
Temporal Trends in Geographical Variation in Breast Cancer Mortality in China, 1973–2005: An Analysis of Nationwide Surveys on Cause of Death


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
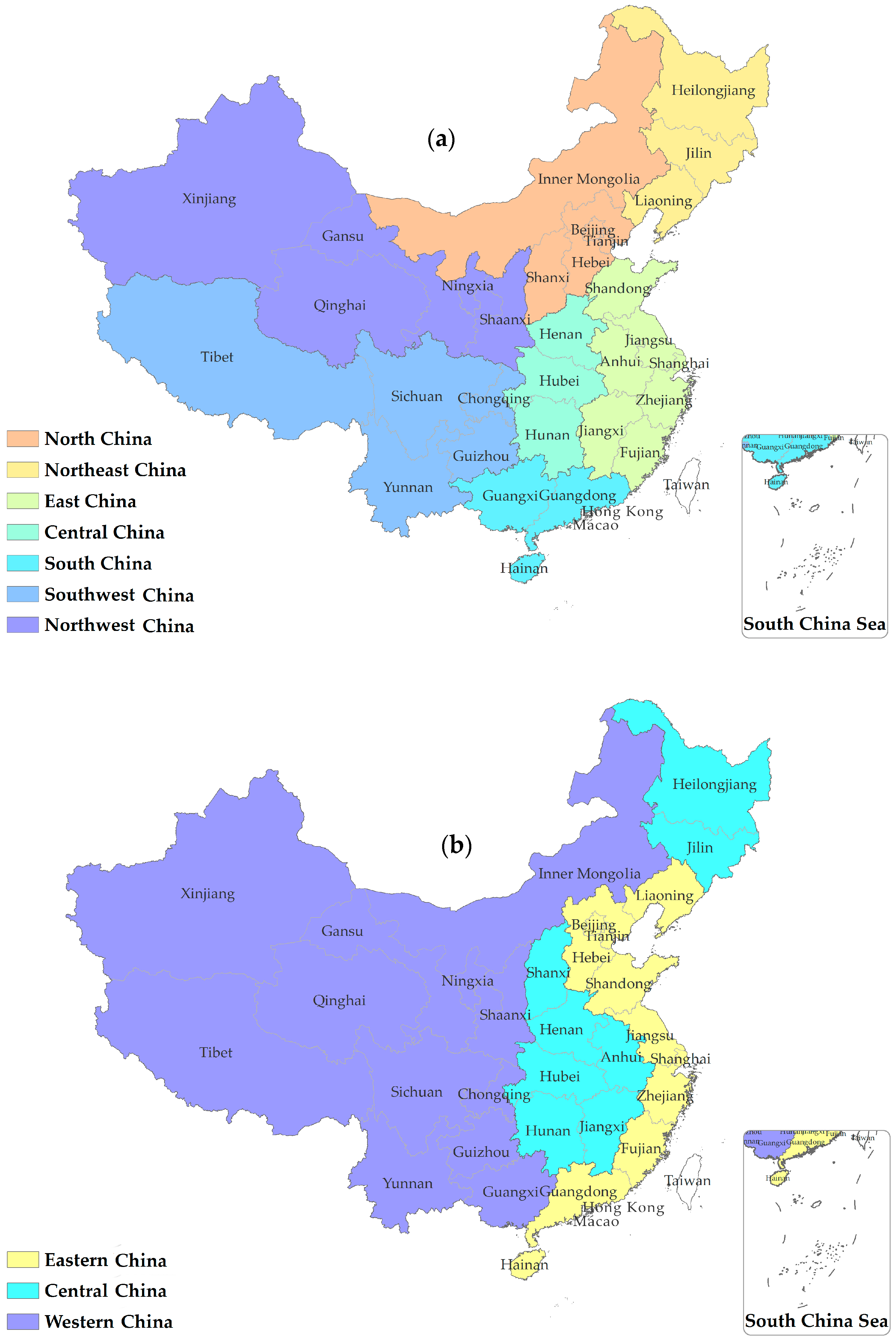
2.2. Geographical Unit Used in Analyses
2.3. Data Analysis
3. Results
3.1. Age-Standardized Mortality Rate
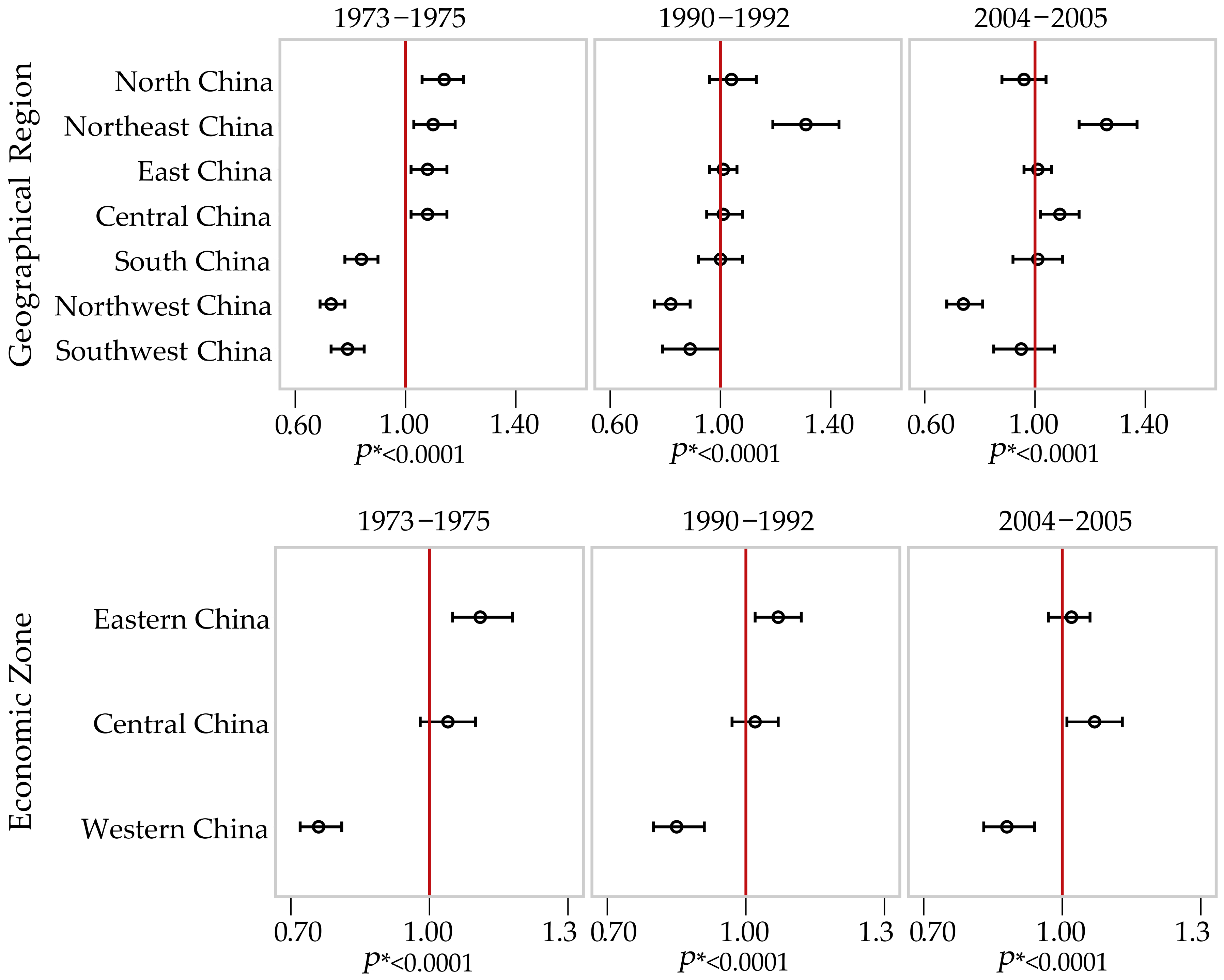
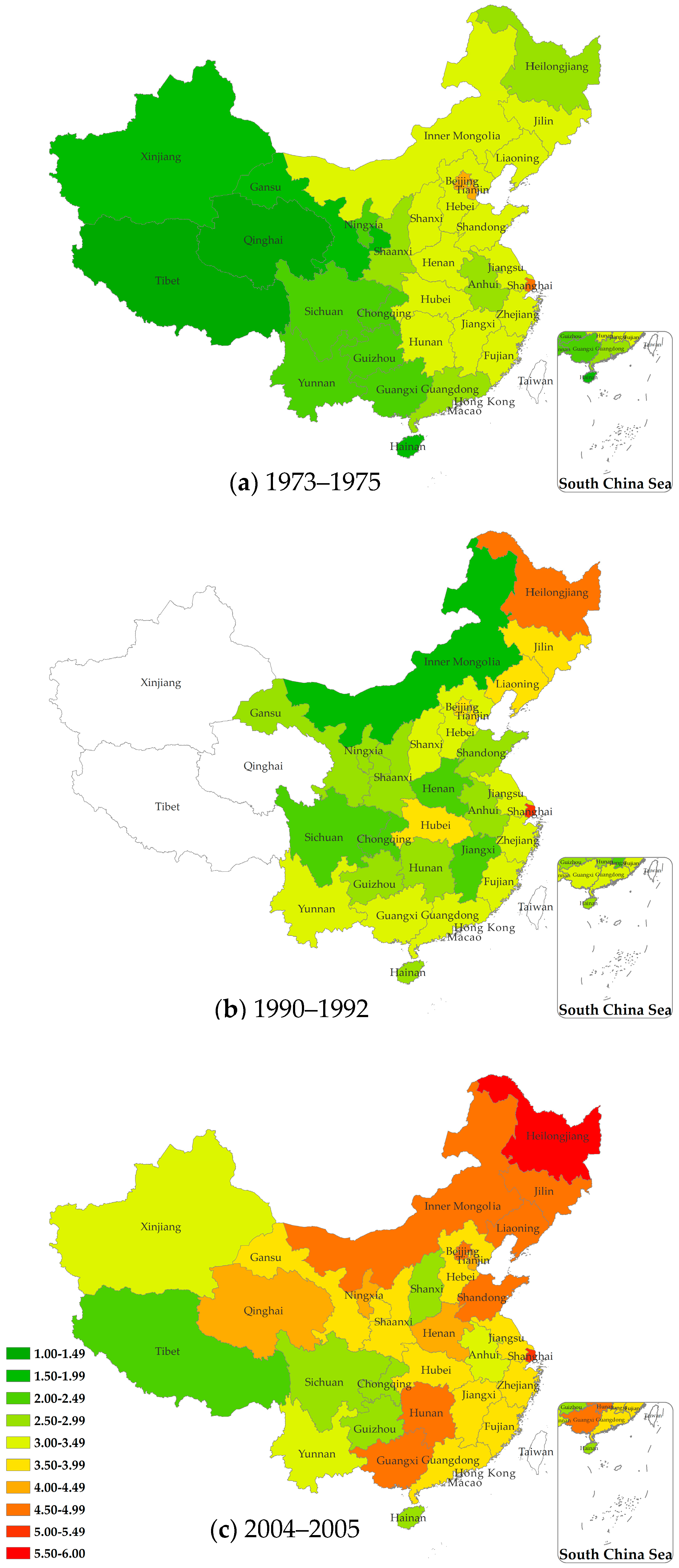
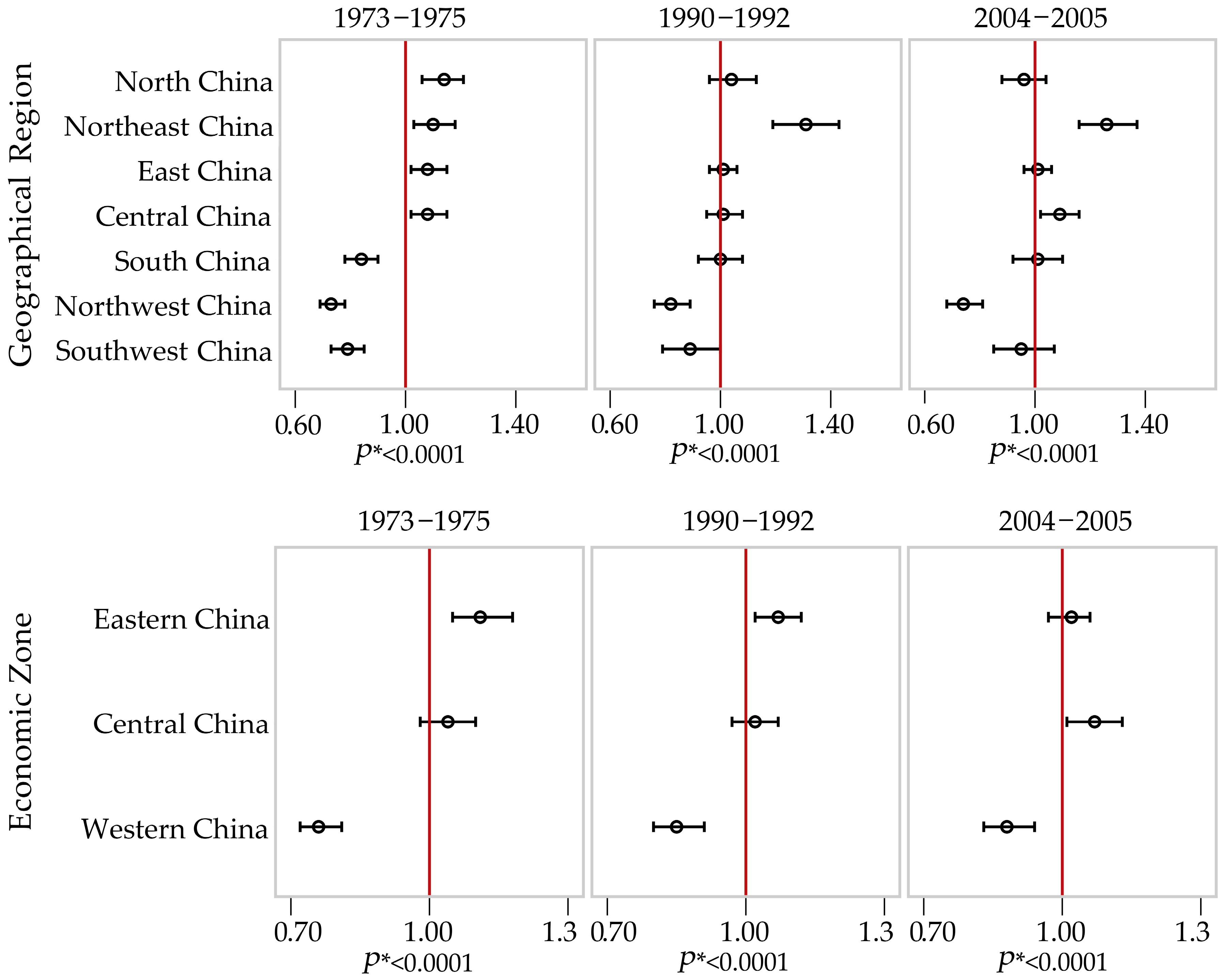
3.2. Geographical Variation over Time
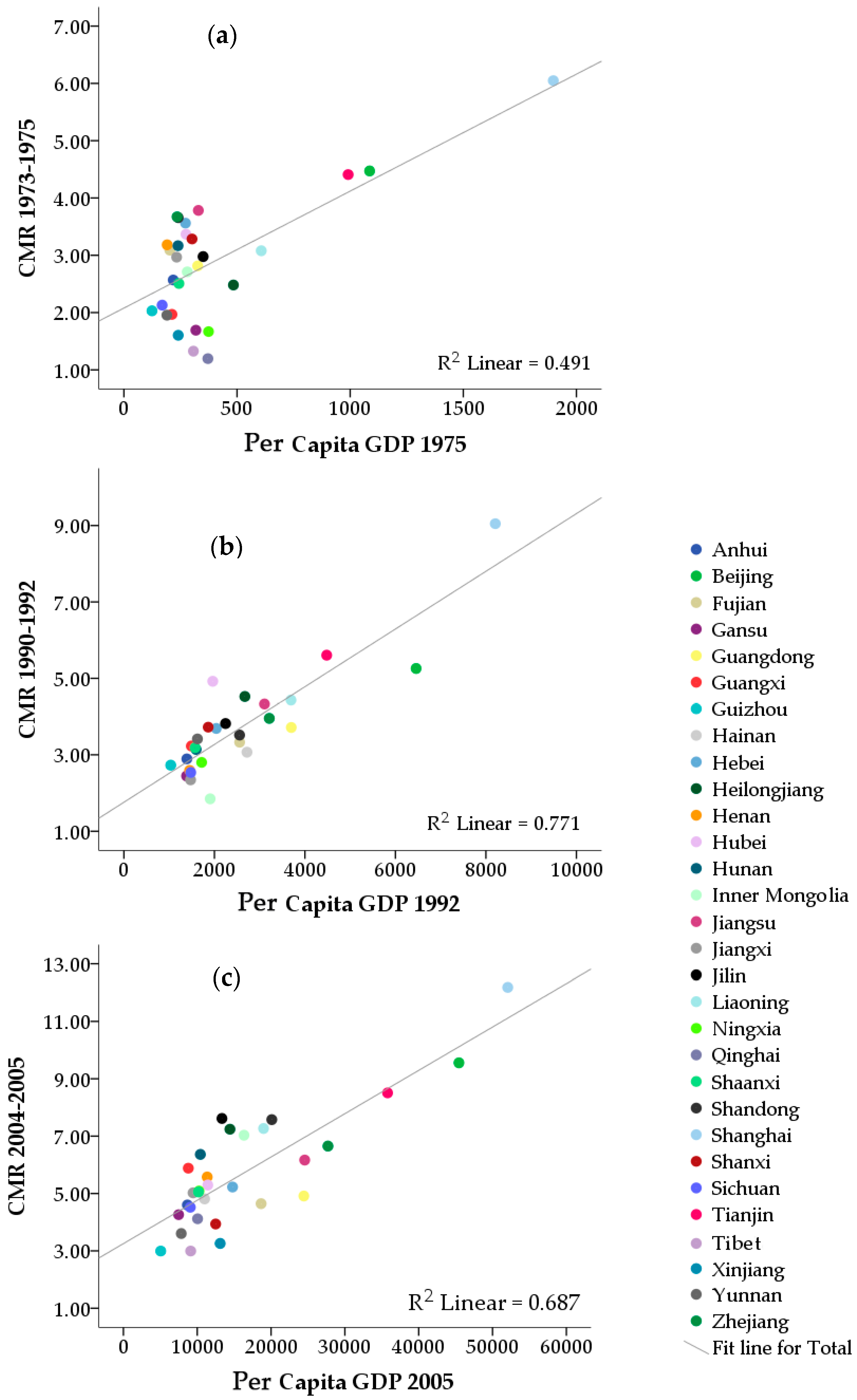
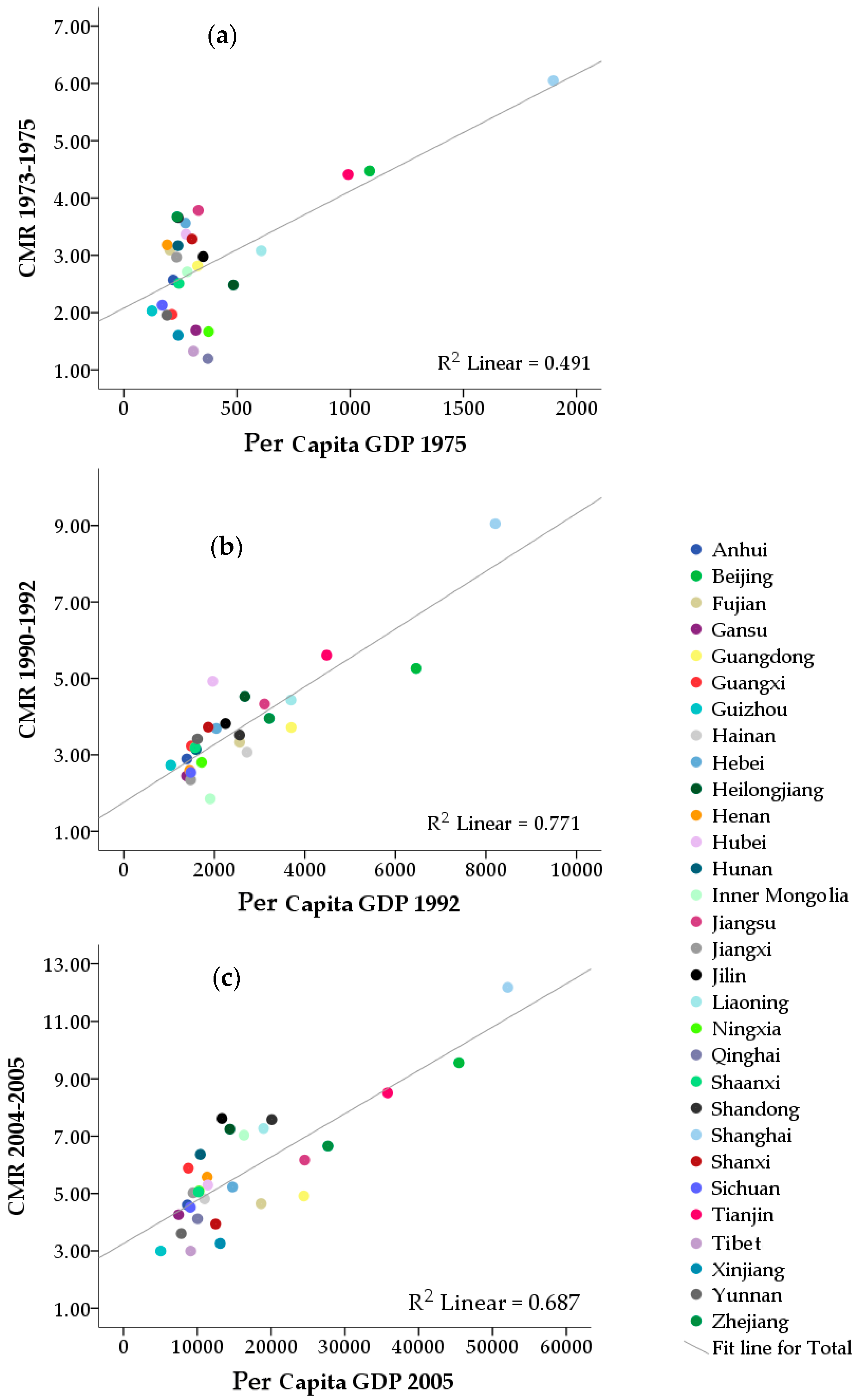
3.3. Correlation Analysis
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A
- North China (Beijing, Tianjin, Shanxi, Hebei, Inner Mongolia Autonomous Region)
- Northeast China (Heilongjiang, Jilin, Liaoning)
- East China (Shanghai, Jiangsu, Zhejiang, Anhui, Jiangxi, Shandong, Fujian)
- Central China (Henan, Hubei, Hunan)
- South China (Guangdong, Guangxi, Hainan)
- Southwest China (Chongqing, Sichuan, Guizhou, Yunnan, Tibet)
- Northwest China (Shaanxi, Gansu, Qinghai, Ningxia Hui Autonomous Region, Xinjiang Uygur Autonomous Region)
Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Deaths | Population | Per Capita GPD | Number of Deaths | Population | Per Capita GPD | Number of Deaths | Population | Per Capita GPD | |
|---|---|---|---|---|---|---|---|---|---|
| 1973–1975 | 1990–1992 | 2004–2005 | |||||||
| Province | |||||||||
| Beijing | 533 | 11,921,385 | 1086 | 80 | 1,521,398 | 6458 | 120 | 1,255,754 | 45,444 |
| Tianjin | 441 | 10,003,046 | 991 | 68 | 1,213,045 | 4481 | 113 | 1,328,365 | 35,783 |
| Hebei | 2493 | 70,018,076 | 272 | 349 | 9,461,858 | 2040 | 209 | 3,998,627 | 14,782 |
| Shanxi | 1074 | 32,697,776 | 301 | 120 | 3,224,205 | 1862 | 124 | 3,149,896 | 12,495 |
| Inner Mongolia | 306 | 11,286,804 | 280 | 22 | 1,189,805 | 1906 | 94 | 1,336,708 | 16,331 |
| Liaoning | 1605 | 52,136,241 | 607 | 183 | 4,130,045 | 3693 | 285 | 3,921,907 | 18,983 |
| Jilin | 1019 | 34,233,741 | 350 | 142 | 3,720,631 | 2246 | 155 | 2,035,309 | 13,348 |
| Heilongjiang | 1010 | 40,709,250 | 484 | 182 | 4,022,425 | 2672 | 190 | 2,623,978 | 14,434 |
