
An Update on Hypomagnesemia and Hypermagnesemia

Renal Division, Department of Internal Medicine and Pediatrics, Ghent University Hospital, 9000 Ghent, Belgium
Kidney Dial. 2024, 4(1), 1-14; https://doi.org/10.3390/kidneydial4010001
Submission received: 4 September 2023
/
Revised: 28 October 2023
/
Accepted: 1 November 2023
/
Published: 24 December 2023
Abstract
:Magnesium is an essential element with a pleiotropic role in human biology. Despite tight intestinal and renal regulation of its balance, insufficient intake can finally result in hypomagnesemia, which is a proxy of intracellular deficiency. Conditions such as diabetes, cancer, and infections are often associated with hypomagnesemia, which mostly predicts an unfavorable outcome. The effects of hypomagnesemia can either be direct and include neurological and cardiovascular symptoms or indirect, taking a mechanistic role in inflammation, endothelial dysfunction, and oxidative stress. The indication for intravenous magnesium as a treatment of torsades de pointes and pre-eclampsia is unrefuted, but new indications of peroral or intravenous supplementation, albeit with less supporting evidence, have emerged suggesting, respectively, an attenuation of vascular calcification in chronic kidney disease and improved rate control in atrial fibrillation. Other potential beneficial properties of magnesium, which were claimed by observational data, such as lipid lowering and renal protection, were not, or only partially, investigated in randomized controlled trials. Thus, the role of peroral supplementation of mild chronic asymptomatic hypomagnesemia should be separated from the more targeted prescription of magnesium in specific study populations. (Severe) hypermagnesemia is potentially life-threatening and occurs almost uniformly in subjects with severe renal failure exposed to either supplements or to magnesium-containing cathartics or antacids. Moderate hypermagnesemia is very common in pre-eclamptic women treated with intravenous magnesium. For most (but not all) studied endpoints, mild hypermagnesemia yields a survival benefit. Long-lasting concerns about the potential negative effects of mild hypermagnesemia on bone physiology and structure have so far not been unequivocally demonstrated to be troublesome.
1. Introduction
Magnesium is the second most abundant intracellular cation, which acts as a cofactor of >600 enzymes in human biology. It is therefore involved in many essential cellular processes, which include glycolysis, oxidative phosphorylation, transmembrane ion transport, signal transduction, and protein and deoxyribonucleic acid (DNA) synthesis and polymerization [1,2]. Almost the entire magnesium content of the body (25 g) is located in bone (60%), where it is incorporated into hydroxyapatite and, to a lesser degree, in soft tissue (38%), lessening its exchangeability. The small extracellular magnesium fraction is protein-bound (20–30%) and complexed to anions, including bicarbonate, citrate, sulfate, or phosphate (5–15%) [1,2]. Of the serum fraction of magnesium, more than half (55–70%) is ionized and thus biologically active.
The increased interest in magnesium is illustrated by an exponential rise in publications during the last decade. This is largely driven by accumulating evidence of a potential role of hypomagnesemia (mild if serum Mg < 0.7 mM and severe if serum Mg < 0.4 mM) or, more accurately, magnesium depletion in the development of cardiovascular disease [2,3]. Also, the list of etiologies of magnesium deficiency is still expanding. Novel hereditary causes of hypomagnesemia are being deciphered in tight conjunction with the exploration of the various pathways of renal tubular magnesium transport [4,5]. The causal role of commonly used drugs such as proton pump inhibitors or, more rarely, cetuximab (monoclonal antibodies against epidermal growth factor receptor) adds to the increasing list of drugs associated with decreased magnesium absorption or enhanced urinary loss. At least as important from a general population perspective is an observed deficient magnesium intake, not only in adults but also in adolescents following a high consumption of refined food with simultaneous insufficient intake of whole grains and of green leafy vegetables, with magnesium being a constituent of chlorophyll [6,7,8]. In vitro data and a relatively low number of clinical trials performed so far hinted at a beneficial effect of magnesium supplementation on intermediate endpoints such as endothelial dysfunction, telomere shortening as a proxy of aging, intima media thickness, and vascular calcification in chronic kidney disease (CKD) patients [2,9,10,11,12,13]. Low magnesium intake and/or hypomagnesemia is associated with poor outcomes, especially due to cardiovascular events and heart failure or with mortality in diabetes next to sarcopenia, acute kidney injury, CKD progression, hypertension, diabetes, infections, cerebrovascular disease including stroke, cancer, osteoporosis, and fractures [14,15,16,17,18,19,20,21,22,23,24,25,26]. Observational cohort studies remain, however, very prone to selection bias since high magnesium intake reflects a healthier lifestyle, less sedentarism, more leanness, and so on. Also, questions concerning the ideal magnesium formulation and the role of Sodium-Glucose Transport Protein-2 (SGLT2) inhibitors in the therapeutic approach of hypomagnesemia are still unanswered [27]. Finally, the significance of hypermagnesemia (mild if serum Mg > 1.2 mM and severe if serum Mg > 1.9 mM) remains more enigmatic: a more favorable outcome is commonly reported for mild hypermagnesemia although U-shaped curves have also been described for outcomes such as cancer or mortality [2,28,29,30]. And so, many questions concerning the biological relevance of altered magnesium status until now remain unanswered.
2. Hypomagnesemia
2.1. Pathophysiology
About 80 to 90% of the daily food intake of magnesium is absorbed via non-saturable paracellular concentration-driven passive uptake, especially in the jejunum and, to a lesser degree, the colon [1]. The potentially saturable active transcellular transport is restricted and occurs across the colonic channels transient receptor of melastatin (TRPM) 6 and 7 [1]. Both hypomagnesemia by itself and active vitamin D promote intestinal magnesium absorption, which can be upregulated from 40 to about 80% in case of magnesium deficiency. Most of the filtered magnesium load in the kidney is reabsorbed in the thick ascending limb (TAL) of Henle (70%) across an electrochemical gradient via the tight junction channels claudin-16 and -19 [1]. Next to hypervolemia, hypermagnesemia and hypercalcemia also inhibit the renal magnesium absorption at the level of the TAL of Henle via stimulation of the calcium-sensing receptor (CaSR), while hyperparathyroidism increases the renal magnesium absorption [31,32]. The remainder of the tubular absorption occurs in the proximal tubule (10–25%), while the distal convoluted tubule (DCT) is responsible for the regulation of the final urinary magnesium output via the adaptation of active absorption via TRMP6 [1]. In magnesium deficiency or hypomagnesemia, the fractional urinary magnesium excretion can be adapted and can decrease to as low as 0.5%. The dysregulation of this delicate balance of renal tubular magnesium homeostasis can trigger hypomagnesemia. Drugs interfering with intestinal and/or renal magnesium absorption can accordingly play a causal role, whereby some drugs such as epidermal growth factor receptor (EGFR) inhibitors cetuximab and cisplatinum downregulate the expression of TRPM6 in the DCT. In patients exposed to calcineurin inhibitors, and especially tacrolimus, a dose-dependent inhibition of TRPM6 expression at the level of the DCT leads to enhanced urinary magnesium wasting and mild to moderate hypomagnesemia in half of all kidney transplant recipients treated with tacrolimus [33]. In rodents, estrogens increase the expression of TRPM6 in the DCT, and ovariectomized rats have enhanced urinary magnesium loss, but the role of sex hormones in humans is largely unexplored [34]. PPI impairs intestinal magnesium absorption as a higher luminal pH decreases its solubility [35]. PPI, moreover, lowers the expression of claudin channels and increases the transepithelial electrical resistance in the small intestine [35]. In the colon, decreased activity of TRPM6 is partially driven by changes in microbiota [35]. These mechanisms explain why, in most studies, PPI users have a twofold risk of developing hypomagnesemia [35]. PPI-induced hypomagnesemia can be potentiated by concomitant intake of diuretics (loop diuretics and thiazides which, respectively, target the TAL and DCT segments) and lead to sporadically severe and potentially life-threatening hypomagnesemia [1,36]. Hypomagnesemia is not uncommon upon intake of resins but also of newer potassium binders such as patiromer, where it was reported in 7% of all patients [37,38]. Also, proteinuria results in renal magnesium wasting and is associated with refractoriness to correct hypomagnesemia by magnesium supplementation [39].
Gastrointestinal causes of hypomagnesemia are not uncommon and include deficient intake or intestinal malabsorption of magnesium with incomplete renal compensation. In this regard, determination of fractional urinary magnesium excretion on a morning voiding sample can demonstrate urinary magnesium wasting if >2%, but only in the setting of a normal kidney function. Magnesium deficiency can occur even with normal serum magnesium concentrations, which reflects the limitations of serum magnesium as a proxy of total body magnesium content. Some authors have claimed that the biologically active ionized serum magnesium fraction is a more specific marker of magnesium status and correlates better with blood pressure measurements and other clinical assessments [40]. Altogether, the clinical value of the measurable ionized magnesium fraction remains undefined, as reflected by its ongoing omission even from recent clinical trials [41,42,43,44]. A laborious intravenous magnesium tolerance test could theoretically aid in diagnosing magnesium deficiency despite normomagnesemia, provided the absence of renal magnesium wasting and/or renal dysfunction. Following this line of reasoning and considering the finding of unfavorable outcomes in patients with serum magnesium concentrations in the lower normal range, a generalized adaptation of the reference range for normal magnesium values has recently been proposed with an adaptation of the lower limit of the reference range from 0.75 mM to 0.85 mM [45].
