The Risks of Inappropriateness in Cardiac Imaging


Abstract
:1. Introduction
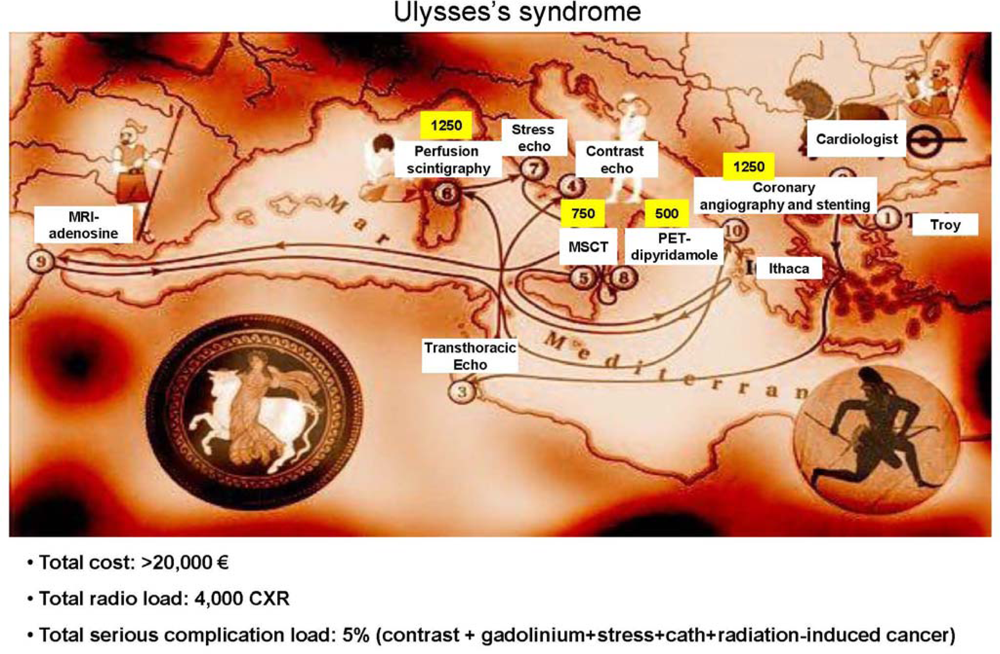
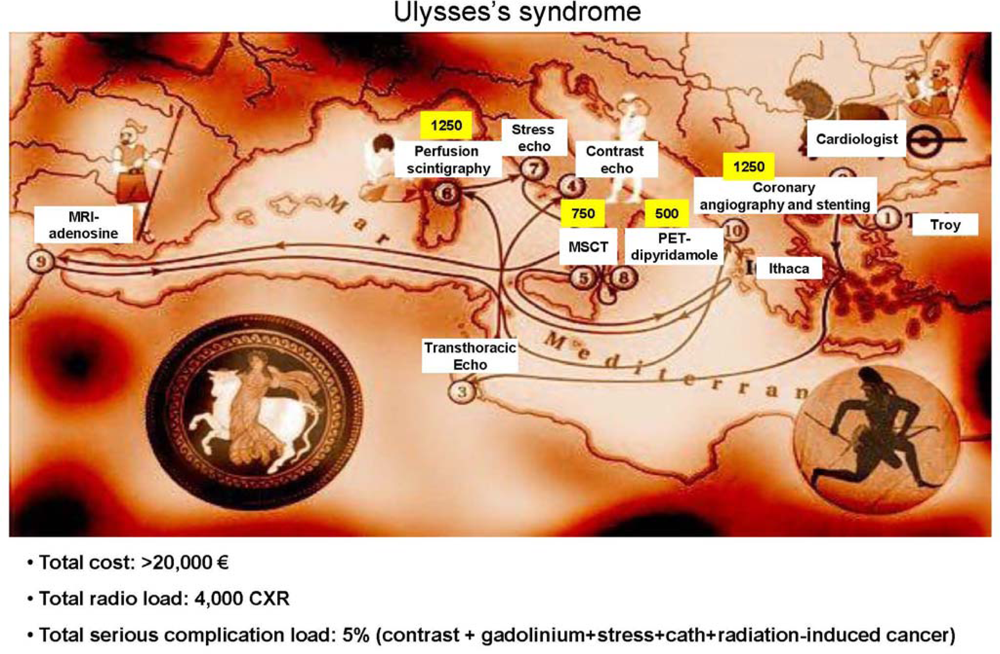
2. The Ulysses Syndrome in the Cardiac Imaging Lab
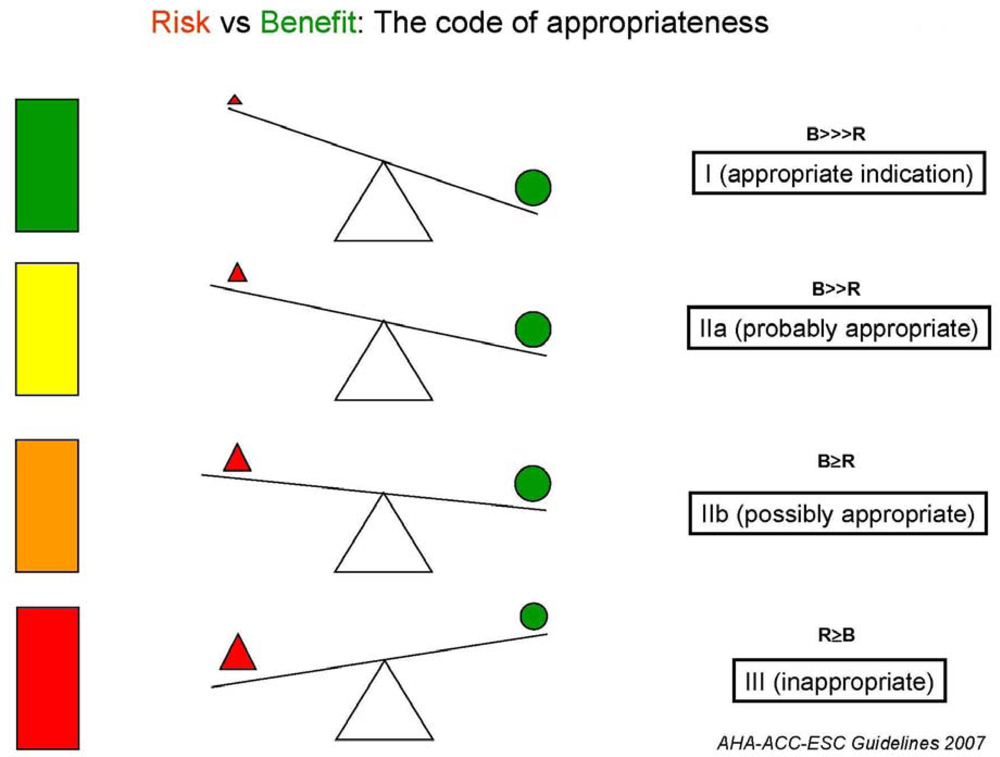
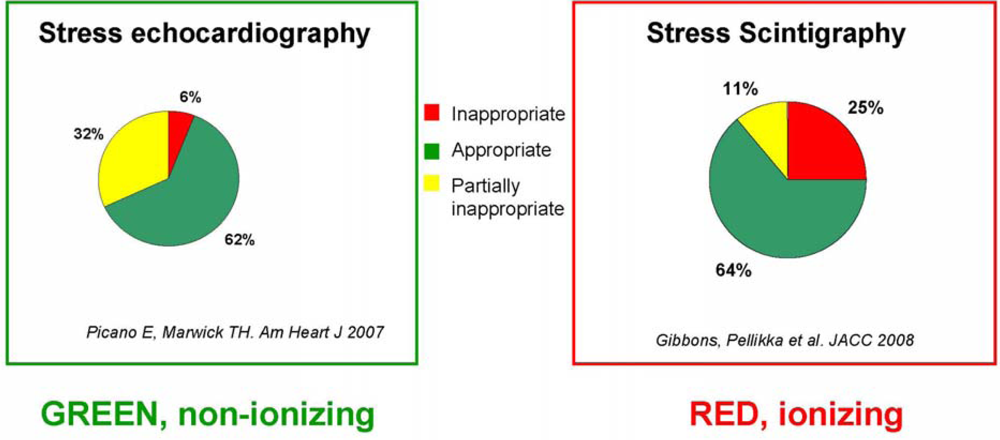
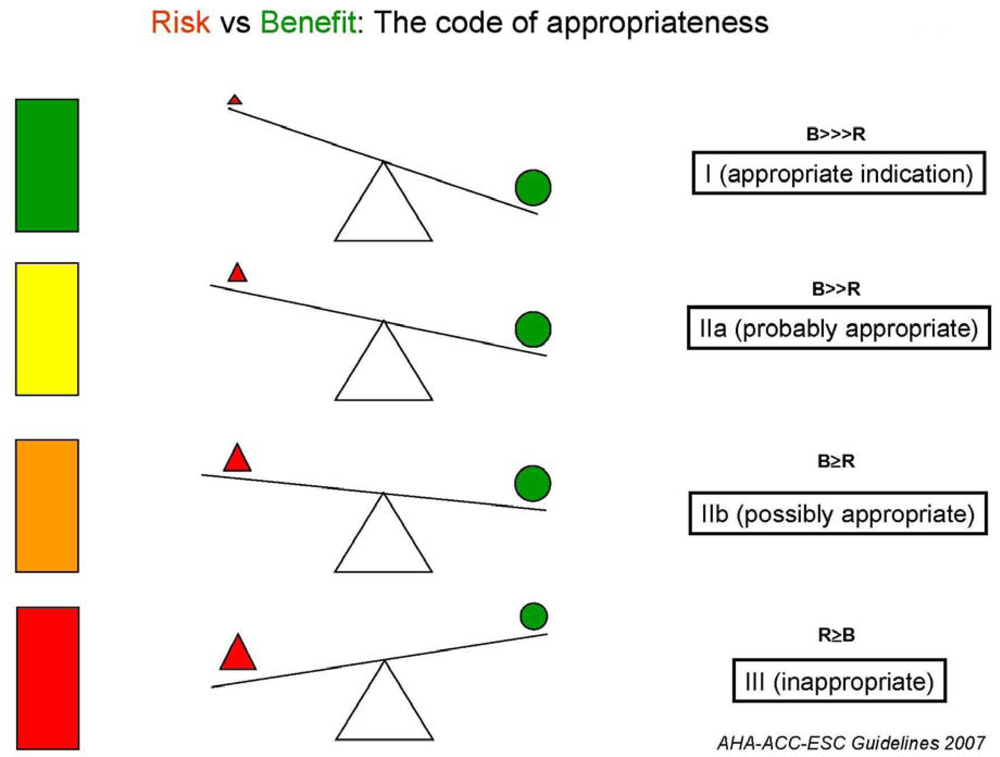
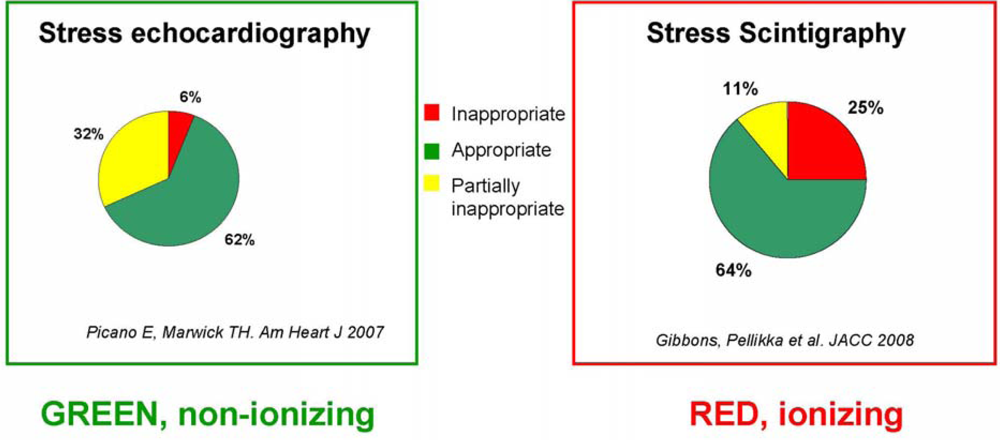
3. Appropriateness in Cardiac Stress Imaging
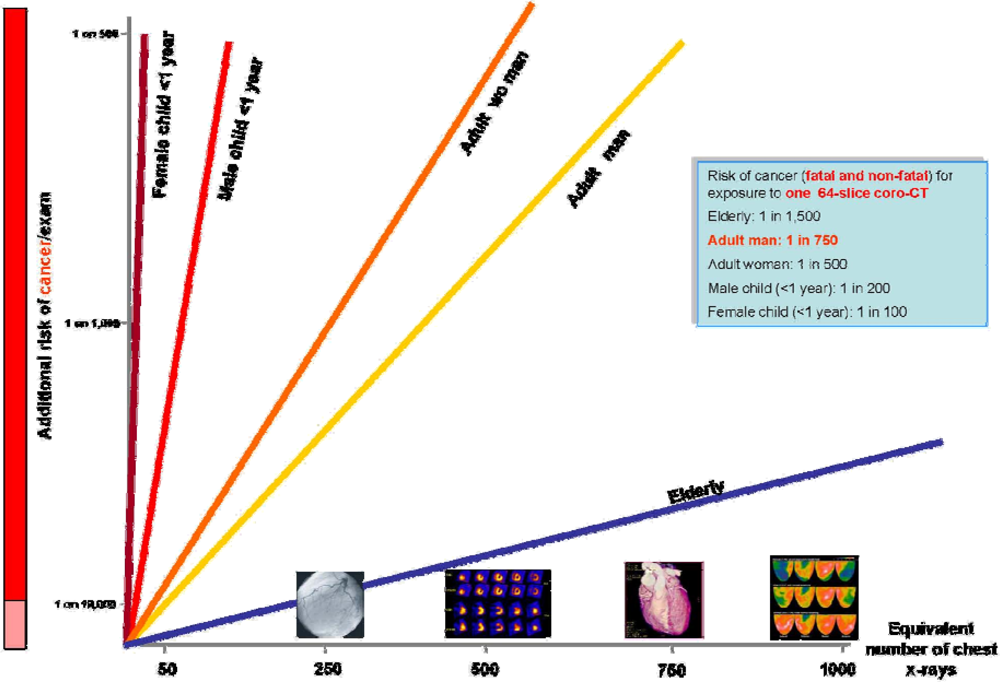
4. The Risks of Unawareness
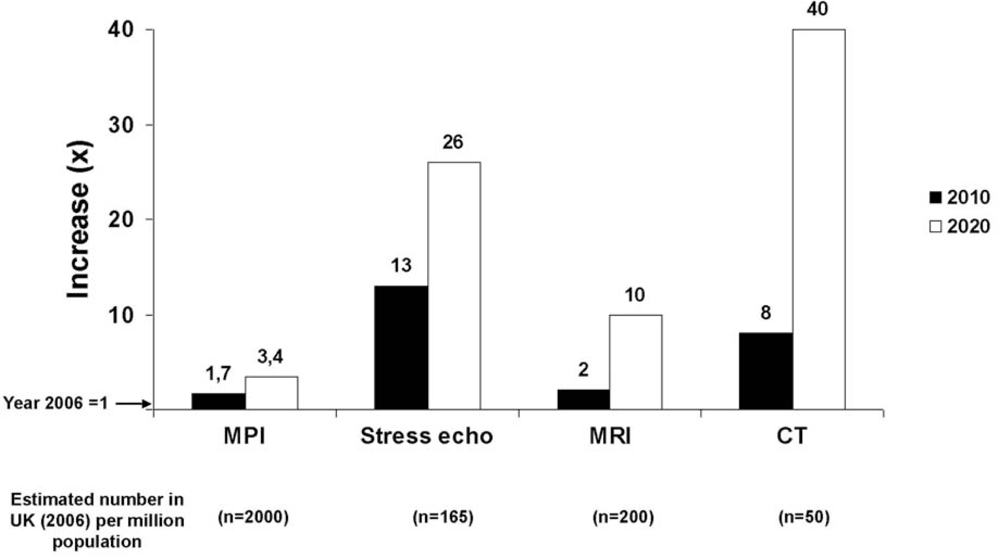
5. The Risks of Technology Underuse
6. Conclusions
References
- Picano, E. Economic and biological costs of cardiac imaging. Cardiovasc. Ultrasound 2005, 3, 13. [Google Scholar]
- Herzog, C; Rieger, CT. Risk of cancer from diagnostic X-rays. Lancet 2004, 363, 340–341. [Google Scholar]
- Lattanzi, F; Magnani, M; Cortigiani, L; Mandorla, S; Zuppiroli, A; Lorenzoni, R. Gruppo di Valutazione dell’Appropriatezza ANMCO-Toscana. Evaluation of appropriateness of prescribing echocardiography. Ital. Heart J 2002, 3, 613–618. [Google Scholar]
- Gontijo, RV; Proietti, FA; Amaral, CF; de Rezende, NA. Appropriateness use of coronary angiography in patients with suspected ischemic heart disease in Brazil. Int. J. Cardiol 2005, 104, 348–349. [Google Scholar]
- Picano, E; Pasanisi, E; Brown, J; Marwick, TH. A gatekeeper for the gatekeeper: inappropriate referrals to stress echocardiography. Am. Heart J 2007, 154, 285–290. [Google Scholar]