| Shanghai | 985 | 16,287,701 | 1898 | 183 | 2,022,405 | 8208 | 103 | 845,386 | 52,060 |
| Jiangsu | 3126 | 82,630,955 | 329 | 492 | 11,367,746 | 3106 | 537 | 8,708,157 | 24,560 |
| Zhejiang | 1894 | 51,588,553 | 235 | 350 | 8,855,355 | 3212 | 431 | 6,478,093 | 27,703 |
| Anhui | 1646 | 64,089,979 | 218 | 231 | 7,985,474 | 1390 | 252 | 5,477,507 | 8670 |
| Fujian | 949 | 30,708,605 | 203 | 150 | 4,505,502 | 2557 | 154 | 3,314,821 | 18,646 |
| Jiangxi | 1222 | 41,191,696 | 233 | 124 | 5,290,316 | 1472 | 164 | 3,265,107 | 9440 |
| Shandong | 1963 | 53,688,310 | 240 | 363 | 10,323,297 | 2556 | 507 | 6,692,702 | 20,096 |
| Henan | 3134 | 98,471,373 | 191 | 284 | 10,955,314 | 1452 | 490 | 8,789,059 | 11,346 |
| Hubei | 2045 | 60,725,263 | 274 | 504 | 10,237,560 | 1962 | 291 | 5,495,822 | 11,431 |
| Hunan | 2213 | 69,870,339 | 239 | 296 | 9,424,817 | 1595 | 267 | 4,196,179 | 10,426 |
| Guangdong | 1777 | 63,123,805 | 326 | 417 | 11,227,881 | 3699 | 257 | 5,230,642 | 24,438 |
| Guangxi | 706 | 35,877,301 | 212 | 208 | 6,441,808 | 1490 | 245 | 4,164,893 | 8788 |
| Hainan | 127 | 5,711,874 | 326 | 26 | 847,327 | 2719 | 35 | 727,437 | 10,998 |
| Sichuan | 2811 | 132,015,851 | 169 | 322 | 12,685,421 | 1477 | 213 | 5,073,707 | 9060 |
| Guizhou | 723 | 35,608,036 | 124 | 148 | 5,424,985 | 1034 | 53 | 1,769,571 | 5052 |
| Yunnan | 813 | 41,588,565 | 190 | 197 | 5,768,515 | 1625 | 140 | 3,884,535 | 7835 |
| Tibet | 17 | 1,281,431 | 307 | * | * | 1468 | 6 | 200,357 | 9114 |
| Shaanxi | 892 | 35,584,375 | 243 | 148 | 4,642,551 | 1571 | 100 | 1,979,434 | 10,161 |
| Gansu | 369 | 21,802,163 | 318 | * | * | 1384 | 101 | 2,370,347 | 7477 |
| Qinghai | 57 | 4,765,301 | 371 | * | * | 1912 | 17 | 412,737 | 10,045 |
| Ningxia | 80 | 4,795,636 | 374 | 127 | 5,190,772 | 1718 | 36 | 707,641 | 10,239 |
| Xinjiang | 241 | 15,028,025 | 240 | 31 | 1,106,540 | 2477 | 48 | 1,472,894 | 13,108 |
| Geographical Region | |||||||||
| North China | 4847 | 135,927,087 | 639 | 16,610,311 | 660 | 11,069,350 | |||
| Northeast China | 3634 | 127,079,232 | 507 | 11,873,101 | 630 | 8,581,194 | |||
