Integrating Social Capital Theory, Social Cognitive Theory, and the Technology Acceptance Model to Explore a Behavioral Model of Telehealth Systems

Abstract
:1. Introduction
2. Literature Review
2.1. Telecare and Telehealth
2.2. Technology Acceptance Model
2.3. Social Capital and the Technology Acceptance Model
2.4. System Self-efficacy and the Technology Acceptance Model
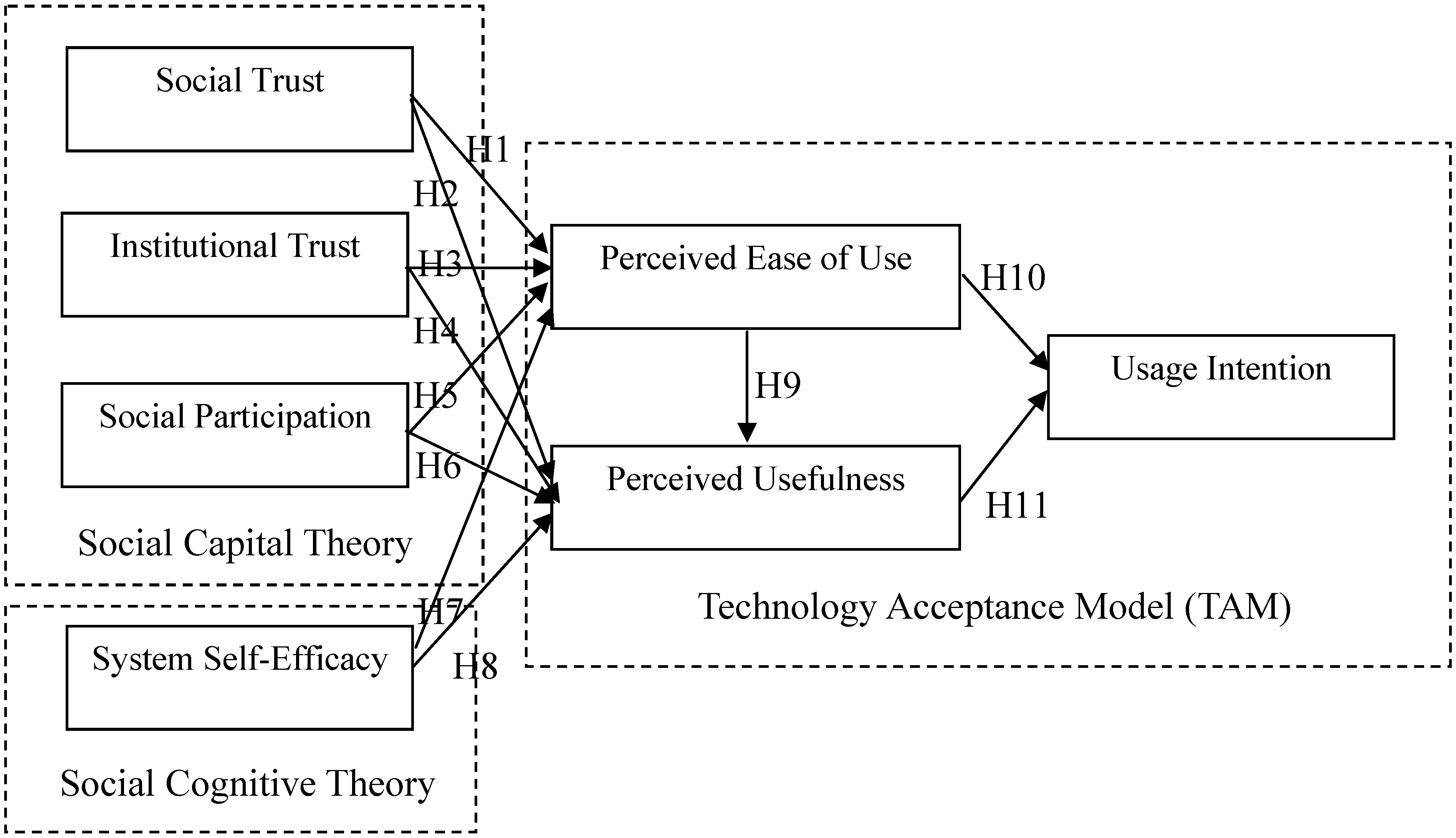
- H1: Social trust positively affects perceived ease of use in a telehealth context.