- Gibbons, RJ; Miller, TD; Hodge, D; Urban, L; Araoz, PA; Pellikka, P; McCully, RB. Application of appropriateness criteria to stress single-photon emission computed tomography sestamibi studies and stress echocardiograms in an academic medical center. J. Am. Coll. Cardiol 2008, 51, 1283–1289. [Google Scholar]
- Oikarinen, H; Meriläinen, S; Pääkkö, E; Karttunen, A; Nieminen, MT; Tervonen, O. Unjustified CT examinations in young patients. Eur. Radiol 2009, 19, 1161–1165. [Google Scholar]
- Ayyad, AE; Cole, J; Syed, A; Desai, MY; Halliburton, S; Schoenhagen, P; Flamm, SD; Sola, S. Temporal trends in utilization of cardiac computed tomography. J. Cardiovasc. Comput. Tomogr 2009, 3, 16–21. [Google Scholar]
- Patel, MR; Spertus, JA; Brindis, RG; Hendel, RC; Douglas, PS; Peterson, ED; Wolk, MJ; Allen, JM; Raskin, IE. American College of Cardiology Foundation ACCF proposed method for evaluating the appropriateness of cardiovascular imaging. J. Am. Coll. Cardiol 2005, 46, 1606–1613. [Google Scholar]
- Redberg, RF. The appropriateness imperative. Am. Heart J 2007, 154, 201–202. [Google Scholar]
- Shaw, LJ; Hachamovitch, R; Berman, DS; Marwick, TH; Lauer, MS; Heller, GV; Iskandrian, AE; Kesler, KL; Travin, MI; Lewin, HC; Hendel, RC; Borges-Neto, S; Miller, DD. The economic consequences of available diagnostic and prognostic strategies for the evaluation of stable angina patients: an observational assessment of the value of precatheterization ischemia. Economics of Noninvasive Diagnosis (END) Multicenter Study Group. J. Am. Coll. Cardiol 1999, 33, 661–669. [Google Scholar]