| East China | 11,785 | 340,185,799 | 1893 | 50,350,065 | 2148 | 34,781,773 | |||
| Central China | 7392 | 229,066,975 | 1084 | 30,617,691 | 1048 | 18,481,060 | |||
| South China | 2610 | 104,712,980 | 651 | 18,517,016 | 537 | 10,122,972 | |||
| Southwest China | 4364 | 210,493,883 | 667 | 23,878,939 | 558 | 13,799,681 | |||
| Northwest China | 1639 | 81,975,500 | 306 | 10,939,863 | 302 | 6,943,053 | |||
| Economic zone | |||||||||
| Eastern China | 15,893 | 447,818,551 | 2661 | 65,475,829 | 2875 | 45,651,787 | |||
| Central China | 13,363 | 441,989,417 | 1883 | 54,860,742 | 1809 | 31,882,961 | |||
| Western China | 7015 | 339,633,488 | 1203 | 42,450,415 | 1199 | 26,244,335 | |||
Appendix C
| Code | Name | Areas | 1975 | 1992 | 2005 |
|---|---|---|---|---|---|
| 110000 | 北京市 | Beijing | 4.32 | 3.71 | 4.73 |
| 120000 | 天津市 | Tianjin | 4.25 | 3.76 | 4.36 |
| 130000 | 河北省 | Hebei | 3.20 | 3.28 | 3.55 |
| 140000 | 山西省 | Shanxi | 3.17 | 3.43 | 2.58 |
| 150000 | 内蒙古自治区 | Inner Mongolia | 3.34 | 1.74 | 4.80 |
| 210000 | 辽宁省 | Liaoning | 3.40 | 3.72 | 4.59 |
| 220000 | 吉林省 | Jilin | 3.49 | 3.76 | 4.82 |
| 230000 | 黑龙江省 | Heilongjiang | 2.85 | 4.63 | 5.69 |
| 310000 | 上海市 | Shanghai | 4.80 | 5.03 | 5.21 |
| 320000 | 江苏省 | Jiangsu | 3.50 | 3.22 | 3.63 |
| 330000 | 浙江省 | Zhejiang | 3.40 | 3.02 | 3.84 |
| 340000 | 安徽省 | Anhui | 2.56 | 2.59 | 3.38 |
| 350000 | 福建省 | Fujian | 3.26 | 3.10 | 3.61 |
| 360000 | 江西省 | Jiangxi | 3.07 | 2.45 | 3.62 |
| 370000 | 山东省 | Shandong | 3.19 | 2.95 | 4.56 |
| 410000 | 河南省 | Henan | 3.09 | 2.37 | 4.16 |
| 420000 | 湖北省 | Hubei | 3.42 | 3.94 | 3.90 |
| 430000 | 湖南省 | Hunan | 3.27 | 2.91 | 4.55 |
| 440000 | 广东省 | Guangdong | 2.66 | 3.17 | 3.67 |
| 450000 | 广西壮族自治区 | Guangxi | 2.16 | 3.07 | 4.53 |
| 460000 | 海南省 | Hainan | 1.92 | 2.96 | 2.79 |
| 500000 | 重庆市 | Chongqing | 2.24 | 2.20 | 2.92 |
| 510000 | 四川省 | Sichuan | 2.24 | 2.20 | 2.92 |
| 520000 | 贵州省 | Guizhou | 2.16 | 2.80 | 2.52 |
| 530000 | 云南省 | Yunnan | 2.01 | 3.10 | 3.01 |
| 540000 | 西藏自治区 | Tibet | 1.23 | 2.45 | |
| 610000 | 陕西省 | Shaanxi | 2.73 | 2.99 | 3.85 |
| 620000 | 甘肃省 | Gansu | 1.88 | 2.59 | 3.82 |
| 630000 | 青海省 | Qinghai | 1.48 | 4.15 | |
