
Validation of Quantitative Flow Ratio-Derived Virtual Angioplasty with Post-Angioplasty Fractional Flow Reserve—The QIMERA-I Study
 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Methods
2.1. Design and Study Population
2.2. Study Endpoint
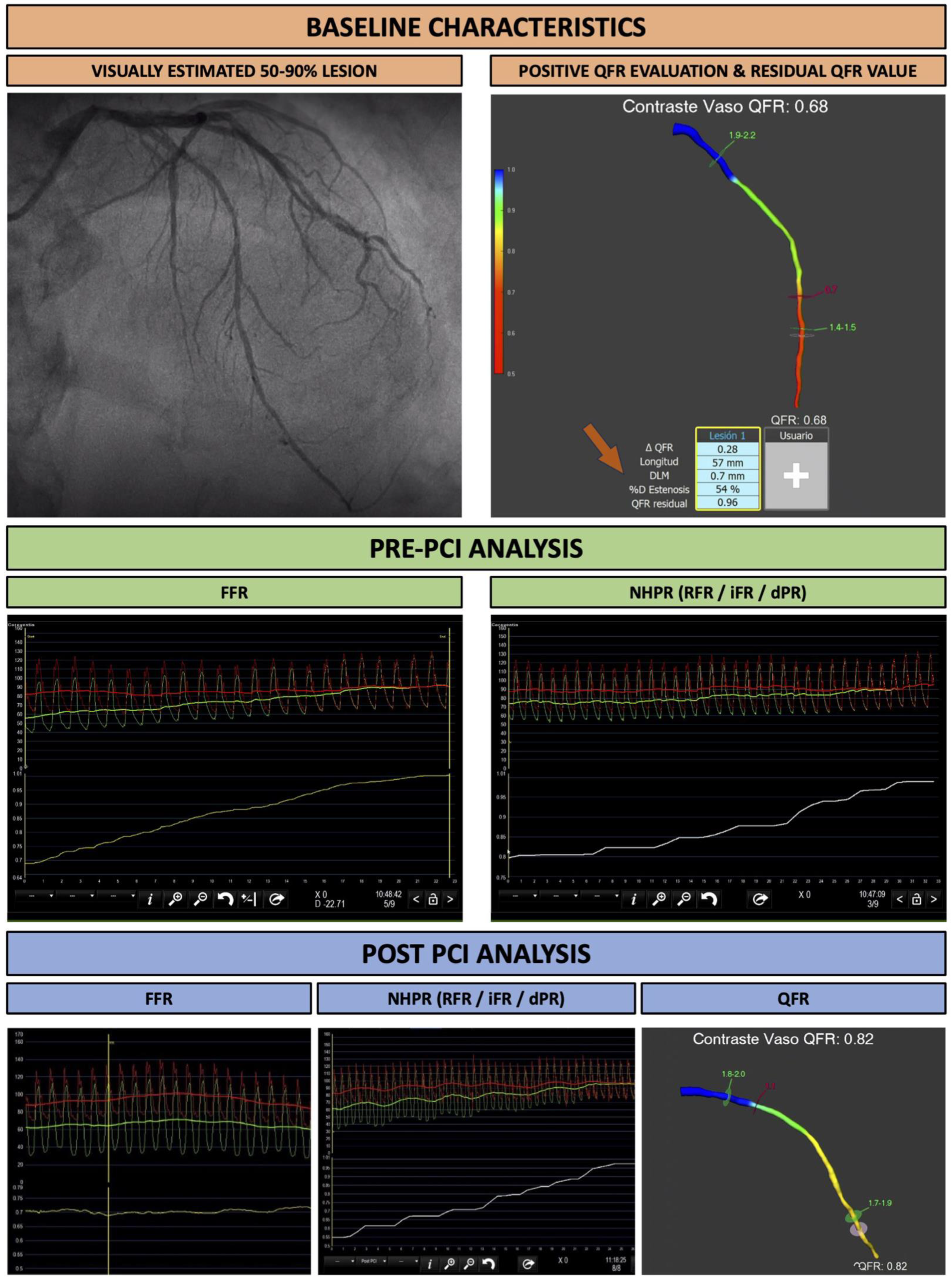
2.3. Quantitative Flow Ratio Analysis
2.4. Hyperemic and Non-Hyperemic Indexes Analysis
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Study Population
3.2. Procedural Characteristics
3.3. Physiological Analysis
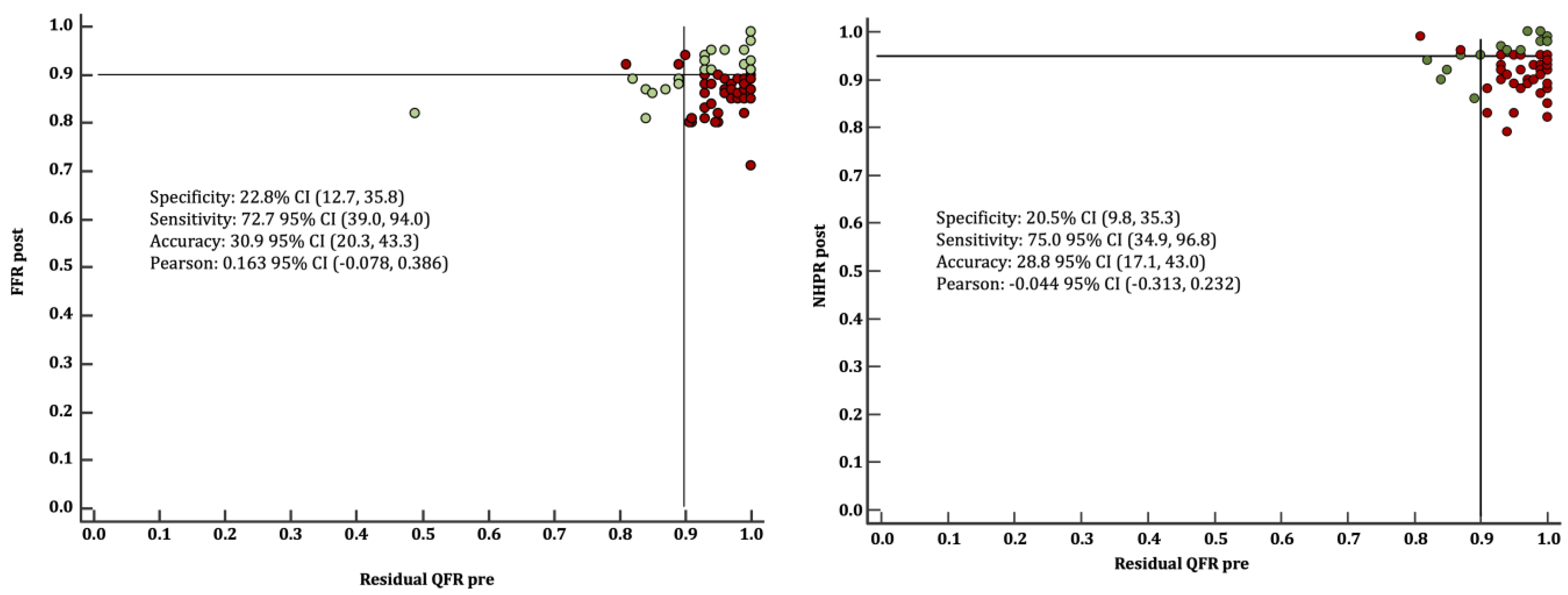
3.4. Correlation between Virtual Angioplasty and Post-PCI FFR, QFR and NHPR
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CAD | Coronary artery disease |
| dPR | Diastolic Resting Pressure Ratio |
| FFR | Fractional Flow Reserve |
| iFR | Instantaneous Wave-free Ratio |
| NPHR | Non-hyperemic pressure ratio |
| NSTEMI | Non-ST-elevation myocardial infarction |
| OMT | Optimal Medical Therapy |
| PCI | Percutaneous coronary intervention |
| QFR | Quantitative Flow Ratio |
| RFR | Resting Full-cycle Ratio |
| STEMI | ST-elevation myocardial infarction |
References
- Ahn, J.M.; Park, D.W.; Shin, E.S.; Koo, B.K.; Nam, C.W.; Doh, J.H.; Kim, J.H.; Chae, I.H.; Yoon, J.H.; Her, S.H.; et al. IRIS-FFR Investigators. Fractional flow reserve and cardiac events in coronary artery disease: Data from a prospective IRIS-FFR Registry (Interventional Cardiology Research In cooperation Society Fractional Flow Reserve). Circulation 2017, 135, 2241–2251. [Google Scholar] [CrossRef]
- Tonino, P.A.L.; De Bruyne, B.; Pijls, N.H.J.; Siebert, U.; Ikeno, F.; van’t Veer, M.; Klauss, V.; Manoharan, G.; Engstrøm, T.; Oldroyd, K.G.; et al. Fractional Flow Reserve versus Angiography for Guiding Percutaneous Coronary Intervention. N. Engl. J. Med. 2009, 360, 213–224. [Google Scholar] [CrossRef]
