Comparison between Dual-Energy X-ray Absorptiometry and Bioelectrical Impedance Analyses for Accuracy in Measuring Whole Body Muscle Mass and Appendicular Skeletal Muscle Mass

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Subjects
2.2. Measurement of Clinical and Biochemical Parameters
2.3. Muscle Mass Measurement Using DXA
2.4. Muscle Mass Estimation by BIA
2.5. Statistical Analysis
3. Results
3.1. Baseline Clinical Characteristics of the Study Population
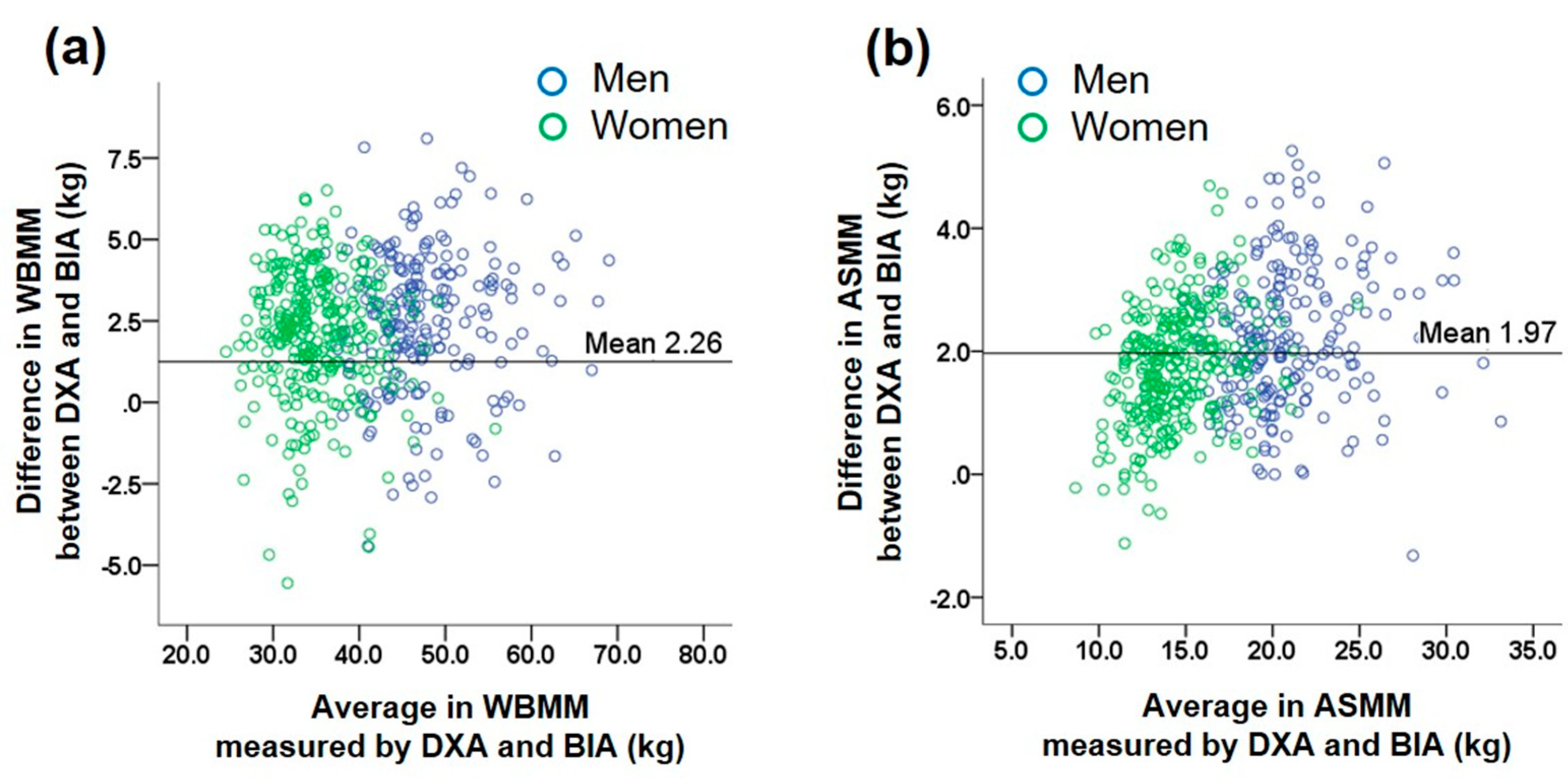
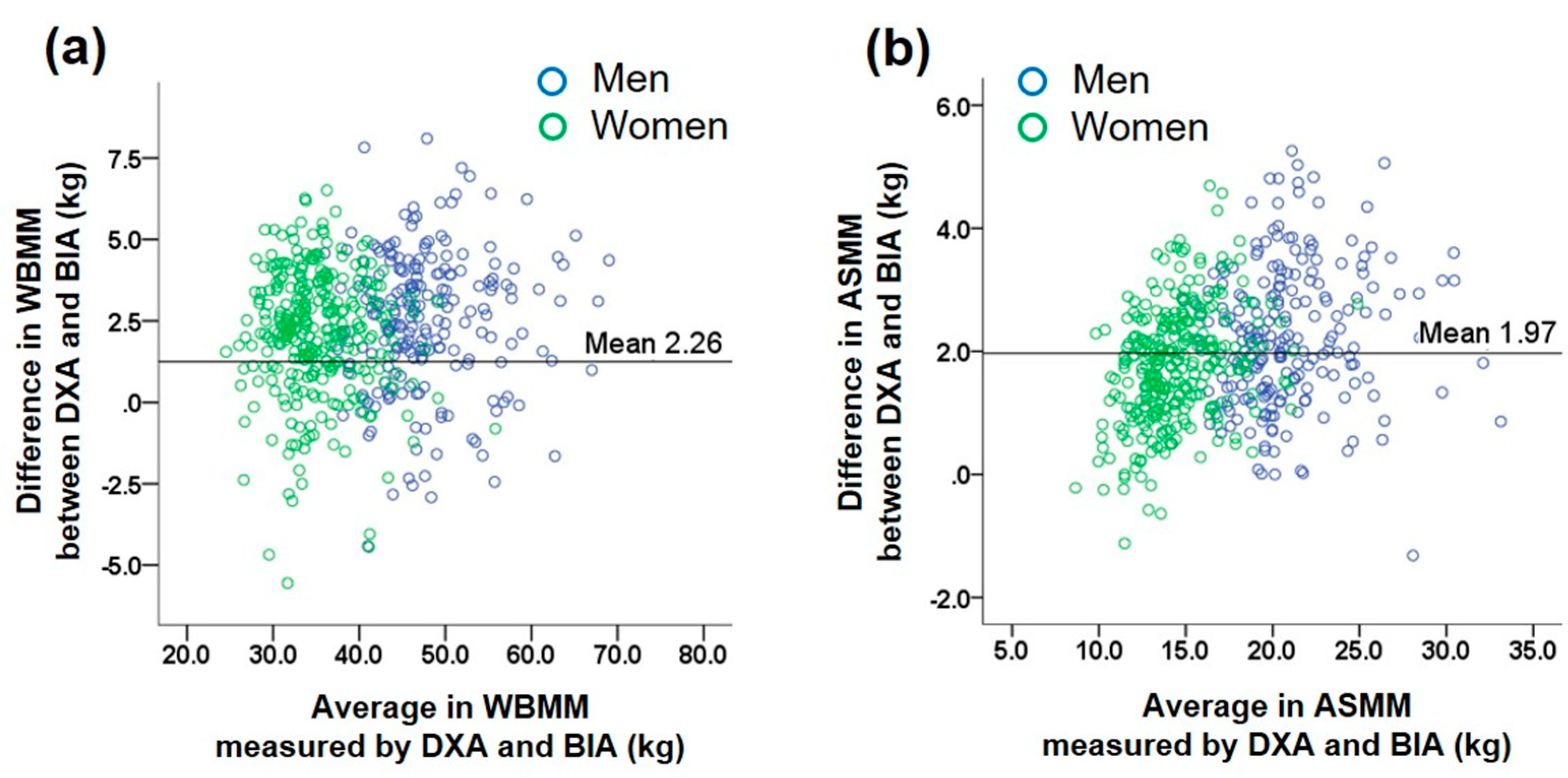
3.2. Comparison of Muscle Mass Estimated by BIA with That Measured by DXA (Table 2)
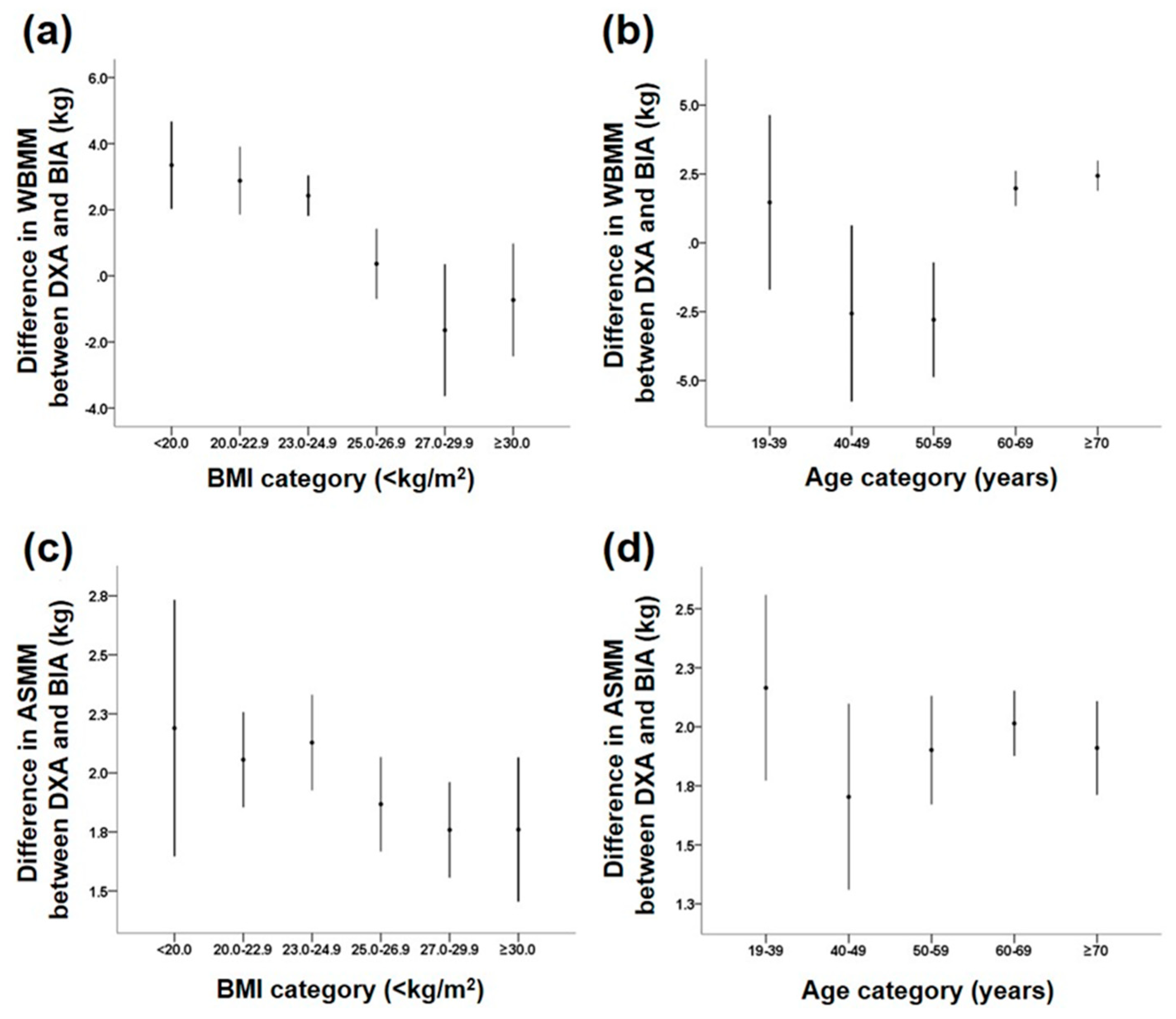
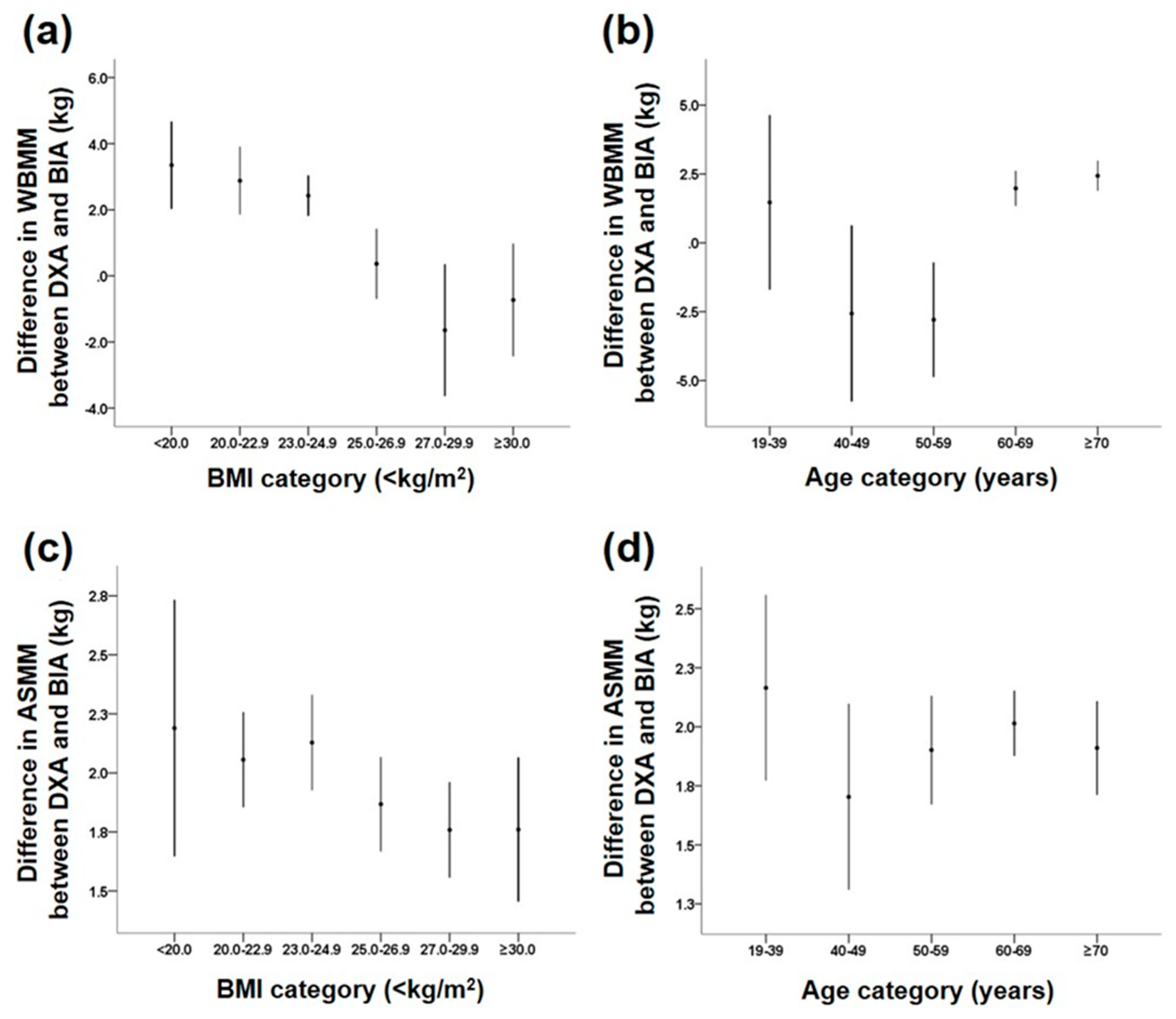
3.3. Subgroup Analysis of Mean Differences in Muscle Mass Estimates between DXA and BIA Methods According to Clinical Features (Table 3)
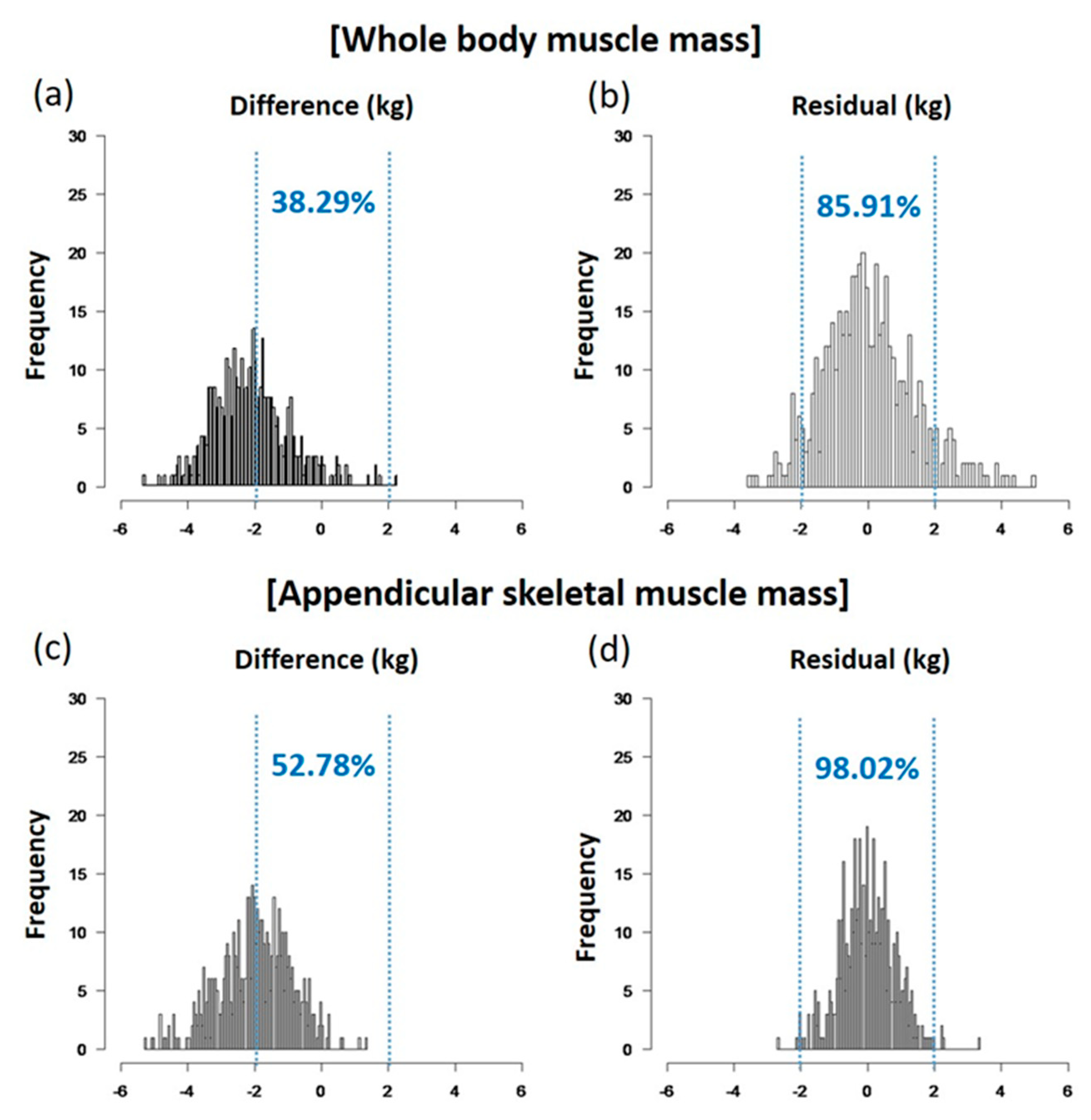
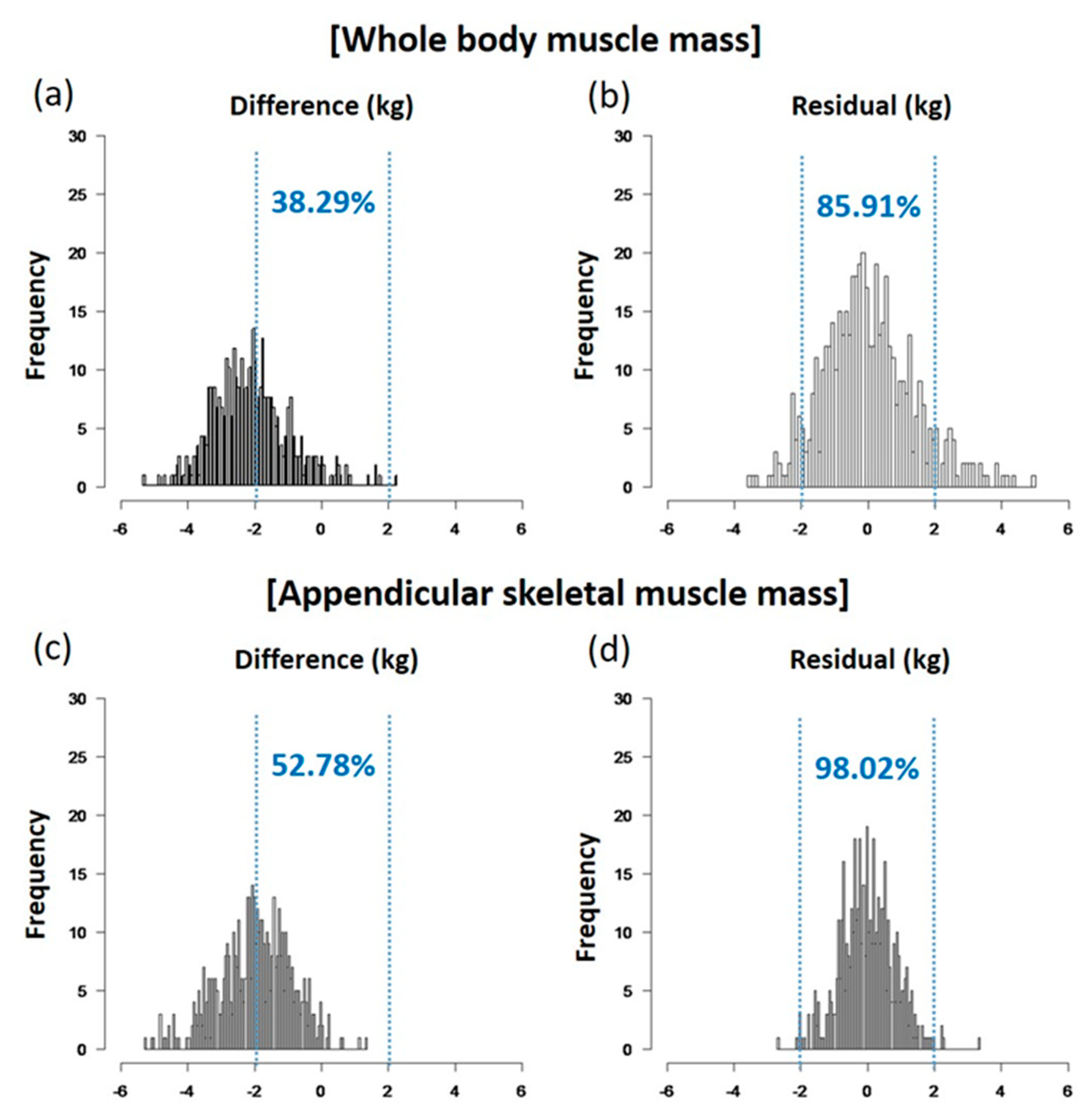
3.4. Prediction of DXA Estimation of Muscle Mass Measured by BIA Method by Multivariate Regression Models (Table 4)
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Kim, J.H.; Lim, S.; Choi, S.H.; Kim, K.M.; Yoon, J.W.; Kim, K.W.; Lim, J.Y.; Park, K.S.; Jang, H.C. Sarcopenia: An independent predictor of mortality in community-dwelling older Korean men. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 1244–1252. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian working group for sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Visser, M.; Schaap, L.A. Consequences of sarcopenia. Clin. Geriatr. Med. 2011, 27, 387–399. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, R.N.; Koehler, K.M.; Gallagher, D.; Romero, L.; Heymsfield, S.B.; Ross, R.R.; Garry, P.J.; Lindeman, R.D. Epidemiology of sarcopenia among the elderly in new Mexico. Am. J. Epidemiol. 1998, 147, 755–763. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I. Influence of sarcopenia on the development of physical disability: The cardiovascular health study. J. Am. Geriatr. Soc. 2006, 54, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Heymsfield, S.B.; Ross, R. Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disability. J. Am. Geriatr. Soc. 2002, 50, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Roubenoff, R. Sarcopenia and its implications for the elderly. Eur. J. Clin. Nutr. 2000, 54 (Suppl. 3), S40. [Google Scholar] [CrossRef] [PubMed]