2.2. Hereditary Etiologies of Hypomagnesemia
In the last decade, transgenic murine models and the identification of their disorders have provided valuable insights into the molecular mechanisms of renal magnesium absorption [5]. The spectrum of etiologies of hereditary magnesium wasting related to monogenic mutations yielding dysfunctional transporter proteins, is still expanding [1,4,46]. Phenotypic traits alluding to a genetic etiology and warranting advice from the geneticist apart from family history, are features like early-onset hypomagnesemia, dysmorphic characteristics, neurosensorial hearing loss, cognitive dysfunction, epilepsy, diabetes, nephrocalcinosis and biochemical features such as hypercalciuria, metabolic alkalosis, and hypokalemia. A de novo disturbance of renal magnesium handling due to pathogenic claudin-19 antibodies with ensuing severe hypomagnesemia was recently described in a patient with tubulointerstitial nephritis and acute kidney injury [47]. Gitelman syndrome is traditionally the most common hereditary etiology of magnesium wasting, explained by heterozygous mutations in the thiazide-sensitive Na+-Cl−cotransporter NCC (SLCC12A3) in the DCT [48].
More recently, however, mutations of other genes such as CKCNKB, KCNJ10, FXYD2, or HNF1B, which indirectly reduce NCC activity, can lead to the same clinical phenotype, explaining why the genotype in Gitelman syndrome is often unknown [49]. Also, four pathogenic variants in the mitochondrial genome leading to defective oxidative phosphorylation and hence NCC-mediated uptake were reported in 13 families with a Gitelman-like syndrome [50]. Gitelman syndrome was usually considered a benign condition despite the presence of hyperaldosteronism and hypomagnesemia. This premise has more recently been challenged by the confirmation of adverse metabolic and cardiovascular effects, including disturbed glucose metabolism, insulin resistance, and immunodeficiency due to impaired IL-17 response [51,52]. These findings highlight the active role of elements such as magnesium (and, to a lesser degree, potassium) in glucose metabolism and immunology. To conclude, the spectrum of hereditary etiologies of renal magnesium wasting is still expanding, while the clinical phenotype of its most archetypical example (Gitelman syndrome) has been recently redefined.
2.3. Hypomagnesemia and Glucose Metabolism
The relationship between (mild to moderate) hypomagnesemia and disturbed glucose metabolism, including diabetes mellitus, is quite well established with magnesium deficiency, which correlates inversely with glycemic control [53]. This relationship is, however, bidirectional. Both low dietary magnesium intake, hypomagnesemia, and single nucleotide polymorphisms in genes involved in cellular magnesium physiology, which influence serum magnesium concentration, predict the development of diabetes or prediabetes in the general population or in kidney transplant recipients [54,55,56]. Magnesium is an essential element for insulin secretion, which, moreover, increases the insulin-dependent glucose uptake in adipocytes, contributing to improved insulin sensitivity [57]. Conversely, insulin decreases the expression of TRPM6 in the DCT and hence promotes renal magnesium wasting, which is commonly observed in type 2 diabetes [54]. Improvement in insulin sensitivity by excessive weight loss after bariatric surgery not only improved glycemic control but also increased serum magnesium concentration, while chronic hypomagnesemia predicted the irreversibility of diabetes in these morbidly obese subjects [58]. Furthermore, hypomagnesemia in patients with diabetes has been associated not only with the occurrence of cardiac events such as heart failure but also with end-organ damage, including microvascular complications [14]. Of note, although exercise and sports improve insulin sensitivity, correction of hypomagnesemia may be offset by increased sweating and increased urinary magnesium excretion [59]. Sports competition can further enhance these processes, and marathon runners accordingly have a significant drop in their serum magnesium concentration, which lasts, on average, for three days after the run [60]. To summarize, the bidirectional relationship between hypomagnesemia and disturbed glucose metabolism is established and appears to be clinically relevant.
3. Symptoms
The variety of symptoms related to hypomagnesemia and their severity depend not only upon the degree of hypomagnesemia but also the (absence of) chronicity and the presence of concomitant electrolyte disturbances, including hypocalcemia and hypokalemia [61]. The majority of patients with moderate hypomagnesemia (0.5–0.65 mM) have chronic asymptomatic hypomagnesemia. Non-specific and therefore under-recognized symptoms are drowsiness and fatigue. Neuromuscular symptoms include the somewhat specific downbeat vertical nystagmus in severely hypomagnesiemic subjects in the absence of structural brain lesions [61]. The risk for choreiform movements, tetany, and seizures is amplified in patients with hypocalcemia [1,61]. Following severe hypomagnesemia (<0.5 mM), parathyroid hormone (PTH) hyposecretion and renal and skeletal resistance to PTH might aggravate hypocalcemia and ensuing neuromuscular symptoms [62]. Furthermore, magnesium deficiency impairs active vitamin D synthesis, which can contribute to the co-existence of both electrolyte abnormalities [61]. Hypomagnesemia, often in concordance with hypokalemia, has cardiotropic effects, including a lower threshold for cardiac arrhythmia, atrial fibrillation, supraventricular tachycardia, and, less commonly, ventricular fibrillation [62]. Hypomagnesemia can promote hypokalemia by inhibiting the transcellular tubular gradients generated across the renal outer medullary potassium (ROMK) channels, leading to renal potassium wasting and impairing the function of the cellular Na+-K+-ATPase [62,63]. The correction of hypokalemia should equally include treatment of concomitant hypomagnesemia. Correction of even asymptomatic hypomagnesemia should also be considered in patients with heart failure, especially when treated with digitalis or ischemic heart disease and liver cirrhosis.
3.1. Hypomagnesemia and Its Clinical Correlates
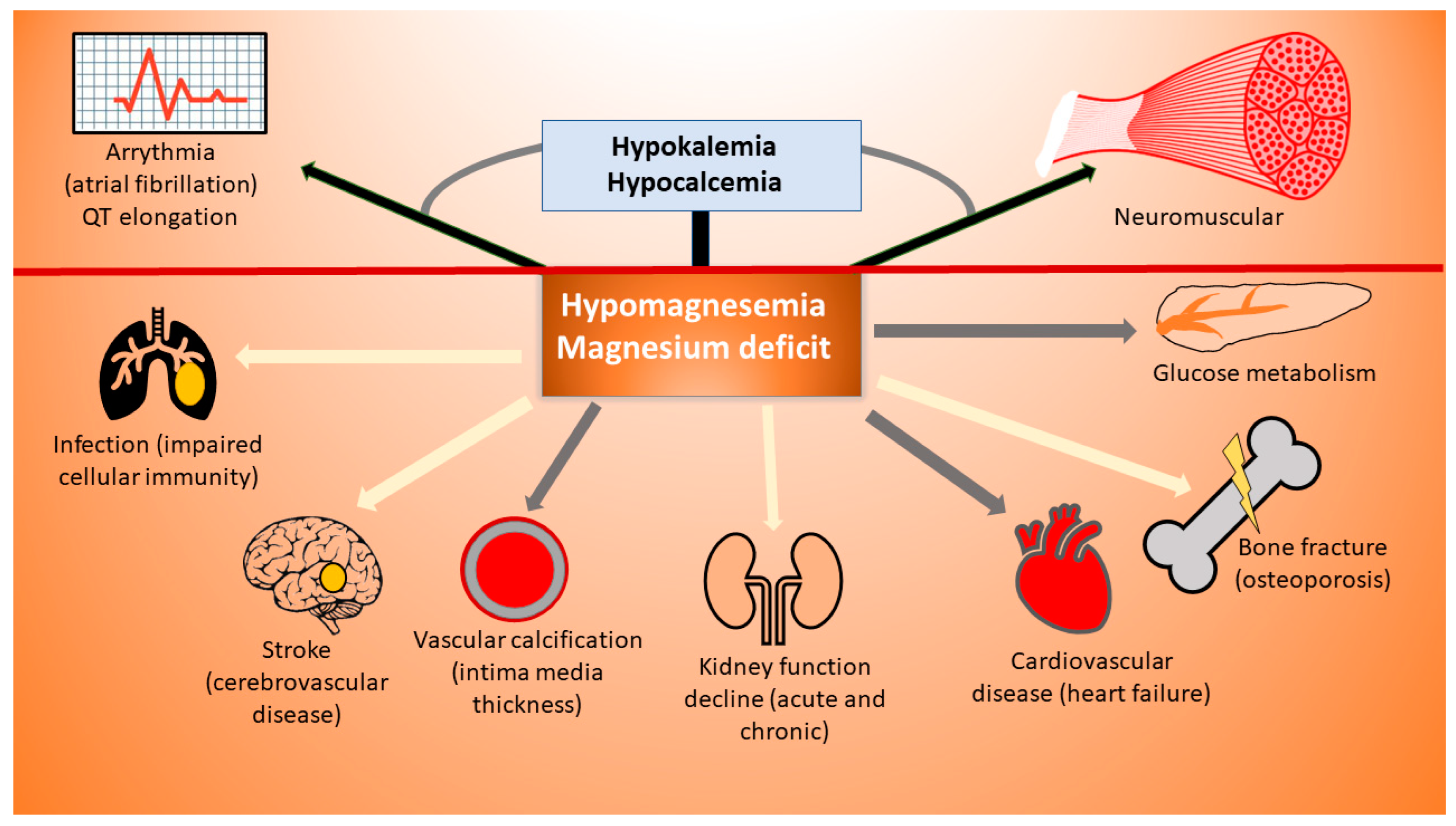
Meta-analyses of prospective studies in the general population pointed to a dismal cardiovascular outcome corresponding with hypomagnesemia [26]. An increased mortality risk was also observed in particular populations such as the elderly, people with variable degrees of CKD, kidney transplantation (KTR), and people with heart failure [29,30,64,65,66,67,68,69]. Hypomagnesemia also has immunotropic properties considering the extracellular magnesium regulation of the activity of CD8+ T-cells via their sensing co-stimulatory molecule LFA-1 and by increasing the cellular expression of activating NK receptors (NKG2D) [70,71]. A functional defect in MAGT1 transcellular receptors leads to the hereditary X-linked disease X-men disease, which is characterized by recurrent Epstein–Barr viremia (EBV) and a propensity to develop B-cell lymphoma [71]. The beneficial role of magnesium supplements, as described in the original paper, could, however, not be validated in a recent trial [72]. Hypomagnesemia was associated with increased infection risk and/or mortality in kidney transplant recipients and systemic lupus erythematodes (SLE) patients and higher mortality risk in patients with community-acquired pneumonia. Serum magnesium was also lower in children with increasing circulating Epstein–Barr Virus (EBV) levels and lymphoma [20,30,73,74,75,76]. Hypomagnesemia is also associated with the occurrence of cerebrovascular disease, including Alzheimer’s disease, while a higher serum magnesium concentration correlated with a higher brain volume and the absence of subclinical cerebrovascular disease according to data from the ARIC study [77,78]. Middle-aged patients with hypomagnesemia have a higher risk of hip fracture, in line with a meta-analysis demonstrating an increase in hip and femoral neck bone density with increasing magnesium intake in older people [22,79,80]. In patients admitted to the hospital and especially the intensive care unit (ICU), hypomagnesemia is associated with overall mortality [61,81,82]. Hypomagnesemia at admission has also been associated with a higher risk of valve dysfunction after transcatheter aortic valve implantation (TAVI) in hemodialysis patients [83]. Preoperative hypomagnesemia was also associated with acute kidney injury after cardiac surgery and has been associated with a faster decline in kidney function in many population-based observational studies, including a recent analysis from the CRIC cohort [18,19,84,85]. However, another observational study could not confirm this association between serum magnesium and decline in kidney function [69]. Although studies have demonstrated an association between not only hypomagnesemia but also lower dietary magnesium intake and faster decline in kidney function, we need to consider the risk of bias inherent to the design of these studies; so far, no clinical trials have been conducted to evaluate the nephroprotective properties of Mg supplementation [19,65,86,87]. Considering the risk of bias inherent to the design of these studies, the need to supplement magnesium in vulnerable populations should be ascertained by interventional studies. With variable success, beneficial effects were demonstrated on intermediate outcomes such as intima media thickness and endothelial function, although the lack of trials focusing on pre-defined hard cardiac endpoints has precluded its broad application in populations at risk of cardiovascular events [12]. To conclude, there is still a gap between broad evidence in support of a negative outcome related to hypomagnesemia and the clinical translation into targeted supplementation. The clinical spectrum of hypomagnesemia and magnesium deficiency is summarized in Figure 1.
