
Urgent-Start Peritoneal Dialysis: Current State and Future Directions

1
The Warren Alpert Medical School of Brown University, Providence, RI 02903, USA
2
Division of Kidney Disease and Hypertension, Rhode Island Hospital, Providence, RI 02903, USA
*
Author to whom correspondence should be addressed.
Kidney Dial. 2024, 4(1), 15-26; https://doi.org/10.3390/kidneydial4010002
Submission received: 13 October 2023
/
Revised: 28 December 2023
/
Accepted: 29 December 2023
/
Published: 4 January 2024
(This article belongs to the Special Issue Feature Papers for Kidney and Dialysis: Advances in Nephrology and Dialysis—Series II)
Abstract
:Urgent-start peritoneal dialysis (USPD) is defined as peritoneal dialysis initiated within 14 days of catheter insertion. In this review, the authors describe the most recent data on USPD, including outcomes, complications, barriers to implementation, and areas for future research. Outcomes appear similar between catheter insertion techniques, so patient factors and institutional workflow should guide practice. Mechanical complications may occur at a higher rate in USPD, but it does not impact technique survival or mortality. Infectious complications appear unchanged in USPD, and there may be fewer complications compared to urgent-start hemodialysis. Barriers to implementation are multifactorial, including physician and staff unfamiliarity and lack of institutional support. A significant limitation within the field includes lack of uniform terminology and definitions.
1. Introduction
Hemodialysis (HD) remains the most common form of renal replacement therapy in the United States, accounting for over 85% of incident dialysis in 2020 [1]. However, peritoneal dialysis (PD) is equally efficacious and allows patients to dialyze at home, leading to increased independence and quality of life for patients [2,3]. Furthermore, due to decreased healthcare costs and infrastructure, many countries are creating incentives to increase the percentage of patients on PD [4]. However, these incentives have not always been effective, and compared to locations such as Hong Kong, New Zealand, and Thailand, the United States lags far behind in PD utilization [5]. While dialysis ideally occurs after months to years of pre-dialysis care, up to 33% of patients receive little to no nephrology care before dialysis, and up to 60% of dialysis is initiated unplanned [6]. Peritoneal dialysis is a viable option for patients initiating dialysis in an unplanned manner, even prior to catheter site maturation. Typically, the catheter is placed and remains unused for at least 14 days. When initiated prior to 14 days after catheter implantation, it is termed urgent-start peritoneal dialysis (USPD). Furthermore, the majority of patients who begin dialysis while in the hospital continue the same modality as outpatients [7]. Given that a high percentage of patients initiate dialysis unplanned and many patients continue the same modality in the hospital, expanding the use of USPD may increase the use in the outpatient setting, especially among those who originally elected for PD. In an effort to maintain PD as an option for patients in the outpatient setting, USPD has been studied to determine its efficacy, especially in comparison to planned PD and urgent-start hemodialysis (USHD). In this literature review, we will highlight the impactful and recent literature on urgent-start dialysis. Due to a lack of coverage by Medicare for USPD in acute kidney injury, this review will focus on the application of USPD in the setting of end-stage kidney disease. Attention will be given to current definitions of urgent-start dialysis given its heterogeneity in current literature. We will discuss the clinical considerations, efficacy, current system-wide practices and barriers, and future directions of USPD.
2. Clinical Considerations in Urgent-Start Peritoneal Dialysis
2.1. Patient Selection Criteria for USPD
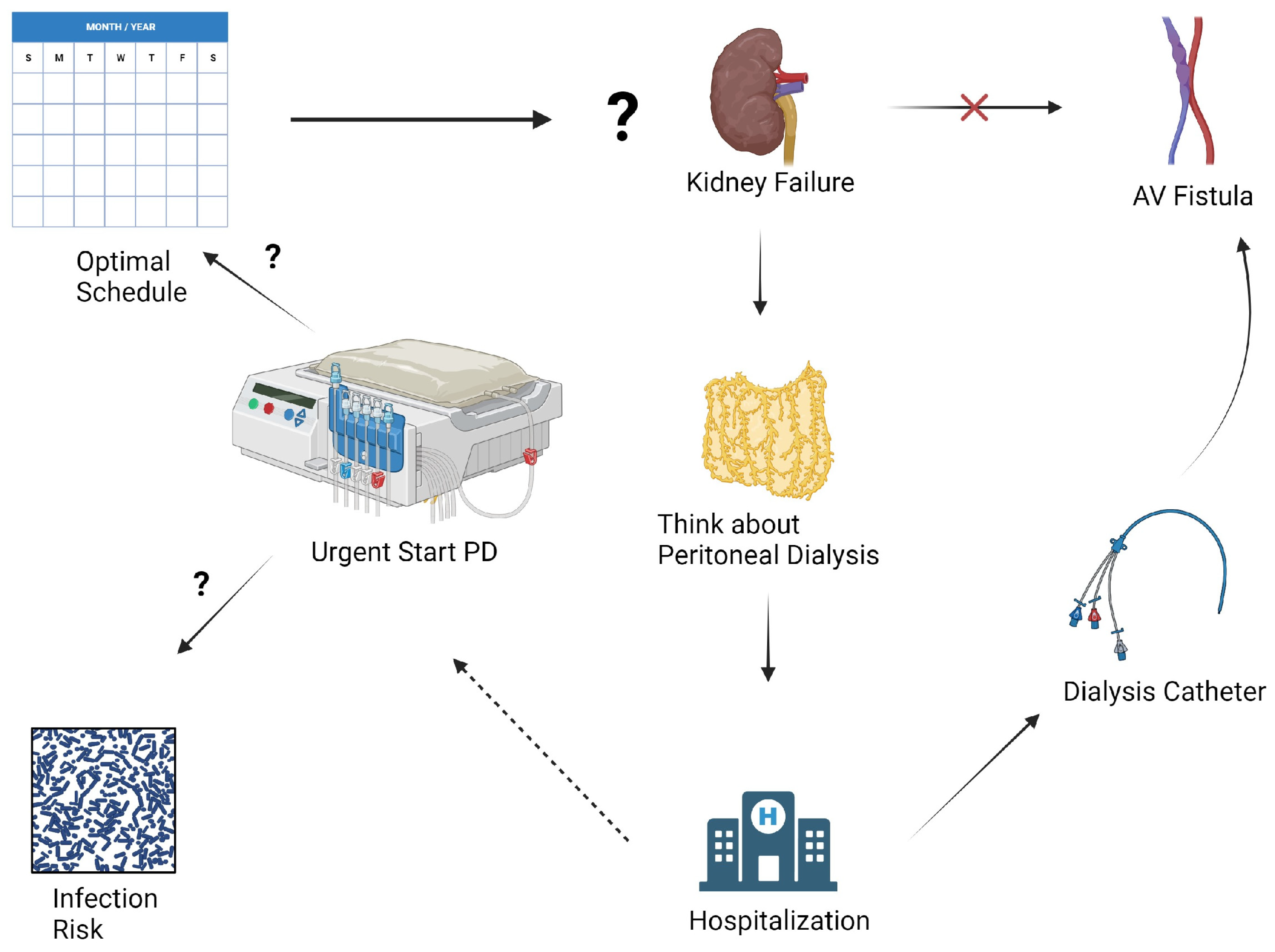
Prior to initiating USPD, the patient must first go through a thorough evaluation. The initial evaluation can be performed by a nurse, social-worker, nurse care manager, nephrology fellow, or attending nephrologist using a standardized questionnaire [8]. There are few absolute contraindications to PD, especially if PD is to be started immediately in the inpatient setting. Broadly, PD requires a peritoneal cavity free of significant scarring or adhesions, a clean environment where exchanges can occur, and the mental/physical ability to perform PD [9]. Although some urgent-start PD may begin in the hospital, it is often initiated in outpatients, and therefore, social factors must also be considered. Due to the risk of infection, a clean environment in a stable home is required [9]. Given the increased patient responsibility in PD, including performing self-exchanges, the patient must have a high degree of motivation for PD and health literacy. When this is not met, or the patient has cognitive impairment, a caregiver or family member must meet these qualifications. Among the most important aspects of patient selection criteria is patient preference. While education in the inpatient setting may be time consuming and logistically difficult, it facilitates shared decision making and is vital to patient selection in USPD [10]. Most patients who initiate dialysis as inpatients will continue the same modality as outpatients [7]. Therefore, some patients who originally elected for outpatient PD but received USHD as inpatients may continue without their preferred modality. This process is described in Figure 1. In a patient who is a candidate for both USPD and USHD, it is most reasonable to initiate their preferred maintenance modality. USPD may be suboptimal in situations in which rapid clearance is needed such as severe hyperkalemia, severe acidosis, or ingestions.