- Shaw, LJ; Marwick, TH; Berman, DS; Sawada, S; Heller, GV; Vasey, C; Miller, DD. Incremental cost-effectiveness of exercise echocardiography vs. SPECT imaging for the evaluation of stable chest pain. Eur. Heart J 2006, 27, 2448–2458. [Google Scholar]
- Ayanian, JZ. Rising rates of cardiac procedures in the United States and Canada: too much of a good thing? Circulation 2006, 113, 333–335. [Google Scholar]
- Good Practice Guide for Clinical Radiologists. Ref No: BFCR(99)11. Board of Faculty of Clinical Radiology; The Royal College of Radiologists: London, UK, 2007.
- European Commission. Radiation protection 118: referral guidelines for imaging.
- Hendel, RC; Wackers, FJ; Berman, DS; Ficaro, E; DePuey, EG; Klein, L; Cerqueira, M. American Society of Nuclear Cardiology American Society of Nuclear Cardiology consensus statement: Reporting of radionuclide myocardial perfusion imaging studies. J. Nucl. Cardiol 2006, 13, 152–156. [Google Scholar]
- Douglas, PS; Khandheria, B; Stainback, RF; Blaivas, M; Des Prez, RD; Gillam, LD; Golash, T; Hiratzka, LF; Kussmaul, WG; Labovitz, AJ; Lindenfeld, J; Masoudi, FA; Mayo, PH; Porembka, D; Spertus, JA; Wann, LS; Wiegers, SE; Brindis, RG; Douglas, PS; Hendel, RC; Patel, MR; Peterson, ED; Wolk, MJ; Allen, JM. American College of Cardiology Foundation Appropriateness Criteria Task Force; American Society of Echocardiography; American College of Emergency Physicians; American Heart