Low-Pass Filtering Approach via Empirical Mode Decomposition Improves Short-Scale Entropy-Based Complexity Estimation of QT Interval Variability in Long QT Syndrome Type 1 Patients


 ,
,  and
and 
Abstract
:
1. Introduction
2. Methods
2.1. EMD-Based Filtering Approach
2.2. SampEn
3. Study Population, Experimental Protocol and Data Analysis
3.1. Study Population
3.2. Data Acquisition
3.3. Data Analysis
3.4. Statistical Analysis
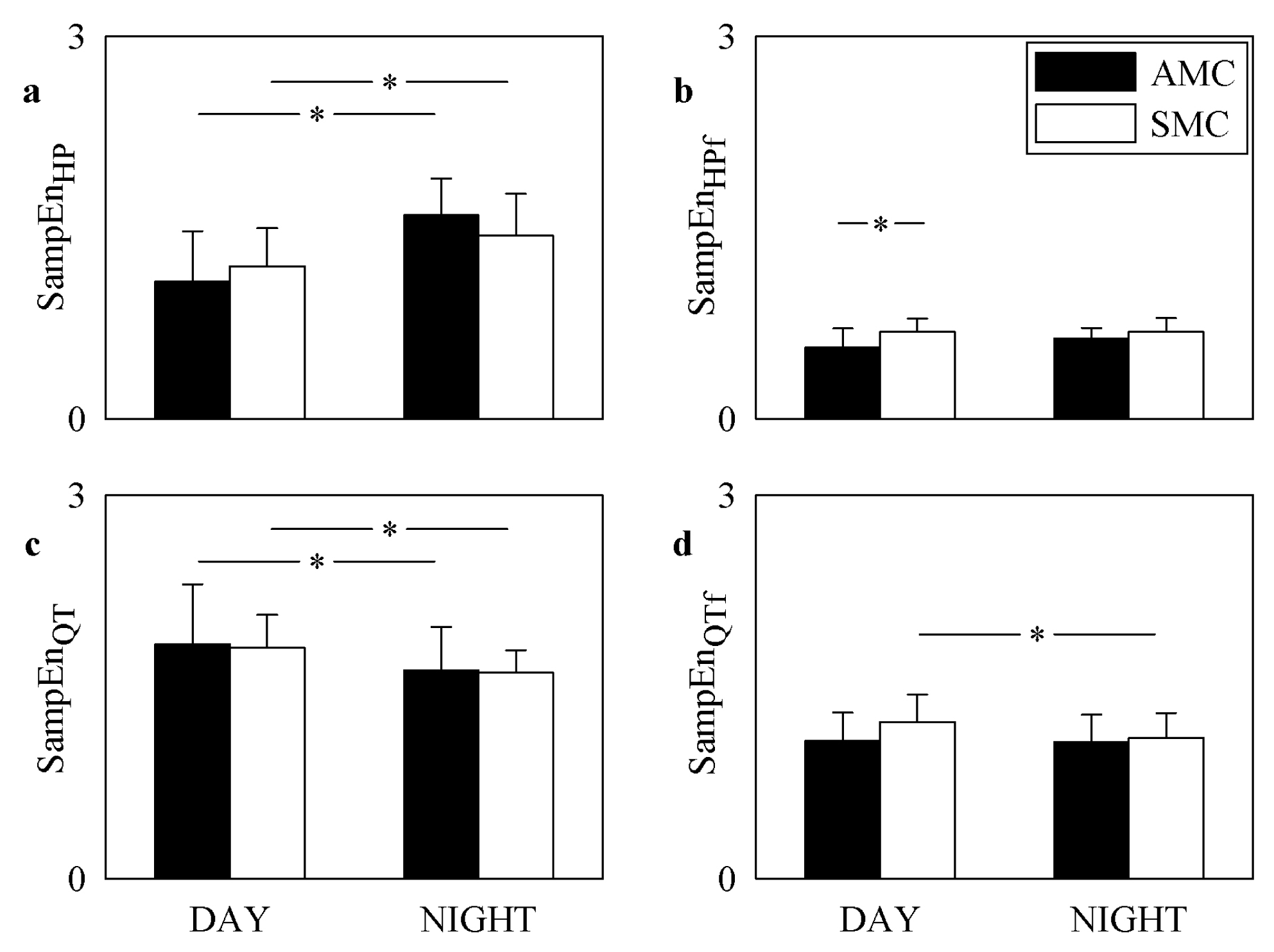
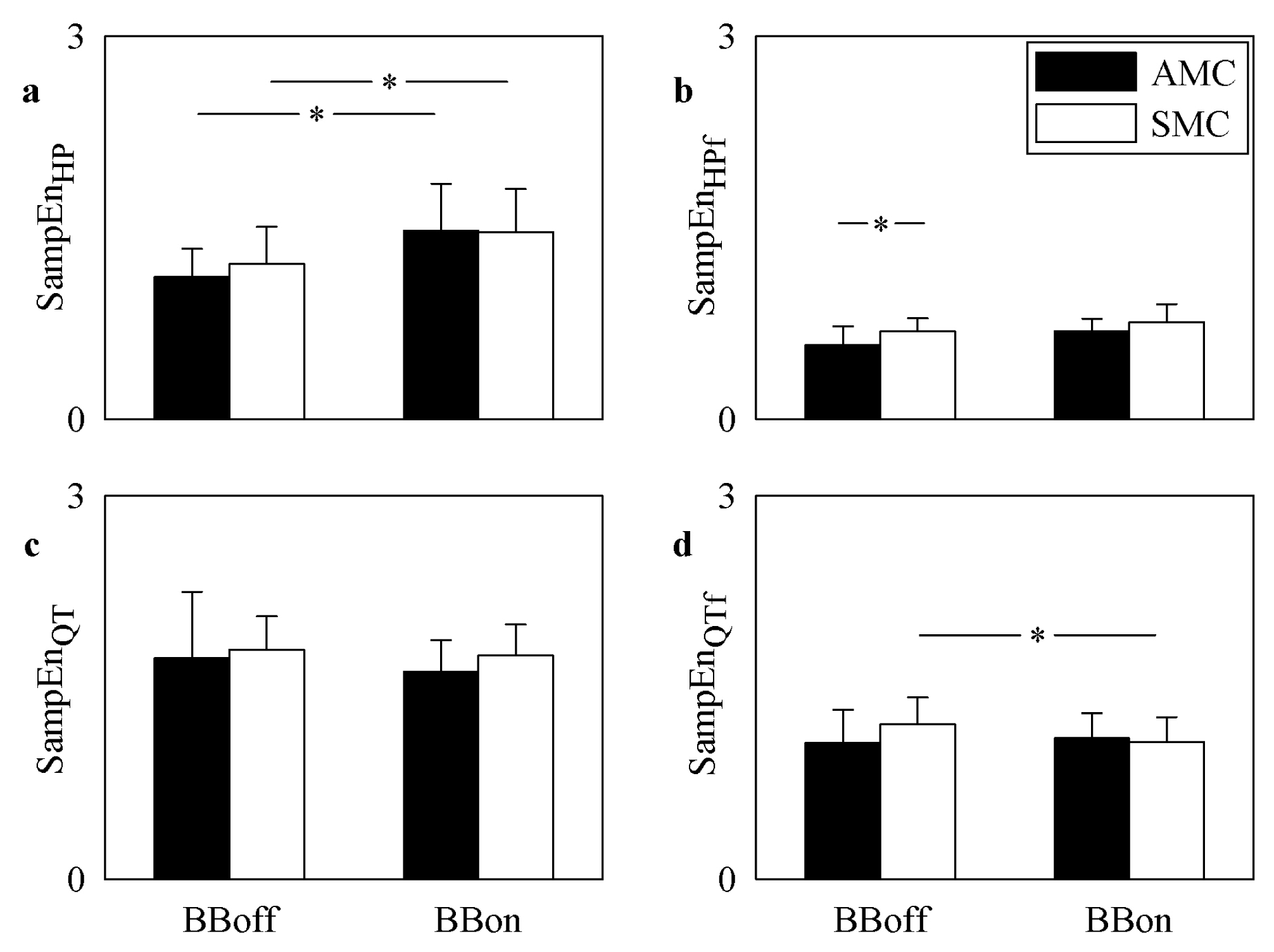
4. Results
5. Discussion
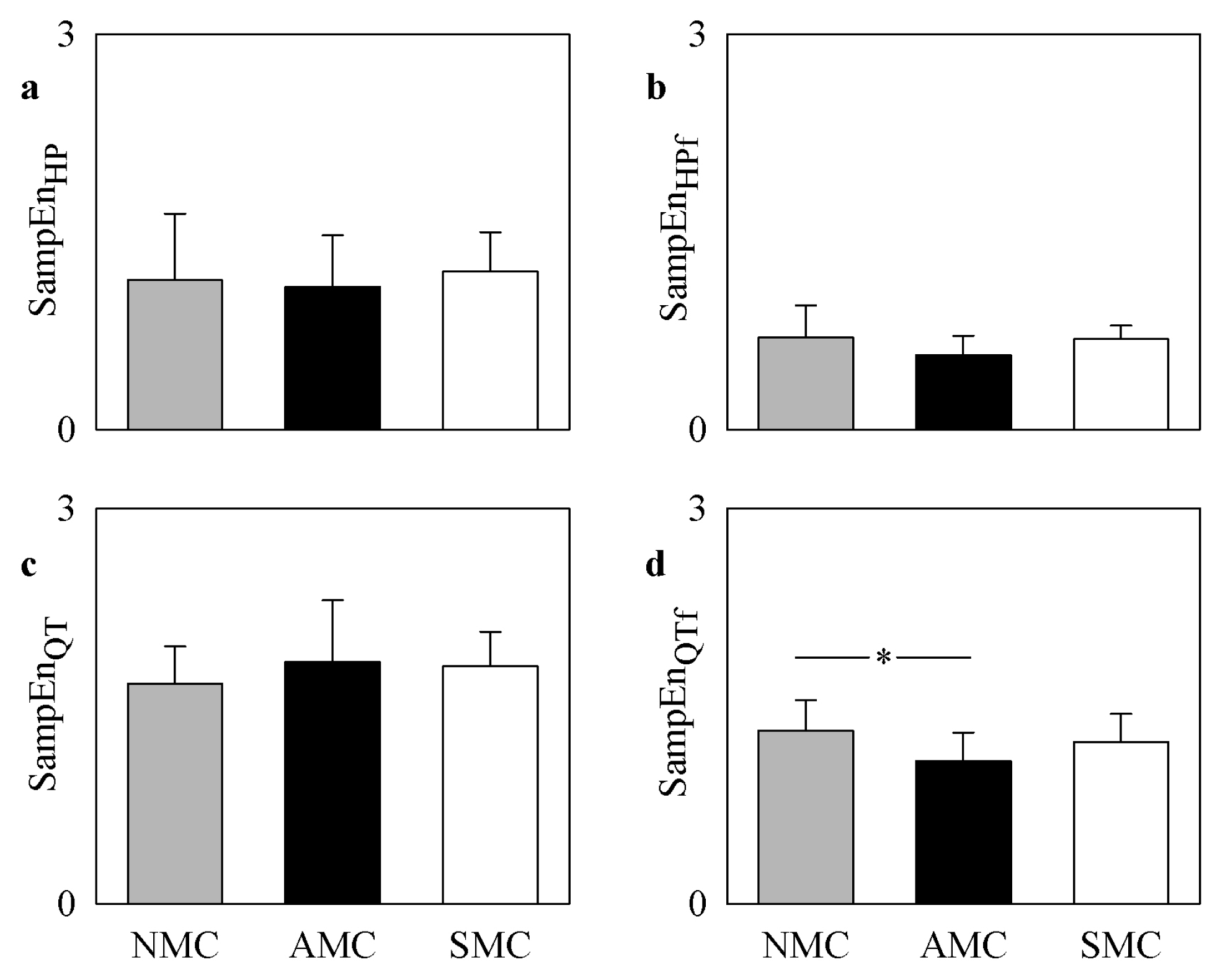
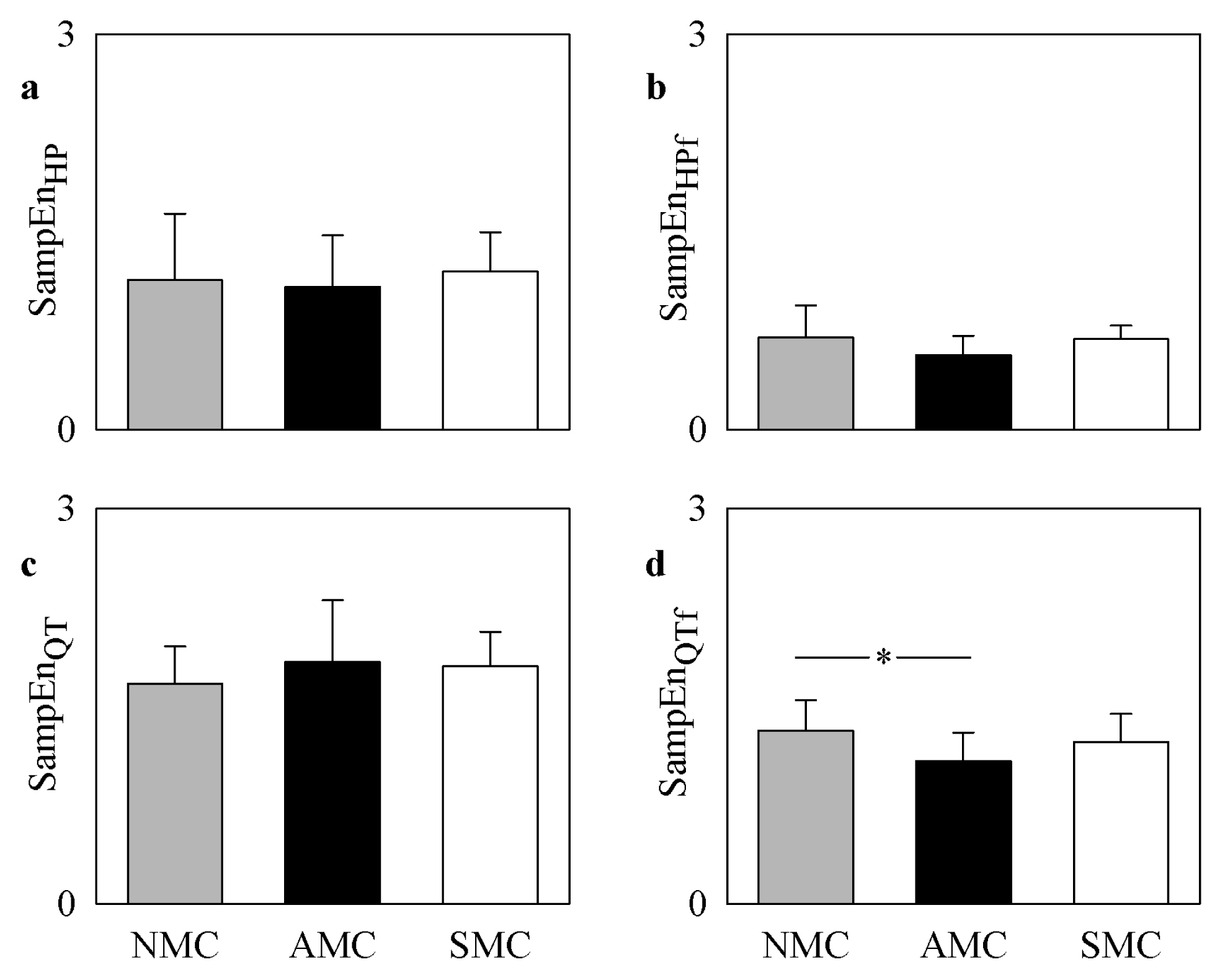
5.1. EMD-Filtered QT Variability Allowed the Separation of AMCs from NMCs
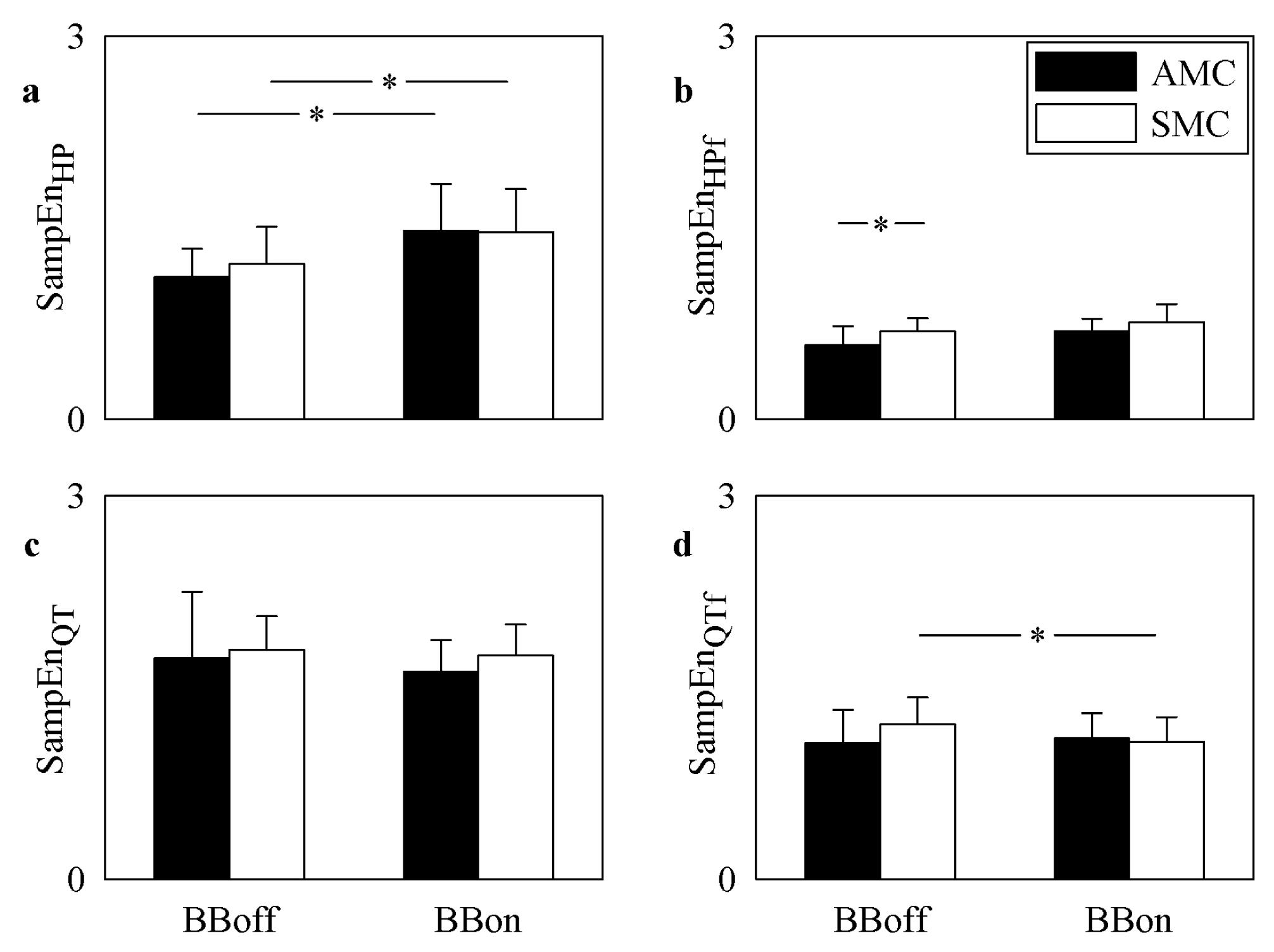
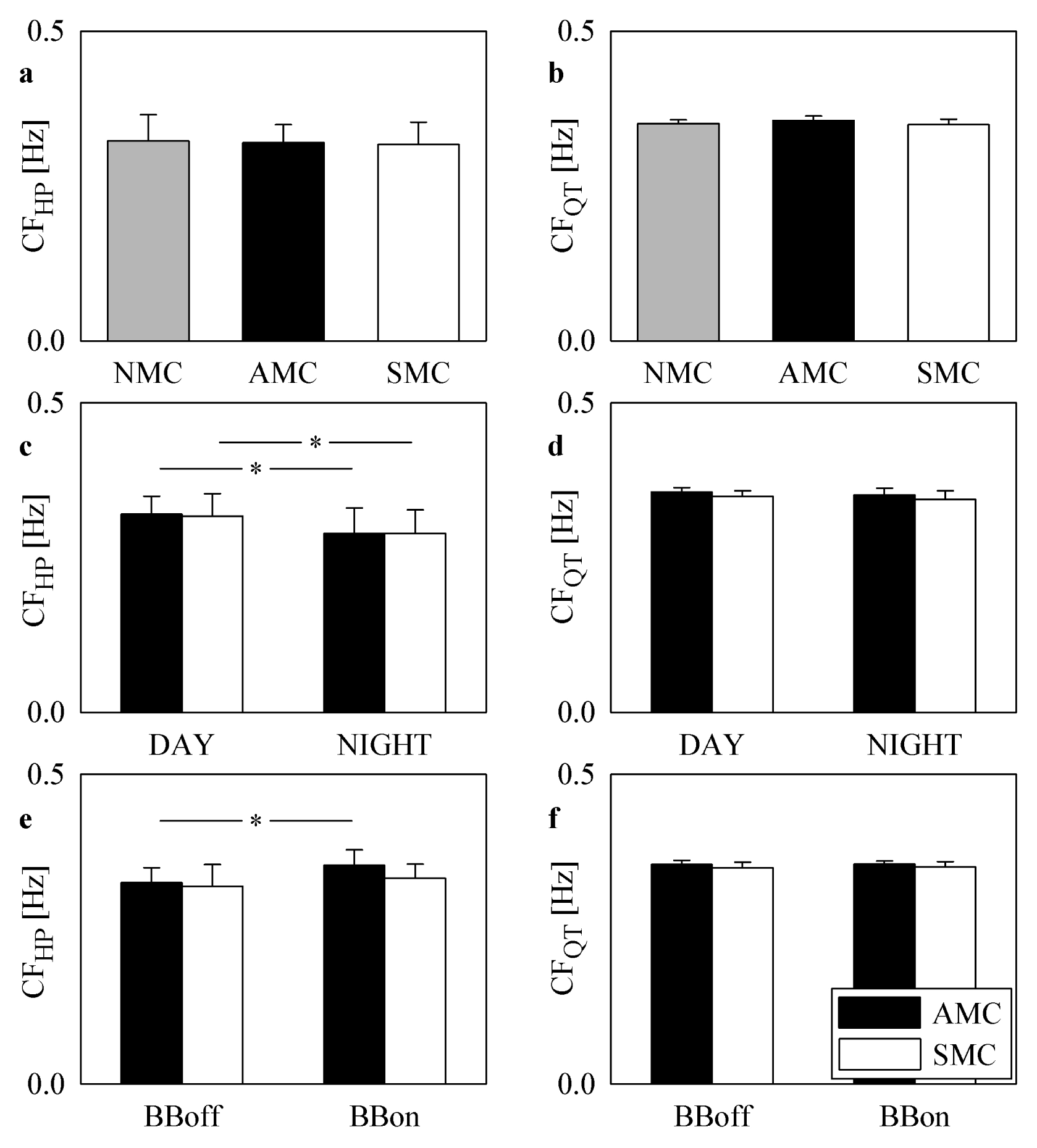
5.2. EMD-Filtered QT Variability Allowed the Detection of the Effect of BB
5.3. EMD-Based Filtering Approach Cancelled Respiratory Sinus Arrhythmia from HP Variability
5.4. EMD-Based Filtering of HP Variability Enhanced Cardiac Control Targeting the Sinus Node at Frequencies Slower Than the Respiratory One
5.5. Comparison between Complexity of EMD-Filtered HP and QT Variability
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
List of Abbreviations
| LQT1 | long QT syndrome type 1 |
| HP | heart period |
| QT | interval from Q-wave onset to T-wave end |
| QTc | corrected QT |
| MC | mutation carrier |
| NMC | non-mutation carrier |
| AMC | asymptomatic MC |
| SMC | symptomatic MC |
| DAY | daytime |
