2.1. Hysterectomy Specimens as a Tissue Source
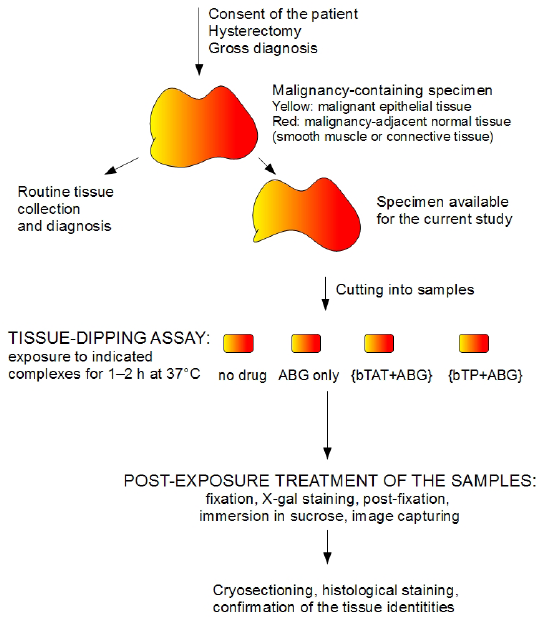
Our aim was to evaluate the possibility that the transportan and the TAT-peptide would differentiate between the different types of tissues, using a tissue-dipping assay. We defined tissue-dipping assay as the exposure of a tissue sample to the biotinylated transportan or the biotinylated TAT-peptide complexed with reporter cargo avidin-β-galactosidase (ABG) over 1–2 h at 37 °C in a well of a 12 or 24-well plate. The optimal specimen for our tissue-dipping assay (
Figure 1) had the following characteristics. First, the specimen contained two types of tissue and the visual discrimination of the tissues was possible even for a non-pathologist. Secondly, it was possible to cut the specimen so that each sample of the tissue-dipping assay contained approximately the same volume of each tissue type.
Figure 2.
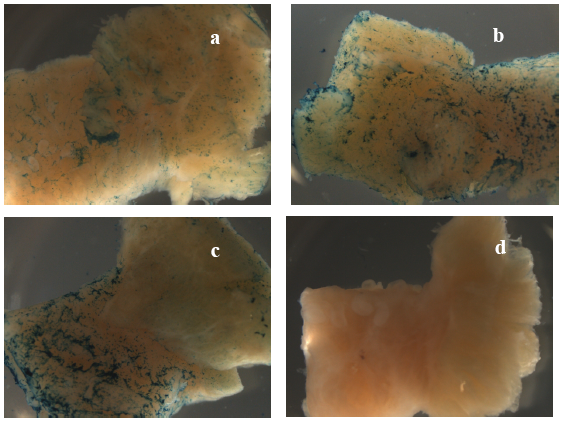
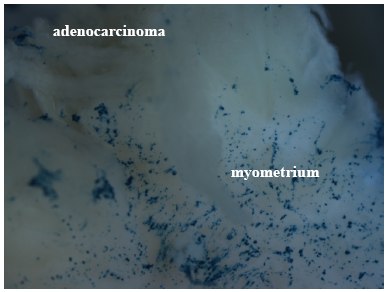
Macrophotographs (at 7.5x magnification) of tissue samples exposed to uncomplexed ABG (a), {bTAT+ABG} (b) and {bTP+ABG} (c) in the experiment abbreviated as “ACE_1” (see
Table 1 for details). The tissue samples were from the specimen diagnosed with stage IA adenocarcinoma of the endometrium (ACE). The myometrial parts of samples are directed to the left. The image of the negative control (“no drug”) is in panel d.
Figure 2.