| 640000 | 宁夏回族自治区 | Ningxia | 2.41 | 2.61 | 4.36 |
| 650000 | 新疆维吾尔自治区 | Xinjiang | 1.97 | 3.12 |
Appendix D
| RR and 95% CI | |||
|---|---|---|---|
| 1973–1975 | 1990–1992 | 2004–2005 | |
| Geographical region | |||
| Northern China | 1.14 (1.06–1.21) | 1.04 (0.96–1.13) | 0.96 (0.88–1.04) |
| Northeast China | 1.10 (1.03–1.18) | 1.31 (1.19–1.43) | 1.26 (1.16–1.37) |
| East China | 1.08 (1.02–1.15) | 1.01 (0.96–1.06) | 1.01 (0.96–1.06) |
| Central China | 1.08 (1.02–1.15) | 1.01 (0.95–1.08) | 1.09 (1.02–1.16) |
| South China | 0.84 (0.78–0.90) | 1.00 (0.92–1.08) | 1.01 (0.92–1.10) |
| Northwest China | 0.73 (0.69–0.78) | 0.82 (0.76–0.89) | 0.74 (0.68–0.81) |
| Southwest China | 0.79 (0.73–0.85) | 0.89 (0.79–1.00) | 0.95 (0.85–1.07) |
| p-value for the effect of geographical region | <0.0001 | <0.0001 | <0.0001 |
| Economic zone | |||
| East China | 1.11 (1.05–1.18) | 1.07 (1.02–1.12) | 1.02 (0.97–1.06) |
| Central China | 1.04 (0.98–1.10) | 1.02 (0.97–1.07) | 1.07 (1.01–1.13) |
| Western China | 0.76 (0.72–0.81) | 0.85 (0.80–0.91) | 0.88 (0.83–0.94) |
| p-value for the effect of economic zone | <0.0001 | <0.0001 | <0.0001 |
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.Q.; Zheng, R.S.; Zhang, S.W.; Zeng, H.M.; Zuo, T.T.; Jia, M.M.; Xia, C.F.; Zou, X.N.; He, J. Report of Cancer Incidence and Mortality in China, 2012. China Cancer 2016, 25, 1–8. [Google Scholar]
- Fan, L.; Zheng, Y.; Yu, K.D.; Liu, G.Y.; Wu, J.; Lu, J.S.; Shen, K.W.; Shen, Z.Z.; Shao, Z.M. Breast cancer in a transitional society over 18 years: Trends and present status in Shanghai, China. Breast Cancer Res. Treat 2009, 117, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Fan, L.; Strasser-Weippl, K.; Li, J.J.; St Louis, J.; Finkelstein, D.M.; Yu, K.D.; Chen, W.Q.; Shao, Z.M.; Goss, P.E. Breast cancer in China. Lancet Oncol. 2014, 15, e279–e289. [Google Scholar] [CrossRef]