- H2: Social trust positively affects perceived usefulness in a telehealth context.
- H3: Institutional trust positively affects perceived ease of use in a telehealth context.
- H4: Institutional trust positively affects perceived usefulness in a telehealth context.
- H5: Social participation positively affects perceived ease of use in a telehealth context.
- H6: Social participation positively affects perceived usefulness in a telehealth context.
- H7: System self-efficacy positively affects perceived ease of use in a telehealth context.
- H8: System self-efficacy positively affects perceived usefulness in a telehealth context.
- H9: Perceived ease of use positively affects perceived usefulness in a telehealth context.
- H10: Perceived ease of use positively affects usage intention in a telehealth context.
- H11: Perceived usefulness positively affects usage intention in a telehealth context.
3. Research Method
3.1. Survey Method and Pretest

3.2. Measurement
3.3. Statistical Method
4. Results
4.1. Sample Characteristics

{kind=link}
{kind=link}
{kind=link}
| Construct | Mean | Standard Deviation | Minimum | Maximum |
|---|---|---|---|---|
| Social Trust | 4.70 | 0.58 | 1 | 5 |
| Institutional Trust | 4.48 | 0.69 | 2 | 5 |
| Social participation | 4.09 | 1.05 | 1 | 5 |
| System Self-efficacy | 3.44 | 1.47 | 1 | 5 |
| Perceived Ease of Use | 4.50 | 0.79 | 2 | 5 |
| Perceived Usefulness | 4.72 | 0.52 | 3 | 5 |
| Usage Intention | 4.59 | 0.70 | 2 | 5 |
4.2. Measurement Model Results
| Construct | Cronbach’s α | Composite Reliability | Average Variance Extracted |
|---|---|---|---|
| Social Trust | 0.99 | 0.99 | 0.98 |
| Institutional Trust | 0.96 | 0.96 | 0.90 |
| Social participation | 0.80 | 0.81 | 0.59 |
| System Self-efficacy | 0.99 | 0.99 | 0.97 |
| Perceived Ease of Use | 0.96 | 0.96 | 0.92 |