- Periasamy, M.; Herrera, J.L.; Reis, F.C.G. Skeletal muscle thermogenesis and its role in whole body energy metabolism. Diabetes Metab. J. 2017, 41, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Cawthon, P.M. Assessment of lean mass and physical performance in sarcopenia. J. Clin. Densitom. 2015, 18, 467–471. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.R. Sarcopenia. Clin. Geriatr. Med. 2010, 26, 331–346. [Google Scholar] [CrossRef] [PubMed]
- Buckinx, F.; Landi, F.; Cesari, M.; Fielding, R.A.; Visser, M.; Engelke, K.; Maggi, S.; Dennison, E.; Al-Daghri, N.M.; Allepaerts, S.; et al. Pitfalls in the measurement of muscle mass: A need for a reference standard. J. Cachexia Sarcopenia Muscle 2018. [Google Scholar] [CrossRef] [PubMed]
- Bazzocchi, A.; Diano, D.; Ponti, F.; Andreone, A.; Sassi, C.; Albisinni, U.; Marchesini, G.; Battista, G. Health and ageing: A cross-sectional study of body composition. Clin. Nutr. 2013, 32, 569–578. [Google Scholar] [CrossRef] [PubMed]
- Buckinx, F.; Reginster, J.Y.; Dardenne, N.; Croisiser, J.L.; Kaux, J.F.; Beaudart, C.; Slomian, J.; Bruyere, O. Concordance between muscle mass assessed by bioelectrical impedance analysis and by dual energy X-ray absorptiometry: A cross-sectional study. BMC Musculoskelet. Disord. 2015, 16, 60. [Google Scholar] [CrossRef] [PubMed]
- Thibault, R.; Pichard, C. The evaluation of body composition: A useful tool for clinical practice. Ann. Nutr. Metab. 2012, 60, 6–16. [Google Scholar] [CrossRef] [PubMed]
- Bosaeus, I.; Wilcox, G.; Rothenberg, E.; Strauss, B.J. Skeletal muscle mass in hospitalized elderly patients: Comparison of measurements by single-frequency bia and dxa. Clin. Nutr. 2014, 33, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Kyle, U.G.; Genton, L.; Hans, D.; Pichard, C. Validation of a bioelectrical impedance analysis equation to predict appendicular skeletal muscle mass (asmm). Clin. Nutr. 2003, 22, 537–543. [Google Scholar] [CrossRef]
- Sergi, G.; De Rui, M.; Veronese, N.; Bolzetta, F.; Berton, L.; Carraro, S.; Bano, G.; Coin, A.; Manzato, E.; Perissinotto, E. Assessing appendicular skeletal muscle mass with bioelectrical impedance analysis in free-living caucasian older adults. Clin. Nutr. 2015, 34, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Bohm, A.; Heitmann, B.L. The use of bioelectrical impedance analysis for body composition in epidemiological studies. Eur. J. Clin. Nutr. 2013, 67 (Suppl. 