Association; American Society of Nuclear Cardiology; Society for Cardiovascular Angiography and Interventions; Society of Cardiovascular Computed Tomography; Society for Cardiovascular Magnetic Resonance. ACCF/ASE/ACEP/AHA/ASNC/SCAI/SCCT/SCMR 2008 appropriateness criteria for stress echocardiography: a report of the American College of Cardiology Foundation Appropriateness Criteria Task Force, American Society of Echocardiography, American College of Emergency Physicians, American Heart Association, American Society of Nuclear Cardiology, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, and Society for Cardiovascular Magnetic Resonance: endorsed by the Heart Rhythm Society and the Society of Critical Care Medicine. Circulation 2008, 117, 1478–1497. [Google Scholar]
- Rang, M. The Ulysses syndrome. Can. Med. Assoc. J 1972, 106, 122–123. [Google Scholar]
- Gibbons, RJ; Abrams, J; Chatterjee, K; Daley, J; Deedwania, PC; Douglas, JS; Ferguson, TB, Jr; Fihn, SD; Fraker, TD, Jr; Gardin, JM; O’Rourke, RA; Pasternak, RC; Williams, SV. American College of Cardiology; American Heart Association Task Force on practice guidelines (Committee on the Management of Patients With Chronic Stable Angina) ACC/AHA 2002 guideline update for the management of patients with chronic stable angina-summary article: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. (Committee on the Management of Patients with Chronic Stable Angina). J. Am. Coll. Cardiol 2003, 41, 159–168. [Google Scholar]
