
Adolescent Overweight and Obesity: Links to Socioeconomic Status and Fruit and Vegetable Intakes

Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Measurements
2.3. Ethical Considerations
2.4. Data Analysis
3. Results
3.1. Participants’ General Characteristics
3.2. Crude Associations of Sociodemographic and Behavioral Characteristics with Overweight/Obesity
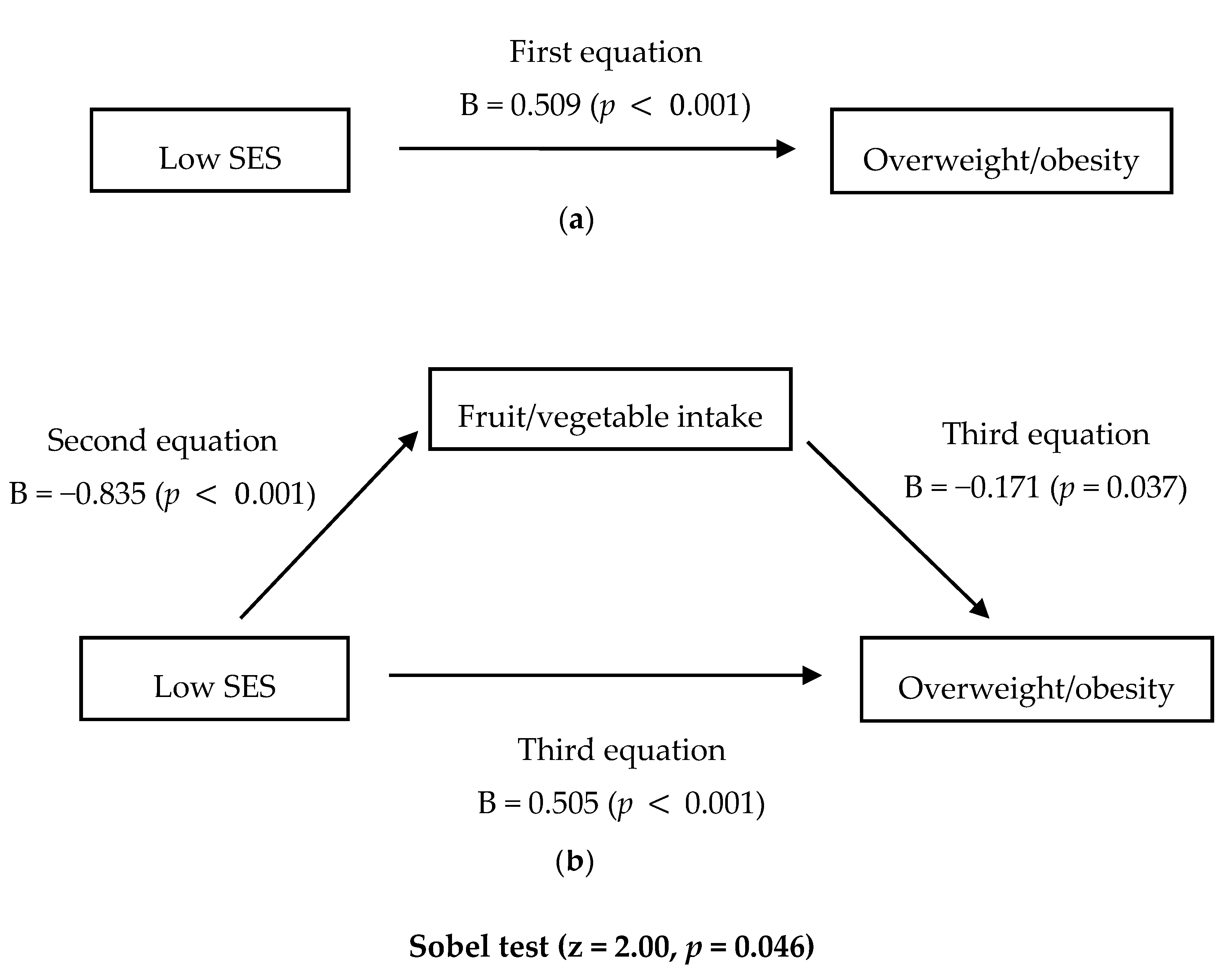
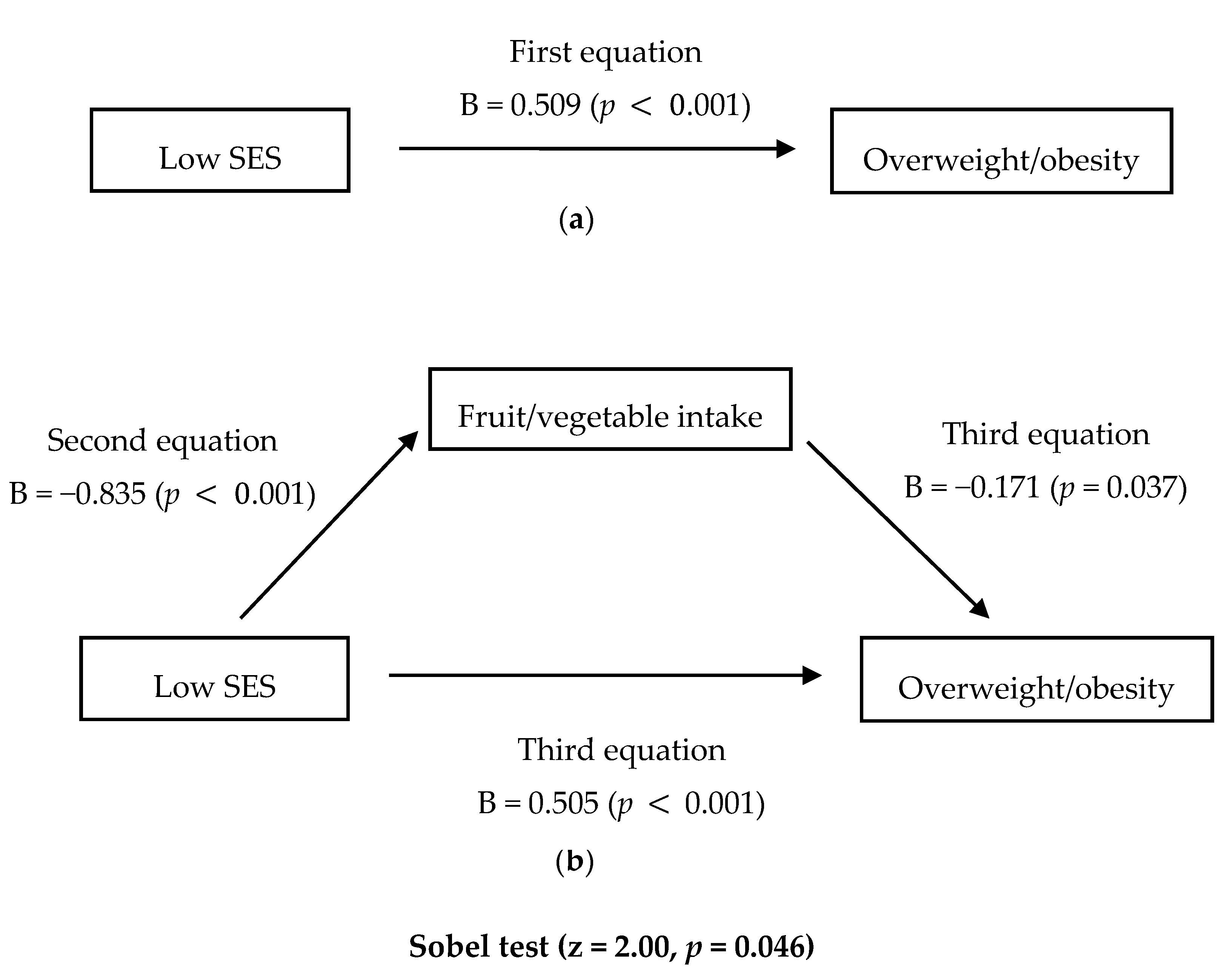
3.3. Testing of Four Hypotheses: Associations among SES, F/V Intakes, and Overweight/Obesity
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kosti, R.I.; Panagiotakos, D.B. The epidemic of obesity in children and adolescents in the world. Cent. Eur. J. Public Health 2006, 14, 151–159. [Google Scholar] [PubMed]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA 2014, 311, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Ogden, C.L.; Flegal, K.M.; Carroll, M.D.; Johnson, C.L. Prevalence and trends in overweight among US children and adolescents, 1999–2000. JAMA 2002, 288, 1728–1732. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Welfare, Korea Center for Disease Control and Prevention. 2012 Korea National Health and Nutrition Examination Survey; Ministry of Health and Welfare, Korea Center for Disease Control and Prevention: Seoul, Korea, 2012. [Google Scholar]
- Deshmukh-Taskar, P.; Nicklas, T.A.; Morales, M.; Yang, S.J.; Zakeri, I.; Berenson, G.S. Tracking of overweight status from childhood to young adulthood: The Bogalusa Heart Study. Eur. J. Clin. Nutr. 2006, 60, 48–57. [Google Scholar] [CrossRef] [PubMed]
- The, N.S.; Suchindran, C.; North, K.E.; Popkin, B.M.; Gordon-Larsen, P. Association of adolescent obesity with risk of severe obesity in adulthood. JAMA 2010, 304, 2042–2047. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, R.C.; Wright, J.A.; Pepe, M.S.; Seidel, K.D.; Dietz, W.H. Predicting obesity in young adulthood from childhood and parental obesity. N. Engl. J. Med. 1997, 337, 869–873. [Google Scholar] [CrossRef] [PubMed]