3.2. When and How to Treat Hypomagnesemia?
A solid indication to treat hypomagnesemia is the presence of clinical symptoms and/or severe hypomagnesemia (<0.5 mM), which classically necessitates intravenous correction. The short-acting and thus transient effect of intravenous magnesium sulfate, of which half is renally excreted, should be taken into account as it temporarily abolishes the concentration gradient and hence the tubular magnesium reabsorption and can lead to hypotension and more sporadically hyperphosphatemia [62,88]. Oral magnesium supplements are used for the correction of mild to moderate chronic hypomagnesemia [62]. Meta-analyses of RCTs have demonstrated small but statistically significant effects on surrogate endpoints such as CRP and blood pressure [89]. Of relevance, some of the included participants in these trials were not hypomagnesemic and hence the value of magnesium supplementation in subjects with hypomagnesemia on classical cardiovascular risk factors remains ill-defined.
SGLT2 inhibitors could theoretically become an elegant option to treat patients with hypomagnesemia, especially in patients with diabetes mellitus, renal disease, and/or cardiovascular disease. The magnesiotropic effect of these drugs seems related to the increased renal expression of TRPM6/7 and Claudin-16 (TAL Henle), which led to an increment in serum magnesium concentration of 0.05–0.2 mM in treated patients in the published large RCT [90,91,92]. In the CANVAS trial, the rise in serum magnesium in patients treated with canagliflozin did, however, not correlate with the better cardiovascular outcome of these treated patients [93]. In any case, the potential role of SGLT2-inhibitors in hereditary tubulopathies such as Gitelman syndrome is promising, while its pleiotropic effects in transplant recipients also warrant further investigation. And so, SGLT2 inhibitors could become an additive therapy to optimize magnesium status in selected patients.
3.3. Magnesium and Pregnancy
Intravenous magnesium sulfate is an evidence-based treatment of pre-eclampsia, but iatrogenic hypermagnesemia is rather common and should be monitored, especially in case of decreased kidney function. According to a recent retrospective study of 429 severely pre-eclamptic women, the majority (61%) developed critical hypermagnesemia, which was associated with lower gestational age, a higher uric acid concentration, and a higher baseline serum magnesium concentration [94]. Peroral magnesium supplements were demonstrated to improve metabolic control in women with gestational diabetes, and nocturnal cramps in pregnancy seem to respond to supplementation in most trials [95,96].
3.4. Magnesium and Critical Illness
Although of potential use in critically ill patients, the role of correcting hypomagnesemia remains unclear, and a meta-analysis including three RCTs demonstrated lower mortality (RR 0.54 with 95%CI of 0.30–0.96) although high-quality trials are warranted to further support this [61,97].
Intravenous (IV) magnesium supplementation decreased the incidence of atrial fibrillation by 49% after cardiac surgery and has shown (in addition to standard-of-care treatment of rapid atrial fibrillation) significantly improved rate control and, to a lesser degree, the restoration of sinus rhythm [98,99]. Also, other therapeutic indications of intravenous magnesium sulfate exist, such as torsades de pointes, analgesic properties where it may reduce postoperative morphine consumption, asthma, and status asthmaticus in children, and/or chronic obstructive pulmonary disease exacerbations [100,101,102]. In the aforementioned placebo-controlled trials, hypomagnesemia was, interestingly, not a prerequisite for inclusion in the studies. To conclude, the therapeutic role of magnesium in the ICU remains relatively uncertain despite its beneficial effects for various indications. In Table 1, the evidence-based indications for magnesium supplementation were summarized and categorized according to the degree of supporting evidence.
3.5. Efficacy of Magnesium Supplementation
The evidence to support one magnesium formulation over another is rather limited but favors the use of organic magnesium compounds, although bioavailability is also enhanced by concomitant intake with food with the exception of partly fermentable and non-fermentable fibers, phytate, and oxalate [27]. Also, high intestinal concentrations of minerals such as calcium lower intestinal magnesium absorption. Absorption is enhanced with lower intestinal pH in conjunction with intake of proteins, medium-chain triglycerides, and low- or non-digestible carbohydrates (and avoidance of proton pump inhibitors if feasible) [27]. And so, an analysis of dietary intake could be relevant to reveal undesirable food interactions in patients with ongoing hypomagnesemia.
Refractoriness to magnesium supplementation is very prevalent among transplant recipients treated with calcineurin inhibitors, patients with diabetes, particularly with poor glycemic control, and CKD patients with proteinuria [33,39,53]. Of note, magnesium supplements decrease the bioavailability of non-steroidal anti-inflammatory drugs, tetracyclines, calcium channel blockers, aminoglycosides, bisphosphonates, and fluoroquinolones. In analogy, rats exposed to quinolones and a magnesium-deficient diet were more prone to develop tendinopathy. Magnesium could thus have pleiotropic effects, which prevent this drug-related adverse event [103].
4. Hypermagnesemia
Hypermagnesemia is defined by a serum magnesium concentration >1.2 mM (2.5 mg/dL) and is almost non-existent in patients with normal kidney function unless exposure occurs to huge concentrations of magnesium, for instance, in survivors of near-drowning in the Dead Sea [104]. A decline in glomerular filtrations impairs the adaptive ability to decrease renal magnesium absorption, although this does not automatically translate into hypermagnesemia, considering the prevalence of hypomagnesemia in CKD and even ESKD. This paradox is due to dietary restrictions to limit potassium exposure, generalized malnutrition, vitamin D insufficiency, use of diuretics and, of course, the development of a negative magnesium balance due to the low magnesium dialysate concentration in patients on peritoneal or hemodialysis [39,105]. Hypoalbuminemia can aggravate the negative magnesium balance in hemodialysis patients due to a higher concentration of free and dialyzable ionized fraction.
In patients with kidney dysfunction, exposure to magnesium-containing antacids and laxatives has been described to cause life-threatening hypermagnesemia, partially due to the unsaturable passive absorption [106,107,108]. Patients in the intensive care unit (ICU) with hypermagnesemia face a higher mortality even after adjustment for kidney function [109,110]. A U-shaped mortality curve has been observed in other study populations as well (such as hemodialysis patients). On the other hand, both higher and lower serum magnesium concentrations are associated with the development of cancer [2,28,29,30].
Symptoms of hypermagnesemia (>1.7–2.1 mM) are mostly neurological, with typically absent deep tendon reflexes, impaired consciousness, and disturbed gait, although more vague symptoms such as nausea and vomiting can co-exist. Hypermagnesemia can result in arrhythmia, including bradycardia and malignant ventricular tachycardia. The treatment of symptomatic and/or severe hypermagnesemia (>3 mM) includes airway management, continuous cardiac monitoring, and intravenous calcium (100–200 mg over 5–10 min), which antagonizes the neuromuscular and cardiac effects of magnesium and rarely renal replacement therapy [111]. For mild hypermagnesemia, the removal of sources of exogenous magnesium is mostly sufficient.