- De Bruyne, B.; Pijls, N.H.J.; Kalesan, B.; Barbato, E.; Tonino, P.A.; Piroth, Z.; Jagic, N.; Mobius-Winckler, S.; Rioufol, G.; Witt, N.; et al. Fractional Flow Reserve–Guided PCI versus Medical Therapy in Stable Coronary Disease. N. Engl. J. Med. 2012, 367, 991–1001. [Google Scholar] [CrossRef] [PubMed]
- Bech, G.J.; De Bruyne, B.; Pijls, N.H.J.; de Muinck, E.D.; Hoorntje, J.C.; Escaned, J.; Stella, P.R.; Boersma, E.; Bartunek, J.; Koolen, J.J.; et al. Fractional Flow Reserve to Determine the Appropriateness of Angioplasty in Moderate Coronary Stenosis. Circulation 2001, 103, 2928–2934. [Google Scholar] [CrossRef]
- Pijls, N.H.; van Schaardenburgh, P.; Manoharan, G.; Boersma, E.; Bech, J.-W.; Veer, M.V.; Bär, F.; Hoorntje, J.; Koolen, J.; Wijns, W.; et al. Percutaneous coronary intervention of functionally nonsignificant stenosis: 5-year follow-up of the DEFER Study. J. Am. Coll. Cardiol. 2007, 49, 2105–2111. [Google Scholar] [CrossRef]
- Adjedj, J.; De Bruyne, B.; Flore, V.; Di Gioia, G.; Ferrara, A.; Pellicano, M.; Toth, G.G.; Bartunek, J.; Vanderheyden, M.; Heyndrickx, G.R.; et al. Significance of intermediate values of fractional flow reserve in patients with coronary artery disease. Circulation 2016, 133, 502–508. [Google Scholar] [CrossRef]
- Götberg, M.; Christiansen, E.H.; Gudmundsdottir, I.J.; Sandhall, L.; Danielewicz, M.; Jakobsen, L.; Olsson, S.-E.; Öhagen, P.; Olsson, H.; Omerovic, E.; et al. Instantaneous Wave-free Ratio versus Fractional Flow Reserve to Guide PCI. N. Engl. J. Med. 2017, 376, 1813–1823. [Google Scholar] [CrossRef]
- Davies, J.E.; Sen, S.; Dehbi, H.M.; Al-Lamee, R.; Petraco, R.; Nijjer, S.S.; Bhindi, R.; Lehman, S.J.; Walters, D.; Sapontis, J.; et al. Use of the instantaneous wave-free ratio or fractional flow reserve in PCI. N. Engl. J. Med. 2017, 376, 1824–1834. [Google Scholar] [CrossRef]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.-P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef]