- Biro, F.M.; Wien, M. Childhood obesity and adult morbidities. Am. J. Clin. Nutr. 2010, 91, 1499s–1505s. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.J.; Kelly, J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: Systematic review. Int. J. Obes. (Lond.) 2011, 35, 891–898. [Google Scholar] [CrossRef] [PubMed]
- Weiss, R.; Dziura, J.; Burgert, T.S.; Tamborlane, W.V.; Taksali, S.E.; Yeckel, C.W.; Allen, K.; Lopes, M.; Savoye, M.; Morrison, J.; et al. Obesity and the metabolic syndrome in children and adolescents. N. Engl. J. Med. 2004, 350, 2362–2374. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.K.; Kogan, M.D.; Van Dyck, P.C.; Siahpush, M. Racial/ethnic, socioeconomic, and behavioral determinants of childhood and adolescent obesity in the United States: Analyzing independent and joint associations. Ann. Epidemiol. 2008, 18, 682–695. [Google Scholar] [CrossRef] [PubMed]
- Barriuso, L.; Miqueleiz, E.; Albaladejo, R.; Villanueva, R.; Santos, J.M.; Regidor, E. Socioeconomic position and childhood-adolescent weight status in rich countries: A systematic review, 1990–2013. BMC Pediatr. 2015, 15, 129. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.K.; Siahpush, M.; Kogan, M.D. Neighborhood socioeconomic conditions, built environments, and childhood obesity. Health Aff. (Millwood) 2010, 29, 503–512. [Google Scholar] [CrossRef] [PubMed]
- Zahnd, W.E.; Rogers, V.; Smith, T.; Ryherd, S.J.; Botchway, A.; Steward, D.E. Gender-specific relationships between socioeconomic disadvantage and obesity in elementary school students. Prev. Med. (Baltim.) 2015, 81, 138–141. [Google Scholar] [CrossRef] [PubMed]