- Pennell, DJ; Sechtem, UP; Higgins, CB; Manning, WJ; Pohost, GM; Rademakers, FE; van Rossum, AC; Shaw, LJ; Yucel, EK. Society for Cardiovascular Magnetic Resonance; Working Group on Cardiovascular Magnetic Resonance of the European Society of Cardiology Clinical indications for cardiovascular magnetic resonance (CMR): Consensus Panel report. Eur. Heart J 2004, 25, 1940–1965. [Google Scholar]
- Picano, E; Mathias, W, Jr; Pingitore, A; Bigi, R; Previtali, M. Safety and tolerability of dobutamine-atropine stress echocardiography: a prospective, multicentre study. Echo Dobutamine International Cooperative Study Group. Lancet 1994, 344, 1190–1192. [Google Scholar]
- Picano, E; Marini, C; Pirelli, S; Maffei, S; Bolognese, L; Chiriatti, G; Chiarella, F; Orlandini, A; Seveso, G; Colosso, MQ; et al. Safety of intravenous high-dose dipyridamole echocardiography. The Echo-Persantine International Cooperative Study Group. Am. J. Cardiol 1992, 70, 252–258. [Google Scholar]
- Varga, A; Garcia, MA; Picano, E. International Stress Echo Complication Registry Safety of stress echocardiography (from the International Stress Echo Complication Registry). Am. J. Cardiol 2006, 98, 541–543. [Google Scholar]
- Marcassa, C; Bax, JJ; Bengel, F; Hesse, B; Petersen, CL; Reyes, E; Underwood, R. European Council of Nuclear Cardiology (ECNC); European Society of Cardiology Working Group 5 (Nuclear Cardiology and Cardiac CT); European Association of Nuclear Medicine Cardiovascular Committee Clinical value, cost-effectiveness, and safety of myocardial perfusion scintigraphy: a position statement. Eur. Heart J 2008, 29, 557–563. [Google Scholar]