| NIGHT | nighttime |
| BB | beta-blocker therapy |
| BBoff | off BB |
| BBon | on BB |
| EMD | empirical mode decomposition |
| IMF | intrinsic mode function |
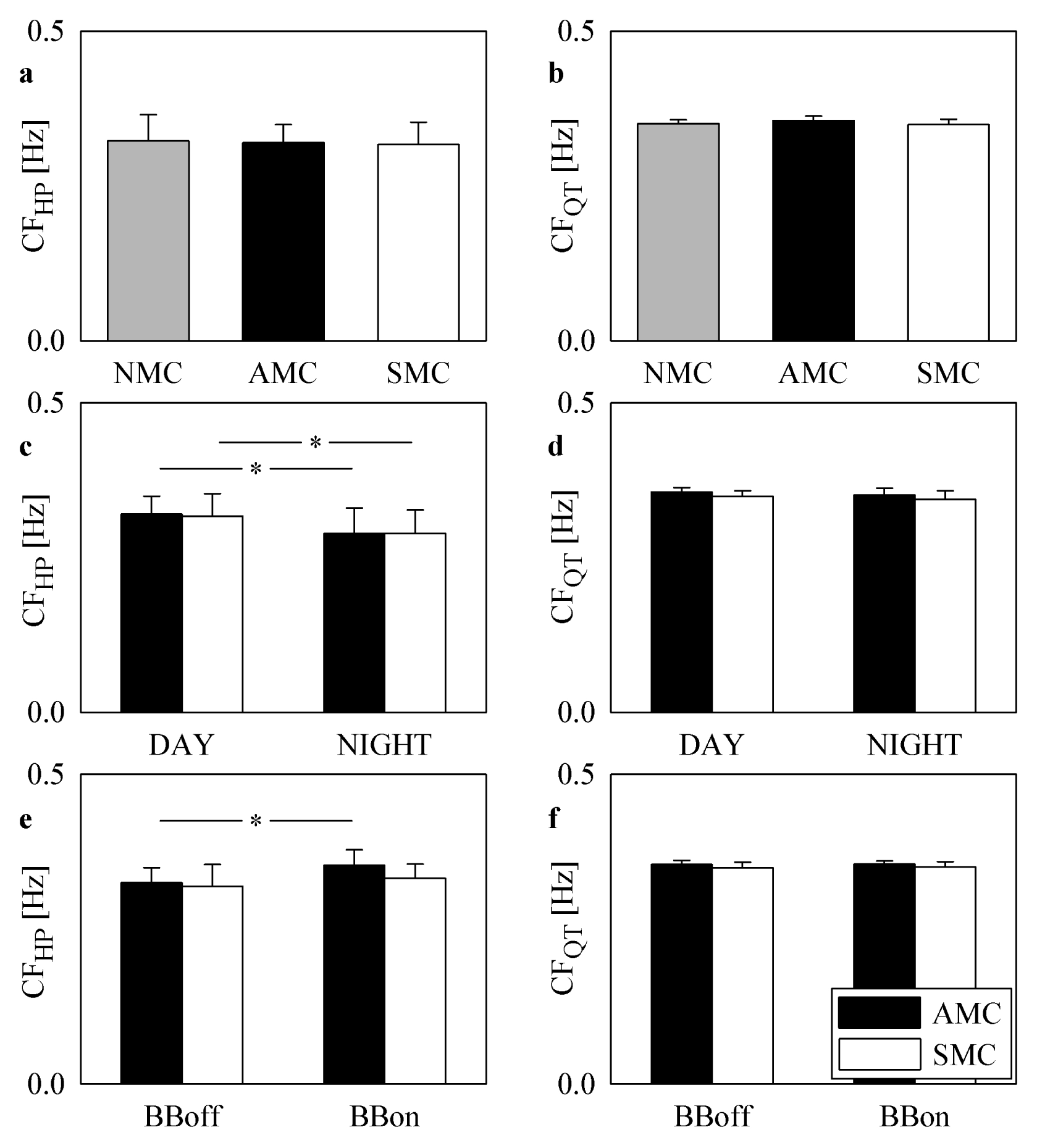
| CF | characteristic frequency |
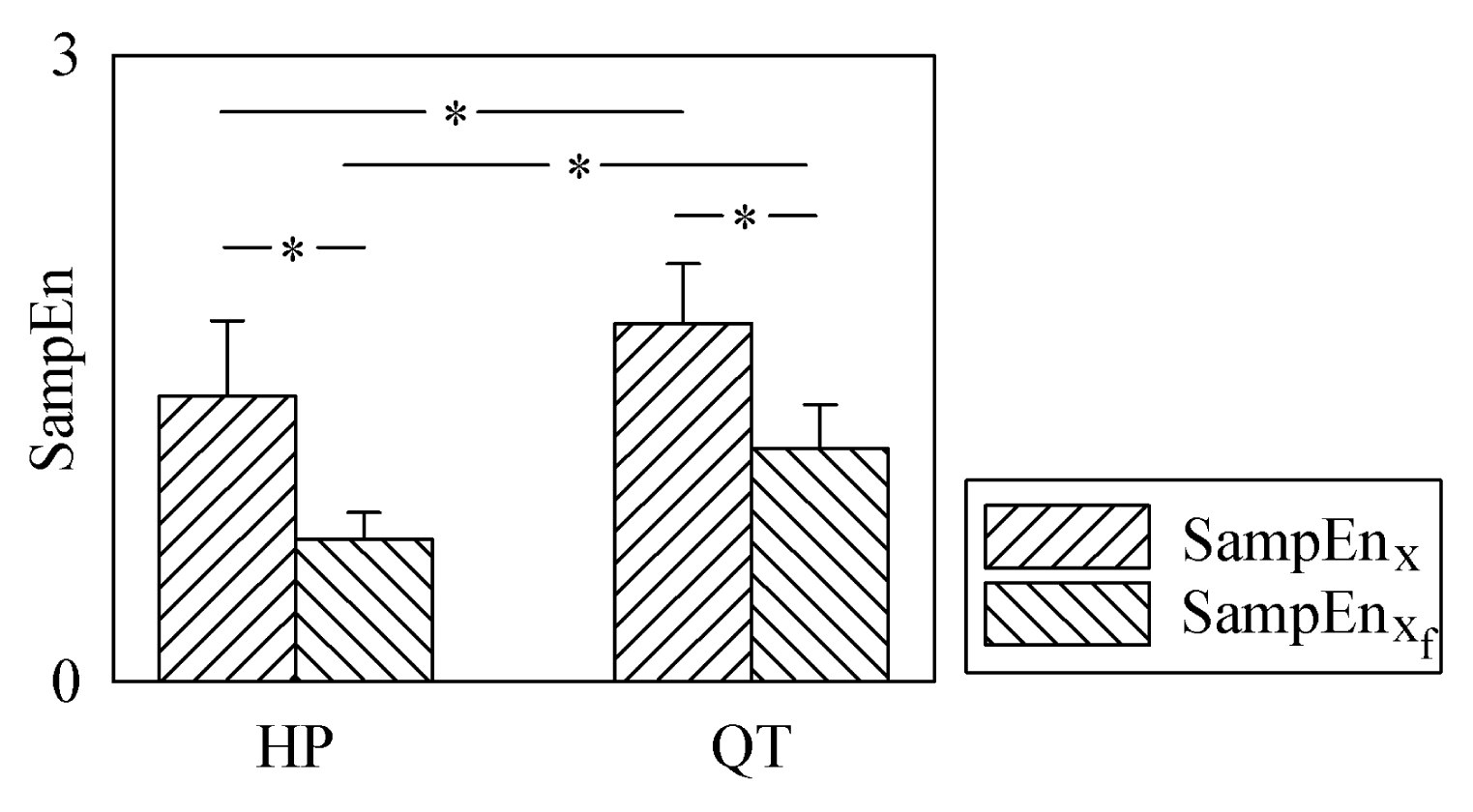
| SampEn | sample entropy |
| μHP | HP mean |
| μQT | QT mean |
| μQTc | QTc mean |
References
- Schwartz, P.J.; Crotti, L. QTc Behavior During Exercise and Genetic Testing for the Long-QT Syndrome. Circulation 2011, 20, 2181–2184. [Google Scholar]
- Schwartz, P.J.; Priori, S.G.; Spazzolini, C.; Moss, A.J.; Vincent, G.M.; Napolitano, C.; Denjoy, I.; Guicheney, P.; Breithardt, G.; Keating, M.T.; et al. Genotype-phenotype correlation in the long-QT syndrome-Gene specific triggers for life threatening arrhythmias. Circulation 2001, 103, 89–95. [Google Scholar]
- Schwartz, P.J.; Ackerman, M.J. The long QT syndrome. A transatlantic clinical approach to diagnosis and therapy. Eur. Heart J 2013, 34, 3109–3116. [Google Scholar]
- Crotti, L.; Lundquist, A.L.; Insolia, R.; Pedrazzini, M.; Ferrandi, C.; De Ferrari, G.M.; Vicentini, A.; Yang, P.; Roden, D.M.; George, A.L.; Schwartz, P.J. KCNH2-K897T is a genetic modifier of latent congenital long QT syndrome. Circulation 2005, 112, 1251–1258. [Google Scholar]
- Crotti, L.; Monti, M.C.; Insolia, R.; Peljto, A.; Goosen, A.; Brink, P.A.; Greenberg, D.A.; Schwartz, P.J.; George, A.L. NOS1AP is a genetic modifier of the long-QT syndrome. Circulation 2009, 120, 1657–1663. [Google Scholar]