1), S79. [Google Scholar] [CrossRef] [PubMed]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gomez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.C.; Pirlich, M.; et al. Bioelectrical impedance analysis—Part I: Review of principles and methods. Clin. Nutr. 2004, 23, 1226–1243. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Heymsfield, S.B.; Baumgartner, R.N.; Ross, R. Estimation of skeletal muscle mass by bioelectrical impedance analysis. J. Appl. Physiol. 2000, 89, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Rangel Peniche, D.B.; Raya Giorguli, G.; Aleman-Mateo, H. Accuracy of a predictive bioelectrical impedance analysis equation for estimating appendicular skeletal muscle mass in a non-caucasian sample of older people. Arch. Gerontol. Geriatr. 2015, 61, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Scott, D.; Park, M.S.; Kim, T.N.; Ryu, J.Y.; Hong, H.C.; Yoo, H.J.; Baik, S.H.; Jones, G.; Choi, K.M. Associations of low muscle mass and the metabolic syndrome in caucasian and asian middle-aged and older adults. J. Nutr. Health Aging 2016, 20, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Haldar, S.; Chia, S.C.; Henry, C.J. Body composition in asians and caucasians: Comparative analyses and influences on cardiometabolic outcomes. Adv. Food Nutr. Res. 2015, 75, 97–154. [Google Scholar] [PubMed]
- Mente, A.; Razak, F.; Blankenberg, S.; Vuksan, V.; Davis, A.D.; Miller, R.; Teo, K.; Gerstein, H.; Sharma, A.M.; Yusuf, S.; et al. Ethnic variation in adiponectin and leptin levels and their association with adiposity and insulin resistance. Diabetes Care 2010, 33, 1629–1634. [Google Scholar] [CrossRef] [PubMed]
- Glickman, S.G.; Marn, C.S.; Supiano, M.A.; Dengel, D.R. Validity and reliability of dual-energy X-ray absorptiometry for the assessment of abdominal adiposity. J. Appl. Physiol. 2004, 97, 509–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Hai, S.; Cao, L.; Zhou, J.; Liu, P.; Dong, B.R. Estimation of prevalence of sarcopenia by using a new bioelectrical impedance analysis in chinese community-dwelling elderly people. BMC Geriatr. 2016, 16, 216. [Google Scholar] [CrossRef] [PubMed]