| Perceived Usefulness | 0.99 | 0.99 | 0.98 |
| Usage Intention | 0.99 | 0.99 | 0.99 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
|---|---|---|---|---|---|---|---|
| 1. Social Trust | (0.98) | ||||||
| 2. Institutional Trust | 0.41 | (0.90) | |||||
| 3. Social participation | 0.29 | 0.15 | (0.59) | ||||
| 4. System Self-efficacy | 0.11 | 0.08 | 0.29 | (0.97) | |||
| 5. Perceived Ease of Use | 0.33 | 0.25 | 0.26 | 0.31 | (0.92) | ||
| 6. Perceived Usefulness | 0.35 | 0.35 | 0.34 | 0.15 | 0.50 | (0.98) | |
| 7. Usage Intention | 0.33 | 0.39 | 0.24 | 0.16 | 0.43 | 0.57 | (0.99) |
4.3. Structural Model Results
| Structural Model Statistic | Fit Indices | Recommended Threshold |
|---|---|---|
| χ2 | 173.287 | - |
| χ2 / d.f. | 1.284 | <5 |
| GFI | 0.952 | >0.9 |
| AGFI | 0.933 | >0.9 |
| RMSEA | 0.028 | <0.05 |
| RMR | 0.024 | <0.05 |
| NFI | 0.986 | >0.9 |
| RFI | 0.982 | >0.9 |
| IFI | 0.997 | >0.9 |
| TLI | 0.996 | >0.9 |
| CFI | 0.997 | >0.9 |
4.4. Hypotheses Testing
| Path | Results | Standardized Path Estimate |
|---|---|---|
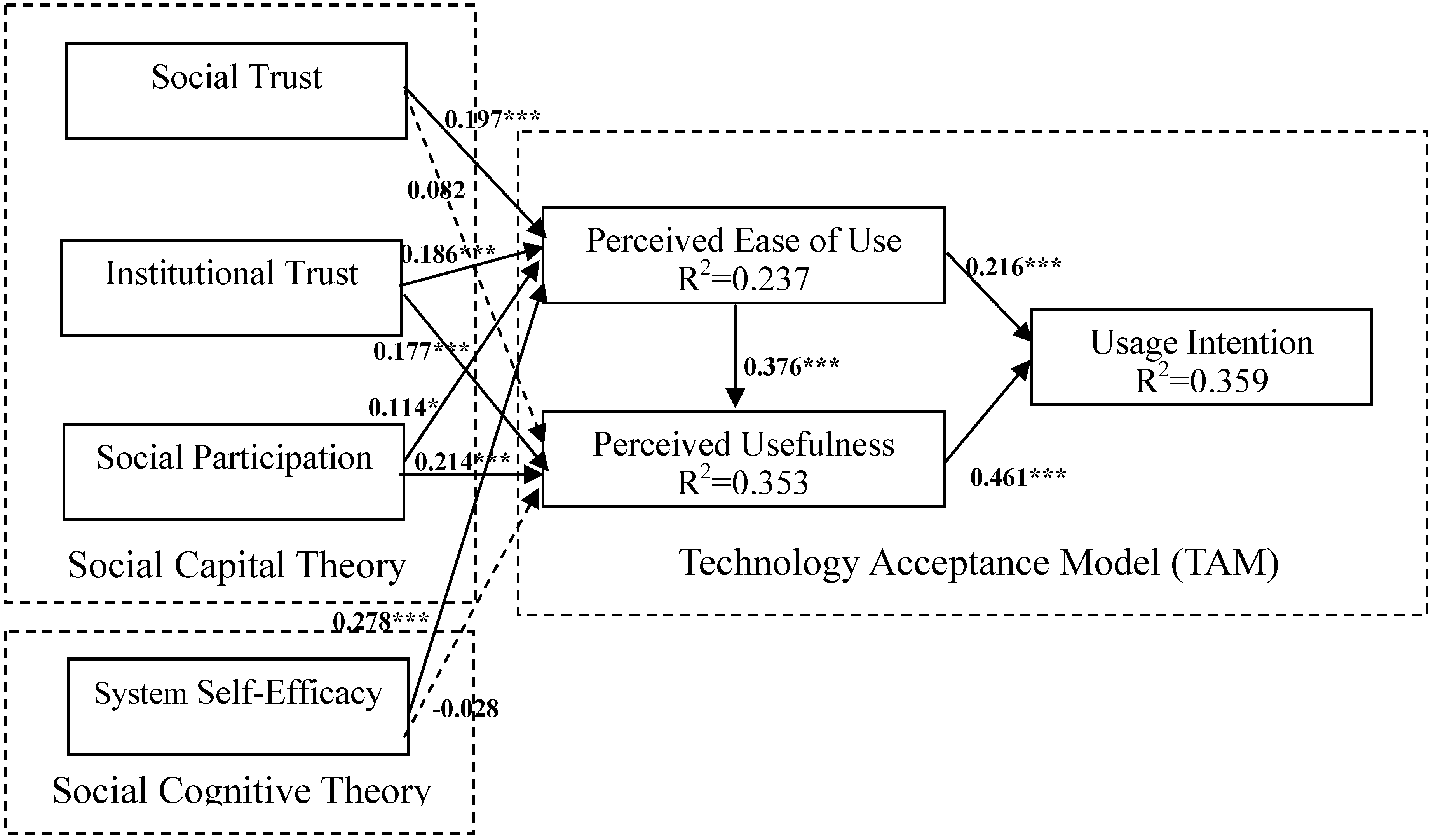
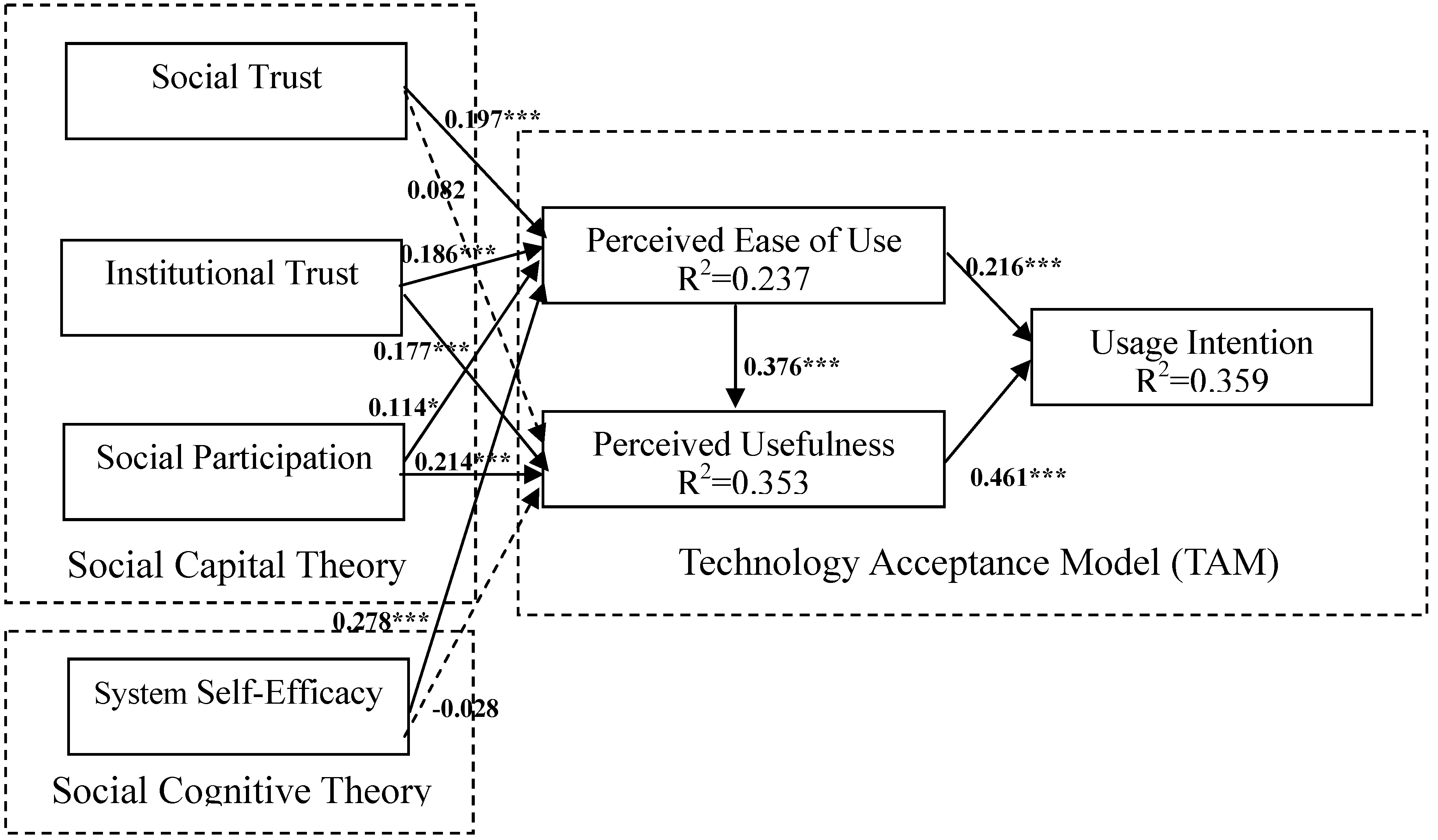
| H1 Social Trust ➔ Perceived Ease of Use | Supported | 0.197 *** |
| H2 Social Trust ➔ Perceived Usefulness | Not Supported | 0.082 |
| H3 Institutional Trust ➔ Perceived Ease of Use | Supported | 0.186 *** |
| H4 Institutional Trust ➔ Perceived Usefulness | Supported | 0.177 *** |
| H5 Social Participation ➔ Perceived Ease of Use | Supported | 0.114 * |
| H6 Social Participation ➔ Perceived Usefulness | Supported | 0.214 *** |
| H7 System Self-Efficacy ➔ Perceived Ease of Use | Supported | 0.278 *** |
| H8 System Self-Efficacy ➔ Perceived Usefulness | Not Supported | -0.028 |
| H9 Perceived Ease of Use ➔ Perceived Usefulness | Supported | 0.376 *** |