- Amin, A.S.; Giudicessi, J.R.; Tijsen, A.J.; Spanjaart, A.M.; Reckman, Y.J.; Klemens, C.A.; Tanck, M.W.; Kapplinger, J.D.; Hofman, N.; Sinner, M.F.; et al. Variants in the 3′ untranslated region of the KCNQ1-encoded Kv7.1 potassium channel modify disease severity in patients with type 1 long QT syndrome in an allele-specific manner. Eur. Heart J 2012, 33, 714–723. [Google Scholar]
- Duchatelet, S.; Crotti, L.; Peat, R.; Denjoy, I.; Itoh, H.; Berthet, M.; Ohno, S.; Fressart, V.; Monti, M.C.; Crocamo, C.; et al. Identification of a KCNQ1 polymorphism acting as a protective modifier against arrhythmic risk in the long QT syndrome. Circ. Cardiovasc. Genet 2013, 6, 354–361. [Google Scholar]
- Schwartz, P.J.; Vanoli, E.; Crotti, L.; Spazzolini, C.; Ferrandi, C.; Goosen, A.; Hedley, P.; Heradien, M.; Bacchini, S.; Turco, A.; et al. Neural control of heart rate is an arrhythmia risk modifier in long QT syndrome. J. Am. Coll. Cardiol 2008, 51, 920–929. [Google Scholar]
- Crotti, L.; Spazzolini, C.; Porretta, A.P.; Dagradi, F.; Taravelli, E.; Petracci, B.; Vicentini, A.; Pedrazzini, F.; La Rovere, M.T.; Vanoli, E.; et al. Vagal reflexes following an exercise stress test. A simple clinical tool for gene-specific risk stratification in the long QT syndrome. J. Am. Coll. Cardiol 2012, 60, 2515–2524. [Google Scholar]