- Gibson, A.L.; Holmes, J.C.; Desautels, R.L.; Edmonds, L.B.; Nuudi, L. Ability of new octapolar bioimpedance spectroscopy analyzers to predict 4-component-model percentage body fat in hispanic, black, and white adults. Am. J. Clin. Nutr. 2008, 87, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Park, K.S.; Ahn, S.; Ku, E.J.; Jung, K.Y.; Kim, Y.J.; Kim, K.M.; Moon, J.H.; Choi, S.H.; Park, K.S.; et al. Comparison of abdominal visceral adipose tissue area measured by computed tomography with that estimated by bioelectrical impedance analysis method in korean subjects. Nutrients 2015, 7, 10513–10524. [Google Scholar] [CrossRef] [PubMed]
- Park, K.S.; Lee, D.H.; Lee, J.; Kim, Y.J.; Jung, K.Y.; Kim, K.M.; Kwak, S.H.; Choi, S.H.; Park, K.S.; Jang, H.C.; et al. Comparison between two methods of bioelectrical impedance analyses for accuracy in measuring abdominal visceral fat area. J. Diabetes Complicat. 2016, 30, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Lukaski, H.C.; Bolonchuk, W.W.; Hall, C.B.; Siders, W.A. Validation of tetrapolar bioelectrical impedance method to assess human body composition. J. Appl. Physiol. 1986, 60, 1327–1332. [Google Scholar] [CrossRef] [PubMed]
- Pietrobelli, A.; Morini, P.; Battistini, N.; Chiumello, G.; Nunez, C.; Heymsfield, S.B. Appendicular skeletal muscle mass: Prediction from multiple frequency segmental bioimpedance analysis. Eur. J. Clin. Nutr. 1998, 52, 507–511. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, D.; Shimada, H.; Park, H.; Anan, Y.; Ito, T.; Harada, A.; Suzuki, T. Development of an equation for estimating appendicular skeletal muscle mass in japanese older adults using bioelectrical impedance analysis. Geriatr. Gerontol. Int. 2014, 14, 851–857. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Choi, S.H.; Lim, S.; Kim, K.W.; Lim, J.Y.; Cho, N.H.; Park, K.S.; Jang, H.C. Assessment of appendicular skeletal muscle mass by bioimpedance in older community-dwelling korean adults. Arch. Gerontol. Geriatr. 2014, 58, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y.; Nishizawa, M.; Uchiyama, T.; Kasahara, Y.; Shindo, M.; Miyachi, M.; Tanaka, S. Developing and validating an age-independent equation using multi-frequency bioelectrical impedance analysis for estimation of appendicular skeletal muscle mass and establishing a cutoff for sarcopenia. Int. J. Environ. Res. Public Health 2017, 14, 809. [Google Scholar] [CrossRef] [PubMed]
