Serum Uromodulin Levels in Prediction of Acute Kidney Injury in the Early Phase of Acute Pancreatitis

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
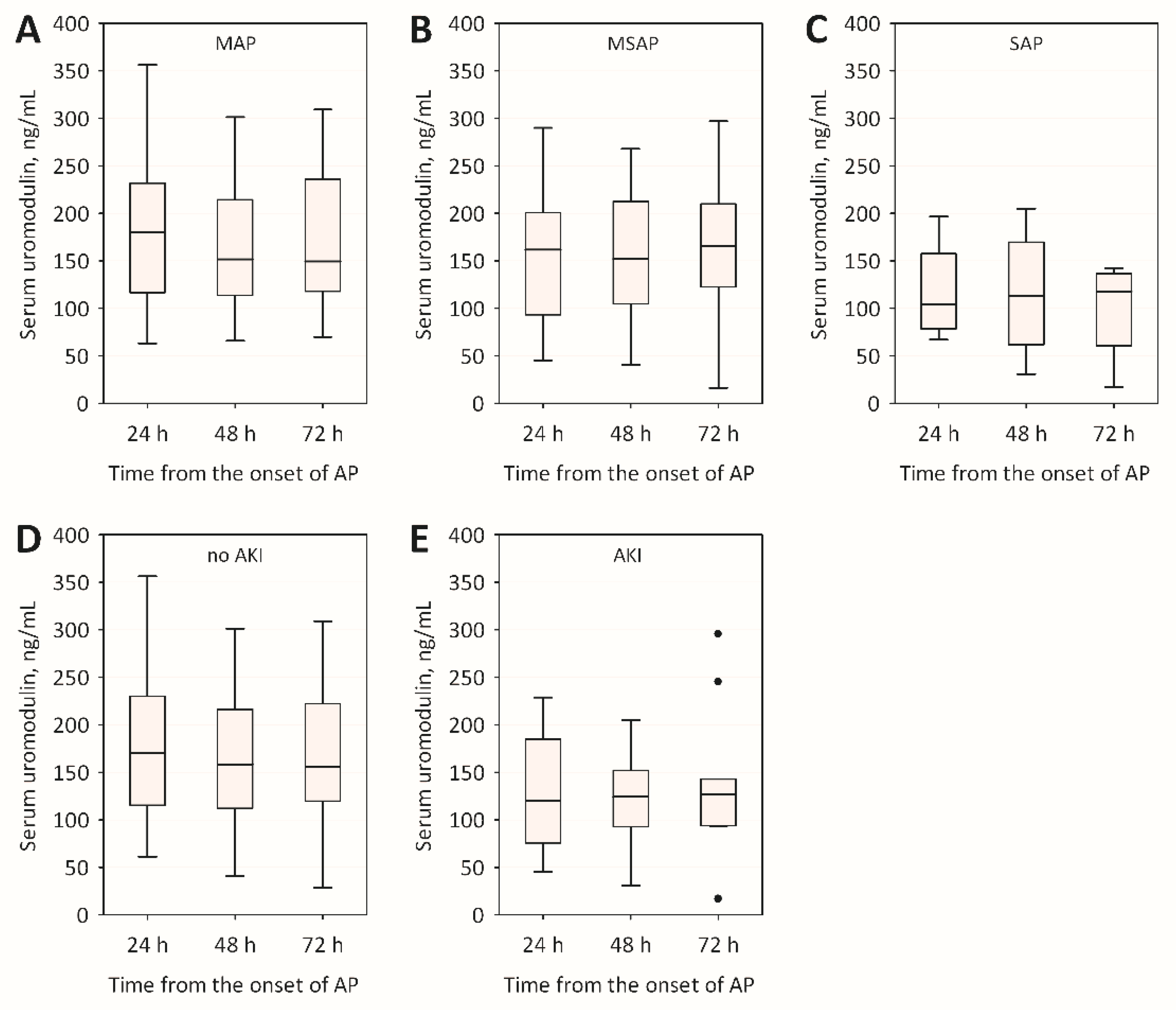
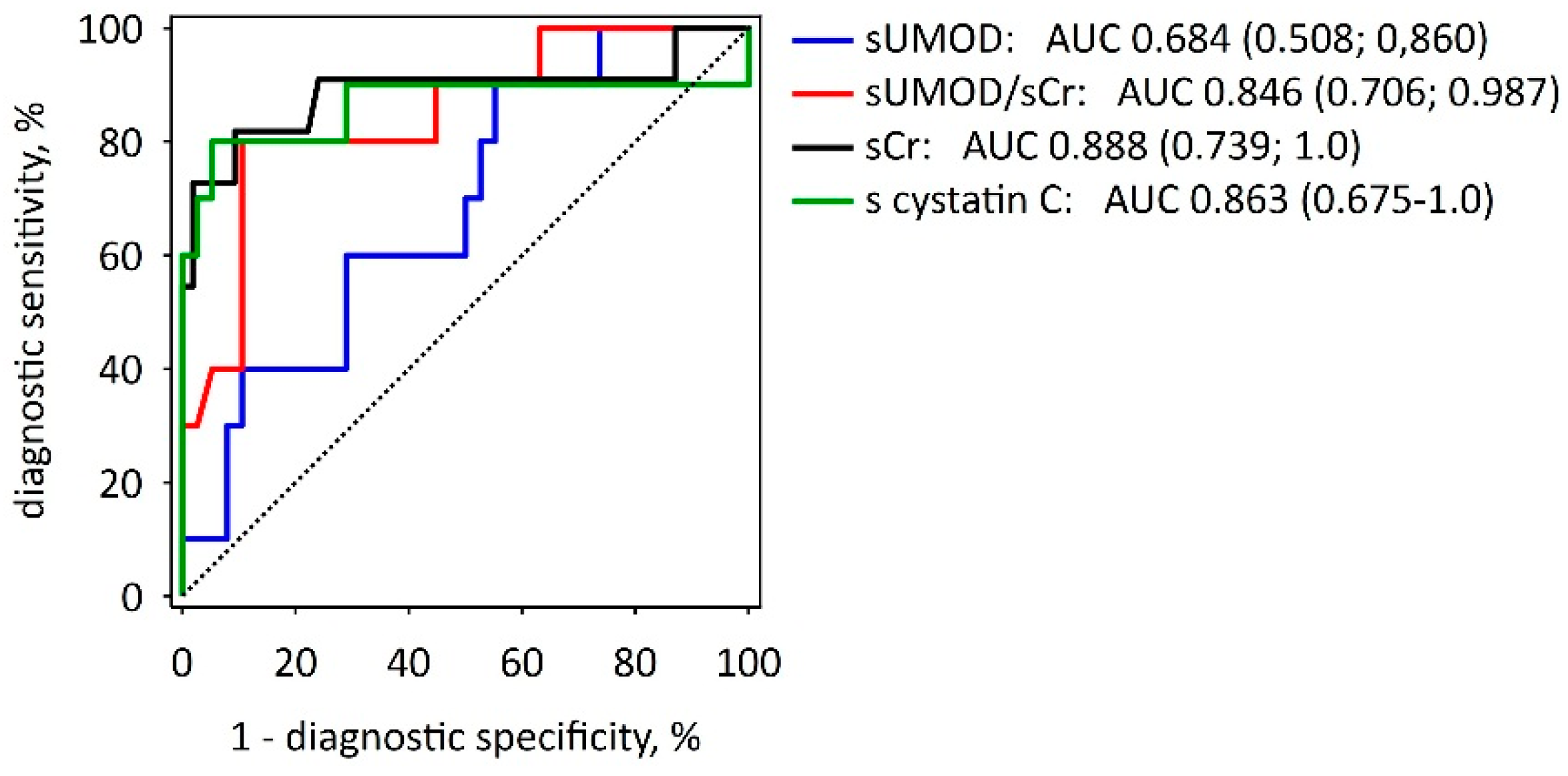
2. Results
3. Discussion
4. Materials and Methods
4.1. Patients and Study Protocol
4.2. Laboratory Measurements
4.3. Statistical Analysis
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Dumnicka, P.; Maduzia, D.; Ceranowicz, P.; Olszanecki, R.; Drożdż, R.; Kuśnierz-Cabala, B. The interplay between inflammation, coagulation and endothelial injury in the early phase of acute pancreatitis: Clinical implications. Int. J. Mol. Sci. 2017, 18, 354. [Google Scholar] [CrossRef] [PubMed]
- Almeida, N.; Fernandes, A.; Casela, A. Predictors of Severity and In-Hospital Mortality for Acute Pancreatitis: Is There Any Role for C-Reactive Protein Determination in the First 24 Hours? GE. J. Port. Gastrenterol. 2015, 22, 2015–2017. [Google Scholar] [CrossRef]
- Do, J.H. Mechanism of Severe Acute Pancreatitis: Focusing on Development and Progression. Korean J. Pancreas Biliary Tract 2015, 20, 115–123. [Google Scholar] [CrossRef]
- Wu, B.U.; Johannes, R.S.; Sun, X.; Tabak, Y.; Conwell, D.L.; Banks, P. The early prediction of mortality in acute pancreatitis: A large population-based study. Gut 2008, 57, 1698–1703. [Google Scholar] [CrossRef] [PubMed]
- Gurda-Duda, A.; Kuśnierz-Cabala, B.; Nowak, W.; Naskalski, J.W.; Kulig, J. Assessment of the prognostic value of certain acute-phase proteins and procalcitonin in the prognosis of acute pancreatitis. Pancreas 2008, 37, 449–453. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.K.; Wu, B.U.; Bollen, T.L.; Repas, K.; Maurer, R.; Johannes, R.S.; Mortele, K.J.; Conwell, D.L.; Banks, P.A. A prospective evaluation of the bedside index for severity in acute pancreatitis score in assessing mortality and intermediate markers of severity in acute pancreatitis. Am. J. Gastroenterol. 2009, 104, 966–971. [Google Scholar] [CrossRef] [PubMed]