- Sicari, R; Nihoyannopoulos, P; Evangelista, A; Kasprzak, J; Lancellotti, P; Poldermans, D; Voigt, JU; Zamorano, JL. European Association of Echocardiography Stress echocardiography expert consensus statement: European Association of Echocardiography (EAE) (a registered branch of the ESC). Eur. J. Echocardiogr 2008, 9, 415–437. [Google Scholar]
- Bashore, TM; Bates, ER; Berger, PB; Laskey, WK; Clark, DA; O’Laughlin, MP; Cusma, JT; Oesterle, S; Dehmer, GJ; Popma, JJ. American College of Cardiology. Task Force on Clinical Expert Consensus Documents. American College of Cardiology/Society for Cardiac Angiography and Interventions Clinical Expert Consensus Document on cardiac catheterization laboratory standards. A report of the American College of Cardiology Task Force on Clinical Expert Consensus Documents. J. Am. Coll. Cardiol 2001, 37, 2170–2214. [Google Scholar]
- Lester, SJ; Miller, FA, Jr; Khandheria, BK. Contrast echocardiography: beyond a black box warning? J. Am. Soc. Echocardiogr 2008, 21, 417–418. [Google Scholar]
- Information for Healthcare Professionals Micro-bubble Contrast Agents (Marketed as Definity (Perflutren Lipid Microsphere)) Injectable Suspension and Opison (Perflutren Protein-Type A Microspheres for Injection); FDA: Silver Spring, MD, USA, 2007.
- Stiles, S. FDA backpedals on warnings in Echo-contrast labelling. Heartwire. 2008.