2.2. Timing of Initiation and Current Data Limitations
Conventional-start PD is defined as dialysis beginning 14 days or more after placement of a PD catheter. Given that a high percentage of patients require dialysis unplanned, the term “urgent start peritoneal dialysis” is applied to dialysis that begins prior to 14 days. However, recent literature has called for further dividing of USPD terminology, as some patients initiate PD within 24 h, while others begin after 13 days. Given the patients who require dialysis within 24 h are quite different from those who begin after 13 days, and there may be large differences in catheter site maturation, new definitions have been proposed. In 2018, Blake et al. proposed the terms “urgent start” for those who began within 72 h, and “early start” for those who began within 14 days [11]. Since publication, there has been an increase in literature that specifically separates these groups. Unfortunately, there is still limited uniformity and adoption of this terminology, as noted in Table A1. Authors have used variable terminology, including “early start” to refer to within 72 h and planned start to refer to within 14 days [12]. In current literature, the use of “urgent start” is too variable for readers to determine the author’s specific intended use. Furthermore, much of the literature can be difficult to compare, as studies define “urgent start” differently, therefore introducing selection bias as a confounder. Throughout the remainder of this review, as much detail on the author’s definition of urgent start as possible will be provided, but readers must be aware of current definitions as a significant limitation of this review. We propose the terms “emergent start peritoneal dialysis” and “early start peritoneal dialysis” be used, with emergent start PD being defined as PD within 72 h of catheter insertion and early start being PD 72 h to 14 days from catheter insertion.
2.3. Catheter Insertion Techniques
Multiple techniques are available to insert catheters for PD. These techniques can be performed both in inpatient and outpatient settings, and depending on the technique, can be implanted by different specialties. Techniques include open surgical, laparoscopic, interventional radiology-guided insertion, or percutaneously by nephrology. Among nonsurgical techniques, both fluoroscopy and ultrasound have demonstrated effectiveness [13]. Most commonly, a PD catheter is placed and secured using a double purse string technique. Among the studies reviewed, six studies compared outcomes between different implantation techniques, including infectious, mechanical, and catheter failure. None of the studies reviewed demonstrated a difference in outcomes [13,14,15,16,17,18]. Additionally, these findings are corroborated by a separate Cochrane review which concluded that no technique leads to different rates of peritonitis, technique failure, or mortality [19]. Given the lack of difference in clinical outcomes, it is up to the provider and institution to determine the appropriate modality based on patient and institutional factors. Each technique has its advantages and disadvantages, so the ideal technique is dependent on the ideal patient [7]. Surgical techniques may be ideal for a patient with a history of abdominal surgeries to allow for lysis of adhesions, but may have higher costs, require operating room (OR) time, and raise anesthesia concerns. Conversely, an institution that primarily inserts PD catheters using interventional radiology or bedside nephrology techniques may be able to perform the procedures quicker, at a lower cost, and without general anesthesia, but may not be able to offer PD to patients with a prior history of abdominal surgery [7]. Hence institutions should be able to offer all the techniques to meet the needs of individual patients and should develop institution-specific algorithms based on their available resources.
2.4. Peritoneal Dialysis Prescription and Modality Choices
When determining an initial PD prescription, there are various forms of PD a provider may choose. Given the concern for increased complications in USPD compared to conventional PD, investigators are interested in whether a certain prescription may decrease complications. Options include automated peritoneal dialysis (APD) and continuous ambulatory peritoneal dialysis (CAPD). Typically, patients receiving USPD will receive incremental PD (IPD) in which their prescription considers residual kidney function. One study of patients undergoing USPD compared APD and intermittent peritoneal dialysis (IPD) and showed that serum potassium and phosphorus were lower in the APD group, suggesting electrolyte clearance may be superior in APD [20]. Two studies investigated the outcomes of patients prescribed APD, CAPD, or combination APD-CAPD in patients requiring USPD, where patients began on APD for 3 days and then switched to CAPD. Both studies demonstrated that combination APD-CAPD is superior at removing small-molecule toxins and correcting electrolyte imbalances [21,22]. In one of these studies, the APD-alone group demonstrated decreases in serum albumin that were not shown in the APD-CAPD group, suggesting that CAPD may be suggestive against protein loss. There is some concern that APD may lead to increased mechanical complications [23], so researchers have attempted to determine if low-volume prescriptions in supine position have been proposed as a way to decrease complications. Multiple studies have investigated this and found that low-volume prescriptions in supine position reduce mechanical complications [23,24,25]. Based on these findings, combination APD-CAPD may be the optimal prescription in USPD and should be further investigated given the limited number of studies. In addition, when using APD alone, low-volume prescriptions in supine position may reduce mechanical complications.