- Banks, P.A.; Bollen, T.L.; Dervenis, C.; Gooszen, H.G.; Johnson, C.D.; Sarr, M.G.; Tsiotos, G.G.; Vege, S.S. Classification of acute pancreatitis-2012: Revision of the Atlanta classification and definitions by international consensus. Gut 2013, 62, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Petejova, N.; Martinek, A. Acute kidney injury following acute pancreatitis: A review. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc. Czech. Repub. 2013, 157, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Tenner, S.; Baillie, J.; De Witt, J.; Vege, S.S. American College of Gastroenterology guideline: Management of acute pancreatitis. Am. J. Gastroenterol. 2013, 108, 1400–1415. [Google Scholar] [CrossRef] [PubMed]
- Working Group IAP/APA Acute Pancreatitis Guidelines. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology 2013, 13, e1–e15. [Google Scholar]
- Sporek, M.; Dumnicka, P.; Gala-Błądzińska, A.; Mazur-Laskowska, M.; Walocha, J.; Ceranowicz, P.; Warzecha, Z.; Dembiński, A.; Kuźniewski, M.; Olszanecki, R.; et al. Determination of serum neutrophil gelatinase-associated lipocalin at the early stage of acute pancreatitis. Folia Med. Cracov. 2016, 56, 5–16. [Google Scholar] [PubMed]
- Sporek, M.; Dumnicka, P.; Gala-Błądzińska, A.; Ceranowicz, P.; Warzecha, Z.; Dembiński, A.; Stępień, E.; Walocha, J.; Drożdż, R.; Kuźniewski, M.; et al. Angiopoietin-2 is an early indicator of acute pancreatic-renal syndrome in patients with acute pancreatitis. Mediat. Inflamm. 2016, 5780903, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Dumnicka, P.; Sporek, M.; Mazur-Laskowska, M.; Ceranowicz, P.; Kuźniewski, M.; Drożdż, R.; Ambroży, T.; Olszanecki, R.; Kuśnierz-Cabala, B. Serum soluble fms-Like tyrosine kinase 1 (sFlt-1) predicts the severity of acute pancreatitis. Int. J. Mol. Sci. 2016, 17, 2038. [Google Scholar] [CrossRef] [PubMed]
- Sporek, M.; Gala-Błądzińska, A.; Dumnicka, P.; Mazur-Laskowska, M.; Kielczewski, S.; Walocha, J.; Ceranowicz, P.; Kuźniewski, M.; Mituś, J.; Kuśnierz-Cabala, B.; et al. Urine NGAL is useful in the clinical evaluation of renal function in the early course of acute pancreatitis. Folia Med. Cracov. 2016, 56, 13–25. [Google Scholar] [PubMed]
- Chen, W.C.; Lin, H.S.; Tsai, F.J.; Li, C.W. Effects of Tamm-Horsfall protein and albumin on the inhibition of free radicals. Urol. Int. 2001, 67, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Serafini-Cessi, F.; Malagolini, N.; Cavallone, D. Tamm-Horsfall glycoprotein: Biology and clinical relevance. Am. J. Kidney Dis. 2003, 42, 658–676. [Google Scholar] [CrossRef]