| H10 Perceived Ease of Use ➔ Intention to Use | Supported | 0.216 *** |
| H11 Perceived Usefulness ➔ Intention to Use | Supported | 0.461 *** |
| Construct | Perceived Ease of Use | Perceived Usefulness | Intention to Use |
|---|---|---|---|
| Social Trust | NA/0.197 | 0.082/0.156 | 0.077/0.077 |
| Institutional Trust | NA/0.186 | 0.177/0.247 | 0.154/0.154 |
| Social Participation | NA/0.114 | 0.214/0.257 | 0.143/0.143 |
| System Self-Efficacy | NA/0.278 | −0.028/0.077 | 0.096/0.096 |
| Perceived Ease of Use | - | NA/0.376 | 0.173/0.389 |
| Perceived Usefulness | - | - | NA/0.461 |
| Intention to Use | - | - | - |
5. Discussion
6. Conclusions
Acknowledgments
Conflicts of Interest
References
- Huang, J.C. Innovative health care delivery system—A questionnaire survey to evaluate the influence of behavioral factors on individuals’ acceptance of telecare. Comput. Biol. Med. 2013, 43, 281–286. [Google Scholar] [CrossRef]
- Güler, N.F.; Übeyli, E.D. Theory and applications of telemedicine. J. Med. Syst. 2002, 26, 199–220. [Google Scholar] [CrossRef]
- Hendy, J.; Barlow, J. The adoption of telecare in the community. Community Pract. 2012, 85, 41–43. [Google Scholar]
- Moffatt, J.J.; Eley, D.S. The reported benefits of telehealth for rural Australians. Aust. Health Rev. 2010, 34, 276–281. [Google Scholar] [CrossRef]
- Young, L.B.; Foster, L.; Silander, A.; Wakefield, B.J. Home telehealth: Patient satisfaction, program functions, and challenges for the care coordinator. J. Gerontol. Nurs. 2011, 37, 38–46. [Google Scholar] [CrossRef]
- Johnston, B.; Kidd, L.; Wengstrom, Y.; Kearney, N. An evaluation of the use of telehealth within palliative care settings across Scotland. Palliat. Med. 2011, 26, 152–161. [Google Scholar]