- Ersoy, H; Rybicki, FJ. Biochemical safety profiles of gadolinium-based extracellular contrast agents and nephrogenic systemic fibrosis. J. Magn. Reson. Imaging 2007, 26, 1190–1197. [Google Scholar]
- Brindis, RG; Douglas, PS; Hendel, RC; Peterson, ED; Wolk, MJ; Allen, JM; Patel, MR; Raskin, IE; Bateman, TM; Cerqueira, MD; Gibbons, RJ; Gillam, LD; Gillespie, JA; Iskandrian, AE; Jerome, SD; Krumholz, HM; Messer, JV; Spertus, JA; Stowers, SA. American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group; American Society of Nuclear Cardiology; American Heart Association ACCF/ASNC appropriateness criteria for single-photon emission computed tomography myocardial perfusion imaging (SPECT MPI): a report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group and the American Society of Nuclear Cardiology endorsed by the American Heart Association. J. Am. Coll. Cardiol 2005, 46, 1587–1605. [Google Scholar]
- Picano, E. Stress echocardiography: a historical perspective. Special Article. Am. J. Med 2003, 114, 126–130. [Google Scholar]
- Committee to Assess Health Risks from Exposure to Low Levels of Ionizing Radiation; Nuclear and Radiation Studies Board, Division on Earth and Life Studies, National Research Council of the National Academies. In Health Risks from Exposure to Low Levels of Ionizing Radiation: BEIR VII Phase 2; The National Academies Press: Washington, DC, USA, 2006.
- Picano, E. Sustainability of medical imaging. Education and Debate. BMJ 2004, 328, 578–580. [Google Scholar]
- Picano, E. Informed consent and communication of risk from radiological and nuclear medicine examinations: how to escape from a communication inferno. Education and Debate. BMJ 2004, 329, 849–851. [Google Scholar]
- Fox, K; Garcia, MA; Ardissino, D; Buszman, P; Camici, PG; Crea, F; Daly, C; de Backer, G; Hjemdahl, P; López-Sendón, J; Morais, J; Pepper, J; Sechtem, U; Simoons, M; Thygesen, K. Task Force on the Management of Stable Angina Pectoris of the European Society of Cardiology; ESC Committee for Practice Guidelines (CPG). Guidelines on the management of stable angina pectoris: executive summary: the Task Force on the Management of Stable Angina Pectoris of the European Society of Cardiology. Eur. Heart J 2006, 27, 1341–1381. [Google Scholar]
- Boden, WE; O’Rourke, RA; Teo, KK; Hartigan, PM; Maron, DJ; Kostuk, WJ; Knudtson, M; Dada, M; Casperson, P; Harris, CL; Chaitman, BR; Shaw, L; Gosselin, G; Nawaz, S; Title, LM; Gau, G; Blaustein, AS; Booth, DC; Bates, ER; Spertus, JA; Berman, DS; Mancini, GB; Weintraub, WS. COURAGE Trial Research Group Optimal medical therapy with or without PCI for stable coronary disease. N. Engl. J. Med 2007, 356, 1503–1516. [Google Scholar]
- Bonow, RO. Is appropriateness appropriate? J. Am. Coll. Cardiol 2008, 51, 1290–1291. [Google Scholar]
- Gershlick, AH; de Belder, M; Chambers, J; Hackett, D; Keal, R; Kelion, A; Neubauer, S; Pennell, DJ; Rothman, M; Signy, M; Wilde, P. Role of non-invasive imaging in the management of coronary artery disease: an assessment of likely change over the next 10 years. A report from the British Cardiovascular Society Working Group. Heart 2007, 93, 423–431. [Google Scholar]
- Gerber, TC; Carr, JJ; Arai, AE; Dixon, RL; Ferrari, VA; Gomes, AS; Heller, GV; McCollough, CH; McNitt-Gray, MF; Mettler, FA; Mieres, JH; Morin, RL; Yester, MV. Ionizing Radiation in Cardiac Imaging A Science Advisory From the American Heart Association Committee on Cardiac Imaging of the Council on Clinical Cardiology and Committee on Cardiovascular Imaging and Intervention of the Council on Cardiovascular Radiology and Intervention. In Circulation; 2009; doi: 10.1161/CIRCULATIONAHA.108.191650. [Google Scholar]
- Shiralkar, S; Rennie, A; Snow, M; Galland, RB; Lewis, MH; Gower-Thomas, K. Doctors’ knowledge of radiation exposure: questionnaire study. BMJ 2003, 327, 371–372. [Google Scholar]
- Finestone, A; Schlesinger, T; Amir, H; Richter, E; Milgrom, C. Do physicians correctly estimate radiation risks from medical imaging? Arch. Environ. Health 2003, 58, 59–61. [Google Scholar]
- Lee, CI; Haims, AH; Monico, EP; Brink, JA; Forman, HP. Diagnostic CT scans: assessment of patient, physician, and radiologist awareness of radiation dose and possible risks. Radiology 2004, 231, 393–398. [Google Scholar]
- Correia, MJ; Hellies, A; Andreassi, MG; Ghelarducci, B; Picano, E. Lack of Radiological Awareness in a Tertiary Care Cardiological Centre. Int. J. Cardiol 2005, 103, 307–311. [Google Scholar]
- The Royal College of Radiologists. Making the best use of clinical radiology services: referral guidelines; The Royal College of Radiologists: London, UK, 2007. [Google Scholar]
- Smeesters, P. Radioprotection and medical practice: progress, distress and treats. Bull. Mem. Acad. R. Med. Belg 2008, 163, 145–158. [Google Scholar]
- IAEA Consultants meeting on “Justification of patient exposure in medical imaging”. Wien, Vienna, December 10–14, 2007.