- Steubl, D.; Block, M.; Herbst, V.; Nockher, W.A.; Schlumberger, W.; Satanovskij, R.; Angermann, S.; Hasenau, A.-L.; Stecher, L.; Heemann, U.; et al. Plasma Uromodulin Correlates with Kidney Function and Identifies Early Stages in Chronic Kidney Disease Patients. Medicine (Baltimore) 2016, 95, e3011. [Google Scholar] [CrossRef] [PubMed]
- Thornley, C.; Dawnay, A.; Cattell, W.R. Human Tamm-Horsfall glycoprotein: Urinary and plasma levels in normal subjects and patients with renal disease determined by a fully validated radioimmunoassay. Clin. Sci. (Lond.) 1985, 68, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Risch, L.; Lhotta, K.; Meier, D.; Medina-Escobar, P.; Nydegger, U.E.; Risch, M. The serum uromodulin level is associated with kidney function. Clin. Chem. Lab. Med. 2014, 52, 1755–1761. [Google Scholar] [CrossRef] [PubMed]
- Fedak, D.; Kuźniewski, M.; Fugiel, A.; Wieczorek-Surdacka, E.; Przepiórkowska-Hoyer, B.; Jasik, P.; Miarka, P.; Dumnicka, P.; Kapusta, M.; Solnica, B.; et al. Serum uromodulin concentrations correlate with glomerular filtration rate in patients with chronic kidney disease. Pol. Arch. Med. Wewnętrznej 2016, 126, 995–1004. [Google Scholar] [CrossRef] [PubMed]
- Bleyer, A.J.; Kmoch, S. Tamm Horsfall glycoprotein and uromodulin: It is all about the tubules! Clin. J. Am. Soc. Nephrol. 2016, 11, 6–8. [Google Scholar] [CrossRef] [PubMed]
- Garimella, P.S.; Jaber, B.L.; Tighiouart, H.; Liangos, O.; Bennett, M.R.; Devarajan, P.; El-Achkar, T.M.; Sarnak, M.J. Association of Preoperative Urinary Uromodulin with AKI after Cardiac Surgery. Clin. J. Am. Soc. Nephrol. 2017, 12, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Askenazi, D.J.; Koralkar, R.; Hundley, H.E.; Montesanti, A.; Parwar, P.; Sonjara, S.; Ambalavanan, N. Urine Biomarkers Predict Acute Kidney Injury in Newborns. J. Pediatr. 2012, 161, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Botelho, T.E.F.; Pereira, A.K.; Teixeira, P.G.; Lage, E.M.; Osanan, G.C.; Silva, A.C.S.e. Uromodulin: A new biomarker of fetal renal function? J. Bras. Nefrol. 2016, 38, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Dawnay, A.B.; Cattell, W.R. Serum Tamm-Horsfall glycoprotein levels in health and in renal disease. Clin. Nephrol. 1981, 15, 5–8. [Google Scholar] [PubMed]