3. Outcomes and Efficacy of Urgent-Start Peritoneal Dialysis
3.1. Mechanical Complications and Technique Failure
Given most PD outcome data include patients who initiated PD after 14 days, clinical outcomes among those undergoing USPD are less well-defined. Mechanical complications such as catheter leaks and migrations are common in USPD. Rates of catheter leak at 30 days vary widely from 2.6% to 12% [25,26,27], and migration rates ranged from 2% to 12% at 30 days [25,26,27]. Overall catheter complications were also highly variable, with one study of 2059 patients reporting a 7.6% rate over a mean 36.5-month follow-up [28], compared to another study that showed a rate of 33.3% at 90 days [29]. Additionally, there is interest in determining if outcomes differ between conventional-start PD and USPD, and recent literature has investigated this relationship. The primary fear among patients who undergo USPD is increased mechanical complications, such as catheter dysfunction, and leakage, due to an immature site. Assuming the accuracy of this proposed mechanism, patients beginning with 72 h may have more mechanical complications than patients beginning with 14 days. Generally, most investigators appear to agree that mechanical complications occur at a higher rate in USPD [30]. Among the studies reviewed, the majority demonstrated an increase in mechanical complications in USPD [12,13,18,31,32,33]. The catheter site maturation hypothesis is further supported by a study by Kim et al. which compared 103 patients who began PD within 48 h vs. patients who began within 2 to 13 days. In this study, there were increased mechanical complications and the need for catheter repositioning procedures among the 48 h group [18]. While this supports evidence that patients who initiate within 48 h have a higher rate of mechanical complications, additional studies demonstrate that initiation within 14 days is associated with increased dialysate leakage (7.6%) compared to conventional-start PD (0.8%) and catheter malfunction (4.5% vs. 3.3%) [32]. While many investigators cite this as an accepted concept, some studies have demonstrated no difference in mechanical complications based on start time [34,35,36]. Furthermore, these studies included sample sizes of 56, 137, and 871, and included initiation timeframes of less than 24 h or within 14 days, reducing the likelihood of these factors skewing results. The ability to draw conclusions is limited by the inconsistency in the method of PD used by the reviewed studies. The majority of studies report that both CAPD and APD were used without reporting the percentages of patients on each modality. Additionally, a small percentage of studies used IPD. Given that the PD prescription may impact mechanical complications, the conclusions are weakened. While most studies have demonstrated increased mechanical complications, it appears there is some dissenting literature. However, regardless of whether the study showed a difference in complication rate, all studies demonstrated no difference in technique survival [12,14,18,31,32,33,34,35,36]. Furthermore, among studies reporting mortality, there was no difference in mortality based on time to PD initiation [31,32,33,37]. Therefore, the literature currently suggests there may be an increase in mechanical complications in USPD, but it does not affect technique survival or mortality.
3.2. Infectious Complications
Peritonitis is a common complication of PD [3]. There is interest in determining the approximate rate of peritonitis in USPD and whether it is different to conventional-start PD. Reported peritonitis rates at 30 days in USPD range from 0% to 8.6% [25,26,27,36]. Catheter site infection rates also vary widely from 0% to 12% [26,27,28]. One study of 310 diabetic patients found a 0.3% rate, while another smaller study of 26 patients found 12%, likely reflecting sample size differences. Additionally, one study found overall infectious complications to be 17% [38]. Although the crude rates were inconsistent, none of the studies demonstrated a statistically significant difference in peritonitis rates at 30 days when compared to conventional PD [24,25,26,27,35]. Additionally, time to first peritonitis [25,28] and peritonitis at one year was not different [25]. Therefore, variable peritonitis rates likely reflect differences in patient factors and methodology rather than PD start time. Gram-positive organisms, especially Staphylococcus aureus (22–31% of infections) and coagulase negative Staphylococcus (13.8–28%), were the most common infectious organisms identified [25,28]. In summary, while crude peritonitis rates in USPD are variable, evidence suggests no significant differences in peritonitis risk between USPD and conventional-start PD when accounting for patient factors. However, further research is needed to additionally clarify the relationship.
3.3. Survival Rates and Patient Outcomes in USPD Compared to Other Modalities
Studies have compared outcomes between USPD and USHD to guide modality selection. USHD has a significantly higher 30-day bacteremia rate (13.4–21%) than USPD (3.0–3.1%) [39,40]. One such study reported a higher mortality rate due to infection, although the trend was not significant (p = 0.11) [39]. A Cochrane review also found more bacteremia with USHD versus USPD [41]. While the available evidence suggests USHD has a higher rate of bacteremia, overall complications may also be higher. Overall dialysis complications in USPD at 30 days were reported as 4.5–5.7% in USPD, compared to 10.7–24% in USHD [40,42,43]. Another study reported lower composite rates of infection at 6 weeks [44]. Multiple studies also found USHD was an independent risk factor for dialysis-related complications [40,42,45]. While the current literature suggests there are likely lower rates of bacteremia and dialysis-related complications in USPD, it is less definitive for overall mortality. Three studies reported lower rates of mortality in USPD [39,40,43], while three studies reported no difference in mortality [30,42,45]. Further studies are needed to determine if there is a mortality difference. Nonetheless, available data suggest USPD may result in better complication outcomes.
