
The Utilization of Body Composition to Predict Cardiorespiratory Fitness and Determine Association with CKD Stage in Individuals with Mid-Spectrum CKD: A Pilot Study
 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Overview
2.2. Research Subjects
2.3. Body Composition Assessment
2.4. Health Screening and Exercise Testing
2.5. Statistical Analysis
3. Results
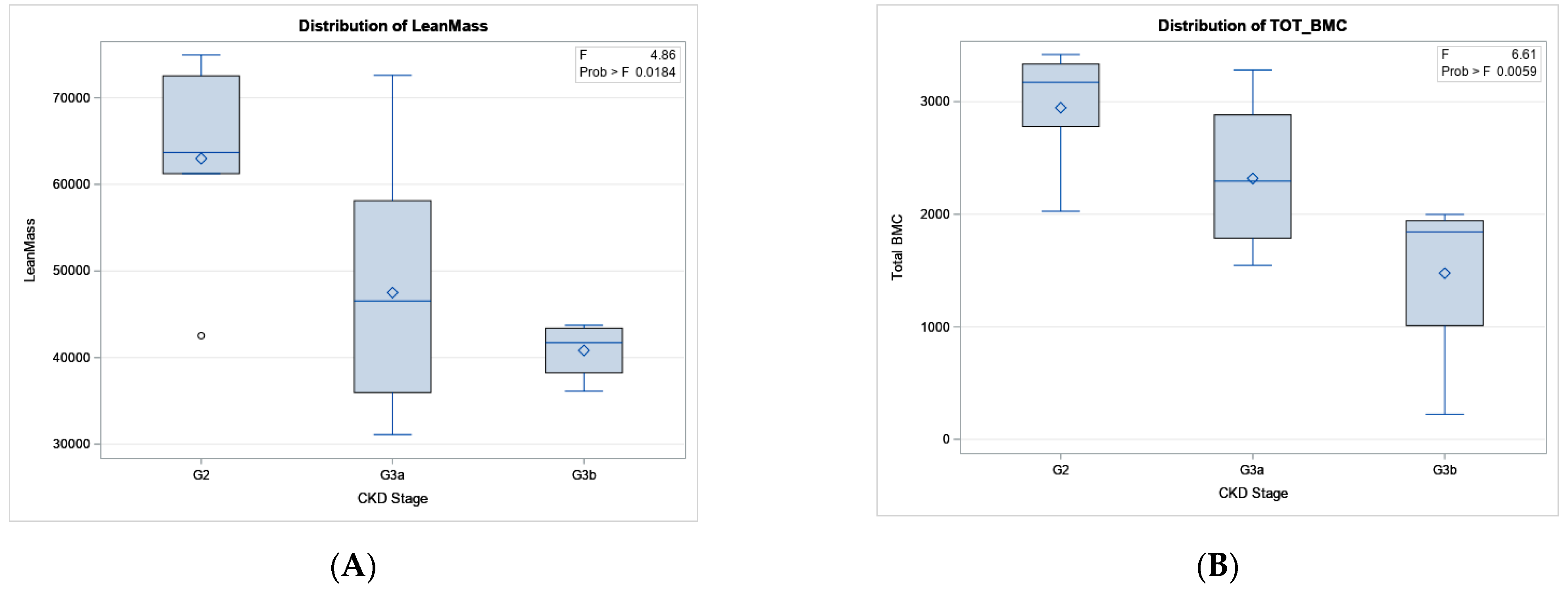
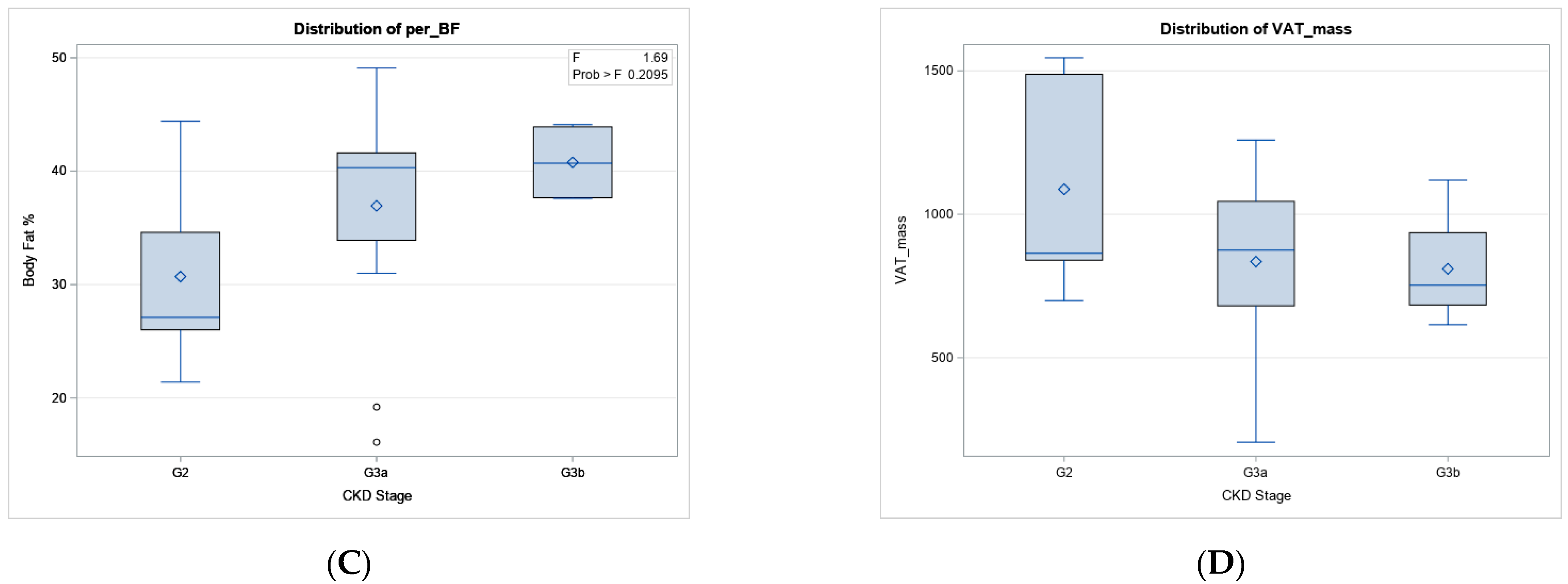
3.1. Differences in Body Composition and CKD Stage
3.2. Exploratory Linear Regression Model
3.3. Correlations between Body Composition Variables, VO2max, and CKD Stage
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Murphy, D.; McCulloch, C.E.; Lin, F.; Banerjee, T.; Bragg-Gresham, J.L.; Eberhardt, M.S.; Morgenstern, H.; Pavkov, M.E.; Saran, R.; Powe, N.R.; et al. Trends in Prevalence of Chronic Kidney Disease in the United States. Ann. Intern. Med. 2016, 165, 473–481. [Google Scholar] [CrossRef] [Green Version]
- Baba, M.; Shimbo, T.; Horio, M.; Ando, M.; Yasuda, Y.; Komatsu, Y.; Masuda, K.; Matsuo, S.; Maruyama, S. Longitudinal Study of the Decline in Renal Function in Healthy Subjects. PLoS ONE 2015, 10, e0129036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saran, A.M.; DuBose, T.D. Cardiovascular disease in chronic kidney disease. Ther. Adv. Cardiovasc. Dis. 2008, 2, 425–434. [Google Scholar] [CrossRef]
- Anderson, T.J. Nitric Oxide, Atherosclerosis and the Clinical Relevance of Endothelial Dysfunction. Heart Fail. Rev. 2003, 8, 71–86. [Google Scholar] [CrossRef]
- Kim, S.; Leng, X.I.; Kritchevsky, S.B. Body Composition and Physical Function in Older Adults with Various Comorbidities. Innov. Aging 2017, 1, igx008. [Google Scholar] [CrossRef] [Green Version]
- Katzmarzyk, P.T.; Church, T.S.; Phd, I.J.; Phd, R.R.; Blair, S.N. Metabolic syndrome, obesity, and mortality: Impact of cardiorespiratory fitness. Diabetes Care 2005, 28, 391–397. [Google Scholar] [CrossRef] [Green Version]
- Dhillon, A.S.; Buckley, D.J.; Ismaeel, A.; Adair, K.; Lowry, C.; Torres, R.; Merrell, H.; Papoutsi, E.; Koutakis, P.; Forsse, J.S. In The Absence of Cardiometabolic Diseases Is Age an Independent Factor in Assessing Renal Health and Function? A Pilot Study: 305. Med. Sci. Sport. Exerc. 2021, 53, 95. [Google Scholar] [CrossRef]
- Cava, E.; Yeat, N.C.; Mittendorfer, B. Preserving Healthy Muscle during Weight Loss. Adv. Nutr. Int. Rev. J. 2017, 8, 511–519. [Google Scholar] [CrossRef] [Green Version]