- Pruijm, M.; Ponte, B.; Ackermann, D.; Paccaud, F.; Guessous, I.; Ehret, G.; Pechére-Bertschi, A.; Vogt, B.; Mohaupt, M.G.; Martin, P.Y.; et al. Associations of urinary uromodulin with clinical characteristics and markers of tubular function in the general population. Clin. J. Am. Soc. Nephrol. 2016, 11, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Heitmeier, M.; McCracken, R.; Micanovic, R.; Khan, S.; El-Achkar, T.M. The role of tumor necrosis factor alpha in regulating the expression of tamm-horsfall protein (uromodulin) in thick ascending limbs during kidney injury. Am. J. Nephrol. 2014, 40, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Safirstein, R. Gene expression in nephrotoxic and ischemic acute renal failure. J. Am. Soc. Nephrol. 1994, 4, 1387–1395. [Google Scholar] [PubMed]
- El-Achkar, T.M.; McCracken, R.; Liu, Y.; Heitmeier, M.R.; Bourgeois, S.; Ryerse, J.; Wu, X.-R. Tamm-Horsfall protein translocates to the basolateral domain of thick ascending limbs, interstitium, and circulation during recovery from acute kidney injury. Am. J. Physiol. Renal Physiol. 2013, 304, F1066–F1075. [Google Scholar] [CrossRef] [PubMed]
- Schaeffer, C.; Santambrogio, S.; Perucca, S.; Casari, G.; Rampoldi, L. Analysis of Uromodulin Polymerization Provides New Insights into the Mechanisms Regulating ZP Domain-mediated Protein Assembly. Mol. Biol. Cell 2008, 20, 589–599. [Google Scholar] [CrossRef] [PubMed]
- Jennings, P.; Aydin, S.; Kotanko, P.; Lechner, J.; Lhotta, K.; Williams, S.; Thakker, R.V.; Pfaller, W. Membrane Targeting and Secretion of Mutant Uromodulin in Familial Juvenile Hyperuricemic Nephropathy. J. Am. Soc. Nephrol. 2007, 18, 264–273. [Google Scholar] [CrossRef] [PubMed]
- Mao, S.; Zhang, A.; Huang, S. The signaling pathway of uromodulin and its role in kidney diseases. J. Recept. Signal Transduct. Res. 2014, 34, 440–444. [Google Scholar] [CrossRef] [PubMed]
- El-Achkar, T.M.; Wu, X. Uromodulin in kidney injury: An instigator, bystander, or protector? Am. J. Kidney Dis. 2012, 59, 452–461. [Google Scholar] [CrossRef] [PubMed]
- Prajczer, S.; Heidenreich, U.; Pfaller, W.; Kotanko, P.; Lhotta, K.; Jennings, P. Evidence for a role of uromodulin in chronic kidney disease progression. Nephrol. Dial. Transplant. 2010, 25, 1896–1903. [Google Scholar] [CrossRef] [PubMed]
- Kreft, B.; Jabs, W.J.; Laskay, T.; Klinger, M.; Solbach, W.; van Zandbergen, G.; Kumar, S. Polarized Expression of Tamm-Horsfall Protein by Renal Tubular Epithelial Cells Activates Human Granulocytes Polarized Expression of Tamm-Horsfall Protein by Renal Tubular Epithelial Cells Activates Human Granulocytes. Infect. Immun. 2002, 70, 2650–2656. [Google Scholar] [CrossRef] [PubMed]