Macrophotographs (at 7.5x magnification) of tissue samples exposed to uncomplexed ABG (a), {bTAT+ABG} (b) and {bTP+ABG} (c) in the experiment abbreviated as “ACE_1” (see
Table 1 for details). The tissue samples were from the specimen diagnosed with stage IA adenocarcinoma of the endometrium (ACE). The myometrial parts of samples are directed to the left. The image of the negative control (“no drug”) is in panel d.
These criteria were met best in early-stage adenocarcinomas of the endometrium (ACE). ACE is also known as endometrial/endometrioid adenocarcinoma or simply uterine/endometrial cancer. As ACE is the most common gynaecological malignancy [
11], specimens can be obtained relatively often. In stage I ACE specimens, the adenocarcinoma-containing epithelial tissue (endometrium) was readily discriminated from the adjacent normal smooth muscle tissue (myometrium). The discrimination was even easier after the fixation steps as the soft adenocarcinoma areas stood out more strikingly against the firmer myometrium (
Figure 2, panel d). The specimens were staged according to the current staging system of the International Federation of Obstetrics and Gynecology (FIGO). In the case of stage IA, the adenocarcinoma was limited to the endometrium (e.g., no invasions to the myometrium). In the case of stage IB, the adenocarcinoma invaded less than half the myometrium. However, the ACE specimens of stage IB were soft and some disaggregation occurred during the exposure step. Therefore, the exposure step was shortened to 1 h in the case of the ACE specimens of stage IB (as specified in
Table 1). In addition, because of the softness of the specimen, we did not trim the samples of the stage IB specimen to fit into the wells of the 24-well plate (as we did for the samples of the stage IA specimen). Instead we increased the exposure solution volume to 2 mL and performed the exposure in the wells of the 12-well plate. The histological grade of most of the ACE specimens was grade 1 (G1), meaning that the adenocarcinoma was well-differentiated and had a good prognosis.
Only two ACE specimens of a higher grade or stage filled the criteria of the optimal specimen. The first specimen had the rare combination of G1 and stage IIIB and the second specimen had the combination of G3 and IB. Histological grade 3 (G3) means that the carcinoma is poorly differentiated and has a poor prognosis. Stage IIIB means that the carcinoma has spread to the vagina but not to lymph nodes or distant sites.
ACE is a disease that predominantly affects post-menopausal women. This means that ideal controls—specimens from age-matched women containing normal endometria in their proliferative phase—do not exist. Unfortunately, the specimens from pre-menopausal women containing endometria in their proliferative phase were not available for this study. Therefore, we used a specimen from a patient who had been diagnosed with hyperplasia of the endometrium (excessive proliferation of the cells of the endometrium). The histological diagnosis of the specimen specified that the hyperplasia was without atypia, indicating a low probability for the development of cancer. The hyperplasia specimen filled the criteria of the optimal specimen: easily discriminated hyperplastic endometrium and adjacent normal myometrium and the possibility to cut the specimen so that each sample contained approximately the same volume of each tissue type. However, hysterectomies are routinely not performed in the case of endometrial hyperplasia, so hyperplasia specimens are rare.
Hysterectomies in patients diagnosed with squamous cell carcinoma of the cervix (SCCC) provided the specimens carrying the combination of squamous cell carcinoma tissue (e.g., epithelial malignant tissue) and the adjacent normal cervical stroma. The cervical stroma is mainly composed of fibrous connective tissue with small amounts elastic fibres and smooth muscle [
12]. The histological grade of both SCCC specimens was G3. The first SCCC specimen had stage IVB, meaning that the cancer had spread to distant organs beyond the pelvic area. The patient had also had previous chemotherapy. The second SCCC specimen had stage IB2, meaning that the cancer had grown into the cervix but had not spread anywhere else. This SCCC specimen had very little of the cervical stroma. In summary, the SCCC specimens were not fully optimal for the current study. However, the SCCC specimens were a valuable source of G3-carcinoma tissue and adjacent normal (mainly) connective tissue.