Controversy exists concerning the potential beneficial role of (mild) hypermagnesemia considering the pleiotropic effects of magnesium, which include anti-inflammatory, anti-oxidant, and anti-apoptotic properties [1,112,113]. Accumulating evidence points to a protective role of magnesium in vascular calcification supported by in vitro data, experiments in rodents with CKD but, more importantly, by RCTs in patients with CKD, where magnesium appears as one of the only treatment options where evidence was generated in favor of anti-calcification properties, although not all studies show a consistent protective effect [10,11,114]. The underlying mechanisms are diverse and include inhibition of the formation of hydroxyapatite and the trans-differentiation of vascular smooth muscle cells. Also, magnesium impedes the transition from calcified protein particles CPP1 into CPP2, restores the CaSR activity of the vascular smooth muscle cells, and activates the expression of the vitamin-K-dependent matrix Gla protein, which inhibits vascular calcification [115]. Magnesium also binds phosphate and improves endothelial function [1,112]. In CKD patients with or without end-stage kidney disease, moderate hypermagnesemia was associated with a survival benefit. These findings were, however, not validated in other study populations, such as people with cardiac failure, post-myocardial infarction, or admitted to the intensive care unit [29,65,66].
The discrepancy of absent benefit despite a biological rationale could allude to the poor reflection of cellular magnesium concentration by serum magnesium levels and has led some investigators to propose an altered reference interval for normal serum magnesium [45]. Moreover, the biologically active free ionized magnesium fraction can be lower due to a high anion gap or to complexing with excess phosphate, systematically biasing outcome according to strata of ionized serum magnesium in ESKD [116]. Anyway, whether serum magnesium is associated with superior clinical outcomes depends on the study population and investigated outcome. According to a recent Spanish study, patients with CKD and hypermagnesemia (serum magnesium > 2.2 mg/dL) had a higher risk of cardiovascular events [117]. Finally, animal experiments raised concerns about enhanced magnesium exposure leading to the development of adynamic bone disease. Bone biopsy studies in humans will be essential to resolve these concerns.
5. Conclusions
Hypomagnesemia is becoming more and more prevalent, and this is most likely attributable to a restricted oral intake and, to a lesser extent, to the widespread use of causal drugs, which include proton pump and calcineurin inhibitors. In line with this, some authors have proposed an adaptation of the normal reference values of serum magnesium concentration to comply with an updated Gaussian distribution.
The indications to correct moderate and asymptomatic hypomagnesemia remain theoretical and are based upon in vitro data, cross-sectional data, or therapeutic trials with mostly surrogate endpoints. Fortunately, trials are ongoing (NCT04079582, NCT03565913) to address the effects of increased magnesium exposure to patients with increased cardiovascular risk including CKD and dialysis patients, bearing in mind the potentially negative effects of overcorrection.
Hypermagnesemia remains mostly confined to patients with ESKD and to women with pre-eclampsia treated with high-dose IV magnesium supplementation. Rather scarcely, case reports and series of hypermagnesemia upon exposure to antacids and cathartics in patients with relatively preserved kidney function have been described. The majority of recently published interventional trials demonstrated no hazardous outcome following magnesium exposure in (CKD) patients with mild hypermagnesemia.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The author declares no conflicts of interest.
References
- de Baaij, J.H.; Hoenderop, J.G.; Bindels, R.J. Magnesium in man: Implications for health and disease. Physiol. Rev. 2015, 95, 1–46. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Castañeda, J.R.; de Mier, M.V.P.-R.; Rodríguez, M.; Rodríguez-Ortiz, M.E. Magnesium Replacement to Protect Cardiovascular and Kidney Damage? Lack of Prospective Clinical Trials. Int. J. Mol. Sci. 2018, 19, 664. [Google Scholar] [CrossRef] [PubMed]
- Tangvoraphonkchai, K.; Davenport, A. Magnesium and Cardiovascular Disease. Adv. Chronic Kidney Dis. 2018, 25, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Tseng, M.-H.; Yang, S.-S.; Sung, C.-C.; Ding, J.-J.; Hsu, Y.-J.; Chu, S.-M.; Lin, S.-H. Novel CNNM2 Mutation Responsible for Autosomal-Dominant Hypomagnesemia With Seizure. Front. Genet. 2022, 13, 875013. [Google Scholar] [CrossRef] [PubMed]
- de Baaij, J.H.F. Magnesium reabsorption in the kidney. Am. J. Physiol. Physiol. 2023, 324, F227–F244. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Chen, L.; Gutin, B.; Huang, Y.; Dong, Y.; Zhu, H. Magnesium Intake, C-Reactive Protein, and Muscle Mass in Adolescents. Nutrients 2022, 14, 2882. [Google Scholar] [CrossRef]
- Schimatschek, H.F.; Rempis, R. Prevalence of hypomagnesemia in an unselected German population of 16,000 individuals. Magnes. Res. 2001, 14, 283–290. [Google Scholar]
- Ma, J.; Folsom, A.R.; Melnick, S.L.; Eckfeldt, J.H.; Sharrett, A.; Nabulsi, A.A.; Hutchinson, R.G.; Metcalf, P.A. Associations of serum and dietary magnesium with cardiovascular disease, hypertension, diabetes, insulin, and carotid arterial wall thickness: The ARIC study. Atherosclerosis Risk in Communities Study. J. Clin. Epidemiol. 1995, 48, 927–940. [Google Scholar] [CrossRef]
- Cunha, A.R.; D’el-Rei, J.; Medeiros, F.; Umbelino, B.; Oigman, W.; Touyz, R.M.; Neves, M.F. Oral magnesium supplementation improves endothelial function and attenuates subclinical atherosclerosis in thiazide-treated hypertensive women. J. Hypertens. 2017, 35, 89–97. [Google Scholar] [CrossRef]
- Sakaguchi, Y.; Hamano, T.; Obi, Y.; Monden, C.; Oka, T.; Yamaguchi, S.; Matsui, I.; Hashimoto, N.; Matsumoto, A.; Shimada, K.; et al. A Randomized Trial of Magnesium Oxide and Oral Carbon Adsorbent for Coronary Artery Calcification in Predialysis CKD. J. Am. Soc. Nephrol. 2019, 30, 1073–1085. [Google Scholar] [CrossRef]
- Xu, C.; Smith, E.R.; Tiong, M.K.; Ruderman, I.; Toussaint, N.D. Interventions To Attenuate Vascular Calcification Progression in Chronic Kidney Disease: A Systematic Review of Clinical Trials. J. Am. Soc. Nephrol. 2022, 33, 1011–1032. [Google Scholar] [CrossRef] [PubMed]
- Zhan, Y.; Zhang, R.; Li, G. Effect of magnesium on vascular calcification in chronic kidney disease patients: A systematic review and meta-analysis. Ren. Fail. 2023, 45, 2182603. [Google Scholar] [CrossRef] [PubMed]
- Pethő, A.G.; Tapolyai, M.; Browne, M.; Fülöp, T. Hypomagnesemia as a Risk Factor and Accelerator for Vascular Aging in Diabetes Mellitus and Chronic Kidney Disease. Metabolites 2023, 13, 306. [Google Scholar] [CrossRef] [PubMed]