- Venkatesh, V.; Davis, F.D. A theoretical extension of the technology acceptance model: Four longitudinal field studies. Manag. Sci. 2000, 46, 186–204. [Google Scholar] [CrossRef]
- Hasan, B. Examining the effects of computer self-efficacy and system complexity on technology acceptance. Inform. Resour. Manag. J. 2007, 20, 76–88. [Google Scholar] [CrossRef]
- Liu, C.F.; Tsai, Y.C.; Jang, F.L. Patients’ acceptance towards a web-based personal health record system: An empirical study in Taiwan. Int. J. Environ. Res. Publ. Health 2013, 10, 5191–5208. [Google Scholar] [CrossRef]
- Rahimpour, M.; Lovell, N.H.; Celler, B.G.; McCormick, J. Patients’ perceptions of a home telecare system. Int. J. Med. Inform. 2008, 77, 486–498. [Google Scholar] [CrossRef]
- Wade, R.; Cartwright, C.; Shaw, K. Factors relating to home telehealth acceptance and usage compliance. Risk Manag. Healthc. Pol. 2012, 5, 25–33. [Google Scholar] [CrossRef]
- Davis, F.D. User acceptance of information technology: System characteristics, user perceptions and behavioral impacts. Int. J. Man. Mach. Stud. 1993, 38, 475–487. [Google Scholar] [CrossRef]
- Putnam, R. Making Democracy Work—Civic Traditions in Modern Italy; Princeton University Press: Englewood Cliffs, NJ, USA, 1993. [Google Scholar]
- Kawachi, I.; Kennedy, B.P. Health and social cohesion: Why care about income inequality. Brit. Med. J. 1997, 314, 1037–1040. [Google Scholar] [CrossRef]
- Bandura, A. Social Foundation of Thought and Action: A Social Cognitive Theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Venkatesh, V.; Davis, F.D. A model of the antecedents of perceived ease of use: Development and test. Decis. Sci. J. 1996, 27, 451–481. [Google Scholar] [CrossRef]
- Dewsbury, G. Defining Telecare? Available online: http://thetelecareblog.blogspot.tw/2009/02/defining-telecare.html (accessed on 5 May 2014).