2.2. ABG (Avidin-β-Galactosidase) as a Reporter Cargo in Tissue-Dipping Experiments
In this study we used ABG as a reporter cargo. In ABG the β-galactosidase from
E. coli was labelled with avidin from egg white. The avidin part of ABG enabled complex formation with biotinylated CPPs (bCPPs). The β-galactosidase part enabled a robust detection system based on X-gal staining. The X-gal is the most widely used chromogenic substrate for β-galactosidase. The cleavage of the glycosidic linkage in X-gal by β-galactosidase produces colourless indoxyl moieties that are nonenzymatically dimerised and oxidised to halogenated indigo—A stable and insoluble blue compound. Dimerisation and oxidation require the presence of electron acceptors of the proper redox potential. We used the most widely used electron acceptors in the X-gal staining procedure—ferric and ferrous ions. The main concern when using β-galactosidase activity as a part of the reporter cargo is the endogenous β-galactosidase activity in tissues, a well-known problem in mice bearing the
lacZ-containing transgene [
12]. However, we never detected the endogenous β-galactosidase activity when we performed the whole-mount X-gal staining at pH 7.4, optimal for
E. coli β-galactosidase. In other words, we could not detect the blue indigo colour in our negative controls (“no drug”), or the tissue samples exposed to the protease inhibitor cocktail-containing RPMI medium only (panel d in
Figure 2,
Figure 3 and
Figure 4).
Figure 3.
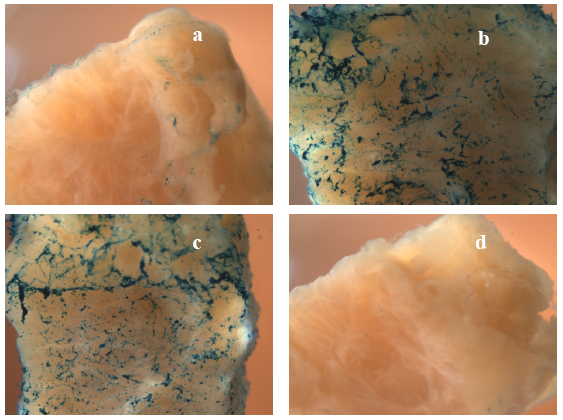
Macrophotographs (at 10x magnification) of tissue samples exposed to 60 μg of uncomplexed ABG (a), to a complex of 60 μg ABG with 5 μM bTP (b) and to a complex of 5 μg ABG with 5 μM bTP (c) in the experiment abbreviated as “SCCC_1” (see
Table 1 for details). The tissue samples were from the specimen diagnosed with stage IVB squamous cell carcinoma of the cervix (SCCC). The cervical stromal parts of samples are directed to the left (a, b, c) or down (d). The image of the negative control (“no drug”) is in panel d.
Figure 3.
Macrophotographs (at 10x magnification) of tissue samples exposed to 60 μg of uncomplexed ABG (a), to a complex of 60 μg ABG with 5 μM bTP (b) and to a complex of 5 μg ABG with 5 μM bTP (c) in the experiment abbreviated as “SCCC_1” (see
Table 1 for details). The tissue samples were from the specimen diagnosed with stage IVB squamous cell carcinoma of the cervix (SCCC). The cervical stromal parts of samples are directed to the left (a, b, c) or down (d). The image of the negative control (“no drug”) is in panel d.
Figure 4.
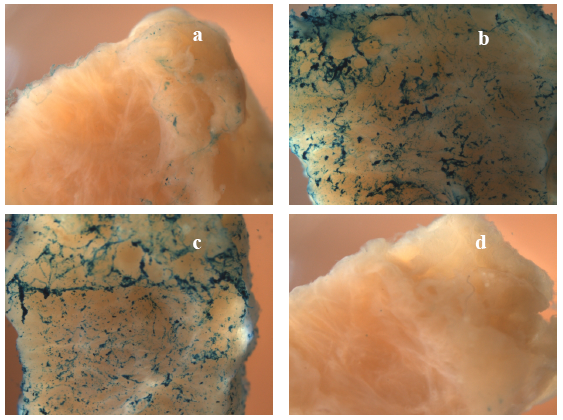
Macrophotographs (at 10x magnification) of tissue samples exposed to uncomplexed ABG (a), {bTAT+ABG} (b) and {bTP+ABG} (c) in the experiment abbreviated as “hyperplasia” (see
Table 1 for the details). The tissue samples were from the specimen diagnosed with hyperplasia of the endometrium without atypia. The image of the negative control (“no drug”) is in panel d.