- Alkahtani, S.A. A cross-sectional study on sarcopenia using different methods: Reference values for healthy Saudi young men. BMC Musculoskelet. Disord. 2017, 18, 119. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Khosravi, M.; Massart, A.; Potluri, M.; Davenport, A. The effects of racial differences on body composition and total body water measured by multifrequency bioelectrical impedance analysis influence delivered kt/v dialysis dosing. Nephron Clin. Pract. 2013, 124, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Bosy-Westphal, A.; Jensen, B.; Braun, W.; Pourhassan, M.; Gallagher, D.; Muller, M.J. Quantification of whole-body and segmental skeletal muscle mass using phase-sensitive 8-electrode medical bioelectrical impedance devices. Eur. J. Clin. Nutr. 2017, 71, 1061–1067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yanovski, S.Z.; Hubbard, V.S.; Heymsfield, S.B.; Lukaski, H.C. Bioelectrical impedance analysis in body composition measurement: National institutes of health technology assessment conference statement. Am. J. Clin. Nutr. 1996, 64, S524–S532. [Google Scholar]
- Jang, H.C. Sarcopenia, frailty, and diabetes in older adults. Diabetes Metab. J. 2016, 40, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Studenski, S.A.; Peters, K.W.; Alley, D.E.; Cawthon, P.M.; McLean, R.R.; Harris, T.B.; Ferrucci, L.; Guralnik, J.M.; Fragala, M.S.; Kenny, A.M.; et al. The fnih sarcopenia project: Rationale, study description, conference recommendations, and final estimates. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.M.; Jang, H.C.; Lim, S. Differences among skeletal muscle mass indices derived from height-, weight-, and body mass index-adjusted models in assessing sarcopenia. Korean J. Intern. Med. 2016, 31, 643–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez, M.C.; Heymsfield, S.B. Bioelectrical impedance analysis for diagnosing sarcopenia and cachexia: What are we really estimating? J. Cachexia Sarcopenia Muscle 2017, 8, 187–189. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Men (n = 213) | Women (n = 294) | * p | |
|---|---|---|---|
| Age (years) | 64.1 ± 1.3 | 63.4 ± 10.3 | 0.511 |
| Height (cm) | 168.6 ± 5.8 | 155.4 ± 5.6 | <0.001 |
| Weight (kg) | 71.8 ± 11.0 | 60.9 ± 10.2 | <0.001 |
| BMI (kg/m2) | 25.2 ± 3.1 | 25.2 ± 3.8 | 0.919 |
| Waist circumference (cm) | 88.9 ± 6.3 | 84.9 ± 8.9 | <0.001 |
| SBP (mmHg) | 128.4 ± 13.7 | 127.2 ± 13.9 | 0.328 |
| DBP (mmHg) | 74.7 ± 10.1 | 75.2 ± 9.1 | 0.565 |
| Laboratory findings | |||
| FPG (70–110 mg/dL) | 135.0 ± 41.5 | 117.6 ± 33.9 | <0.001 |
| HbA1c (4.0–6.4%) | 7.1 ± 1.4 | 6.6 ± 1.2 | <0.001 |
| WBC (4–10 × 103/μL) | 6.4 ± 1.7 | 5.6 ± 1.6 | <0.001 |