- Toth, G.G.; Toth, B.; Johnson, N.P.; De Vroey, F.; Di Serafino, L.; Pyxaras, S.; Rusinaru, D.; Di Gioia, G.; Pellicano, M.; Barbato, E.; et al. Revascularization decisions in patients with stable angina and intermediate lesions: Results of the international survey on interventional strategy. Circ. Cardiovasc. Interv. 2014, 7, 751–759. [Google Scholar] [CrossRef]
- Härle, T.; Zeymer, U.; Hochadel, M.; Zahn, R.; Kerber, S.; Zrenner, B.; Schächinger, V.; Lauer, B.; Runde, T.; Elsässer, A. Real-world use of fractional flow reserve in Germany: Results of the prospective ALKK coronary angiography and PCI registry. Clin. Res. Cardiol. 2017, 106, 140–150. [Google Scholar] [CrossRef]
- Ojeda, S.; Romaguera, R.; Cruz-González, I.; Moreno, R. Spanish Cardiac Catheterization and Coronary Intervention Registry. 29th Official Report of the Interventional Cardiology Association of the Spanish Society of Cardiology (1990–2019). Rev. Esp. Cardiol. 2020, 73, 927–936. [Google Scholar] [CrossRef]
- Tu, S.; Westra, J.; Yang, J.; von Birgelen, C.; Ferrara, A.; Pellicano, M.; Nef, H.; Tebaldi, M.; Murasato, Y.; Lansky, A.; et al. Diagnostic Accuracy of Fast Computational Approaches to Derive Fractional Flow Reserve From Diagnostic Coronary Angiography: The International Multicenter FAVOR Pilot Study. Cardiovasc. Interv. 2016, 9, 2024–2035. [Google Scholar]
- Van Rosendael, A.R.; Koning, G.; Dimitriu-Leen, A.C.; Smit, J.M.; Montero-Cabezas, J.M.; van der Kley, F.; Jukema, J.W.; Reiber, J.H.C.; Bax, J.J.; Scholte, A.J.H.A. Accuracy and reproducibility of fast fractional flow reserve computation from invasive coronary angiography. Int. J. Cardiovasc. Imaging 2017, 33, 1305. [Google Scholar] [CrossRef]
- Yazaki, K.; Otsuka, M.; Kataoka, S.; Kahata, M.; Kumagai, A.; Inoue, K.; Koganei, H.; Enta, K.; Ishii, Y. Applicability of 3-Dimensional Quantitative Coronary Angiography-Derived Computed Fractional Flow Reserve for Intermediate Coronary Stenosis. Circ. J. 2017, 81, 988–992. [Google Scholar] [CrossRef]