Figure 4.
Macrophotographs (at 10x magnification) of tissue samples exposed to uncomplexed ABG (a), {bTAT+ABG} (b) and {bTP+ABG} (c) in the experiment abbreviated as “hyperplasia” (see
Table 1 for the details). The tissue samples were from the specimen diagnosed with hyperplasia of the endometrium without atypia. The image of the negative control (“no drug”) is in panel d.
As expected, endogenous β-galactosidase activity could be readily detected when the pH was lowered to 6.1 (data not shown). The absence of endogenous β-galactosidase activity was the major factor that made us choose ABG as the reporter cargo in our study. In the preliminary experiments we also used fluorescence-based detection. In those experiments we complexed the bCPPs with mouse anti-biotin antibodies and studied the distribution of the complexes by immuno-fluorescence in the cryosections. However, the autofluorescence background was high throughout the visible spectrum, especially in the carcinoma tissue. This complicated the comparison of the distribution of the bCPP-antibody complexes between the carcinoma and the adjacent normal tissue and required extensive image processing.
In some experiments we noticed the development of green-yellow or brown colour in malignant epithelial tissue. Colour development was more intensive in the G3-carcinoma specimens than in the G1-carcinoma specimens or hyperplastic specimens. The colour development was detectable in all samples of those experiments, e.g., even in the negative control. The most striking example is visualised in
Figure 3, panel d. This colour development is most likely due to the production of Prussian green or related products from the ferricyanide and ferrocyanide. The brown colour developed during the staining step and changed to green-yellow when 4% PFA in PBS was used as the post-fixation agent (experiment “ACE_6”,
Table 1) and remained brown when glutaraldehyde was used as a post-fixation agent (experiment “SCCC_1”,
Table 1 and
Figure 4). Whether or not the colour development correlates with the malignancy grade and reflects the redox state of the carcinoma remains to be studied.
Whole-mount X-gal staining was readily detectable when the amount of bCPP-complexed ABG in the tissue-dipping assay well was 33–66 μg (0.025–0.1 μM, see
Table 1 for details). When only 5 μg of ABG was complexed with bCPP, X-gal staining was remarkably weaker (
Figure 3 panel c). The tissue-uptake-enhancing effect of the TAT-peptide and the transportan was readily seen at concentrations of 15–20 μM. The 5 μM bCPP concentration provided readily detectable X-gal staining in experiment “SCCC_1” (
Figure 3), but only weak staining in experiments “ACE_3” and “SCCC_2” (see
Table 1 for details). Surprisingly, the further lowering of the bCPP concentration to 3.25 μM provided readily detectable X-gal staining in experiments “ACE_4” (
Figure 5), “ACE_5” and “ACE_6”. This could be due to the bCPP/ABG molar ratio, which was 50:1 in the experiments with overall weak staining (“ACE_3” and “SCCC_2”) and 55:1 or higher in the rest of the experiments.
Figure 5.
The macrophotograph (at 25x magnification) of the tissue sample exposed to {bTAT+ABG} in the experiment abbreviated as “ACE_4” (see
Table 1 for details). The tissue sample was from the specimen diagnosed with stage IB adenocarcinoma of the endometrium (ACE). Note the blue X-gal staining in the myometrium and the absence of the staining in the adenocarcinoma and its invasions into the myometrium.