- Oost, L.J.; van der Heijden, A.A.; Vermeulen, E.A.; Bos, C.; Elders, P.J.; Slieker, R.C.; Kurstjens, S.; van Berkel, M.; Hoenderop, J.G.; Tack, C.J.; et al. Serum Magnesium Is Inversely Associated with Heart Failure, Atrial Fibrillation, and Microvascular Complications in Type 2 Diabetes. Diabetes Care 2021, 44, 1757–1765. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.-W.; Huang, Y.-T.; Jiang, M.-Y. Association of dietary magnesium intake and glycohemoglobin with mortality risk in diabetic patients. PLoS ONE 2022, 17, e0277180. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.-W.; Chen, Y.-Y.; Chen, W.-L. Association between oral intake magnesium and sarcopenia: A cross-sectional study. BMC Geriatr. 2022, 22, 816. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, H.S.; Burdmann, E.A.; Vieira, E.A.; Ferreira, M.L.; Ferreira, A.P.; Inda-Filho, A.J. Association of magnesium abnormalities at intensive care unit admission with kidney outcomes and mortality: A prospective cohort study. Clin. Exp. Nephrol. 2022, 26, 997–1004. [Google Scholar] [CrossRef]
- Koh, H.B.; Jung, C.-Y.; Kim, H.W.; Kwon, J.Y.; Kim, N.H.; Kim, H.J.; Jhee, J.H.; Han, S.H.; Yoo, T.-H.; Kang, S.-W.; et al. Preoperative Ionized Magnesium Levels and Risk of Acute Kidney Injury After Cardiac Surgery. Am. J. Kidney Dis. 2022, 80, 629–637.e1. [Google Scholar] [CrossRef]
- Correa, S.; Guerra-Torres, X.E.; Waikar, S.S.; Mc Causland, F.R. Serum Magnesium, Blood Pressure, and Risk of Hypertension and Chronic Kidney Disease Progression in the CRIC Study. Hypertension 2021, 78, 1771–1780. [Google Scholar] [CrossRef]
- Van Laecke, S.; Vermeiren, P.; Nagler, E.V.; Caluwe, R.; De Wilde, M.; Van der Vennet, M.; Peeters, P.; Randon, C.; Vermassen, F.; Vanholder, R.; et al. Magnesium and infection risk after kidney transplantation: An observational cohort study. J. Infect. 2016, 73, 8–17. [Google Scholar] [CrossRef]
- Odler, B.; Deak, A.T.; Pregartner, G.; Riedl, R.; Bozic, J.; Trummer, C.; Prenner, A.; Söllinger, L.; Krall, M.; Höflechner, L.; et al. Hypomagnesemia Is a Risk Factor for Infections after Kidney Transplantation: A Retrospective Cohort Analysis. Nutrients 2021, 13, 1296. [Google Scholar] [CrossRef] [PubMed]
- Groenendijk, I.; van Delft, M.; Versloot, P.; van Loon, L.J.; de Groot, L.C. Impact of magnesium on bone health in older adults: A systematic review and meta-analysis. Bone 2022, 154, 116233. [Google Scholar] [CrossRef] [PubMed]
- Veronese, N.; Stubbs, B.; Solmi, M.; Noale, M.; Vaona, A.; Demurtas, J.; Maggi, S. Dietary magnesium intake and fracture risk: Data from a large prospective study. Br. J. Nutr. 2017, 117, 1570–1576. [Google Scholar] [CrossRef] [PubMed]
- Fang, X.; Wang, K.; Han, D.; He, X.; Wei, J.; Zhao, L.; Imam, M.U.; Ping, Z.; Li, Y.; Xu, Y.; et al. Dietary magnesium intake and the risk of cardiovascular disease, type 2 diabetes, and all-cause mortality: A dose–response meta-analysis of prospective cohort studies. BMC Med. 2016, 14, 210. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.-C.; Pang, Z.; Liu, Q.-F. Magnesium intake and risk of colorectal cancer: A meta-analysis of prospective studies. Eur. J. Clin. Nutr. 2012, 66, 1182–1186. [Google Scholar] [CrossRef] [PubMed]
- Del Gobbo, L.C.; Imamura, F.; Wu, J.H.; Otto, M.C.d.O.; Chiuve, S.E.; Mozaffarian, D. Circulating and dietary magnesium and risk of cardiovascular disease: A systematic review and meta-analysis of prospective studies. Am. J. Clin. Nutr. 2013, 98, 160–173. [Google Scholar] [CrossRef]
- Schuchardt, J.P.; Hahn, A. Intestinal Absorption and Factors Influencing Bioavailability of Magnesium- An Update. Curr. Nutr. Food Sci. 2017, 13, 260–278. [Google Scholar] [CrossRef]
- Lin, T.; Bi, C.; Song, Y.; Guo, H.; Liu, L.; Zhou, Z.; Wang, B.; Tang, G.; Liu, C.; Yang, Y.; et al. Plasma Magnesium Concentrations and Risk of Incident Cancer in Adults with Hypertension: A Nested Case-Control Study. Ann. Nutr. Metab. 2020, 76, 304–312. [Google Scholar] [CrossRef]
- Sakaguchi, Y.; Fujii, N.; Shoji, T.; Hayashi, T.; Rakugi, H.; Isaka, Y. Hypomagnesemia is a significant predictor of cardiovascular and non-cardiovascular mortality in patients undergoing hemodialysis. Kidney Int. 2014, 85, 174–181. [Google Scholar] [CrossRef]
- Panthofer, A.M.; Lyu, B.; Astor, B.C.; Singh, T.; Aziz, F.; Mandelbrot, D.; Parajuli, S.; Mohamed, M.; Djamali, A.; Garg, N. Post-kidney transplant serum magnesium exhibits a U-shaped association with subse-quent mortality: An observational cohort study. Transpl. Int. Off. J. Eur. Soc. Organ Transplant. 2021, 34, 1853–1861. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Veronese, N.; Barbagallo, M. Magnesium and Hypertension in Old Age. Nutrients 2020, 13, 139. [Google Scholar] [CrossRef] [PubMed]
- Vetter, T.; Lohse, M.J. Magnesium and the parathyroid. Curr. Opin. Nephrol. Hypertens. 2002, 11, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Van Laecke, S.; Van Biesen, W. Hypomagnesaemia in kidney transplantation. Transplant. Rev. 2015, 29, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Groenestege, W.M.T.; Hoenderop, J.G.; van den Heuvel, L.; Knoers, N.; Bindels, R.J. The Epithelial Mg2+Channel Transient Receptor Potential Melastatin 6 Is Regulated by Dietary Mg2+Content and Estrogens. J. Am. Soc. Nephrol. 2006, 17, 1035–1043. [Google Scholar] [CrossRef] [PubMed]
- Gommers, L.M.M.; Hoenderop, J.G.J.; de Baaij, J.H.F. Mechanisms of proton pump inhibitor-induced hypomagnesemia. Acta Physiol. 2022, 235, e13846. [Google Scholar] [CrossRef] [PubMed]
- Kieboom, B.C.T.; Kiefte–de Jong, J.C.; Eijgelsheim, M.; Franco, O.H.; Kuipers, E.J.; Hofman, A.; Zietse, R.; Stricker, B.H.; Hoorn, E.J. Proton Pump Inhibitors and Hypomagnesemia in the General Population: A Population-Based Cohort Study. Am. J. Kidney Dis. 2015, 66, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Meaney, C.J.; Beccari, M.V.; Yang, Y.; Zhao, J. Systematic Review and Meta-Analysis of Patiromer and Sodium Zirconium Cyclosilicate: A New Armamentarium for the Treatment of Hyperkalemia. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2017, 37, 401–411. [Google Scholar] [CrossRef]
- Weir, M.R.; Bakris, G.L.; Bushinsky, D.A.; Mayo, M.R.; Garza, D.; Stasiv, Y.; Wittes, J.; Christ-Schmidt, H.; Berman, L.; Pitt, B. Patiromer in Patients with Kidney Disease and Hyperkalemia Receiving RAAS Inhibitors. New Engl. J. Med. 2015, 372, 211–221. [Google Scholar] [CrossRef]
- Oka, T.; Hamano, T.; Sakaguchi, Y.; Yamaguchi, S.; Kubota, K.; Senda, M.; Yonemoto, S.; Shimada, K.; Matsumoto, A.; Hashimoto, N.; et al. Proteinuria-associated renal magnesium wasting leads to hypomagnesemia: A common electrolyte abnormality in chronic kidney disease. Nephrol. Dial. Transplant. 2019, 34, 1154–1162. [Google Scholar] [CrossRef]
- Gagliano, V.; Schäffeler, F.; Del Giorno, R.; Bianchetti, M.; Canarte, C.F.C.; Regueira, J.J.C.; Gabutti, L. Does Ionized Magnesium Offer a Different Perspective Exploring the Association between Magnesemia and Targeted Cardiovascular Risk Factors? J. Clin. Med. 2022, 11, 4015. [Google Scholar] [CrossRef]
- Macian, N.; Dualé, C.; Voute, M.; Leray, V.; Courrent, M.; Bodé, P.; Giron, F.; Sonneville, S.; Bernard, L.; Joanny, F.; et al. Short-Term Magnesium Therapy Alleviates Moderate Stress in Patients with Fibromyalgia: A Randomized Double-Blind Clinical Trial. Nutrients 2022, 14, 2088. [Google Scholar] [CrossRef] [PubMed]