3.4. Impact of USPD on Healthcare Utilization
The use of peritoneal dialysis is increasing in developing countries, partially due to potentially lower costs and infrastructure needs compared to hemodialysis. However, the impact of complications on costs in urgent-start PD is unclear. One study analyzed costs in the first 90 days for USPD versus USHD. Mean costs were lower with USPD (USD 16,398) versus USHD (USD 19,352), primarily due to lower access-related costs (USD 2492 for USPD versus USD 5227 for USHD) [46]. The higher USHD costs reflect initial catheter placement and subsequent permanent access creation. Patients starting with USHD then transitioning to PD had similar costs to USHD alone (USD 19,400) [46]. A limitation of this study includes the method of access procedure. The cited study used procedure codes including both laparoscopic and percutaneous PD catheter insertion techniques. Given the preferred method differs by institution, and operating room time can significantly impact costs, these average costs may not be generalizable to other institutions. Another study in China found significantly lower mean costs for USPD (RMB 32,386) versus USHD (RMB 52,952), approximately 40% less [47]. Overall, these studies suggest that initiating USPD as the first modality may be successful in controlling healthcare expenditure.
4. Barriers and Strategies to Optimize Urgent-Start Peritoneal Dialysis
4.1. Multidisciplinary Approach and Team Collaboration
Implementing USPD presents logistical challenges including coordination across multiple specialties and ensuring adequate staff familiarity with the modality. A summary of barriers is presented in Figure 2. A standardized evaluation helps identify appropriate candidates, considering social support, medical history, and functional status [8]. Extensive patient education is required as PD relies heavily on patient involvement, presenting workflow challenges when initiating PD urgently in the inpatient setting. Nurses, physicians, dieticians, psychologists, and administrators play a critical role in a successful PD program. Adequate nurse staffing ratios are crucial, since nurses complete many USPD tasks and may lack familiarity compared to conventional PD initiation [8]. Involving nurses in USPD protocol development can optimize success [8]. Post-initiation, vigilant nursing care may reduce complications through early issue recognition and intervention. Timely catheter placement also remains a barrier, as operators are often less comfortable with PD versus HD catheters [48], and catheters must be placed as soon as possible to initiate USPD. Operating room implantation, while facilitating adhesiolysis, presents logistical hurdles. Percutaneous insertion by interventional radiology or nephrology allows for urgent bedside placement in uncomplicated cases [49]. However, ideal methods likely vary across institutions based on resources and expertise. Unfortunately, nephrology trainees often lack confidence in PD catheter skills [50]. While percutaneous techniques are an option, backup surgical support is imperative for managing complications [51]. A coordinated multidisciplinary approach is essential for addressing the logistical challenges of initiating urgent PD.
4.2. Education and Training Programs for Healthcare Professionals
Hemodialysis is a far more prevalent modality than PD in most countries [1]. Due to a lack of exposure, many nephrologists and nephrology trainees do not feel comfortable prescribing PD. This concept is amplified with USPD. One study demonstrated that most fellows felt “moderately comfortable” with PD, and only 3% had ever initiated someone on USPD [50]. Furthermore, only 11% had ever observed a PD catheter insertion, and 3.8% felt competent placing a PD catheter [50]. In candidate patients, it is important to offer USPD as an option, and therefore, we must increase fellow comfortability. This may be through a variety of methods, including awareness, didactics, and hands-on practice. Even among comfortable providers, USPD use is limited by logistical barriers, including urgent placement of PD catheters [48]. While it has been previously stated that nephrology fellows have limited experience placing PD catheters, general surgery fellows feel similarly [48]. The most commonly cited reason for the inadequate training of PD catheters by general surgery trainees was inadequate referrals [48]. Obtaining hands-on practice for managing USPD patients remains a catch-22, as providers are less comfortable and therefore less likely to prescribe USPD, leading to fewer opportunities to place catheters, creating a vicious cycle. In order to offer USPD to candidate patients, there must be a significant effort to increase training among both nephrology fellow and surgery residents.
4.3. Patient Education
Patient education is critical for informed dialysis modality selection and to ensure alignment with patient goals and values. Given that up to 60% of patients crash onto dialysis [6], many must make this life-altering decision in a short timeframe. To effectively inform patients of options, strong educational interventions are required. Among the literature reviewed, some investigated the impact of educational interventions on modality choice. In one prospective, multinational study in Europe, investigators compared patients who received an educational intervention prior to choosing an acute start dialysis modality. After education, 58% chose USPD and participation in the educational program predicted choosing PD [52]. In a German study of 336 patients, PD use increased by 66% with education [53], with male gender and young age being predictive of PD choice. A review noted that among acute start dialysis patients, 21–58% of patients chose PD dialysis after three to five nurse-driven educational sessions [54]. While the authors noted this was similar to the planned dialysis population in the UK, it is significantly higher than the US population [1]. While three to five educational sessions may be unrealistic for some centers, even a single, 1 h education session on modality choice may increase PD initiation [55]. Together, these data suggest that patients may choose PD at higher rates when fully educated. To ensure informed decision making, centers should perform education prior to modality choice. Increased institutional commitment to patient education may increase the diffusion of PD and reduce the number of patients starting urgently.
4.4. Clinical Pathways and Protocols for USPD Initiation and Follow-Up
Due to the significant collaboration and resulting challenges of initiating a USPD program, there is interest in the specific protocols used. Multiple centers have reported on their individual protocols and experiences, providing examples for other centers to potentially implement. Javaid et al. provide excellent examples of their initial experience and sustained success with USPD implementation [49,51]. This center performed a root cause analysis which identified three main barriers to USPD implementation: variation in PD patient selection criteria, unavailability of catheter placement, and lack of a coordinated program. The key to addressing these challenges was hiring a dedicated PD coordinator and ensuring staffing of nephrologists able to place PD catheters [49]. Adequate other staffing was identified, and a dedicated PD initiation clinic was created with nephrologists interested in PD and the PD coordinator to handle logistics. An outpatient center was formed to administer low-volume, supine PD for the first two weeks. Additionally, the authors created a standardized questionnaire for PD eligibility to combat practice variation. Since the creation of this program, the proportion of patients initiating PD per year has increased by 30% and the total number of patients on PD has increased by 25%. At Louisiana State University, Jaikishen et al. report on their experience initiating the program. Prior to initiating, significant education of the staff occurred, beginning with grand rounds [56]. In a stepwise manner, different specialties were educated, beginning with primary care services. Because placing PD catheters is a barrier to implementation, and surgeons were educated on the program and involved in the discussion prior to initiation. Surgeons then participated in a program where a direct feedback loop was created between surgery, nephrology, and PD nurses [56]. This center provides an excellent example of educational practices and inter-specialty coordination prior to initiation of the program. The COVID-19 pandemic provided a unique challenge to dialysis, forcing hospitals to find alternative methods and new ways to urgently dialyze patients. Certain New York hospitals were able to rapidly initiate USPD programs by rapidly addressing barriers. For example, one hospital previously strictly used surgeons to place catheters, but expanded use to include interventional radiology for non-ICU patients to meet the demand for USPD [57]. A separate hospital used experienced personnel to educate staff to meet demands, resulting in approximately 20% of patients receiving dialysis being initiated on USPD [58]. These reports provide evidence of a hospital system’s ability to rapidly implement USPD programs when there is a clinical or logistical need.