- Bari, V.; Valencia, J.F.; Vallverdú, M.; Girardengo, G.; Marchi, A.; Bassani, T.; Caminal, P.; Cerutti, S.; George, A.L.; Brink, P.A.; et al. Multiscale complexity analysis of the cardiac control identifies asymptomatic and symptomatic patients in long QT syndrome type 1. PLoS ONE 2014, 9. [Google Scholar] [CrossRef]
- Costa, M.; Goldberger, A.L.; Peng, C.-K. Multiscale entropy analysis of complex physiologic time series. Phys. Rev. Lett 2002, 89. [Google Scholar] [CrossRef]
- Valencia, J.F.; Porta, A.; Vallverdù, M.; Clarià, F.; Baranowski, R.; Orlowska-Baranowska, E.; Caminal, P. Refined multiscale entropy: Application to 24-h Holter recordings of heart period variability in healthy and aortic stenosis subjects. IEEE Trans. Biomed. Eng 2009, 56, 2202–2213. [Google Scholar]
- Baumert, M.; Starc, V.; Porta, A. Conventional QT variability measurement vs. template matching techniques: comparison of performance using simulated and real ECG. PLoS ONE 2012, 7. [Google Scholar] [CrossRef]
- Huang, N.E.; Zheng, S.; Long, S.R.; Wu, M.C.; Shih, H.H.; Zheng, Q.; Yen, N.-C.; Tung, C.C.; Liu, H.H. The empirical mode decomposition and the Hilbert spectrum for nonlinear and non-stationary time series analysis. Proc. R. Soc. A 1998, 454, 903–995. [Google Scholar]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol 2000, 278, 2039–2049. [Google Scholar]
- Balocchi, R.; Menicucci, D.; Santarcangelo, E.; Sebastian, L.; Gemignani, A.; Ghelarducci, B.; Varanini, M. Deriving the respiratory sinus arrhythmia from the heartbeat time series using empirical mode decomposition. Chaos Solit. Fract 2004, 20, 171–177. [Google Scholar]