| Hemoglobin (13–17 g/dL) | 14.6 ± 1.5 | 13.2 ± 1.0 | <0.001 |
| Hematocrit (39–52%) | 43.1 ± 4.1 | 39.7 ± 3.0 | <0.001 |
| Platelet (130–400 × 103/μL) | 211.5 ± 52.9 | 243.4 ± 53.9 | <0.001 |
| Total cholesterol (0–240 mg/dL) | 161.1 ± 36.1 | 180.8 ± 40.2 | <0.001 |
| Triglycerides (0–200 mg/dL) | 139.2 ± 90.5 | 132.4 ± 65.6 | 0.325 |
| HDL-cholesterol (35–55 mg/dL) | 47.5 ± 10.5 | 54.9 ± 11.9 | <0.001 |
| LDL-cholesterol (0–130 mg/dL) | 91.6 ± 27.3 | 102.1 ± 29.9 | <0.001 |
| BUN (10–26 mg/dL) | 17.4 ± 11.4 | 15.0 ± 4.3 | 0.001 |
| Creatinine (0.70–1.40 mg/dL) | 0.9 ± 0.2 | 0.7 ± 0.1 | <0.001 |
| eGFR (mL/min/1.73 m2) | 85.3 ± 18.8 | 90.5 ± 19.3 | 0.003 |
| Total protein (6.0–8.0 g/dL) | 7.2 ± 0.4 | 7.3 ± 0.4 | 0.034 |
| Albumin (3.3–5.2 g/dL) | 4.4 ± 0.3 | 4.4 ± 0.2 | 0.053 |
| AST (1–40 IU/L) | 25.7 ± 8.3 | 27.2 ± 15.0 | 0.161 |
| ALT (1–40 IU/L) | 27.1 ± 13.8 | 26.1 ± 20.1 | 0.566 |
| Muscle mass by DXA | |||
| Whole body lean mass (kg) | 46.8 ± 6.5 | 34.0 ± 4.8 | <0.001 |
| Appendicular skeletal muscle mass (kg) | 19.9 ± 3.2 | 13.5 ± 2.2 | <0.001 |
| Muscle mass by BIA | |||
| Whole body muscle mass (kg) | 49.3 ± 6.6 | 36.1 ± 4.7 | <0.001 |
| Appendicular skeletal muscle mass (kg) | 22.1 ± 3.3 | 15.3 ± 2.5 | <0.001 |
| Fat mass by BIA | |||
| Fat mass (kg) | 19.6 ± 5.7 | 22.5 ± 6.8 | <0.001 |
| Fat percent (%) | 26.9 ± 5.7 | 36.4 ± 6.3 | <0.001 |
| N | Mass by DXA (kg) | Mass by BIA (kg) | Difference (kg) | * p | †p | ICC | |
|---|---|---|---|---|---|---|---|
| (a) Whole body muscle mass (WBMM) | |||||||
| Total | 507 | 39.4 ± 8.4 | 41.6 ± 8.6 | 2.3 ± 2.0 | <0.001 | 0.972 | |
| Gender | <0.001 | ||||||
| Men | 213 | 46.8 ± 6.5 | 49.3 ± 6.6 | 2.5 ± 2.1 | <0.001 | 0.947 | |
| Women | 294 | 34.0 ± 4.8 | 36.1 ± 4.7 | 2.1 ± 1.9 | <0.001 | 0.918 | |
| BMI (kg/m2) | <0.001 | ||||||
| <20 | 22 | 30.4 ± 4.7 | 33.8 ± 5.8 | 3.4 ± 2.1 | <0.001 | 0.936 | |
| 20–22.9 | 112 | 35.3 ± 6.7 | 38.5 ± 7.3 | 3.2 ± 1.7 | <0.001 | 0.975 | |
| 23–24.9 | 97 | 38.2 ± 6.9 | 41.3 ± 7.1 | 3.0 ± 1.6 | <0.001 | 0.973 | |
| 25–26.9 | 137 | 39.8 ± 7.0 | 41.7 ± 7.6 | 1.9 ± 2.0 | <0.001 | 0.965 | |
| 27–29.9 | 75 | 43.1 ± 9.0 | 44.6 ± 9.8 | 1.5 ± 1.8 | <0.001 | 0.986 | |
| ≥30 | 47 | 47.0 ± 10.2 | 47.5 ± 10.8 | 0.4 ± 2.1 | <0.001 | 0.982 | |
| Age (years) | <0.001 | ||||||
| 19–39 | 21 | 44.7 ± 12.5 | 47.7 ± 12.9 | 2.9 ± 1.9 | <0.001 | 0.989 | |
| 40–49 | 33 | 47.7 ± 9.5 | 49.3 ± 9.7 | 1.6 ± 1.7 | <0.001 | 0.984 | |