Figure 5.
The macrophotograph (at 25x magnification) of the tissue sample exposed to {bTAT+ABG} in the experiment abbreviated as “ACE_4” (see
Table 1 for details). The tissue sample was from the specimen diagnosed with stage IB adenocarcinoma of the endometrium (ACE). Note the blue X-gal staining in the myometrium and the absence of the staining in the adenocarcinoma and its invasions into the myometrium.
2.3. Distribution of {bCPP+ABG} Complexes in Tissue Samples
In every experiment we could readily detect the enhancing effect of the transportan and the TAT-peptide (reflected in the last three columns in
Table 1 and in
Figure 2,
Figure 3,
Figure 4, panels a–c). In other words, the X-gal staining intensity of uncomplexed ABG was always lower than the X-gal staining intensity of {bTAT+ABG} and {bTP+ABG}. This was most prominent in the hyperplasia specimen (
Figure 4).
Table 1.
Results from the tissue-dipping experiments.
Table 1.
Results from the tissue-dipping experiments.
| Specimens | Experiment abbreviation and comments | Exposure solution parameters | Malignancy grade, stage | Character of X-gal staining, Figure number and panel |
| [bCPP] μM | ABG μg | molar ratio bCPP/ABG | ABG | {bTAT+ABG} | {bTP+ABG} |
| ACE specimens: contained malignant epithelial tissue (malignant endometrium, E) and adjacent histologically normal smooth muscle tissue (normal myometrium, M) | ACE_1 | 15 | 60 | 165:1 | G1, stage IA | even
Figure 2a | even
Figure 2b | M >> E
Figure 2c |
| ACE_2 | 15 | 66 | 150:1 | G1, stage IA | E > M | even | M > E |
| ACE_3§ | 5 | 66 | 50:1 | G1, stage IB | - | even* | even* |
| ACE_4§¥ | 3.25 | 33 | 65:1 | G1, stage IB | - | M >> E
Figure 5 | even* |
| ACE_5§¥ | 3.25 | 33 | 65:1 | G1, stage IIIB | - | even* | even |
| ACE_6§¥ | 3.25 | 33 | 65:1 | G3, stage IB | - | M > E | M > E |
| SCCC specimens: contained malignant epithelial tissue (E) and adjacent histologically normal cervical stroma (C) | SCCC_1
post-fixation with glutaraldehyde | 5
5 | 60
5 | 55:1
661:1 | G3, stage IVB previous chemotherapy | C > E
Figure 3a | not tested | C >> E
Figure 3b-c |
| SCCC_2 | 5 | 66 | 50:1 | G3, stage IB2 | - | even* | even* |
| Hyperplasia of the endometrium: contained hyperplastic endometrium and adjacent histo-logically normal myometrium | hyperplasia | 20 | 66 | 200:1 | - | -
Figure 4a | even
Figure 4b | even
Figure 4c |
We wanted to exclude the possibility that weak or non-detectable X-gal staining of uncomplexed ABG was due to its adherence to the walls of the wells, thereby diminishing the ABG available for the tissue. Therefore, we performed a quantitative luminescence-based analysis of the residual β-galactosidase activity of the exposure solutions. We found that in the case of the non-detectable X-gal staining in the tissue samples exposed to uncomplexed ABG, the residual β-galactosidase activity value in the exposure solution was the same as the start value (e.g., before the immersion of the tissue sample).