- Bazzano, L.A.; He, J.; Ogden, L.G.; Loria, C.M.; Vupputuri, S.; Myers, L.; Whelton, P.K. Fruit and vegetable intake and risk of cardiovascular disease in US adults: The first National Health and Nutrition Examination Survey Epidemiologic Follow-up Study. Am. J. Clin. Nutr. 2002, 76, 93–99. [Google Scholar] [PubMed]
- Llewellyn, A.; Simmonds, M. Childhood obesity as a predictor of morbidity in adulthood: A systematic review and meta-analysis. Obes. Rev. 2016, 17, 56–67. [Google Scholar] [CrossRef] [PubMed]
- Van Duyn, M.A.; Pivonka, E. Overview of the health benefits of fruit and vegetable consumption for the dietetics professional: Selected literature. J. Am. Diet. Assoc. 2000, 100, 1511–1521. [Google Scholar] [CrossRef]
- Ledoux, T.A.; Hingle, M.D.; Baranowski, T. Relationship of fruit and vegetable intake with adiposity: A systematic review. Obes. Rev. 2011, 12, e143–e150. [Google Scholar] [CrossRef] [PubMed]
- Bes-Rastrollo, M.; Martinez-Gonzalez, M.A.; Sanchez-Villegas, A.; de la Fuente Arrillaga, C.; Martinez, J.A. Association of fiber intake and fruit/vegetable consumption with weight gain in a Mediterranean population. Nutrition 2006, 22, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Heo, M.; Kim, R.S.; Wylie-Rosett, J.; Allison, D.B.; Heymsfield, S.B.; Faith, M.S. Inverse association between fruit and vegetable intake and BMI even after controlling for demographic, socioeconomic and lifestyle factors. Obes. Facts 2011, 4, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Pitel, L.; Madarasova Geckova, A.; Reijneveld, S.A.; van Dijk, J.P. Socioeconomic differences in adolescent health-related behavior differ by gender. J. Epidemiol. 2013, 23, 211–218. [Google Scholar] [PubMed]
- Ministry of Education Science and Technology; Ministry of Health and Welfare; Korea Center for Disease Control and Prevention. Korea Youth Risk Behavior Web-based Survey 2013. Available online: http://yhs.cdc.go.kr/new/ (accessed on 19 December 2015).