4.5. Evidence Gaps and Areas for Future Research
As previously stated, a lack of clear terminology has plagued the field of USPD. Because quite different patient populations are all termed “urgent start peritoneal dialysis”, there is difficulty in comparing groups. The inability to adequately compare groups has led to low confidence data, hindering the advancement of USPD as a technique. While Blake et al.’s call for uniformity of terminology made some progress, it appears insufficient. The authors of this review believe the term “urgent start peritoneal dialysis” has been used so variably that new terms are necessary. We propose “emergent start peritoneal dialysis” be used to indicate patients initiating within 72 h, and “early start peritoneal dialysis” be used to indicate patients beginning between 72 h and 14 days. We believe this highlights the differences in these populations and provides concrete terminology that has not been used to refer to a different population. However, we believe leaders of the field should draft a unified statement proposing specific terminology to maximize adoption, as previous author’s proposals have not been fully adopted.
Another challenge within the field appears to be the logistical implementation of USPD. While specific centers have reported their experience, there is currently minimal generalizable data for the field to draw on in implementation at new centers. Successful implementation has required the onboarding of support personnel, hiring of physicians with specific skills, and creation of new clinics. Due to upfront financial investment, administrators may be hesitant to agree, even though maintenance PD has been shown to decrease costs. Reports of program costs may be persuasive to health systems. Finally, there still appears to be disagreement among the optimal initial dialysis prescription. Some evidence in this review suggested that APD-CAPD may be beneficial, but the evidence is preliminary. Furthermore, some authors suggest low-volume, supine PD, but this is not universally promoted. More definitive protocols would be beneficial, especially to new centers with limited experience.
5. Conclusions
In summary, USPD is a viable modality for patients who require initiation within 14 days. Given the potential patient and societal benefits of PD, increasing its use in the urgent setting may allow more patients to utilize the modality for maintenance. High rates of unplanned dialysis and continued use of the in-hospital form of dialysis in the outpatient setting suggest that increasing USPD may increase outpatient PD. Current literature suggests that the various methods of PD catheter insertion result in similar outcomes, so centers should individualize their workflow based on available resources. Mechanical complications may occur at greater rates in USPD dialysis compared to conventional start, but it is often treated conservatively and does not impact technique survival. Infectious complications in urgent-start peritoneal dialysis additionally appear similar to conventional-start PD. USPD appears to result in lower rates of dialysis-related complications and bacteremia but has an unclear impact on mortality. A significant challenge in USPD is implementation, especially with the implantation of catheters. Educational interventions among clinicians and patients play an important role in USPD. Further defining generalizable urgent-start protocols may help clinicians. Of great importance is the need for uniform terminology in USPD, as the patient population that requires treatment to be started within 72 h is much different to those who require initiation within 14 days. Our review concludes that “emergent start peritoneal dialysis” should be used for starts within 72 h, and early start used for those within 14 days. However, a statement from unified peritoneal dialysis leaders may be required before implementation occurs.
Author Contributions
Conceptualization, B.V. and A.D.S.; investigation, B.V. and A.D.S.; writing—original draft preparation, B.V. and A.D.S.; writing—review and editing, B.V. and A.D.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
B.V. declares no conflicts of interest. A.S. declares: Consulting—Otsuka, CareDx; Research Funding—Lifespan; Honoraria—JSOM (Japanese Society of Obstetric Medicine), University of South Carolina-Greenville, Care Transformation Collaborative RI. None of these declarations were involved in the creation of this manuscript.
Appendix A

{kind=link}
{kind=link}
Table A1.
Reviewed publications illustrating heterogeneity in terminology and definition of urgent-start peritoneal dialysis.
Table A1.
Reviewed publications illustrating heterogeneity in terminology and definition of urgent-start peritoneal dialysis.
| Publication | Terminology Used | Definition |
|---|---|---|
| Bittencourt, 2017 [27] | Early-start PD | PD started within 3 days |
| Kim, 2018 [18] | Urgent-start PD | Within 14 Days |
| Blake, 2018 [11] | Early-start PD and urgent-start PD | Review proposing uniform terminology: early start = within 3 days; urgent start = within 14 days |
| Sharma, 2020 [59] | Urgent Initiated PD | PD started within 3 days |
| Hu, 2022 [27] | Urgent-start PD | Within 3 days or within 14 days |
| Ng, 2022 [12] | Urgent-start PD and early-start PD | Urgent start = within 48–72 h; early start = within 14 days |
| Pilatti, 2022 [36] | Urgent-start PD | PD started within 7 days |
References
- United States Renal Data System. 2022 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2022. [Google Scholar]