- Shi, X.J.; Au, W.W.; Wu, K.S.; Chen, L.X.; Lin, K. Mortality characteristics and prediction of female breast cancer in China from 1991 to 2011. Asian Pac. J. Cancer Prev. 2014, 15, 2785–2791. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Yu, C.; Wang, P. An age-period-cohort analysis of female breast cancer mortality from 1990–2009 in China. Int. J. Equity Health 2015. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Wu, C.X.; Wu, F. Status and trends of breast cancer mortality in Chinese females. Chin. J. Prev. Med. 2011, 45, 150–154. (In Chinese) [Google Scholar]
- Peng, X.D.; Peng, L.; Wu, K.S. An Analysis of Spatial Risk Factors on Breast Cancer by Using Geographic Information System. China Cancer 2015, 24, 805–810. (In Chinese) [Google Scholar]
- Fei, X.; Wu, J.; Kong, Z.; Christakos, G. Urban-rural disparity of breast cancer and socioeconomic risk factors in China. PLoS ONE 2015. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.G.; Wang, X.F.; Hu, J.P.; Li, G.L.; Chen, W.Q.; Zhang, S.W.; Wan, X.; Wang, L.J.; Xiang, C.; Hu, Y.S.; et al. Geographical distribution of cancer mortality in China, 2004–2005. Chin. J. Prev. Med. 2010, 44, 303–308. (In Chinese) [Google Scholar]
- The National Cancer Control Office of the Ministry of Health. China Cancer Death Survey; People’s Medical Publishing House: Beijing, China, 1980. (In Chinese)
- National Office for Cancer Prevention and Control. China Cancer Death Survey (1990–1992); People’s Medical Publishing House: Beijing, China, 2008. (In Chinese)
- Chen, Z. The Third National Retrospective Sampling Survey of Death Causes in China; China Union Medical University Press: Beijing, China, 2008. (In Chinese) [Google Scholar]
- Department of Comprehensive Statistics of National Bureau of Statistics. China Compendium of Statistics 1949–2008; China Statistics Press: Beijing, China, 2010. (In Chinese)
- National Bureau of Statistics of China. National Data. Available online: http://data.stats.gov.cn/easyquery.htm?cn=C01 (accessed on 17 May 2016).
- Ministry of Health of the People’s Republic of China. China Health Statistics Yearbook, 2006; China Union Medical University Press: Beijing, China, 2006. (In Chinese)