- Neto, E.S.; Custaud, M.A.; Cejka, J.C.; Abry, P.; Frutoso, J.; Gharib, C.; Flandrin, P. Assessment of cardiovascular autonomic control by the empirical mode decomposition. Methods Inf. Med 2004, 43, 60–65. [Google Scholar]
- Echeverría, J.C.; Crowe, J.A.; Woolfson, M.S.; Hayes-Gill, B.R. Application of empirical mode decomposition to heart rate variability analysis. Med. Biol. Eng. Comput 2001, 39, 471–479. [Google Scholar]
- Maestri, R.; Pinna, G.D.; Accardo, A.; Allegrini, P.; Balocchi, R.; D’Addio, G.; Ferrario, M.; Menicucci, D.; Porta, A.; Sassi, R.; et al. Nonlinear indices of heart rate variability in chronic heart failure patients: redundancy and comparative clinical value. J. Cardiovasc. Electrophysiol 2007, 18, 425–433. [Google Scholar]
- Porta, A.; Castiglioni, P.; Bari, V.; Bassani, T.; Marchi, A.; Cividjian, A.; Quintin, L.; Di Rienzo, M. K-nearest-neighbor conditional entropy approach for the assessment of short-term complexity of cardiovascular control. Physiol. Meas 2013, 34, 17–33. [Google Scholar]
- Porta, A.; Gnecchi-Ruscone, T.; Tobaldini, E.; Guzzetti, S.; Furlan, R.; Montano, N. Progressive decrease of heart period variability entropy-based complexity during graded head-up tilt. J. Appl. Physiol 2007, 103, 1143–1149. [Google Scholar]
- Brink, P.A.; Crotti, L.; Corfield, V.; Goosen, A.; Durrheim, G.; Hedley, P.; Heradien, M.; Geldenhuys, G.; Vanoli, E.; Bacchini, S.; et al. Phenotypic variability and unusual clinical severity of congenital long-QT syndrome in a founder population. Circulation 2005, 112, 2602–2610. [Google Scholar]