- Chuasuwan, A.; Pooripussarakul, S.; Thakkinstian, A.; Ingsathit, A.; Pattanaprateep, O. Comparisons of quality of life between patients underwent peritoneal dialysis and hemodialysis: A systematic review and meta-analysis. Health Qual. Life Outcomes 2020, 18, 191. [Google Scholar] [CrossRef] [PubMed]
- Vogt, B.; Painter, D.F.; Saad Berreta, R.; Lokhande, A.; Shah, A.D. Hospitalization in maintenance peritoneal dialysis: A review. Hosp. Pract. 2023, 51, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.X.; Gao, X.; Inglese, G.; Chuengsaman, P.; Pecoits-Filho, R.; Yu, A. A Global Overview of the Impact of Peritoneal Dialysis First or Favored Policies: An Opinion. Perit. Dial. Int. 2015, 35, 406–420. [Google Scholar] [CrossRef] [PubMed]
- Briggs, V.; Davies, S.; Wilkie, M. International Variations in Peritoneal Dialysis Utilization and Implications for Practice. Am. J. Kidney Dis. 2019, 74, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Radhakrishnan, J.; Remuzzi, G.; Saran, R.; Williams, D.E.; Rios-Burrows, N.; Powe, N.; CDC-CKD Surveillance for the CDC-CKD Surveillance Team; Brück, K.; Wanner, C.; Stel, V.S.; et al. Taming the chronic kidney disease epidemic: A global view of surveillance efforts. Kidney Int. 2014, 86, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Rajora, N.; Shastri, S.; Pirwani, G.; Saxena, R. How To Build a Successful Urgent-Start Peritoneal Dialysis Program. Kidney360 2020, 1, 1165–1177. [Google Scholar] [CrossRef] [PubMed]
- Ghaffari, A.; Kumar, V.; Guest, S. Infrastructure requirements for an urgent-start peritoneal dialysis program. Perit. Dial. Int. 2013, 33, 611–617. [Google Scholar] [CrossRef]
- Teitelbaum, I. Peritoneal Dialysis. N. Engl. J. Med. 2021, 385, 1786–1795. [Google Scholar] [CrossRef]
- Rosner, M.H. Peritoneal Dialysis Should Be Considered the First Option for Patients Requiring Urgent Start Dialysis: COMMENTARY. Kidney360 2023, 4, 141–142. [Google Scholar] [CrossRef]
- Blake, P.G.; Jain, A.K. Urgent Start Peritoneal Dialysis: Defining What It Is and Why It Matters. Clin. J. Am. Soc. Nephrol. CJASN 2018, 13, 1278–1279. [Google Scholar] [CrossRef]
- Ng, A.K.H.; Tan, S.N.; Tay, M.E.; Van Der Straaten, J.C.; Cremere, G.; Chionh, C.Y. Comparison of planned-start, early-start and deferred-start strategies for peritoneal dialysis initiation in end-stage kidney disease. Ann. Acad. Med. Singap. 2022, 51, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Aal, A.K.; Dybbro, P.; Hathaway, P.; Guest, S.; Neuwirth, M.; Krishnamurthy, V. Best practices consensus protocol for peritoneal dialysis catheter placement by interventional radiologists. Perit. Dial. Int. 2014, 34, 481–493. [Google Scholar] [CrossRef] [PubMed]
- Abdel Aal, A.K.; Mahmoud, K.; Moustafa, A.S.; Aboueldahab, N.A.; Souid, A.; Gunn, A.; Li, Y.; Wang, Z.; Almehmi, A. Comparative Study on the Outcomes of Elective-Start versus Urgent-Start Peritoneal Dialysis Catheter Placement. Radiol. Res. Pract. 2020, 2020, 3751827. [Google Scholar] [CrossRef]
- Javaid, M.M.; Khan, B.A.; Subramanian, S. Is surgical PD catheter insertion safe for urgent-start peritoneal dialysis? Semin. Dial. 2019, 32, 225–228. [Google Scholar] [CrossRef]
- Scalamogna, A.; Nardelli, L.; Zanoni, F.; Messa, P. Double purse-string around the inner cuff of the peritoneal catheter: A novel technique for an immediate initiation of continuous peritoneal dialysis. Int. J. Artif. Organs 2020, 43, 365–371. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, M.J.; Ye, B.M.; Kim, J.H.; Kim, S.; Kim, I.Y.; Kim, H.J.; Han, M.; Rhee, H.; Song, S.H.; et al. Percutaneous peritoneal dialysis catheter implantation with no break-in period: A viable option for patients requiring unplanned urgent-start peritoneal dialysis. Kidney Res. Clin. Pract. 2020, 39, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Son, Y.K.; Lee, S.M.; Kim, S.E.; An, W.S. Early technical complications and long-term survival of urgent peritoneal dialysis according to break-in periods. PLoS ONE 2018, 13, e0206426. [Google Scholar] [CrossRef]
- Htay, H.; Johnson, D.W.; Craig, J.C.; Schena, F.P.; Strippoli, G.F.; Tong, A.; Cho, Y. Catheter type, placement and insertion techniques for preventing catheter-related infections in chronic peritoneal dialysis patients. Cochrane Database Syst. Rev. 2019, 5, Cd004680. [Google Scholar] [CrossRef]
- Wang, C.; Fu, X.; Yang, Y.; Deng, J.; Lu, J.; Peng, Y.; Liu, Y.; Zhang, H.-Q.; Deng, H.-M.; Liu, H.; et al. A Comparison between Intermittent Peritoneal Dialysis and Automatic Peritoneal Dialysis on Urgent Peritoneal Dialysis. Am. J. Nephrol. 2017, 45, 540–548. [Google Scholar] [CrossRef]
- Xia, X.; He, X.; Pu, L.; Liu, X.; Zhou, X.; Wu, X.F.; Zang, Z.; Li, Z. A randomized controlled comparative study of different fluid exchange modes in urgent-start peritoneal dialysis in patients with end-stage renal disease: Automated peritoneal dialysis combined with manual fluid exchange vs. manual fluid exchange alone. Ren. Fail. 2023, 45, 2202756. [Google Scholar] [CrossRef]
- Liu, S.; Zhuang, X.; Zhang, M.; Wu, Y.; Liu, M.; Guan, S.; Liu, S.; Miao, L.; Cui, W. Application of automated peritoneal dialysis in urgent-start peritoneal dialysis patients during the break-in period. Int. Urol. Nephrol. 2018, 50, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Javaid, M.M.; Khan, B.A.; Subramanian, S. The modality of choice, manual or automated, for urgent start peritoneal dialysis. Clin. Kidney J. 2019, 12, 443–446. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.; Wang, H.; Li, S.; Zuo, Y.; Wang, Y.; Zhang, Y.; Liang, T.; Li, J.; Wang, L.; Feng, Z.; et al. Low-Volume Tidal Peritoneal Dialysis Is a Preferable Mode in Patients Initiating Urgent-Start Automated Peritoneal Dialysis: A Randomized, Open-Label, Prospective Control Study. Ther. Apher. Dial. 2019, 23, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Scalamogna, A.; Nardelli, L.; Cicero, E.; Castellano, G. Analysis of mechanical complications in urgent-start peritoneal dialysis. J. Nephrol. 2022, 35, 1489–1496. [Google Scholar] [CrossRef] [PubMed]