- Heileson, J.L.; Papadakis, Z.; Ismaeel, A.; Richardson, K.A.; Torres, R.; Funderburk, L.; Gallucci, A.; Koutakis, P.; Forsse, J.S. The Benefits of Utilizing Total Body Composition as a Predictor of Cardiorespiratory Fitness Based on Age: A Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 5758. [Google Scholar] [CrossRef]
- Johansen, K.L.; Lee, C. Body composition in chronic kidney disease. Curr. Opin. Nephrol. Hypertens. 2015, 24, 268–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- George, C.; Matsha, T.E.; Davidson, F.E.; Goedecke, J.H.; Erasmus, R.T.; Kengne, A.P. Chronic Kidney Disease Modifies the Relationship Between Body Fat Distribution and Blood Pressure: A Cross-Sectional Analysis. Int. J. Nephrol. Renov. Dis. 2020, 13, 107–118. [Google Scholar] [CrossRef]
- Formiga, F.; Moreno-González, R.; Corsonello, A.; Carlsson, A.; Ärnlöv, J.; Mattace-Raso, F.; Kostka, T.; Weingart, C.; Roller-Wirnsberger, R.; Tap, L.; et al. Diabetes, sarcopenia and chronic kidney disease; the Screening for CKD among Older People across Europe (SCOPE) study. BMC Geriatr. 2022, 22, 254. [Google Scholar] [CrossRef]
- Rigalleau, V.; Lasseur, C.; Chauveau, P.; Barthes, N.; Raffaitin, C.; Combe, C.; Perlemoine, C.; Baillet-Blanco, L.; Gin, H. Body Composition in Diabetic Subjects with Chronic Kidney Disease: Interest of Bio-Impedance Analysis, and Anthropometry. Ann. Nutr. Metab. 2004, 48, 409–413. [Google Scholar] [CrossRef]
- Shen, F.-C.; Chiu, Y.-W.; Kuo, M.-C.; Lin, M.-Y.; Lee, J.-J.; Hwang, S.-J.; Chang, J.-M.; Hung, C.-C.; Chen, H.-C. U-Shaped Association between Waist-to-Hip Ratio and All-Cause Mortality in Stage 3–5 Chronic Kidney Disease Patients with Body Mass Index Paradox. J. Pers. Med. 2021, 11, 1355. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Solal, M.; Funck-Brentano, T.; Torres, P.U. Bone fragility in patients with chronic kidney disease. Endocr. Connect. 2020, 9, R93–R101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakshi, A.; Singh, K.; Siddhu, A. Body Composition of Chronic Kidney Disease Patients: A Multi-Stage Analysis. J. Ren. Hepatic Disord. 2021, 5, 54–58. [Google Scholar] [CrossRef]
- Lin, T.-Y.; Peng, C.-H.; Hung, S.-C.; Tarng, D.-C. Body composition is associated with clinical outcomes in patients with non–dialysis-dependent chronic kidney disease. Kidney Int. 2018, 93, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Mafra, D.; Guebre-Egziabher, F.; Fouque, D. Body mass index, muscle and fat in chronic kidney disease: Questions about survival. Nephrol. Dial. Transplant. 2008, 23, 2461–2466. [Google Scholar] [CrossRef] [Green Version]