- Salehidoost, R.; Boroujeni, G.T.; Feizi, A.; Aminorroaya, A.; Amini, M. Effect of oral magnesium supplement on cardiometabolic markers in people with prediabetes: A double blind randomized controlled clinical trial. Sci. Rep. 2022, 12, 18209. [Google Scholar] [CrossRef] [PubMed]
- Schutten, J.C.; Joris, P.J.; Groendijk, I.; Eelderink, C.; Groothof, D.; van der Veen, Y.; Westerhuis, R.; Goorman, F.; Danel, R.M.; de Borst, M.H.; et al. Effects of Magnesium Citrate, Magnesium Oxide, and Magnesium Sulfate Supplementation on Arterial Stiffness: A Randomized, Double-Blind, Placebo-Controlled Intervention Trial. J. Am. Heart Assoc. 2022, 11, e021783. [Google Scholar] [CrossRef]
- Schutten, J.C.; Joris, P.J.; Minović, I.; Post, A.; van Beek, A.P.; de Borst, M.H.; Mensink, R.P.; Bakker, S.J.L. Long-term magnesium supplementation improves glucocorticoid metabolism: A post-hoc analysis of an intervention trial. Clin. Endocrinol. 2021, 94, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Micke, O.; Vormann, J.; Kraus, A.; Kisters, K. Serum magnesium: Time for a standardized and evidence-based reference range. Magnes. Res. 2021, 34, 84–89. [Google Scholar] [PubMed]
- Viering, D.H.H.M.; de Baaij, J.H.F.; Walsh, S.B.; Kleta, R.; Bockenhauer, D. Genetic causes of hypomagnesemia, a clinical overview. Pediatr. Nephrol. 2017, 32, 1123–1135. [Google Scholar] [CrossRef]
- Figueres, L.; Bruneau, S.; Prot-Bertoye, C.; Brideau, G.; Néel, M.; Griveau, C.; Cheval, L.; Bignon, Y.; Dimitrov, J.; Dejoie, T.; et al. Hypomagnesemia, Hypocalcemia, and Tubulointerstitial Nephropathy Caused by Claudin-16 Autoantibodies. J. Am. Soc. Nephrol. 2022, 33, 1402–1410. [Google Scholar] [CrossRef]
- Blanchard, A.; Bockenhauer, D.; Bolignano, D.; Calò, L.A.; Cosyns, E.; Devuyst, O.; Ellison, D.H.; Frankl, F.E.K.; Knoers, N.V.; Konrad, M.; et al. Gitelman syndrome: Consensus and guidance from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2017, 91, 24–33. [Google Scholar] [CrossRef]
- Schlingmann, K.P.; de Baaij, J.H. The genetic spectrum of Gitelman(-like) syndromes. Curr. Opin. Nephrol. Hypertens. 2022, 31, 508–515. [Google Scholar] [CrossRef]
- Viering, D.; Schlingmann, K.P.; Hureaux, M.; Nijenhuis, T.; Mallett, A.; Chan, M.M.; van Beek, A.; van Eerde, A.M.; Coulibaly, J.-M.; Vallet, M.; et al. Gitelman-Like Syndrome Caused by Pathogenic Variants in mtDNA. J. Am. Soc. Nephrol. 2022, 33, 305–325. [Google Scholar] [CrossRef]
- Blanchard, A.; Vallet, M.; Dubourg, L.; Hureaux, M.; Allard, J.; Haymann, J.-P.; de la Faille, R.; Arnoux, A.; Dinut, A.; Bergerot, D.; et al. Resistance to Insulin in Patients with Gitelman Syndrome and a Subtle Intermediate Phenotype in Heterozygous Carriers: A Cross-Sectional Study. J. Am. Soc. Nephrol. 2019, 30, 1534–1545. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.D.R.; Antonelou, M.; Sathiananthamoorthy, S.; Rega, M.; Henderson, S.; Ceron-Gutierrez, L.; Barcenas-Morales, G.; Müller, C.A.; Doffinger, R.; Walsh, S.B.; et al. Inherited salt-losing tubulopathies are associated with immunodeficiency due to impaired IL-17 responses. Nat. Commun. 2020, 11, 4368. [Google Scholar] [CrossRef] [PubMed]
- Barbagallo, M.; Di Bella, G.; Brucato, V.; D’angelo, D.; Damiani, P.; Monteverde, A.; Belvedere, M.; Dominguez, L.J. Serum ionized magnesium in diabetic older persons. Metabolism 2014, 63, 502–509. [Google Scholar] [CrossRef]
- Kieboom, B.C.T.; Ligthart, S.; Dehghan, A.; Kurstjens, S.; de Baaij, J.H.F.; Franco, O.H.; Hofman, A.; Zietse, R.; Stricker, B.H.; Hoorn, E.J. Serum magnesium and the risk of prediabetes: A population-based cohort study. Diabetologia 2017, 60, 843–853. [Google Scholar] [CrossRef] [PubMed]
- Van Laecke, S.; Van Biesen, W.; Verbeke, F.; De Bacquer, D.; Peeters, P.; Vanholder, R. Posttransplantation Hypomagnesemia and Its Relation with Immunosuppression as Predictors of New-Onset Diabetes after Transplantation. Am. J. Transplant. 2009, 9, 2140–2149. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.W.; Famure, O.; Li, Y.; Kim, S.J. Hypomagnesemia and the Risk of New-Onset Diabetes Mellitus after Kidney Transplantation. J. Am. Soc. Nephrol. 2016, 27, 1793–1800. [Google Scholar] [CrossRef] [PubMed]
- Oost, L.J.; Kurstjens, S.; Ma, C.; Hoenderop, J.G.J.; Tack, C.J.; de Baaij, J.H.F. Magnesium increases insulin-dependent glucose uptake in adipocytes. Front. Endocrinol. 2022, 13, 986616. [Google Scholar] [CrossRef]
- Lecube, A.; Baena-Fustegueras, J.A.; Fort, J.M.; Pelegrí, D.; Hernández, C.; Simó, R. Diabetes Is the Main Factor Accounting for Hypomagnesemia in Obese Subjects. PLoS ONE 2012, 7, e30599. [Google Scholar] [CrossRef]
- Nielsen, F.H.; Lukaski, H.C. Update on the relationship between magnesium and exercise. Magnes. Res. 2006, 19, 180–189. [Google Scholar]
- Scherr, J.; Schuster, T.; Pressler, A.; Roeh, A.; Christle, J.; Wolfarth, B.; Halle, M. Repolarization Perturbation and Hypomagnesemia after Extreme Exercise. Med. Sci. Sports Exerc. 2012, 44, 1637–1643. [Google Scholar] [CrossRef]
- Hansen, B.A.; Bruserud, Ø. Hypomagnesemia in critically ill patients. J. Intensive Care 2018, 6, 21. [Google Scholar] [CrossRef] [PubMed]
- Agus, Z.S. Hypomagnesemia. J. Am. Soc. Nephrol. 1999, 10, 1616–1622. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.-L.; Kuo, E. Mechanism of Hypokalemia in Magnesium Deficiency. J. Am. Soc. Nephrol. 2007, 18, 2649–2652. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-C.; Wahlqvist, M.L.; Kao, M.-D.; Wang, J.-L.; Lee, M.-S. Optimal Dietary and Plasma Magnesium Statuses Depend on Dietary Quality for a Reduction in the Risk of All-Cause Mortality in Older Adults. Nutrients 2015, 7, 5664–5683. [Google Scholar] [CrossRef] [PubMed]
- Van Laecke, S.; Nagler, E.V.; Verbeke, F.; Van Biesen, W.; Vanholder, R. Hypomagnesemia and the Risk of Death and GFR Decline in Chronic Kidney Disease. Am. J. Med. 2013, 126, 825–831. [Google Scholar] [CrossRef] [PubMed]
- Lacson, E.; Wang, W.; Ma, L.; Passlick-Deetjen, J. Serum Magnesium and Mortality in Hemodialysis Patients in the United States: A Cohort Study. Am. J. Kidney Dis. 2015, 66, 1056–1066. [Google Scholar] [CrossRef]
- Lutsey, P.L.; Alonso, A.; Michos, E.D.; Loehr, L.R.; Astor, B.C.; Coresh, J.; Folsom, A.R. Serum magnesium, phosphorus, and calcium are associated with risk of incident heart failure: The Atherosclerosis Risk in Communities (ARIC) Study. Am. J. Clin. Nutr. 2014, 100, 756–764. [Google Scholar] [CrossRef]
- Ferrè, S.; Li, X.; Adams-Huet, B.; Maalouf, N.M.; Sakhaee, K.; Toto, R.D.; Moe, O.W.; Neyra, J.A. Association of serum magnesium with all-cause mortality in patients with and without chronic kidney disease in the Dallas Heart Study. Nephrol. Dial. Transplant. 2018, 33, 1389–1396. [Google Scholar] [CrossRef]
- Azem, R.; Daou, R.; Bassil, E.; Anvari, E.M.; Taliercio, J.J.; Arrigain, S.; Schold, J.D.; Vachharajani, T.; Nally, J.; Na Khoul, G.N. Serum magnesium, mortality and disease progression in chronic kidney disease. BMC Nephrol. 2020, 21, 49. [Google Scholar] [CrossRef]