- Korea Centers for Disease Control and Prevention. The Statistics of 9th Korea Youth Risk Behavior Web-Based Survey (KYRBWS) in 2013. Available online: http://yhs.cdc.go.kr/ (accessed on 19 December 2015).
- Goodman, E.; Huang, B.; Schafer-Kalkhoff, T.; Adler, N.E. Perceived socioeconomic status: A new type of identity that influences adolescents’ self-rated health. J. Adolesc. Health 2007, 41, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Quon, E.C.; McGrath, J.J. Subjective socioeconomic status and adolescent health: A meta-analysis. Health Psychol. 2014, 33, 433–447. [Google Scholar] [CrossRef] [PubMed]
- Finger, J.D.; Varnaccia, G.; Tylleskar, T.; Lampert, T.; Mensink, G.B. Dietary behaviour and parental socioeconomic position among adolescents: The German Health Interview and Examination Survey for Children and Adolescents 2003–2006 (KiGGS). BMC Public Health 2015, 15, 498. [Google Scholar] [CrossRef] [PubMed]
- Fradkin, C.; Wallander, J.L.; Elliott, M.N.; Tortolero, S.; Cuccaro, P.; Schuster, M.A. Associations between socioeconomic status and obesity in diverse, young adolescents: Variation across race/ethnicity and gender. Health Psychol. 2015, 34, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Welfare. Health Plan 2020; Ministry of Health and Welfare: Seoul, Korea, 2011. [Google Scholar]
- Park, S.; Choi, B.Y.; Wang, Y.; Colantuoni, E.; Gittelsohn, J. School and neighborhood nutrition environment and their association with students’ nutrition behaviors and weight status in Seoul, South Korea. J. Adolesc. Health 2013, 53, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.G.; Kim, J.Y.; Kim, K.Y.; Park, S.W.; Bae, J.; Lee, W.K. Changes in dietary behavior among adolescents and their association with government nutrition policies in Korea, 2005–2009. J. Prev. Med. Public Health 2012, 45, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Welfare. Dietary Guidelines for Adolescent; Ministry of Health and Welfare: Seoul, Korea, 2009. [Google Scholar]
- Centers for Disease Control and Prevention. 2008 Physical Activity Guidelines for Americans; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2008. [Google Scholar]
- Tremblay, M.S.; LeBlanc, A.G.; Janssen, I.; Kho, M.E.; Hicks, A.; Murumets, K.; Colley, R.C.; Duggan, M. Canadian sedentary behaviour guidelines for children and youth. Appl. Physiol. Nutr. Metab. 2011, 36, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Korea Center for Disease Control and Prevention; The Korean Pediatric Society. 2007 Korean National Growth Charts; Korea Center for Disease Control and Prevention, The Korean Pediatric Society: Seoul, Korea, 2007. [Google Scholar]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Sobel, M.E. Asymptotic confidence intervals for indirect effects in structural equation models. Sociol. Methodol. 1982, 13, 290–312. [Google Scholar] [CrossRef]
- Frederick, C.B.; Snellman, K.; Putnam, R.D. Increasing socioeconomic disparities in adolescent obesity. Proc. Natl. Acad. Sci. USA 2014, 111, 1338–1342. [Google Scholar] [CrossRef] [PubMed]
- Stamatakis, E.; Wardle, J.; Cole, T.J. Childhood obesity and overweight prevalence trends in England: Evidence for growing socioeconomic disparities. Int. J. Obes. (Lond.) 2010, 34, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Currie, C. Social Determinants of Health and Well-Being among Young People; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2012. [Google Scholar]
