 (6.6) [45] | 27 | 24 |
| Iodine (μg) [44] | 247.6 (163.0) [44] | NR | 200 | N/A |
| Magnesium (mg) [45] | NR | 228 (51) [45] | NR | 220 |
| Folic acid (g) [48] | NR | 399.5 (109) [48] | NR | 400 |
| Zinc (mg) [45,48] | NR | 13.0 (3.1) [48] 4.1 (0.7) [45] | NR | 4.9–9.8 |
| Phosphorus (mg) [45] | NR | 635 (15) [45] | NR | 580 |
| Author | Host Country | Population Countries of Origin | PA 1 Outcome Measured (Including Definitions of PA) | Method of PA Assessment |
|---|---|---|---|---|
| Dassanayake et al., 2011 [41] | Australia | North Africa, Other Africa (countries not specified), n = 122 Comparison group–Australia (n = 6460) | frequency and amount of time spent on PA relating to sport and fitness in the past 2 weeks | Self-report |
| Persson et al., 2014 [51] | Sweden | East Africa (Somalia), n = 26 | Determinants of PA behaviours | Self-report |
| Quintanilha et al., 2016 [52] 1 | Canada | North East Africa (Eritrea, Ethiopia, Oromo, Somalia), n = 80 | Determinants of PA behaviours | Self-report |
| Delisle et al., 2009 [50] | Spain | West Africa (countries not specified), n = 130 | Frequency of exercise (activities not defined) | Self-report |
| Dominguez et al., 2008 [43] | Italy | Sub-Saharan Africa (Ivory Coast, Ghana, Nigeria, Mali, Benin), n = 23 | Frequency of PA per week. PA defined as moderate or strenuous exercise sufficient to induce sweating including any sport, brisk walking, or doing housework at least once a week for >30 min | Self-report |
| Regev et al., 2012 [45] | Israel | North East Africa (Ethiopia), n = 53 | Daily exercise, PA at work, time spent walking per day | Self-report |
| Smith et al., 2011 [46] | England | Black African (region or countries not specified), n = 587 | Moderate or vigorous PA of at least 30 min in the last 4 weeks | Self-report |
| Nicolaou et al., 2012 [54] | Netherlands | North Africa (Morocco), n = 22 | Determinants of PA behaviours | Self-report |
| Gil et al., 2005 [48] | Spain | West Africa (countries not specified), n = 130 | Regular practice of exercise (activities not defined) | Self-report |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ngongalah, L.; Rankin, J.; Rapley, T.; Odeniyi, A.; Akhter, Z.; Heslehurst, N. Dietary and Physical Activity Behaviours in African Migrant Women Living in High Income Countries: A Systematic Review and Framework Synthesis. Nutrients 2018, 10, 1017. https://doi.org/10.3390/nu10081017
Ngongalah L, Rankin J, Rapley T, Odeniyi A, Akhter Z, Heslehurst N. Dietary and Physical Activity Behaviours in African Migrant Women Living in High Income Countries: A Systematic Review and Framework Synthesis. Nutrients. 2018; 10(8):1017. https://doi.org/10.3390/nu10081017
Chicago/Turabian StyleNgongalah, Lem, Judith Rankin, Tim Rapley, Adefisayo Odeniyi, Zainab Akhter, and Nicola Heslehurst. 2018. "Dietary and Physical Activity Behaviours in African Migrant Women Living in High Income Countries: A Systematic Review and Framework Synthesis" Nutrients 10, no. 8: 1017. https://doi.org/10.3390/nu10081017