- Lötscher, J.; i Líndez, A.-A.M.; Kirchhammer, N.; Cribioli, E.; Attianese, G.M.P.G.; Trefny, M.P.; Lenz, M.; Rothschild, S.I.; Strati, P.; Künzli, M.; et al. Magnesium sensing via LFA-1 regulates CD8+ T cell effector function. Cell 2022, 185, 585–602.e29. [Google Scholar] [CrossRef]
- Chaigne-Delalande, B.; Li, F.-Y.; O’connor, G.M.; Lukacs, M.J.; Jiang, P.; Zheng, L.; Shatzer, A.; Biancalana, M.; Pittaluga, S.; Matthews, H.F.; et al. Mg2+ Regulates Cytotoxic Functions of NK and CD8 T Cells in Chronic EBV Infection Through NKG2D. Science 2013, 341, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Chauvin, S.D.; Price, S.; Zou, J.; Hunsberger, S.; Brofferio, A.; Matthews, H.; Similuk, M.; Rosenzweig, S.D.; Su, H.C.; Cohen, J.I.; et al. A Double-Blind, Placebo-Controlled, Crossover Study of Magnesium Supplementation in Patients with XMEN Disease. J. Clin. Immunol. 2022, 42, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Lian, X.; Chen, H. The association of serum magnesium with infection in new-onset systemic lupus erythematosus patients. Lupus 2023, 32, 9612033221149884. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.-L.; Wang, S.-Q.; Ji, M.-J.; Wang, X.-M.; Sun, J.; Zhang, M.-M.; Ma, C.-M. Hypomagnesemia is associated with increased mortality in the short-term but not the long-term in community-acquired pneumonia patients with type 2 diabetes. Magnes. Res. 2022, 35, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Juan, R.; Otim, I.; Nabalende, H.; Legason, I.D.; Reynolds, S.J.; Ogwang, M.D.; Ndugwa, C.M.; Marshall, V.; Whitby, D.; Goedert, J.J.; et al. Plasma magnesium is inversely associated with Epstein-Barr virus load in peripheral blood and Burkitt lymphoma in Uganda. Cancer Epidemiol. 2018, 52, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Ravell, J.; Chaigne-Delalande, B.; Lenardo, M. X-linked immunodeficiency with magnesium defect, Epstein-Barr virus infection, and neoplasia disease: A combined immune deficiency with magnesium defect. Curr. Opin. Pediatr. 2014, 26, 713–719. [Google Scholar] [CrossRef]
- Alam, A.B.; Thomas, D.S.; Lutsey, P.L.; Shrestha, S.; Alonso, A. Associations of Serum Magnesium with Brain Morphology and Subclinical Cerebrovascular Disease: The Atherosclerosis Risk in Communities-Neurocognitive Study. Nutrients 2021, 13, 4496. [Google Scholar] [CrossRef]
- Kieboom, B.C.; Licher, S.; Wolters, F.J.; Ikram, M.K.; Hoorn, E.J.; Zietse, R.; Stricker, B.H. Serum magnesium is associated with the risk of dementia. Neurology 2017, 89, 1716–1722. [Google Scholar] [CrossRef]
- Sakaguchi, Y.; Hamano, T.; Wada, A.; Hoshino, J.; Masakane, I. Magnesium and Risk of Hip Fracture among Patients Undergoing Hemodialysis. J. Am. Soc. Nephrol. 2018, 29, 991–999. [Google Scholar] [CrossRef]
- Kunutsor, S.K.; Whitehouse, M.R.; Blom, A.W.; Laukkanen, J.A. Low serum magnesium levels are associated with increased risk of fractures: A long-term prospective cohort study. Eur. J. Epidemiol. 2017, 32, 593–603. [Google Scholar] [CrossRef]
- Soliman, H.M.; Mercan, D.; Lobo, S.S.M.; Mélot, C.; Vincent, J.-L. Development of ionized hypomagnesemia is associated with higher mortality rates. Crit. Care Med. 2003, 31, 1082–1087. [Google Scholar] [CrossRef] [PubMed]
- Upala, S.; Jaruvongvanich, V.; Wijarnpreecha, K.; Sanguankeo, A. Hypomagnesemia and mortality in patients admitted to intensive care unit: A systematic review and meta-analysis. QJM 2016, 109, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Masuyama, S.; Mizui, M.; Maeda, K.; Shimamura, K.; Sakaguchi, Y.; Morita, M.; Kuratani, T.; Mizote, I.; Nakamura, D.; Sakata, Y.; et al. Preoperative hypomagnesemia as a possible predictive factor for postoperative increase of transvalvular pressure gradient in hemodialysis patients treated with transcatheter aortic valve implantation. Ren. Fail. 2022, 44, 1083–1089. [Google Scholar] [CrossRef]
- Ferrè, S.; Li, X.; Adams-Huet, B.; Maalouf, N.M.; Sakhaee, K.; Toto, R.D.; Moe, O.W.; Neyra, J.A. Low Serum Magnesium is associated with Faster Decline in Kidney Function: The Dallas Heart Study Experience. J. Investig. Med. 2019, 67, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Joosten, M.M.; Gansevoort, R.T.; Bakker, S.J. Low plasma magnesium and risk of developing chronic kidney disease: Results from the PREVEND Study. Kidney Int. 2015, 87, 1262–1263. [Google Scholar] [CrossRef] [PubMed]
- Sakaguchi, Y.; Iwatani, H.; Hamano, T.; Tomida, K.; Kawabata, H.; Kusunoki, Y.; Shimomura, A.; Matsui, I.; Hayashi, T.; Tsubakihara, Y.; et al. Magnesium modifies the association between serum phosphate and the risk of progression to end-stage kidney disease in patients with non-diabetic chronic kidney disease. Kidney Int. 2015, 88, 833–842. [Google Scholar] [CrossRef] [PubMed]
- Rebholz, C.M.; Tin, A.; Liu, Y.; Kuczmarski, M.F.; Evans, M.K.; Zonderman, A.B.; Crews, D.C. Dietary Magnesium and Kidney Function Decline: The Healthy Aging in Neighborhoods of Diversity across the Life Span Study. Am. J. Nephrol. 2016, 44, 381–387. [Google Scholar] [CrossRef]
- Brown, R.S. Magnesium Sulfate: Another Cause of a Solute Diuresis. Am. J. Kidney Dis. 2017, 69, 550–551. [Google Scholar] [CrossRef]
- Veronese, N.; Pizzol, D.; Smith, L.; Dominguez, L.J.; Barbagallo, M. Effect of Magnesium Supplementation on Inflammatory Parameters: A Meta-Analysis of Randomized Controlled Trials. Nutrients 2022, 14, 679. [Google Scholar] [CrossRef]
- Ng, H.Y.; Kuo, W.H.; Tain, Y.L.; Leung, F.F.; Lee, W.C.; Lee, C.T. Effect of Dapagliflozin and Magnesium Supplementation on Renal Magnesium Handling and Magnesium Homeostasis in Metabolic Syndrome. Nutrients 2021, 13, 4088. [Google Scholar] [CrossRef]
- Tang, H.; Zhang, X.; Zhang, J.; Li, Y.; Del Gobbo, L.C.; Zhai, S.; Song, Y. Elevated serum magnesium associated with SGLT2 inhibitor use in type 2 diabetes patients: A meta-analysis of randomised controlled trials. Diabetologia 2016, 59, 2546–2551. [Google Scholar] [CrossRef] [PubMed]
- Palmer, B.F.; Clegg, D.J. Kidney-Protective Effects of SGLT2 Inhibitors. Clin. J. Am. Soc. Nephrol. 2023, 18, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.M.; Li, J.; Bhalla, V.; Jardine, M.J.; Neal, B.; de Zeeuw, D.; Fulcher, G.; Perkovic, V.; Mahaffey, K.W.; Chang, T.I. Canagliflozin, serum magnesium and cardiovascular outcomes—Analysis from the CANVAS Program. Endocrinol. Diabetes Metab. 2021, 4, e00247. [Google Scholar] [CrossRef] [PubMed]
- Elasy, A.N.; Nafea, O.E. Critical Hypermagnesemia in Preeclamptic Women Under a Magnesium Sulfate Regimen: Incidence and Associated Risk Factors. Biol. Trace Element Res. 2022, 201, 3670–3678. [Google Scholar] [CrossRef] [PubMed]
- Qu, Q.; Rong, R.; Yu, J. Effect of magnesium supplementation on pregnancy outcome in gestational diabetes mellitus patients: A meta-analysis of randomized controlled trials. Food Sci. Nutr. 2022, 10, 3193–3202. [Google Scholar] [CrossRef] [PubMed]
- Garrison, S.R.; Allan, G.M.; Sekhon, R.K.; Musini, V.M.; Khan, K.M. Magnesium for skeletal muscle cramps. Cochrane Database Syst. Rev. 2020, 9, Cd009402. [Google Scholar] [CrossRef] [PubMed]
- Vesterlund, G.K.; Jensen, T.S.; Ellekjaer, K.L.; Møller, M.H.; Thomsen, T.; Perner, A. Effects of magnesium, phosphate, or zinc supplementation in intensive care unit patients—A systematic review and meta-analysis. Acta Anaesthesiol. Scand. 2023, 67, 264–276. [Google Scholar] [CrossRef]