- Rubin, M.S.; Clouston, S.; Link, B.G. A fundamental cause approach to the study of disparities in lung cancer and pancreatic cancer mortality in the United States. Soc. Sci. Med. 2014, 100, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.Q.; Luo, Q.; Kahn, C.; O’Connell, D.L.; Houssami, N. Temporal trends show improved breast cancer survival in Australia but widening urban-rural differences. Breast 2015, 24, 524–527. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.Q.; Luo, Q.; Smith, D.P.; O’Connell, D.L.; Baade, P.D. Geographic variation in prostate cancer survival in New South Wales. Med. J. Aust. 2014, 200, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Wu, C.; Zhang, M. The epidemic and characteristics of female breast cancer in China. China Oncol. 2013, 23, 561–569. (In Chinese) [Google Scholar]
- Chen, W.; Zheng, R.; Baade, P.D.; Zhang, S.; Zeng, H.; Bray, F.; Jemal, A.; Yu, X.Q.; He, J. Cancer statistics in China, 2015. CA Cancer J. Clin. 2016, 66, 115–132. [Google Scholar] [CrossRef] [PubMed]
- Linos, E.; Spanos, D.; Rosner, B.A.; Linos, K.; Hesketh, T.; Qu, J.D.; Gao, Y.T.; Zheng, W.; Colditz, G.A. Effects of reproductive and demographic changes on breast cancer incidence in China: A modeling analysis. J. Natl. Cancer Inst. 2008, 100, 1352–1360. [Google Scholar] [CrossRef] [PubMed]
- Shi, X.J.; Zhang, X.J.; Wang, F.S.; Jiang, J.D.; Lin, K. Analysis on mortality distribution of female breast cancer in China, 1991–2010. Chin. J. Dis. Contr. Prev. 2012, 16, 743–747. (In Chinese) [Google Scholar]
- Yang, L.; Sun, T.; Yuan, Y.; Wang, N. Relationship between female breast cancer incidence and the socioeconomic status in Beijing. Chin. J. Oncol. 2014, 36, 713–716. (In Chinese) [Google Scholar]
- Yu, X.Q. Socioeconomic disparities in breast cancer survival: Relation to stage at diagnosis, treatment and race. BMC Cancer 2009. [Google Scholar] [CrossRef] [PubMed]
- Walsh, P.M.; Byrne, J.; Kelly, M.; McDevitt, J.; Comber, H. Socioeconomic disparity in survival after breast cancer in ireland: Observational study. PLoS ONE 2014. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.Q.; O’Connell, D.L.; Gibberd, R.W.; Armstrong, B.K. Assessing the impact of socio-economic status on cancer survival in New South Wales, Australia 1996–2001. Cancer Causes Contr. 2008, 19, 1383–1390. [Google Scholar] [CrossRef] [PubMed]