- Lee, C.Y.; Huang, E.W.; Chiou, S.F.; Yang, R.J.; Chao, P.J.; Hung, R.S.; Lin, Y.T. Design and development of a new community healthcare management model by using telehealth service system. J. Taiwan Assoc. Med. Inform. 2009, 18, 39–53. [Google Scholar]
- Brownsell, S.; Blackburn, S.; Hawley, M.S. An evaluation of second and third generation telecare services in older people’s housing. J. Telemed. Telecare 2008, 14, 8–12. [Google Scholar] [CrossRef]
- Miller, T.W.; Miller, J.M.; Kraus, R.F.; Kaak, O.; Sprang, R.; Veltkamp, L.J. Telehealth: A clinical application model for rural consultation. Consult. Psychol. J. Pract. Res. 2003, 55, 119–127. [Google Scholar] [CrossRef]
- Ahn, T.; Ryu, S.; Han, I. The impact of web quality and playfulness on user acceptance of online retailing. Inform. Manage. 2007, 44, 263–275. [Google Scholar] [CrossRef]
- Davis, F.D.; Bagozzi, R.P.; Warshaw, P.R. User acceptance of computer technology: A comparison of two theoretical models. Manag. Sci. 1989, 35, 982–1002. [Google Scholar] [CrossRef]
- Or, C.; Karsh, B.T.; Severtson, D.J.; Burke, L.J.; Brown, R.L.; Brennan, P.F. Factors affecting home care patients’ acceptance of a web-based interactive self-management technology. J. Amer. Med. Inform. Assoc. 2011, 18, 51–59. [Google Scholar] [CrossRef]
- DeLone, W.H.; McLean, E.R. The DeLone and McLean model of information systems success: A ten-year update. J. Manage. Inform. Syst. 2003, 19, 9–30. [Google Scholar]
- Mathieson, K. Predicting user intention: comparing the technology acceptance model with theory of planned behavior. Inform. Syst. Res. 1991, 2, 173–191. [Google Scholar] [CrossRef]
- Jackson, C.M.; Chow, S.; Leitch, R.A. Toward an understanding of the behavioral intention to use an information system. Decision Sci. 1997, 28, 357–389. [Google Scholar] [CrossRef]
- Williams, M.D.; Slade, E.L.; Dwivedi, Y.K. Consumers’ intentions to use e-readers. J. Comput. Inform. Syst. 2014, 54, 66–76. [Google Scholar]
- Hu, P.J.; Chau, P.Y.K.; Liu Sheng, O.R.; Kar, Y.T. Examining the technology acceptance model using physician acceptance of telemedicine technology. J. Manage. Inform. Syst. 1999, 16, 91–112. [Google Scholar]
- Bourdieu, P. The Forms of Capital. In Handbook of Theory and Research for the Sociology of Education; Richardson, J.G., Ed.; Greenwood: New York, NY, USA, 1985. [Google Scholar]
- Coleman, J. Foundations of Social Theory; Harvard University Press: Cambridge, MA, USA, 1990. [Google Scholar]
- Woolcock, M. Social capital and economic development: Toward a theoretical synthesis and policy framework. Theor. Soc. 1998, 27, 151–208. [Google Scholar] [CrossRef]
- Nahapiet, J.; Ghoshal, S. Social capital, intellectual capital, and the organizational advantage. Acad. Manage. Rev. 1998, 23, 242–266. [Google Scholar]
- Felício, J.A.; Couto, E.; Caiado, J. Human capital and social capital in entrepreneurs and managers of small and medium enterprises. J. Bus. Econ. Manage. 2012, 13, 395–420. [Google Scholar] [CrossRef]
- Adler, P.S.; Kwon, S.W. Social capital: Prospects for a new concept. Acad. Manage. Rev. 2002, 27, 17–40. [Google Scholar]