- Brink, P.A.; Schwartz, P.J. Of founder populations, long QT syndrome, and destiny. Heart Rhythm 2009, 6, 25–33. [Google Scholar]
- Porta, A.; Baselli, G.; Lombardi, F.; Cerutti, S.; Antolini, R.; Del Greco, M.; Ravelli, F.; Nollo, G. Performance assessment of standard algorithms for dynamic R-T interval measurement: Comparison between R-Tapex and R-Tend approach. Med. Biol. Eng. Comput 1998, 36, 35–42. [Google Scholar]
- Bazett, H.C. An analysis of the time-relations of electrocardiograms. Heart 1920, 7, 353–370. [Google Scholar]
- Turianikova, Z.; Javorka, K.; Baumert, M.; Calkovska, A.; Javorka, M. The effect of orthostatic stress on multiscale entropy of heart rate and blood pressure. Physiol. Meas 2011, 32, 1425–1437. [Google Scholar]
- Porta, A.; Faes, L.; Masé, M.; D’Addio, G.; Pinna, G.D.; Maestri, R.; Montano, N.; Furlan, R.; Guzzetti, S.; Nollo, G.; et al. An integrated approach based on uniform quantization for the evaluation of complexity of short-term heart period variability: Application to 24h Holter recordings in healthy and heart failure humans. Chaos 2007, 17. [Google Scholar] [CrossRef]
- Baumert, M.; Javorka, M.; Seeck, A.; Faber, R.; Sanders, P.; Voss, A. Multiscale entropy and detrended fluctuation analysis of QT interval and heart rate variability during normal pregnancy. Comput. Biol. Med 2012, 42, 347–352. [Google Scholar]