- Jin, Z.; Yang, Y.H.; Mei, Y.; Cheng, G.W. Relationship between Birth Number and Breast Cancer Risk of Chinese Female: A Meta-analysis. Chin. J. Evid.-Based Med. 2015, 15, 1148–1152. (In Chinese) [Google Scholar]
- Turkoz, F.P.; Solak, M.; Petekkaya, I.; Keskin, O.; Kertmen, N.; Sarici, F.; Arik, Z.; Babacan, T.; Ozisik, Y.; Altundag, K. Association between common risk factors and molecular subtypes in breast cancer patients. Breast 2013, 22, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Lian, Z.Q. Current status and challenges of screening and early diangosis for breast cancer in China. J. Chin. Oncol. 2011, 17, 321–324. (In Chinese) [Google Scholar]
- Davies, N.J.; Batehup, L.; Thomas, R. The role of diet and physical activity in breast, colorectal, and prostate cancer survivorship: A review of the literature. Br. J. Cancer 2011, 105 (Suppl. 1), S52–S73. [Google Scholar] [CrossRef] [PubMed]
- Shu, X.O.; Jin, F.; Dai, Q.; Shi, J.R.; Potter, J.D.; Brinton, L.A.; Hebert, J.R.; Ruan, Z.; Gao, Y.T.; Zheng, W. Association of body size and fat distribution with risk of breast cancer among Chinese women. Int. J. Cancer 2001, 94, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Mi, Y.J.; Zhang, B.; Wang, H.J.; Yan, J.; Han, W.; Zhao, J.; Liu, D.W.; Tian, Q.B. Prevalence and Secular Trends in Obesity Among Chinese Adults, 1991–2011. Am. J. Prev. Med. 2015, 49, 661–669. [Google Scholar] [CrossRef] [PubMed]
- He, M.; Guo, Q.; Hu, G. Reversed urban-rural differences in breast cancer mortality (China, 2002–2008). Breast Cancer Res. Treat 2011, 126, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Wen, W.; Zheng, Y.; Gao, Y.T.; Wu, C.; Bao, P.; Wang, C.; Gu, K.; Peng, P.; Gong, Y.; et al. Breast cancer incidence and mortality: Trends over 40 years among women in Shanghai, China. Ann. Oncol. 2016, 27, 1129–1134. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Bao, J.; Yu, C.; Wang, J.; Li, C. Secular Trends of Breast Cancer in China, South Korea, Japan and the United States: Application of the Age-Period-Cohort Analysis. Int. J. Environ. Res. Public Health 2015, 12, 15409–15418. [Google Scholar] [CrossRef] [PubMed]