- Fisher, ES. Medical care-is more always better. N Engl J Med 2003, 349, 1665–1667. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ACUTE | SUBACUTE | CHRONIC | |
|---|---|---|---|
| Most frequent cause | Stress | Iodinated contrast | Radiation |
| Timing | Seconds | Days | Years |
| Examples | Myocardial infarction | Renal failure | Cancer |
| Cellular target | Endothelium of coronary arteries | Kidney tubular cell | Somatic cells (lung, breast, bone marrow) |
| Risk per exam | 1 in 500-1 in 1,000 | 1 in 50-1 in 100 | 1 in 500-1 in 1,000 |
| Cumulative nature | No | No | yes |
| Appropriate | Uncertain | Inappropriate | |
|---|---|---|---|
| ECG uninterpretable or unable to exercise, or prior stress ECG equivocal | √ | ||
| Coronary artery stenosis of unclear significance (CT or angio) | √ | ||
| Post-revascularization not in the early post-procedure period, with change in symptoms | √ | ||
| Pre-surgery, high risk non-emergent, poor exercise tolerance <4 METS | √ | ||
| Viability (dobutamine) Ischemic cardiomyopathy, known CAD, pt eligible for revascularization | √ | ||
| Asymptomatic or stable symptoms, repeat stress echo after > 5 yrs | √ | ||
| Asymptomatic < 5 yrs post CABG or < 2 yrs post-PCI | √ | ||
| Asymptomatic, low risk | √ | ||
| Pre-op, intermediate risk surgery, good exercise capacity | √ | ||
| Symptomatic, low pre-test probability, interpretable ECG, able to exercise | √ |
| Investigation | Effective Dose (mSv) | Equivalent No. of Plain Chest Radiographs | Approximate Equivalent Period of Natural Background Radiation | Additional Lifetime Risk of Fatal and Non-Fatal Cancer* | RCR Symbolic Representation** |
|---|---|---|---|---|---|
| Plain PA chest radiograph | 0.02 | 1 | 3 days | 1:1,000,000 |  |
| Lung perfusion scintigraphy (Tc99m) | 1 | 50 | 6 months | 1:10,000 |  |
| CT chest (non contrast) | 8 | 400 | 3.6 years | 1: 1,200 |  |
| Perfusion cardiac Rest-stress Technetium 99m sestamibi scan | 10 | 500 | 4 years | 1:1,000 |  |
| MDCT Cardiac (64-slice) | 15 | 750 | 7 years | 1:750 | |
| Coronary stenting | 20 | 1050 | 8 years | 1:500 | |
| Thallium-201 scan | 41 | 2000 | 16 years | 1:250 | |
 : <1 mSv,
: <1 mSv,
 : 1 – 5 mSv,
: 1 – 5 mSv,
 : 5 – 10 mSv,
: 5 – 10 mSv,
 : > 10 mSv; On the right side column, symbology proposed by Royal College of Radiology, 2007 [45].
: > 10 mSv; On the right side column, symbology proposed by Royal College of Radiology, 2007 [45].© 2009 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Picano, E. The Risks of Inappropriateness in Cardiac Imaging. Int. J. Environ. Res. Public Health 2009, 6, 1649-1664. https://doi.org/10.3390/ijerph6051649
Picano E. The Risks of Inappropriateness in Cardiac Imaging. International Journal of Environmental Research and Public Health. 2009; 6(5):1649-1664. https://doi.org/10.3390/ijerph6051649
Chicago/Turabian StylePicano, Eugenio. 2009. "The Risks of Inappropriateness in Cardiac Imaging" International Journal of Environmental Research and Public Health 6, no. 5: 1649-1664. https://doi.org/10.3390/ijerph6051649