- El-Achkar, T.M.; McCracken, R.; Rauchman, M.; Heitmeier, M.R.; Al-Aly, Z.; Dagher, P.C.; Wu, X.-R. Tamm-Horsfall protein-deficient thick ascending limbs promote injury to neighboring S3 segments in an MIP-2-dependent mechanism. Am. J. Physiol. Renal Physiol. 2011, 300, F999–F1007. [Google Scholar] [CrossRef] [PubMed]
- Horton, J.K.; Davies, M.; Topley, N.; Thomas, D.; Williams, J.D. Activation of the inflammatory response of neutrophils by Tamm-Horsfall glycoprotein. Kidney Int. 1990, 37, 717–726. [Google Scholar] [CrossRef] [PubMed]
- Wimmer, T.; Cohen, G.; Saemann, M.D.; Hörl, W.H. Effects of Tamm-Horsfall protein on polymorphonuclear leukocyte function. Nephrol. Dial. Transplant. 2004, 19, 2192–2197. [Google Scholar] [CrossRef] [PubMed]
- Schmid, M.; Prajczer, S.; Gruber, L.N.; Bertocchi, C.; Gandini, R.; Pfaller, W.; Jennings, P.; Joannidis, M. Uromodulin facilitates neutrophil migration across renal epithelial monolayers. Cell. Physiol. Biochem. 2010, 26, 311–318. [Google Scholar] [CrossRef] [PubMed]
Sample Availability: Samples of the compounds are not available from the authors. |

{kind=link}
{kind=link}
| Variable | MAP (n = 46) | MSAP (n = 15) | SAP (n = 5) | p * |
|---|---|---|---|---|
| Age, years | 59 ± 19 | 64 ± 16 | 70 ± 19 | NS |
| Male gender, n (%) | 25 (54) | 6 (40) | 3 (60) | NS |
| Duration of hospital stay, days | 6 (5–7) | 12 (10–17) | 27 (13–31) | <0.001 a,b |
| BISAP score ≥3 in first 24 h, n (%) | 0 | 2 (13) | 4 (80) | <0.001 d |
| Comorbidities, n (%) | 33 (72) | 12 (80) | 5 (100) | NS |
| Mortality, n (%) | 0 | 0 | 3 (60) | - |
| Amylase, U/L | 1085 (571–1722) | 1038 (772–1917) | 1013 (357–1909) | NS |
| Urea, mmol/L | 5.5 (4.1–6.8) | 6.7 (5.6–8.4) | 13.4 (11.7–15.1) | 0.002 a |
| Creatinine, µmol/L | 72.7 (63.4–94.8) | 90.7 (67.6–113.4) | 194.4 (120.0–228.0) | 0.008 a |
| Cystatin C, mg/L | 0.87 (0.65–1.07) | 0.84 (0.76–1.58) | 1.98 (1.65–2.42) | 0.009 a |
| eGFR, mL/min/1.73 m2 | 84.1 (61.2–120.7) | 71.5 (41.7–116.6) | 29.0 (24.7–33.7) | 0.005 a |
| Uromodulin, ng/mL | 180 (116–232) | 162 (93–201) | 104 (79–158) | NS |
| CRP, mg/L | 5.9 (1.9–48.6) | 24.4 (9.0–103.2) | 191.1 (74.6–258.2) | 0.003 a |
| Albumin, g/dL | 40.6 ± 4.0 | 39.7 ± 3.9 | 30.7 ± 8.4 | 0.030 a |
| WBC, ×103/µL | 11.1 (9.2–14.6) | 12.4 (10.6–15.3) | 10.4 (9.8–18.4) | NS |