In four out of six ACE specimens, we could detect a difference in the X-gal staining intensities in the same tissue sample when exposed to the {bCPP+ABG} complexes. Surprisingly, it was the normal tissue that had more intensive X-gal staining (last two columns in
Table 1). In two ACE specimens we detected a remarkable selectivity of either {bTAT+ABG} or {bTP+ABG} for the normal myometrium. In experiment “ACE_4” we detected a obvious selectivity of the {bTAT+ABG} complex for the normal myometrium and exclusion from the carcinoma area (
Figure 5). In experiment “ACE_1” we detected an noticeable selectivity of the {bTP+ABG} complex for the normal myometrium and exclusion from the carcinoma area (
Figure 2, panel c). The histological examination of the haematoxylin-eosin stained cryosections of these tissue samples could not point out any differences between the {bTP+ABG}-preferring myometrium and the {bTAT+ABG}-preferring myometrium, as both were histologically normal. The only difference between them was the stage of the adjacent carcinoma: the {bTP+ABG}-preferring myometrium was adjacent to stage IA carcinoma whereas the {bTAT+ABG}-preferring myometrium was adjacent to stage IB carcinoma. One common phenomenon of carcinomas is field cancerisation, which is the occurrence of molecular alterations in the histologically normal tissues surrounding the areas of an overt malignancy [
13]. The highest number of markers of field cancerisation is specified for head and neck squamous cell carcinoma, followed by oesophageal cancer [
14]. Unfortunately, the field cancerisation of adjacent and distant tissues has not been studied in the case of ACE. In other words, we did not have a set of established markers to evaluate the condition of the myometria of the tissue samples used in this study.
In accordance with the results obtained in the ACE specimens, both CPPs enhanced ABG-uptake in the SCCC specimens. In experiment “SCCC_1” we detected a preferential localisation of {bTP+ABG} complexes in the normal cervical stroma (
Figure 3 panel b).
Our second aim was the comparison of the CPP-induced distribution of ABG in different normal tissues (epithelial versus connective versus muscular). Based on X-gal staining, the distribution was enhanced in all normal tissues tested. The quantification of the enhancing effect of CPPs in normal tissue was beyond the scope of this study.
In most specimens used in our study, both tested CPPs showed a preference for histologically normal tissue. We do not currently have an explanation for such selectivity. However, in the light of some recent studies, the lower uptake of CPP-protein complexes in malignant cells is not fully surprising. The
in vitro uptake of CPP-protein complexes consisting of avidin complexed with bTAT and bTP occurs dominantly via caveolin-mediated endocytosis [
15]. The
in vitro uptake of an albumin-based magnetic resonance contrast medium is also suggested to occur
via caveolin-mediated endocytosis [
16]. When the albumin-based contrast medium was administered intravenously to mice bearing subcutaneous tumours, the histological analysis of the tumours revealed that the contrast medium was internalised by perivascular myofibroblasts and excluded from tumour nodules [
17]. Myofibroblasts (also known as cancer-associated fibroblasts) are not malignant cells but are one the most abundant cell types in the tumour stroma [
18]. One could conclude that the caveolin-based uptake of the albumin-based contrast medium was more efficient in non-malignant cells than in malignant cells. Whether or not this is the case for the CPP-protein complexes used in our study (e.g., the detailed analysis of their internalisation mechanisms in the presence of both malignant and non-malignant cells) remains to be studied.
We believe that our findings encourage the evaluation of CPPs as local delivery agents in non-malignant situations, for example in the intrauterine gene therapy of benign gynaecological diseases such as leiomyoma. Uterine leiomyomas (also known as uterine fibroids) are the most common benign tumours of the female genital tract [
19] and a leading cause of hysterectomy in premenopausal women [
20]. The development of a nonsurgical and localised treatment would greatly benefit many women [
21]. Uterine leiomyomas are attractive targets for gene therapy because the disease is localised and well circumscribed in the uterus, making ultrasound-guided intratumoural injection simple [
22]. Indeed, the adenovirus-mediated delivery of dominant-negative oestrogen receptor genes [
21] and herpes simplex virus 1 thymidine kinase genes followed by Ganciclovir treatment [
23] shrank the leiomyomas in Eker rats when administered intratumourally. As several CPPs have been shown to enhance adenovirus-mediated transduction [
24], the application of the same approach in the context of intrauterine gene therapy is promising.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}