- Ramesh, T.; Lee, P.Y.K.; Mitta, M.; Allencherril, J. Intravenous magnesium in the management of rapid atrial fibrillation: A systematic review and meta-analysis. J. Cardiol. 2021, 78, 375–381. [Google Scholar] [CrossRef]
- Fairley, J.L.; Zhang, L.; Glassford, N.J.; Bellomo, R. Magnesium status and magnesium therapy in cardiac surgery: A systematic review and meta-analysis focusing on arrhythmia prevention. J. Crit. Care 2017, 42, 69–77. [Google Scholar] [CrossRef]
- Jahangir, A.; Zia, Z.; Niazi, M.R.K.; Sahra, S.; Jahangir, A.; Sharif, M.A.; Chalhoub, M.N. Efficacy of Magnesium Sulfate in the Chronic Obstructive Pulmonary Disease Population: A Systematic Review and Meta-Analysis. Adv. Respir. Med. 2022, 90, 125–133. [Google Scholar] [CrossRef]
- Ng, K.T.; Yap, J.L.; Izham, I.N.; Teoh, W.Y.; Kwok, P.E.; Koh, W.J. The effect of intravenous magnesium on postoperative morphine consumption in noncardiac surgery: A systematic review and meta-analysis with trial sequential analysis. Eur. J. Anaesthesiol. 2020, 37, 212–223. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.N.; Drury, A.S.; Gupta, N. Continuous Magnesium Sulfate Infusions for Status Asthmaticus in Children: A Systematic Review. Front. Pediatr. 2022, 10, 853574. [Google Scholar] [CrossRef] [PubMed]
- Shakibaei, M.; Pfister, K.; Schwabe, R.; Vormann, J.; Stahlmann, R. Ultrastructure of Achilles Tendons of Rats Treated with Ofloxacin and Fed a Normal or Magnesium-Deficient Diet. Antimicrob. Agents Chemother. 2000, 44, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Oren, S.; Rapoport, J.; Zlotnik, M.; Brami, J.; Heimer, D.; Chaimovitz, C. Extreme Hypermagnesemia Due to Ingestion of Dead Sea Water. Nephron 1987, 47, 199–201. [Google Scholar] [CrossRef]
- Wyskida, K.; Witkowicz, J.; Chudek, J.; Więcek, A. Daily Magnesium Intake and Hypermagnesemia in Hemodialysis Patients With Chronic Kidney Disease. J. Ren. Nutr. 2012, 22, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Weng, Y.-M.; Chen, S.-Y.; Chen, H.-C.; Yu, J.-H.; Wang, S.-H. Hypermagnesemia in a Constipated Female. J. Emerg. Med. 2013, 44, e57–e60. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, H.; Shimada, H.; Yoshita, K.; Tsubata, Y.; Ikarashi, K.; Morioka, T.; Saito, N.; Sakai, S.; Narita, I. Severe hypermagnesemia induced by magnesium oxide ingestion: A case series. CEN Case Rep. 2019, 8, 31–37. [Google Scholar] [CrossRef]
- Wakai, E.; Ikemura, K.; Sugimoto, H.; Iwamoto, T.; Okuda, M. Risk factors for the development of hypermagnesemia in patients prescribed magnesium oxide: A retrospective cohort study. J. Pharm. Health Care Sci. 2019, 5, 4. [Google Scholar] [CrossRef]
- Tuttle, A.; Fitter, S.; Hua, H.; Moussavi, K. The Effects of Magnesium Coadminstration During Treatment of Hypokalemia in the Emergency Department. J. Emerg. Med. 2022, 63, 399–413. [Google Scholar] [CrossRef]
- Naksuk, N.; Hu, T.; Krittanawong, C.; Thongprayoon, C.; Sharma, S.; Park, J.Y.; Rosenbaum, A.N.; Gaba, P.; Killu, A.M.; Sugrue, A.M.; et al. Association of Serum Magnesium on Mortality in Patients Admitted to the Intensive Cardiac Care Unit. Am. J. Med. 2017, 130, 229.e5–229.e13. [Google Scholar] [CrossRef]
- Dibaba, D.T.; Xun, P.; Song, Y.; Rosanoff, A.; Shechter, M.; He, K. The effect of magnesium supplementation on blood pressure in individuals with insulin resistance, prediabetes, or noncommunicable chronic diseases: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2017, 106, 921–929. [Google Scholar] [CrossRef] [PubMed]
- Simental-Mendia, L.E.; Sahebkar, A.; Rodriguez-Moran, M.; Zambrano-Galvan, G.; Guerrero-Romero, F. Effect of Magnesium Supplementation on Plasma C-reactive Protein Concentrations: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Curr. Pharm. Des. 2017, 23, 4678–4686. [Google Scholar] [CrossRef] [PubMed]
- Van Laecke, S.; Van Biesen, W.; Vanholder, R. Hypomagnesaemia, the kidney and the vessels. Nephrol. Dial. Transplant. 2012, 27, 4003–4010. [Google Scholar] [CrossRef] [PubMed]
- Leenders, N.H.J.; Bos, C.; Hoekstra, T.; Schurgers, L.J.; Vervloet, M.G.; Hoenderop, J.G.J. Dietary magnesium supplementation inhibits abdominal vascular calcification in an experimental animal model of chronic kidney disease. Nephrol. Dial. Transplant. 2022, 37, 1049–1058. [Google Scholar] [CrossRef]
- Ter Braake, A.D.; Vervloet, M.G.; de Baaij, J.H.F.; Hoenderop, J.G.J. Magnesium to prevent kidney disease-associated vascular calcification: Crystal clear? Nephrol. Dial. Transplant. 2022, 37, 421–429. [Google Scholar] [CrossRef]
- Sakaguchi, Y.; Hamano, T.; Kubota, K.; Oka, T.; Yamaguchi, S.; Matsumoto, A.; Hashimoto, N.; Mori, D.; Obi, Y.; Matsui, I.; et al. Anion Gap as a Determinant of Ionized Fraction of Divalent Cations in Hemodialysis Patients. Clin. J. Am. Soc. Nephrol. 2018, 13, 274–281. [Google Scholar] [CrossRef]
- Carrillo, I.G.; Vega, A.; Goicoechea, M.; Shabaka, A.; Gatius, S.; Abad, S.; López-Gómez, J.M. Impact of Serum Magnesium Levels on Kidney and Cardiovascular Prognosis and Mortality in CKD Patients. J. Ren. Nutr. 2021, 31, 494–502. [Google Scholar] [CrossRef]
Figure 1.
The clinical spectrum of hypomagnesemia. Depicted in the upper part are symptoms related to hypomagnesemia (or a magnesium deficit), both of which are potentiated by concomitant hypokalemia and hypocalcemia, electrolyte disturbances that are more common in subjects with hypomagnesemia. Depicted in the lower part are clinical associations with hypomagnesemia (arrows in grey point to a strong association; arrows in yellow point to a described association with less supportive evidence) [8,12,13,14,18,19,20,21,22,23,24,53,62,67,73,74,75,76,77].
Figure 1.
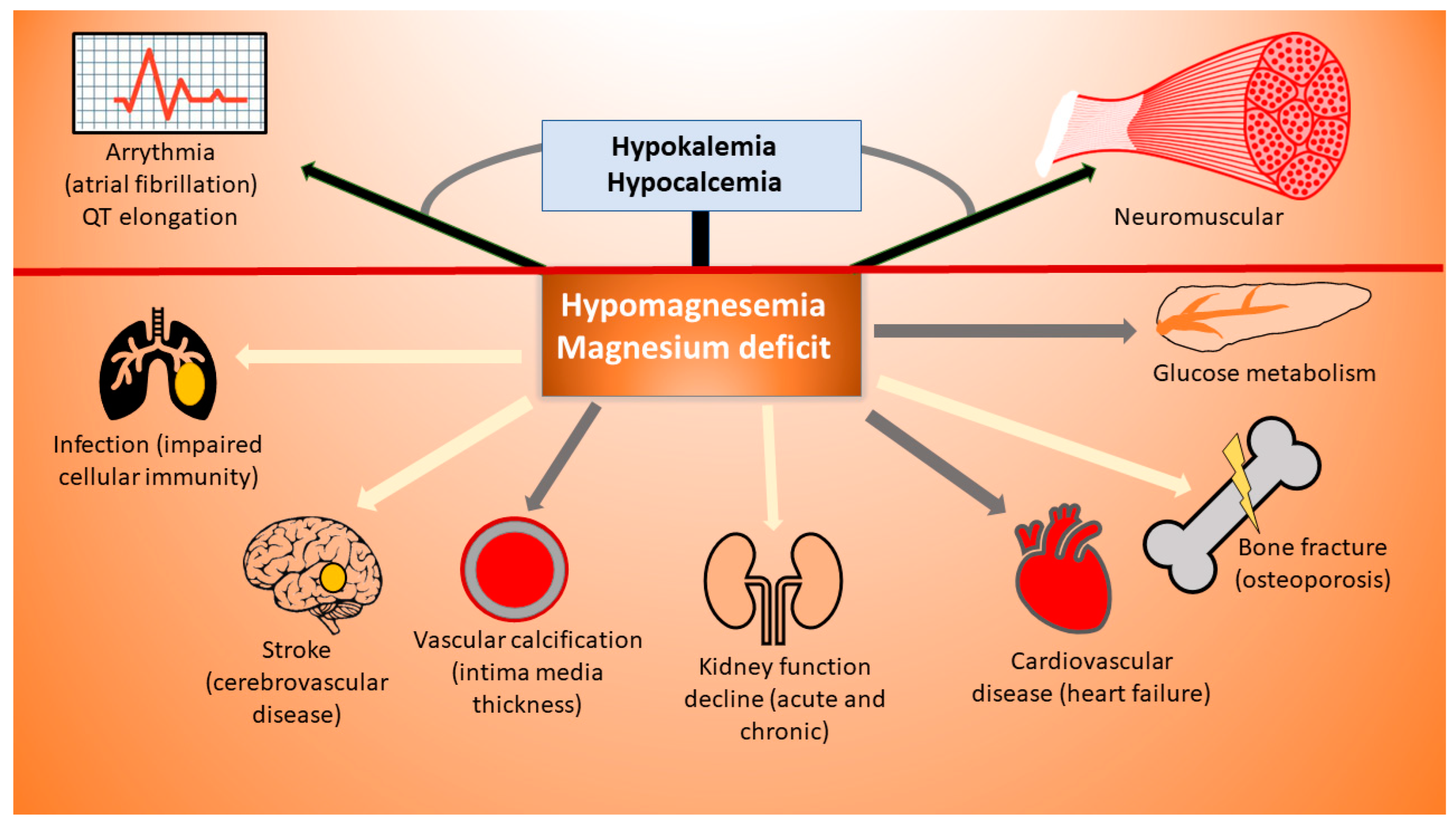
The clinical spectrum of hypomagnesemia. Depicted in the upper part are symptoms related to hypomagnesemia (or a magnesium deficit), both of which are potentiated by concomitant hypokalemia and hypocalcemia, electrolyte disturbances that are more common in subjects with hypomagnesemia. Depicted in the lower part are clinical associations with hypomagnesemia (arrows in grey point to a strong association; arrows in yellow point to a described association with less supportive evidence) [8,12,13,14,18,19,20,21,22,23,24,53,62,67,73,74,75,76,77].

{kind=link}
Table 1.
Therapeutic effects of magnesium supplementation (derived mostly from randomized controlled trials) *.
Table 1.
Therapeutic effects of magnesium supplementation (derived mostly from randomized controlled trials) *.
| Proven | Probable | Uncertain or Unproven |
|---|---|---|
|
|
|
* High-grade evidence despite the absence of randomized controlled trials.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Van Laecke, S. An Update on Hypomagnesemia and Hypermagnesemia. Kidney Dial. 2024, 4, 1-14. https://doi.org/10.3390/kidneydial4010001
AMA Style
Van Laecke S. An Update on Hypomagnesemia and Hypermagnesemia. Kidney and Dialysis. 2024; 4(1):1-14. https://doi.org/10.3390/kidneydial4010001
Chicago/Turabian StyleVan Laecke, Steven. 2024. "An Update on Hypomagnesemia and Hypermagnesemia" Kidney and Dialysis 4, no. 1: 1-14. https://doi.org/10.3390/kidneydial4010001