| MONO, ×10/µL | 0.51 (0.40–0.73) | 0.51 (0.26–0.76) | 0.43 (0.25–0.46) | NS |
| NEU, ×103/µL | 9.18 (7.35–12.71) | 9.38 (6.59–14.06) | 9.90 (8.78–15.43) | NS |
| LYM, ×103/µL | 1.31 (0.95–1.80) | 1.63 (1.17–2.87) | 0.57 (0.36–1.01) | 0.006 a,c |
| Hematocrit, % | 42.5 ± 4.1 | 43.2 ± 6.7 | 39.0 ± 7.1 | NS |
| PLT, ×103/µL | 237 (196–255) | 230 (210–267) | 128 (121–150) | NS |
| Variable | 24 h | 48 h | 72 h | |||
|---|---|---|---|---|---|---|
| R | p | R | p | R | p | |
| Age | −0.43 | 0.002 | −0.28 | 0.049 | −0.22 | NS |
| BISAP * | −0.36 | 0.011 | - | - | - | - |
| CRP | −0.29 | 0.043 | −0.11 | NS | −0.13 | NS |
| NEU | −0.29 | 0.044 | −0.10 | NS | −0.07 | NS |
| Creatinine | −0.47 | <0.001 | −0.46 | 0.001 | −0.34 | 0.015 |
| eGFR | 0.47 | <0.001 | 0.49 | <0.001 | 0.38 | 0.009 |
| Cystatin C | −0.48 | <0.001 | −0.51 | <0.001 | −0.45 | 0.002 |
| Urea | −0.51 | <0.001 | −0.44 | 0.001 | −0.37 | 0.010 |
| Independent Variables | 24 h | 48 h | 72 h | |||
|---|---|---|---|---|---|---|
| Beta ± SE | p | Beta ± SE | p | Beta ± SE | p | |
| Age | −0.60 ± 0.11 | <0.001 | −0.57 ± 0.12 | <0.001 | −0.63 ± 0.12 | <0.001 |
| Male sex | −0.03 ± 0.10 | NS | 0.01 ± 0.11 | NS | 0.02 ± 0.12 | NS |
| Uromodulin | 0.24 ± 0.11 | 0.037 | 0.35 ± 0.12 | 0.006 | 0.29 ± 0.12 | 0.020 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuśnierz-Cabala, B.; Gala-Błądzińska, A.; Mazur-Laskowska, M.; Dumnicka, P.; Sporek, M.; Matuszyk, A.; Gil, K.; Ceranowicz, P.; Walocha, J.; Kucharz, J.; et al. Serum Uromodulin Levels in Prediction of Acute Kidney Injury in the Early Phase of Acute Pancreatitis. Molecules 2017, 22, 988. https://doi.org/10.3390/molecules22060988
Kuśnierz-Cabala B, Gala-Błądzińska A, Mazur-Laskowska M, Dumnicka P, Sporek M, Matuszyk A, Gil K, Ceranowicz P, Walocha J, Kucharz J, et al. Serum Uromodulin Levels in Prediction of Acute Kidney Injury in the Early Phase of Acute Pancreatitis. Molecules. 2017; 22(6):988. https://doi.org/10.3390/molecules22060988
Chicago/Turabian StyleKuśnierz-Cabala, Beata, Agnieszka Gala-Błądzińska, Małgorzata Mazur-Laskowska, Paulina Dumnicka, Mateusz Sporek, Aleksandra Matuszyk, Krzysztof Gil, Piotr Ceranowicz, Jerzy Walocha, Jakub Kucharz, and et al. 2017. "Serum Uromodulin Levels in Prediction of Acute Kidney Injury in the Early Phase of Acute Pancreatitis" Molecules 22, no. 6: 988. https://doi.org/10.3390/molecules22060988