- Soh, C.-H.S. Sexual equality, male superiority, and Korean women in politics: Changing gender relations in a “patriarchal democracy”. Sex Roles. 1993, 28, 73–90. [Google Scholar] [CrossRef]
- Wang, W. Son preference and educational opportunities of children in China—“I wish you were a boy!”. Gend. Issues 2005, 22, 3–30. [Google Scholar] [CrossRef]
- Rolls, B.J.; Ello-Martin, J.A.; Tohill, B.C. What can intervention studies tell us about the relationship between fruit and vegetable consumption and weight management? Nutr. Rev. 2004, 62, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Whigham, L.D.; Valentine, A.R.; Johnson, L.K.; Zhang, Z.; Atkinson, R.L.; Tanumihardjo, S.A. Increased vegetable and fruit consumption during weight loss effort correlates with increased weight and fat loss. Nutr. Diabetes. 2012, 2, e48. [Google Scholar] [CrossRef] [PubMed]
- Sweeting, H.N. Gendered dimensions of obesity in childhood and adolescence. Nutr. J. 2008, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Glanz, K. The role of built environments in physical activity, eating, and obesity in childhood. Future. Child. 2006, 16, 89–108. [Google Scholar] [CrossRef] [PubMed]
- Campbell, M.K. Biological, environmental, and social influences on childhood obesity. Pediatr. Res. 2016. [Google Scholar] [CrossRef] [PubMed]
- Bae, J.; Joung, H.; Kim, J.Y.; Kwon, K.N.; Kim, Y.; Park, S.W. Validity of self-reported height, weight, and body mass index of the Korea Youth Risk Behavior Web-based Survey questionnaire. J. Prev. Med. Public. Health 2010, 43, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Sherry, B.; Jefferds, M.E.; Grummer-Strawn, L.M. Accuracy of adolescent self-report of height and weight in assessing overweight status: A literature review. Arch. Pediatr. Adolesc. Med. 2007, 161, 1154–1161. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| n (Weighted %), Mean (SE) | t/χ2 | p | ||||||
|---|---|---|---|---|---|---|---|---|
| All | Girls | Boys | ||||||
| (n = 31,343) | (n = 31,768) | |||||||
| Sociodemographic Characteristics | ||||||||
| Age | 14.8 | (0.05) | 14.9 | (0.06) | 14.7 | (0.07) | 1.54 | <0.001 |
| School type | 7.24 | 0.518 | ||||||
| Middle | 31,894 | (53.5) | 16,102 | (54.0) | 15,792 | (52.9) | ||
| High | 31,217 | (46.5) | 15,241 | (46.0) | 15,976 | (47.1) | ||
| Learning achievement | 151.85 | <0.001 | ||||||
| High | 7057 | (11.5) | 3086 | (9.9) | 3971 | (13.0) | ||
| Low | 56,054 | (88.5) | 28,257 | (90.1) | 27,797 | (87.0) | ||
| Residental setting | 74.67 | 0.166 | ||||||
| City | 55,717 | (89.2) | 27,925 | (90.3) | 27,792 | (88.2) | ||
| Rural | 7394 | (10.8) | 3418 | (9.7) | 3976 | (11.8) | ||
| Living arrangement | 30.47 | 0.023 | ||||||
| With family | 60,607 | (96.3) | 30,201 | (96.7) | 30,406 | (95.9) | ||
| Without family | 2504 | (3.7) | 1142 | (3.3) | 1362 | (4.1) | ||
| Parents’ nationality | 0.001 | 0.976 | ||||||
| Korean | 62,460 | (99.0) | 31,010 | (99.0) | 31,450 | (99.0) | ||
| Foreign | 651 | (1.0) | 333 | (1.0) | 318 | (1.0) | ||
| SES | 16.90 | 0.026 | ||||||
| High | 55,685 | (88.6) | 27,520 | (88.1) | 28,165 | (89.1) | ||
| Low | 7426 | (11.4) | 3826 | (11.9) | 3603 | (10.9) | ||
| Behavioral characteristics | ||||||||
| F/V intakes (per day) 1 | 11.61 | 0.004 | ||||||
| Low | 59,695 | (94.5) | 29,728 | (94.8) | 29,967 | (94.2) | ||