- Jayanama, K.; Putadechakun, S.; Srisuwarn, P.; Vallibhakara, S.A.-O.; Chattranukulchai Shantavasinkul, P.; Sritara, C.; Kantachuvesiri, S.; Komindr, S. Evaluation of Body Composition in Hemodialysis Thai Patients: Comparison between Two Models of Bioelectrical Impedance Analyzer and Dual-Energy X-Ray Absorptiometry. J. Nutr. Metab. 2018, 2018, 4537623. [Google Scholar] [CrossRef] [Green Version]
- Maciejczyk, M.; Więcek, M.; Szymura, J.; Szyguła, Z.; Wiecha, S.; Cempla, J. The Influence of Increased Body Fat or Lean Body Mass on Aerobic Performance. PLoS ONE 2014, 9, e95797. [Google Scholar] [CrossRef]
- Forsse, J.S.; Papadakis, Z.; Peterson, M.N.; Taylor, J.K.; Hess, B.W.; Schwedock, N.; Allison, D.C.; Griggs, J.O.; Wilson, R.L.; Grandjean, P.W. The Influence of an Acute Bout of Aerobic Exercise on Vascular Endothelial Function in Moderate Stages of Chronic Kidney Disease. Life 2022, 12, 91. [Google Scholar] [CrossRef]
- Beddhu, S.; Baird, B.C.; Zitterkoph, J.; Neilson, J.; Greene, T. Physical Activity and Mortality in Chronic Kidney Disease (NHANES III). Clin. J. Am. Soc. Nephrol. 2009, 4, 1901–1906. [Google Scholar] [CrossRef] [Green Version]
- Forsse, J.S.; Peterson, M.N.; Papadakis, Z.; Taylor, J.K.; Hess, B.W.; Schwedock, N.; Allison, D.C.; Griggs, J.O.; Wilson, R.L.; Grandjean, P.W. The Effect of Acute Aerobic Exercise on Biomarkers of Renal Health and Filtration in Moderate-CKD. Res. Q. Exerc. Sport 2023, 1–9. [Google Scholar] [CrossRef] [PubMed]
- El Khoury, C.; Pinti, A.; Lespessailles, E.; Maalouf, G.; Watelain, E.; El Khoury, G.; Berro, A.-J.; Ayoub, M.-L.; Toumi, H.; El Hage, R. Physical Performance Variables and Bone Mineral Density in a Group of Young Overweight and Obese Men. J. Clin. Densitom. 2018, 21, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Bates, D.W.; Black, D.M.; Cummings, S.R. Clinical Use of Bone Densitometry: Clinical Applications. JAMA 2002, 288, 1898. [Google Scholar] [CrossRef] [Green Version]
- Stevens, L.A.; Levey, A.S. Measured GFR as a Confirmatory Test for Estimated GFR. J. Am. Soc. Nephrol. 2009, 20, 2305–2313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forsse, J.S.; Buckley, D.; Ismaeel, A.; Richardson, K.A.; Oliver, A.; Koutakis, P. Effect of Age and Acute-Moderate Intensity Exercise on Biomarkers of Renal Health and Filtration. Biology 2022, 11, 527. [Google Scholar] [CrossRef] [PubMed]
- Tinsley, G.M.; Forsse, J.S.; Morales, E.; Grandjean, P.W. Dual-energy X-ray absorptiometry visceral adipose tissue estimates: Reproducibility and impact of pre-assessment diet. Eur. J. Clin. Nutr. 2017, 72, 609–612. [Google Scholar] [CrossRef] [PubMed]
- Kelly, T.L.; Wilson, K.E.; Heymsfield, S.B. Dual Energy X-ray Absorptiometry Body Composition Reference Values from NHANES. PLoS ONE 2009, 4, e7038. [Google Scholar] [CrossRef] [Green Version]