- See, E.J.; Cho, Y.; Hawley, C.M.; Jaffrey, L.R.; Johnson, D.W. Early and Late Patient Outcomes in Urgent-Start Peritoneal Dialysis. Perit. Dial. Int. 2017, 37, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Yang, L.; Sun, Z.; Zhang, X.; Zhu, X.; Zhou, W.; Wen, X.; Liu, S.; Cui, W. Break-in Period ≤ 24 Hours as an Option for Urgent-start Peritoneal Dialysis in Patients with Diabetes. Frontiers in endocrinology. 2022, 13, 93657. [Google Scholar] [CrossRef] [PubMed]
- Ye, H.; Yang, X.; Yi, C.; Guo, Q.; Li, Y.; Yang, Q.; Chen, W.; Mao, H.; Li, J.; Qiu, Y.; et al. Urgent-start peritoneal dialysis for patients with end stage renal disease: A 10-year retrospective study. BMC Nephrol. 2019, 20, 238. [Google Scholar] [CrossRef]
- Abrantes, A.R.M.; Gonçalves, H.; Ferrer, F.A.D.; Lobos, A.M.V. Urgent start peritoneal dialysis: Is there room for more? Nefrologia 2021, 41, 573–577. [Google Scholar] [CrossRef]
- Dias, D.B.; Mendes, M.L.; Caramori, J.T.; Falbo dos Reis, P.; Ponce, D. Urgent-start dialysis: Comparison of complications and outcomes between peritoneal dialysis and haemodialysis. Perit. Dial. Int. 2021, 41, 244–252. [Google Scholar] [CrossRef]
- Wojtaszek, E.; Grzejszczak, A.; Grygiel, K.; Małyszko, J.; Matuszkiewicz-Rowińska, J. Urgent-Start Peritoneal Dialysis as a Bridge to Definitive Chronic Renal Replacement Therapy: Short- and Long-Term Outcomes. Front. Physiol. 2019, 9, 1830. [Google Scholar] [CrossRef]
- Phang, C.C.; Foo, M.W.Y.; Johnson, D.W.; Wu, S.Y.; Hao, Y.; Jayaballa, M.; Koniman, R.; Chan, C.M.; Oei, E.L.; Chong, T.T.; et al. Comparison of outcomes of urgent-start and conventional-start peritoneal dialysis: A single-centre experience. Int. Urol. Nephrol. 2021, 53, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Müller, J.V.C.; Ponce, D. Infectious and mechanical complications in planned-start vs. urgent-start peritoneal dialysis: A cohort study. Braz. J. Nephrol. 2023, 45, 27–35. [Google Scholar] [CrossRef]
- Nayak, K.S.; Subhramanyam, S.V.; Pavankumar, N.; Antony, S.; Sarfaraz Khan, M.A. Emergent Start Peritoneal Dialysis for End-Stage Renal Disease: Outcomes and Advantages. Blood Purif. 2018, 45, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Wen, X.; Yang, L.; Sun, Z.; Zhang, X.; Zhu, X.; Zhou, W.; Hu, X.; Liu, S.; Luo, P.; Cui, W. Feasibility of a break-in period of less than 24 hours for urgent start peritoneal dialysis: A multicenter study. Ren. Fail. 2022, 44, 450–460. [Google Scholar] [CrossRef] [PubMed]
- Pilatti, M.; Theodorovitz, V.C.; Hille, D.; Sevignani, G.; Ferreira, H.C.; Vieira, M.A.; Calice-Silva, V.; de França, P.H.C. Urgent vs. planned peritoneal dialysis initiation: Complications and outcomes in the first year of therapy. Braz. J. Nephrol. 2022, 44, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Bitencourt Dias, D.; Mendes, M.L.; Burgugi Banin, V.; Barretti, P.; Ponce, D. Urgent-Start Peritoneal Dialysis: The First Year of Brazilian Experience. Blood Purif. 2017, 44, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Bhalla, N.M.; Arora, N.; Darbinian, J.A.; Zheng, S. Urgent Start Peritoneal Dialysis: A Population-Based Cohort Study. Kidney Med. 2022, 4, 100414. [Google Scholar] [CrossRef]
- Koch, M.; Kohnle, M.; Trapp, R.; Haastert, B.; Rump, L.C.; Aker, S. Comparable outcome of acute unplanned peritoneal dialysis and haemodialysis. Nephrol. Dial. Transplant. 2012, 27, 375–380. [Google Scholar] [CrossRef]
- Jin, H.; Fang, W.; Zhu, M.; Yu, Z.; Fang, Y.; Yan, H.; Zhang, M.; Wang, Q.; Che, X.; Xie, Y.; et al. Urgent-Start Peritoneal Dialysis and Hemodialysis in ESRD Patients: Complications and Outcomes. PLoS ONE 2016, 11, e0166181. [Google Scholar] [CrossRef]
- Htay, H.; Johnson, D.W.; Craig, J.C.; Teixeira-Pinto, A.; Hawley, C.M.; Cho, Y. Urgent-start peritoneal dialysis versus haemodialysis for people with chronic kidney disease. Cochrane Database Syst. Rev. 2021, 2021, CD012899. [Google Scholar] [CrossRef]
- Jin, H.; Ni, Z.; Mou, S.; Lu, R.; Fang, W.; Huang, J.; Hu, C.; Zhang, H.; Yan, H.; Li, Z.; et al. Feasibility of Urgent-Start Peritoneal Dialysis in Older Patients with End-Stage Renal Disease: A Single-Center Experience. Perit. Dial. Int. 2018, 38, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Zang, X.; Du, X.; Li, L.; Mei, C. Complications and outcomes of urgent-start peritoneal dialysis in elderly patients with end-stage renal disease in China: A retrospective cohort study. BMJ Open 2020, 10, e032849. [Google Scholar] [CrossRef] [PubMed]
- Parapiboon, W.; Sangsuk, J.; Nopsopon, T.; Pitsawong, W.; Tatiyanupanwong, S.; Kanjanabuch, T.; Johnson, D.W. Randomized Study of Urgent-Start Peritoneal Dialysis Versus Urgent-Start Temporary Hemodialysis in Patients Transitioning to Kidney Failure. Kidney Int. Rep. 2022, 7, 1866–1877. [Google Scholar] [CrossRef] [PubMed]