- Kawachi, I.; Kennedy, B.P.; Glass, R. Social capital and self-rated health: A contextual analysis. Amer. J. Publ. Health 1999, 89, 1187–1193. [Google Scholar] [CrossRef]
- Lindstrom, M.; Janzon, E. Social capital, institutional (vertical) trust and smoking: A study of daily smoking and smoking cessation among ever smokers. Scand. J. Public Health 2007, 35, 460–467. [Google Scholar] [CrossRef]
- Nummela, O.; Sulander, T.; Rahkonen, O.; Karisto, A.; Uutela, A. Social participation, trust, and self-rated health: A study among ageing people in urban, semi-urban and rural settings. Health Place 2008, 14, 243–253. [Google Scholar] [CrossRef]
- Mohseni, M.; Lindstrom, M. Social capital, trust in the health-care system and self-rated health: The role of access to health care in a population-based study. Soc. Sci. Med. 2007, 64, 1373–1383. [Google Scholar] [CrossRef]
- Russell, S. Treatment seeking behaviour in urban Sri Lanka: Trusting the state, trusting private doctors. Soc. Sci. Med. 2005, 61, 1396–1407. [Google Scholar] [CrossRef]
- Cattell, V. Poor people, poor places, and poor health: The mediating role of social networks and social capital. Soc. Sci. Med. 2001, 52, 1501–1516. [Google Scholar] [CrossRef]
- Wang, L.; Graddy, E. Social capital, volunteering, and charitable giving. Int. J. Volunt. Nonprofit Organ. 2008, 19, 23–42. [Google Scholar] [CrossRef]
- Reid, M. Integrating trust and computer self-efficacy with TAM: An empirical assessment of customers’ acceptance of banking information systems (BIS) in Jamaica. J. Inter. Bank. Commerce 2008, 12, 1–18. [Google Scholar]
- Gefen, D.; Karahanna, E.; Straub, D.W. Trust and TAM in online shopping: an integrated model. MIS Quart. 2003, 27, 51–90. [Google Scholar]
- Pavlou, P.A. Consumer acceptance of electronic commerce: Integrating trust and risk with the technology acceptance model. Int. J. Electron. Commerce 2003, 7, 101–134. [Google Scholar]
- Chow, W.S.; Chan, L.S. Social network, social trust and shared goals in organizational knowledge sharing. Inform. Manage. 2008, 45, 458–465. [Google Scholar] [CrossRef]
- Shu, Q.; Tu, Q.; Wang, K. The impact of computer self-efficacy and technology dependence on computer-related technostress: A social cognitive theory perspective. Int. J. Human-Computer Interact. 2011, 27, 923–939. [Google Scholar]
- Gist, M.E. Self-efficacy: Implications for organizational behavior and human resource management. Acad. Manage. Rev. 1987, 12, 472–485. [Google Scholar]
- Compeau, D.R.; Higgins, C.A. Computer self-efficacy: Development of a measure and initial test. MIS Quart. 1995, 19, 189–211. [Google Scholar] [CrossRef]
- Venkatesh, V. Determinants of perceived ease of use: Integrating control, intrinsic motivation, and emotion into the technology acceptance model. Inform. Syst. Res. 2000, 11, 342–365. [Google Scholar] [CrossRef]
- Ong, C.S.; Lai, J.Y.; Wang, Y.S. Factors affecting engineers’ acceptance of asynchronous e-learning systems in high-tech companies. Inform. Manage. 2004, 41, 795–804. [Google Scholar] [CrossRef]
- Hung, S.Y.; Liang, T.P. Effect of computer self-efficacy on the use of executive support systems. Industrial Manage. Data Syst. 2001, 101, 227–237. [Google Scholar] [CrossRef]