- Westra, J.; Tu, S.; Winther, S.; Nissen, L.; Vestergaard, M.B.; Andersen, B.K.; Holck, E.N.; Fox Maule, C.; Johansen, J.K.; Andreasen, L.N.; et al. Evaluation of Coronary Artery Stenosis by Quantitative Flow Ratio during Invasive Coronary Angiography: The WIFI II Study (Wire-Free Functional Imaging II). Circ. Cardiovasc. Imaging 2018, 11, e007107. [Google Scholar] [CrossRef]
- Westra, J.; Andersen, B.K.; Campo, G.; Matsuo, H.; Koltowski, L.; Eftekhari, A.; Liu, T.; Di Serafino, L.; Di Girolamo, D.; Escaned, J.; et al. Diagnostic Performance of In-Procedure Angiography-Derived Quantitative Flow Reserve Compared to Pressure-Derived Fractional Flow Reserve: The FAVOR II Europe-Japan Study. J. Am. Heart Assoc. 2018, 7, e009603. [Google Scholar] [CrossRef]
- Cortés, C.; Carrasco-Moraleja, M.; Aparisi, A.; Rodriguez-Gabella, T.; Campo, A.; Gutiérrez, H.; Julca, F.; Gómez, I.; San Román, J.A.; Amat-Santos, I.J. Quantitative flow ratio-Meta-analysis and systematic review. Catheter. Cardiovasc. Interv. 2021, 97, 807–814. [Google Scholar] [CrossRef]
- Rimac, G.; Fearon, W.F.; De Bruyne, B.; Ikeno, F.; Matsuo, H.; Piroth, Z.; Costerousse, O.; Bertrand, O.F. Clinical value of post-percutaneous coronary intervention fractional flow reserve value: A systematic review and meta-analysis. Am. Heart J. 2017, 183, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Azzalini, L.; Poletti, E.; Demir, O.M.; Ancona, M.B.; Mangieri, A.; Giannini, F.; Carlino, M.; Chieffo, A.; Montorfano, M.; Colombo, A.; et al. Impact of Post-Percutaneous Coronary Intervention Fractional Flow Reserve Measurement on Procedural Management and Clinical Outcomes: The REPEAT-FFR Study. J. Invasive Cardiol. 2019, 31, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Kikuta, Y.; Cook, C.M.; Sharp, A.S.P.; Salinas, P.; Kawase, Y.; Shiono, Y.; Giavarini, A.; Nakayama, M.; De Rosa, S.; Sen, S.; et al. Pre-Angioplasty Instantaneous Wave-Free Ratio Pullback Predicts Hemodynamic Outcome In Humans With Coronary Artery Disease: Primary Results of the International Multicenter iFR GRADIENT Registry. JACC Cardiovasc. Interv. 2018, 11, 757–767. [Google Scholar] [CrossRef]