- Jin, H.; Ni, Z.; Che, X.; Gu, L.; Zhu, M.; Yuan, J.; Huang, J.; Gu, A.; Jin, Y.; Yan, H.; et al. Peritoneal Dialysis as an Option for Unplanned Dialysis Initiation in Patients with End-Stage Renal Disease and Diabetes Mellitus. Blood Purif. 2019, 47, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.X.; Ghaffari, A.; Dhatt, H.; Kumar, V.; Balsera, C.; Wallace, E.; Khairullah, Q.; Lesher, B.; Gao, X.; Henderson, H.; et al. Economic evaluation of urgent-start peritoneal dialysis versus urgent-start hemodialysis in the United States. Medicine 2014, 93, e293. [Google Scholar] [CrossRef] [PubMed]
- Jin, H.; Lu, R.; Lv, S.; Wang, L.; Mou, S.; Zhang, M.; Wang, Q.; Pang, H.; Yan, H.; Li, Z.; et al. Automated peritoneal dialysis as a cost-effective urgent-start dialysis option for ESRD patients: A prospective cohort study. Int. J. Artif. Organs 2022, 45, 672–679. [Google Scholar] [CrossRef] [PubMed]
- Dean, D.; Cruz, D.N. We Use Permcaths Instead of Peritoneal Catheters for Acute Kidney Injury and Urgent-Start Dialysis. Semin. Dial. 2016, 29, 260–262. [Google Scholar] [CrossRef]
- Javaid, M.M.; Khan, B.A.; Yeo, E.X.; Teo, B.W.; Subramanian, S. Sustained Increase in Peritoneal Dialysis Prevalence through a Structured PD Initiation Service. Perit. Dial. Int. 2018, 38, 374–376. [Google Scholar] [CrossRef]
- Gupta, N.; Taber-Hight, E.B.; Miller, B.W. Perceptions of Home Dialysis Training and Experience Among US Nephrology Fellows. Am. J. Kidney Dis. 2021, 77, 713–718.e1. [Google Scholar] [CrossRef]
- Javaid, M.M.; Lee, E.; Khan, B.A.; Subramanian, S. Description of an Urgent-Start Peritoneal Dialysis Program in Singapore. Perit. Dial. Int. 2017, 37, 500–502. [Google Scholar] [CrossRef]
- Machowska, A.; Alscher, M.D.; Vanga, S.R.; Koch, M.; Aarup, M.; Qureshi, A.R.; Lindholm, B.; Rutherford, P. Offering Patients Therapy Options in Unplanned Start (OPTiONS): Implementation of an educational program is feasible and effective. BMC Nephrol. 2017, 18, 18. [Google Scholar] [CrossRef] [PubMed]
- Schanz, M.; Ketteler, M.; Heck, M.; Dippon, J.; Alscher, M.D.; Kimmel, M. Impact of an in-Hospital Patient Education Program on Choice of Renal Replacement Modality in Unplanned Dialysis Initiation. Kidney Blood Press. Res. 2017, 42, 865–876. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Baharani, J. Dialysis education and options for late presenters—An ongoing dilemma. Hemodial. Int. 2023, 27, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Sakurada, T.; Koitabashi, K.; Murasawa, M.; Kohatsu, K.; Kojima, S.; Shibagaki, Y. Effects of one-hour discussion on the choice of dialysis modality at the outpatient clinic: A retrospective cohort study using propensity score matching. Ther. Apher. Dial. 2023, 27, 442–451. [Google Scholar] [CrossRef] [PubMed]
- Jaikishen, A.; Lick, A.; Owen, J.G.; Naljayan, M.V. Louisiana State University Nephrology: Initiation of a Multicenter Urgent-Start Peritoneal Dialysis Program. Adv. Perit. Dial. 2016, 32, 11–14. [Google Scholar] [PubMed]
- Sourial, M.Y.; Sourial, M.H.; Dalsan, R.; Graham, J.; Ross, M.; Chen, W.; Golestaneh, L. Urgent Peritoneal Dialysis in Patients With COVID-19 and Acute Kidney Injury: A Single-Center Experience in a Time of Crisis in the United States. Am. J. Kidney 2020, 76, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Akomeah, J.; Apostol, A.; Barnes, E.; Charytan, C.; Enriquez, U.; Katikaneni, M.; Liu, F.; Messina, A.; Neelakantappa, K.; Radhakrishnan, J.; et al. Optimizing Kidney Replacement Therapy During the COVID-19 Pandemic Across a Complex Healthcare System. Front. Med. 2020, 7, 604182. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Parry, M.; Alam, S.; Mahanta, P.; Doley, P.; Mazumder, M.A.; Jeelani, H.; Dange, S. A Comparable Study on the Outcomes of Urgent Initiated Peritoneal Dialysis Versus Conventional Start, A Single Centre Study from North-East India. Iran J. Kidney Dis. 2020, 14, 488–493. [Google Scholar]
Figure 1.
Rethinking Dialysis in the Urgent-Start Patient: Many patients elect for peritoneal dialysis in the outpatient setting but begin in an unplanned manner, often eventually receiving hemodialysis instead. Urgent-start peritoneal dialysis remains an understudied option to allow some of these patients to receive peritoneal dialysis in the outpatient setting. However, many clinical questions remain unanswered, including timing of initiation, terminology, and complications rates, such as infection and mechanical complications. Figure created with BioRender.com.
Figure 1.
Rethinking Dialysis in the Urgent-Start Patient: Many patients elect for peritoneal dialysis in the outpatient setting but begin in an unplanned manner, often eventually receiving hemodialysis instead. Urgent-start peritoneal dialysis remains an understudied option to allow some of these patients to receive peritoneal dialysis in the outpatient setting. However, many clinical questions remain unanswered, including timing of initiation, terminology, and complications rates, such as infection and mechanical complications. Figure created with BioRender.com.

Figure 2.
Summary of interconnected barriers to urgent-start peritoneal dialysis implementation.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Vogt, B.; Shah, A.D. Urgent-Start Peritoneal Dialysis: Current State and Future Directions. Kidney Dial. 2024, 4, 15-26. https://doi.org/10.3390/kidneydial4010002
AMA Style
Vogt B, Shah AD. Urgent-Start Peritoneal Dialysis: Current State and Future Directions. Kidney and Dialysis. 2024; 4(1):15-26. https://doi.org/10.3390/kidneydial4010002
Chicago/Turabian StyleVogt, Braden, and Ankur D. Shah. 2024. "Urgent-Start Peritoneal Dialysis: Current State and Future Directions" Kidney and Dialysis 4, no. 1: 15-26. https://doi.org/10.3390/kidneydial4010002