- Porta, A.; Tobaldini, E.; Gnecchi-Ruscone, T.; Montano, N. RT variability unrelated to heart period and respiration progressively increases during graded head-up tilt. Am. J. Physiol 2010, 298, 1406–1414. [Google Scholar]
- Negoescu, R.; Dinca-Panaitescu, S.; Filcescu, V.; Ionescu, D.; Wolf, S. Mental stress enhances the sympathetic fraction of QT variability in an RR-independent way. Integr. Physiol. Behav. Sci 1997, 32, 220–227. [Google Scholar]
- Browne, K.F.; Prystowsky, E.; Heger, J.J.; Zipes, D.P. Modulation of Q-T interval by the autonomic nervous system. PACE-Pacing Clin. Electrophysiol 1983, 6, 1050–1055. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | Number of subjects | Number of subjects acquired only BBoff | Number of subjects acquired both BBoff and BBon |
|---|---|---|---|
| NMC | 14 | 14 | 0 |
| AMC | 11 | 4 | 7 |
| SMC | 23 | 1 | 22 |
| NMC | AMC | SMC | |
|---|---|---|---|
| μHP (ms) | 697.6 ± 100.6 | 847.9 ± 143.8 § | 761.3 ± 95.0 |
| μQT (ms) | 317.6 ± 39.2 | 422.2 ± 51.7 § | 408.6 ± 42.4 § |
| μQTc (ms·s−1/2) | 397.1 ± 71.9 | 461.9 ± 33.9 § | 468.7 ± 33.4 § |
| DAY | NIGHT | |||
|---|---|---|---|---|
| AMC | SMC | AMC | SMC | |
| μHP (ms) | 847.9 ± 143.8 | 761.3 ± 95.0 | 1,022.6 ± 136.3 * | 952.4 ± 117.1 * |
| μQT (ms) | 422.2 ± 51.7 | 408.6 ± 42.4 | 447.5 ± 42.1 * | 445.3 ± 31.2 * |
| μQTc (ms·s−1/2) | 461.9 ± 33.9 | 468.9 ± 33.4 | 445.0 ± 30.5 * | 458.6 ± 25.4 |
| BBoff | BBon | |||
|---|---|---|---|---|
| AMC | SMC | AMC | SMC | |
| μHP (ms) | 855.8 ± 143.5 | 757.9 ± 95.8 | 1,038.2 ± 176.0 @ | 927.8 ± 117.2 #,@ |