| High | 3416 | (5.5) | 1615 | (5.2) | 1801 | (5.8) | ||
| Fast-food intakes | 4.09 | 0.146 | ||||||
| Ever-consuming | 43,530 | (68.9) | 21,484 | (68.5) | 22,046 | (69.2) | ||
| Never-consuming | 19,581 | (31.1) | 9859 | (31.5) | 9722 | (30.8) | ||
| Regular exercise 2 | 1095.37 | <0.001 | ||||||
| Low | 60,212 | (95.3) | 30,763 | (98.1) | 29,449 | (92.5) | ||
| High | 2899 | (4.7) | 580 | (1.9) | 2319 | (7.5) | ||
| Sedentary behavior 3 | 250.57 | <0.001 | ||||||
| High | 38,207 | (60.8) | 19,982 | (63.8) | 18,225 | (57.7) | ||
| Low | 24,904 | (39.2) | 11,3611 | (36.2) | 13,543 | (42.3) | ||
| Anthropometric characteristics | ||||||||
| BMI | 43.52 | <0.001 | ||||||
| Non-overweight/obese | 54,076 | (85.7) | 27,145 | (86.6) | 26,931 | (84.8) | ||
| Overweight/obese | 9035 | (14.3) | 4198 | (13.4) | 4837 | (15.2) | ||
| Characteristics | Girls (n = 31,343) | Boys (n = 31,768) | ||||
|---|---|---|---|---|---|---|
| OR | (CI) | p | OR | (CI) | p | |
| Sociodemographic Characteristics | ||||||
| Age (ref: younger) | 0.84 | (0.78–0.91) | <0.001 | 1.07 | (1.00–1.15) | 0.065 |
| School type (ref: middle schools) | 1.08 | (1.00–1.17) | 0.045 | 1.06 | (0.98–1.14) | 0.158 |
| Residential setting (ref: city) | 1.10 | (1.00–1.22) | 0.066 | 0.95 | (0.83–1.09) | 0.467 |
| Living arrangement (ref: with family) | 0.98 | (0.84–1.15) | 0.810 | 0.91 | (0.77–1.08) | 0.282 |
| Learning achievement (ref: high) | 1.38 | (1.23–1.54) | <0.001 | 1.22 | (1.11–1.35) | <0.001 |
| Parents’ nationality (ref: Korean) | 1.11 | (0.83–1.49) | 0.496 | 0.76 | (0.54–1.07) | 0.115 |
| SES (ref: high) | 1.66 | (1.52–1.80) | <0.001 | 1.13 | (1.02–1.25) | 0.020 |
| Behavioral Characteristic | ||||||
| F/V intakes (ref: low) 1 | 0.84 | (0.71–0.98) | 0.026 | 0.93 | (0.81–1.05) | 0.233 |
| Fast-food intakes (ref: never-consuming) | 0.76 | (0.72–0.82) | <0.001 | 0.86 | (0.80–0.92) | <0.001 |
| Regular exercise (ref: low) 2 | 1.03 | (0.81–1.31) | 0.798 | 0.79 | (0.69–0.90) | <0.001 |
| Sedentary behavior (ref: low) 3 | 1.06 | (1.00–1.13) | 0.071 | 1.04 | (0.97–1.12) | 0.295 |
| Variables | Girls 1 | Boys 1 | ||||
|---|---|---|---|---|---|---|
| B | SE | p | B | SE | p | |
| First equation | ||||||
| Outcome: overweight/obesity | ||||||
| Predictor: low SES | 0.509 | 0.042 | <0.001 | 0.093 | 0.052 | 0.076 |
| Second equation | ||||||
| Outcome: F/V intake | ||||||
| Predictor: low SES | −0.835 | 0.113 | <0.001 | −0.765 | 0.119 | <0.001 |
| Third equation | ||||||
| Outcome: overweight /obesity | ||||||
| Mediator: F/V intake | −0.171 | 0.082 | 0.038 | −0.040 | 0.068 | 0.554 |
| Predictor: low SES | 0.505 | 0.042 | <0.001 | 0.092 | 0.053 | 0.082 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
You, J.; Choo, J. Adolescent Overweight and Obesity: Links to Socioeconomic Status and Fruit and Vegetable Intakes. Int. J. Environ. Res. Public Health 2016, 13, 307. https://doi.org/10.3390/ijerph13030307
You J, Choo J. Adolescent Overweight and Obesity: Links to Socioeconomic Status and Fruit and Vegetable Intakes. International Journal of Environmental Research and Public Health. 2016; 13(3):307. https://doi.org/10.3390/ijerph13030307
Chicago/Turabian StyleYou, Jihyun, and Jina Choo. 2016. "Adolescent Overweight and Obesity: Links to Socioeconomic Status and Fruit and Vegetable Intakes" International Journal of Environmental Research and Public Health 13, no. 3: 307. https://doi.org/10.3390/ijerph13030307