- Kittiskulnam, P.; Nitesnoppakul, M.; Metta, K.; Suteparuk, S.; Praditpornsilpa, K.; Eiam-Ong, S. Alterations of body composition patterns in pre-dialysis chronic kidney disease patients. Int. Urol. Nephrol. 2020, 53, 137–145. [Google Scholar] [CrossRef]
- Chen, Y.-Y.; Fang, W.-H.; Wang, C.-C.; Kao, T.-W.; Chang, Y.-W.; Yang, H.-F.; Wu, C.-J.; Sun, Y.-S.; Chen, W.-L. Changes of Percent Body Fat as a Useful Surrogate for Risk of Declined Renal Function. Sci. Rep. 2018, 8, 17289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, K.; Zelnick, L.R.; Chertow, G.M.; Himmelfarb, J.; Bansal, N. Body Composition Changes Following Dialysis Initiation and Cardiovascular and Mortality Outcomes in CRIC (Chronic Renal Insufficiency Cohort): A Bioimpedance Analysis Substudy. Kidney Med. 2021, 3, 327–334.e1. [Google Scholar] [CrossRef]
- Watson, S.; Weeks, B.K.; Weis, L.J.; Harding, A.; Horan, S.A.; Beck, B.R. High-Intensity Resistance and Impact Training Improves Bone Mineral Density and Physical Function in Postmenopausal Women with Osteopenia and Osteoporosis: The LIFTMOR Randomized Controlled Trial. J. Bone Miner. Res. 2017, 33, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Lohman, T.; Going, S.; Hall, M.; Ritenbaugh, C.; Bare, L.; Hill, A.; Houtkooper, L.; Aickin, M.; Boyden, T.; Pamenter, R. Effects of resistance training on regional and total bone mineral density in premenopausal women: A randomized prospective study. J. Bone Miner. Res. 2009, 10, 1015–1024. [Google Scholar] [CrossRef]
- JafariNasabian, P.; Inglis, J.E.; Reilly, W.; Kelly, O.; Ilich, J.Z. Aging human body: Changes in bone, muscle and body fat with consequent changes in nutrient intake. J. Endocrinol. 2017, 234, R37–R51. [Google Scholar] [CrossRef] [Green Version]
- McNerny, E.; Nickolas, T.L. Bone Quality in Chronic Kidney Disease: Definitions and Diagnostics. Curr. Osteoporos. Rep. 2017, 15, 207–213. [Google Scholar] [CrossRef]
- Alem, A.M.; Sherrard, D.J.; Gillen, D.L.; Weiss, N.S.; Beresford, S.A.; Heckbert, S.R.; Wong, C.; Stehman-Breen, C. Increased risk of hip fracture among patients with end-stage renal disease. Kidney Int. 2000, 58, 396–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asadipooya, K.; Abdalbary, M.; Ahmad, Y.; Kakani, E.; Monier-Faugere, M.-C.; El-Husseini, A. Bone Quality in CKD Patients: Current Concepts and Future Directions—Part I. Kidney Dis. 2021, 7, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Rysz, J.; Franczyk, B.; Rokicki, R.; Gluba-Brzózka, A. The Influence of Dietary Interventions on Chronic Kidney Disease–Mineral and Bone Disorder (CKD-MBD). Nutrients 2021, 13, 2065. [Google Scholar] [CrossRef] [PubMed]