| μQT (ms) | 424.0 ± 57.6 | 406.5 ± 42.1 | 426.7 ± 58.0 | 429.8 ± 29.3 @ |
| μQTc (ms·s−1/2) | 459.4 ± 43.0 | 467.5 ± 33.7 | 418.8 ± 37.2 @ | 447.4 ± 28.1 @ |
© 2014 by the authors; licensee MDPI, Basel, Switzerland This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Bari, V.; Marchi, A.; De Maria, B.; Girardengo, G.; George, A.L., Jr; Brink, P.A.; Cerutti, S.; Crotti, L.; Schwartz, P.J.; Porta, A. Low-Pass Filtering Approach via Empirical Mode Decomposition Improves Short-Scale Entropy-Based Complexity Estimation of QT Interval Variability in Long QT Syndrome Type 1 Patients. Entropy 2014, 16, 4839-4854. https://doi.org/10.3390/e16094839
Bari V, Marchi A, De Maria B, Girardengo G, George AL Jr, Brink PA, Cerutti S, Crotti L, Schwartz PJ, Porta A. Low-Pass Filtering Approach via Empirical Mode Decomposition Improves Short-Scale Entropy-Based Complexity Estimation of QT Interval Variability in Long QT Syndrome Type 1 Patients. Entropy. 2014; 16(9):4839-4854. https://doi.org/10.3390/e16094839
Chicago/Turabian StyleBari, Vlasta, Andrea Marchi, Beatrice De Maria, Giulia Girardengo, Alfred L. George, Jr, Paul A. Brink, Sergio Cerutti, Lia Crotti, Peter J. Schwartz, and Alberto Porta. 2014. "Low-Pass Filtering Approach via Empirical Mode Decomposition Improves Short-Scale Entropy-Based Complexity Estimation of QT Interval Variability in Long QT Syndrome Type 1 Patients" Entropy 16, no. 9: 4839-4854. https://doi.org/10.3390/e16094839