- Davis, F.D. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Quart. 1989, 13, 319–340. [Google Scholar] [CrossRef]
- Bentler, P.M. Handbook of Multivariate Experimental Psychology; Plenum: New York, NY, USA, 1988. [Google Scholar]
- Anderson, J.C.; Gerbing, D.W. Structural equation modeling in practice: A review and recommended two-step approach. Psychol. Bull. 1988, 103, 411–423. [Google Scholar] [CrossRef]
- Hair, J.F.; Anderson, R.E.; Tatham, R.L.; Black, W.C. Multivariate Data Analysis; Prentice-Hall: Englewood, NJ, USA, 1998. [Google Scholar]
- Nunnally, J.C. Psychometric Theory, 2nd ed.; McGraw-Hill: New York, NY, USA, 1978. [Google Scholar]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Market Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Liu, I.F.; Chen, M.C.; Sun, Y.S.; Wible, D.; Kuo, C.H. Extending the TAM model to explore the factors that affect intention to use an online learning community. Comput. Educ. 2010, 54, 600–610. [Google Scholar] [CrossRef]
- Holbert, R.L.; Stephenson, M.T. The importance of indirect effects in media effects research: Testing for mediation in structural equation modeling. J. Broadcast. Electron. 2003, 4, 556–572. [Google Scholar] [CrossRef]
- Chau, P.Y.K. Influence of computer attitude and self-efficacy on IT usage behavior. J. End-User Comput. 2001, 13, 1, 40–52. [Google Scholar]
- Kwak, N.; Shah, D.V.; Holbert, R.L. Connecting, trusting, and participating: The direct and interactive effects of social associations. Polit. Res. Quart. 2004, 57, 643–652. [Google Scholar] [CrossRef]
- Bakken, S.; Grullon-Frigueroa, L.; Izquierdo, R.; Lee, N.J.; Morin, P.; Palmas, W.; Teresi, J.; Weinstock, R.S.; Shea, S.; Starren, J. Development, validation, and use of English and Spanish versions of the telemedicine satisfaction and usefulness questionnaire. J. Amer. Med. Inform. Assoc. 2006, 13, 660–667. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Tsai, C.-H. Integrating Social Capital Theory, Social Cognitive Theory, and the Technology Acceptance Model to Explore a Behavioral Model of Telehealth Systems. Int. J. Environ. Res. Public Health 2014, 11, 4905-4925. https://doi.org/10.3390/ijerph110504905
Tsai C-H. Integrating Social Capital Theory, Social Cognitive Theory, and the Technology Acceptance Model to Explore a Behavioral Model of Telehealth Systems. International Journal of Environmental Research and Public Health. 2014; 11(5):4905-4925. https://doi.org/10.3390/ijerph110504905
Chicago/Turabian StyleTsai, Chung-Hung. 2014. "Integrating Social Capital Theory, Social Cognitive Theory, and the Technology Acceptance Model to Explore a Behavioral Model of Telehealth Systems" International Journal of Environmental Research and Public Health 11, no. 5: 4905-4925. https://doi.org/10.3390/ijerph110504905
APA StyleTsai, C.-H. (2014). Integrating Social Capital Theory, Social Cognitive Theory, and the Technology Acceptance Model to Explore a Behavioral Model of Telehealth Systems. International Journal of Environmental Research and Public Health, 11(5), 4905-4925. https://doi.org/10.3390/ijerph110504905