| 50–59 | 69 | 42.9 ± 8.7 | 44.5 ± 9.1 | 1.6 ± 2.5 | <0.001 | 0.963 | |
| 60–69 | 228 | 37.7 ± 7.5 | 40.3 ± 7.7 | 2.6 ± 1.9 | <0.001 | 0.963 | |
| ≥ 70 | 142 | 37.2 ± 6.8 | 39.5 ± 7.1 | 2.2 ± 2.0 | <0.001 | 0.961 | |
| Body fat (%) ‡ | 0.003 | ||||||
| Non-obese | 74 | 37.5 ± 8.0 | 40.5 ± 8.4 | 2.9 ± 2.0 | <0.001 | 0.972 | |
| Obese | 420 | 39.6 ± 8.5 | 41.7 ± 8.7 | 2.2 ± 2.0 | <0.001 | 0.972 | |
| (b) Appendicular skeletal muscle mass (ASMM) | |||||||
| Total | 507 | 16.2 ± 4.1 | 18.2 ± 4.4 | 2.0 ± 1.1 | <0.001 | 0.972 | |
| Gender | <0.001 | ||||||
| Men | 213 | 19.9 ± 3.2 | 22.1 ± 3.3 | 2.3 ± 1.1 | <0.001 | 0.939 | |
| Women | 294 | 13.5 ± 2.2 | 15.3 ± 2.5 | 1.8 ± 0.9 | <0.001 | 0.928 | |
| BMI (kg/m2) | 0.093 | ||||||
| <20 | 22 | 12.2 ± 2.4 | 14.4 ± 3.1 | 2.2 ± 1.3 | <0.001 | 0.932 | |
| 20–22.9 | 112 | 14.4 ± 3.3 | 16.5 ± 3.9 | 2.1 ± 1.1 | <0.001 | 0.973 | |
| 23–24.9 | 97 | 15.8 ± 3.3 | 17.9 ± 3.7 | 2.1 ± 1.0 | <0.001 | 0.968 | |
| 25–26.9 | 137 | 16.3 ± 3.6 | 18.2 ± 3.9 | 1.9 ± 1.1 | <0.001 | 0.958 | |
| 27–29.9 | 75 | 17.8 ± 4.7 | 19.6 ± 5.0 | 1.8 ± 0.9 | <0.001 | 0.985 | |
| ≥30 | 47 | 19.5 ± 5.3 | 21.2 ± 5.4 | 1.8 ± 1.0 | <0.001 | 0.981 | |
| Age (years) | 0.503 | ||||||
| 19–39 | 21 | 19.2 ± 6.5 | 21.3 ± 6.7 | 2.2 ± 0.9 | <0.001 | 0.991 | |
| 40–49 | 33 | 20.4 ± 4.7 | 22.1 ± 4.7 | 1.7 ± 1.1 | <0.001 | 0.971 | |
| 50–59 | 69 | 17.8 ± 4.2 | 19.7 ± 4.5 | 1.9 ± 1.0 | <0.001 | 0.979 | |
| 60–69 | 228 | 15.4 ± 3.6 | 17.5 ± 4.0 | 2.0 ± 1.0 | <0.001 | 0.968 | |
| ≥70 | 142 | 15.0 ± 3.3 | 17.0 ± 3.9 | 2.0 ± 1.2 | <0.001 | 0.959 | |
| Body fat (%) ‡ | 0.675 | ||||||
| Non-obese | 74 | 15.4 ± 3.8 | 17.4 ± 4.5 | 2.0 ± 1.1 | <0.001 | 0.975 | |
| Obese | 420 | 16.3 ± 4.2 | 18.2 ± 4.5 | 2.0 ± 1.1 | <0.001 | 0.972 | |
| (a) Whole Body Muscle Mass (WBMM) | ||||||
|---|---|---|---|---|---|---|
| n | BIA-DXA | r | * p | †p | ||
| Anemia | Hb ≥ 12 g/dL | 457 | 2.33 ± 1.93 | 0.971 | <0.001 | 0.734 |
| Hb < 12 g/dL | 50 | 1.93 ± 2.26 | 0.938 | <0.001 | ||
| Kidney function | eGFR ≥ 60 mL/min/1.73 m2 | 480 | 2.25 ± 1.91 | 0.975 | <0.001 | 0.242 |
| eGFR < 60 mL/min/1.73 m2 | 27 | 2.80 ± 2.18 | 0.958 | <0.001 | ||
| DM | DM (+) | 327 | 2.16 ± 2.04 | 0.971 | <0.001 | 0.157 |
| DM (−) | 180 | 2.48 ± 1.70 | 0.978 | <0.001 | ||
| Medication (1) | Diuretics (−) | 457 | 2.32 ± 1.92 | 0.975 | <0.001 | 0.187 |
| Diuretics (+) | 50 | 1.83 ± 1.96 | 0.966 | <0.001 | ||
| Medication (2) | TZD (−) | 477 | 2.28 ± 1.92 | 0.973 | <0.001 | 0.213 |