- Gader, A.G.A. The effect of exercise and nutrition on bone health. J. Musculoskelet. Surg. Res. 2018, 2, 142. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Mean/Median | SD/IQR |
|---|---|---|
| Sample Size (M/F) | 24 (9:15) | |
| eGFR (mL/min/1.73 m2) | 54.38 | 9.04 |
| Age (years) | 62.25 | 9.2 |
| Height (m) | 1.68 | 0.9 |
| Weight (kg) | 83.04 | 16.44 |
| BMI | 28.96 | 4.12 |
| BF (%) | 36.28 | 8.74 |
| SBP (mmHg) | 125.33 | 10.23 |
| DBP (mmHg) * | 82.0 | 78.0, 85.0 |
| HR (bpm) | 70.25 | 11.19 |
| VO2max (mL/kg/min−1) | ||||
|---|---|---|---|---|
| Variables | β | SE | t-Value | p-Value |
| Lean Mass | 0.00026 | 0.000071 | 3.59 | 0.0018 |
| Fat Mass | −0.00024 | 0.000074 | −3.25 | 0.004 |
| BMC | 0.00075 | 0.00128 | 0.59 | 0.5646 |
| Variables | R-Value | p-Value |
|---|---|---|
| Lean mass (g) | 0.74959 | <0.0001 |
| %BF | −0.802 | <0.0001 |
| Fat mass (g) | −0.38403 | 0.0639 |
| VAT mass (g) | −0.01305 | 0.9517 |
| BMC (g) | 0.647 | 0.0006 |
| BMD (g/cm2) | 0.565 | 0.0041 |
| LA-BMD | 0.744 | <0.0001 |
| RA-BMD | 0.57 | 0.0037 |
| L-rib BMD | 0.75 | <0.0001 |
| R-rib BMD * | 0.588 | 0.0025 |
| L-leg BMD * | 0.613 | 0.0014 |
| R-leg BMD * | 0.561 | 0.0044 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forsse, J.S.; Richardson, K.A.; Chapman-Lopez, T.J.; Torres, R.; Heileson, J.L.; Ismaeel, A.; Funderburk, L.; Gallucci, A.R.; Allison, D.C.; Koutakis, P. The Utilization of Body Composition to Predict Cardiorespiratory Fitness and Determine Association with CKD Stage in Individuals with Mid-Spectrum CKD: A Pilot Study. Kidney Dial. 2023, 3, 265-273. https://doi.org/10.3390/kidneydial3030024
Forsse JS, Richardson KA, Chapman-Lopez TJ, Torres R, Heileson JL, Ismaeel A, Funderburk L, Gallucci AR, Allison DC, Koutakis P. The Utilization of Body Composition to Predict Cardiorespiratory Fitness and Determine Association with CKD Stage in Individuals with Mid-Spectrum CKD: A Pilot Study. Kidney and Dialysis. 2023; 3(3):265-273. https://doi.org/10.3390/kidneydial3030024
Chicago/Turabian StyleForsse, Jeffrey S., Kathleen A. Richardson, Tomas J. Chapman-Lopez, Ricardo Torres, Jeffery L. Heileson, Ahmed Ismaeel, LesLee Funderburk, Andrew R. Gallucci, Dale C. Allison, and Panagiotis Koutakis. 2023. "The Utilization of Body Composition to Predict Cardiorespiratory Fitness and Determine Association with CKD Stage in Individuals with Mid-Spectrum CKD: A Pilot Study" Kidney and Dialysis 3, no. 3: 265-273. https://doi.org/10.3390/kidneydial3030024