- Zeng, H.; Zheng, R.; Guo, Y.; Zhang, S.; Zou, X.; Wang, N.; Zhang, L.; Tang, J.; Chen, J.; Wei, K.; et al. Cancer survival in China, 2003–2005: A population-based study. Int. J. Cancer 2015, 136, 1921–1930. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zhang, B.N.; Fan, J.H.; Pang, Y.; Zhang, P.; Wang, S.L.; Zheng, S.; Zhang, B.; Yang, H.J.; Xie, X.M.; et al. A nation-wide multicenter 10-year (1999–2008) retrospective clinical epidemiological study of female breast cancer in China. BMC Cancer 2011. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Hu, J.; Rao, K.Q.; Ma, J.; Rao, C.; Lopez, A.D. Mortality registration and surveillance in China: History, current situation and challenges. Popul. Health Metr. 2005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Z.; Chen, W.; Zhao, J.; Zhang, X. Mortality in China: Data Sources, Trends and Patterns. In Analysing China’s Population; Attané, I., Gu, B., Eds.; Springer: New York, NY, USA, 2014; pp. 205–225. [Google Scholar]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xia, C.; Kahn, C.; Wang, J.; Liao, Y.; Chen, W.; Yu, X.Q. Temporal Trends in Geographical Variation in Breast Cancer Mortality in China, 1973–2005: An Analysis of Nationwide Surveys on Cause of Death. Int. J. Environ. Res. Public Health 2016, 13, 963. https://doi.org/10.3390/ijerph13100963
Xia C, Kahn C, Wang J, Liao Y, Chen W, Yu XQ. Temporal Trends in Geographical Variation in Breast Cancer Mortality in China, 1973–2005: An Analysis of Nationwide Surveys on Cause of Death. International Journal of Environmental Research and Public Health. 2016; 13(10):963. https://doi.org/10.3390/ijerph13100963
Chicago/Turabian StyleXia, Changfa, Clare Kahn, Jinfeng Wang, Yilan Liao, Wanqing Chen, and Xue Qin Yu. 2016. "Temporal Trends in Geographical Variation in Breast Cancer Mortality in China, 1973–2005: An Analysis of Nationwide Surveys on Cause of Death" International Journal of Environmental Research and Public Health 13, no. 10: 963. https://doi.org/10.3390/ijerph13100963