| TZD (+) | 30 | 2.06 ± 1.72 | 0.989 | <0.001 | ||
| (b) Appendicular Skeletal Muscle Mass (ASMM) | ||||||
| Anemia | Hb ≥ 12 g/dL | 457 | 2.01 ± 1.12 | 0.967 | <0.001 | 0.617 |
| Hb < 12 g/dL | 50 | 1.92 ± 1.12 | 0.956 | <0.001 | ||
| Kidney function | eGFR ≥ 60 mL/min/1.73 m2 | 480 | 2.01 ± 1.11 | 0.973 | <0.001 | 0.407 |
| eGFR < 60 mL/min/1.73 m2 | 27 | 2.32 ± 1.13 | 0.962 | <0.001 | ||
| DM | DM (+) | 327 | 2.16 ± 2.04 | 0.971 | <0.001 | 0.697 |
| DM (−) | 180 | 2.48 ± 1.70 | 0.973 | <0.001 | ||
| Medication (1) | Diuretics (−) | 457 | 2.03 ± 1.12 | 0.973 | <0.001 | 0.704 |
| Diuretics (+) | 50 | 1.92 ± 1.12 | 0.971 | <0.001 | ||
| Medication (2) | TZD (−) | 477 | 2.01 ± 1.13 | 0.971 | <0.001 | 0.299 |
| TZD (+) | 30 | 1.82 ± 1.14 | 0.973 | <0.001 | ||
| Whole Body Muscle Mass | Appendicular Skeletal Muscle Mass | ||||||
|---|---|---|---|---|---|---|---|
| Co-Efficient | 95% CI | Co-Efficient | 95% CI | ||||
| Lower | Upper | Lower | Upper | ||||
| Intercept | 4.01 | 0.80 | 7.22 | Intercept | 5.07 | 3.67 | 6.47 |
| BIA-WBMM | 0.61 | 0.48 | 0.74 | BIA-ASMM | 0.24 | 0.12 | 0.37 |
| (BIA-WBMM)2 | 0.00 | 0.00 | 0.00 | (BIA-ASMM)2 | 0.01 | 0.01 | 0.01 |
| BMI | 0.28 | 0.19 | 0.38 | BMI | 0.26 | 0.21 | 0.31 |
| Gender | −2.93 | −3.37 | −2.48 | Gender | −1.19 | −1.45 | −0.93 |
| BIA-fat percent | 0.10 | 0.05 | 0.15 | BIA-fat percent | −0.06 | −0.08 | −0.04 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.Y.; Ahn, S.; Kim, Y.J.; Ji, M.J.; Kim, K.M.; Choi, S.H.; Jang, H.C.; Lim, S. Comparison between Dual-Energy X-ray Absorptiometry and Bioelectrical Impedance Analyses for Accuracy in Measuring Whole Body Muscle Mass and Appendicular Skeletal Muscle Mass. Nutrients 2018, 10, 738. https://doi.org/10.3390/nu10060738
Lee SY, Ahn S, Kim YJ, Ji MJ, Kim KM, Choi SH, Jang HC, Lim S. Comparison between Dual-Energy X-ray Absorptiometry and Bioelectrical Impedance Analyses for Accuracy in Measuring Whole Body Muscle Mass and Appendicular Skeletal Muscle Mass. Nutrients. 2018; 10(6):738. https://doi.org/10.3390/nu10060738
Chicago/Turabian StyleLee, Seo Young, Soyeon Ahn, Young Ji Kim, Myoung Jin Ji, Kyoung Min Kim, Sung Hee Choi, Hak Chul Jang, and Soo Lim. 2018. "Comparison between Dual-Energy X-ray Absorptiometry and Bioelectrical Impedance Analyses for Accuracy in Measuring Whole Body Muscle Mass and Appendicular Skeletal Muscle Mass" Nutrients 10, no. 6: 738. https://doi.org/10.3390/nu10060738