- Zimmermann, F.; Ferrara, A.; Johnson, N.P.; Van Nunen, L.X.; Escaned, J.; Albertsson, P.; Erbel, R.; Legrand, V.; Gwon, H.C.; Remkes, W.S.; et al. Deferral vs. performance of percutaneous coronary intervention of functionally non-significant coronary stenosis: 15-year follow-up of the DEFER trial. Eur. Heart J. 2015, 36, 3182–3188. [Google Scholar] [CrossRef] [PubMed]
- Xaplanteris, P.; Fournier, S.; Pijls, N.; Fearon, W.F.; Barbato, E.; Tonino, P.A.; Engstrøm, T.; Kääb, S.; Dambrink, J.-H.; Rioufol, G.; et al. Five-Year Outcomes with PCI Guided by Fractional Flow Reserve. N. Engl. J. Med. 2018, 379, 250–259. [Google Scholar] [CrossRef] [PubMed]
- Collison, D.; Didagelos, M.; Aetesam-ur-Rahman, M.; Copt, S.; McDade, R.; McCartney, P.; Ford, T.J.; McClure, J.; Lindsay, M.; Shaukat, A.; et al. Post-stenting fractional flow reserve vs coronary angiography for optimization of percutaneous coronary intervention (TARGET-FFR). Eur. Heart J. 2021, 42, 4656–4668. [Google Scholar] [CrossRef] [PubMed]
- Jeremias, A.; Davies, J.E.; Akiko Maehara, A.; Matsumura, M.; Schneider, J.; Tang, K.; Talwar, S.; Marques, K.; Shammas, N.W.; Gruberg, L.; et al. Blinded Physiological Assessment of Residual Ischemia after Successful Angiographic Percutaneous Coronary Intervention: The DEFINE PCI Study. JACC Cardiovasc. Interv. 2019, 12, 1991–2001. [Google Scholar] [CrossRef] [PubMed]
- Hwang, D.; Koo, B.K.; Zhang, J.; Park, J.; Yang, S.; Kim, M.; Yun, J.P.; Lee, J.M.; Nam, C.W.; Shin, E.S.; et al. Prognostic Implications of Fractional Flow Reserve After Coronary Stenting: A Systematic Review and Meta-analysis. JAMA Netw. Open 2022, 5, e2232842. [Google Scholar] [CrossRef] [PubMed]
- Biscaglia, S.; Tebaldi, M.; Brugaletta, S.; Cerrato, E.; Erriquez, A.; Passarini, G.; Ielasi, A.; Spitaleri, G.; Di Girolamo, D.; Mezzapelle, G.; et al. Prognostic Value of QFR Measured Immediately After Successful Stent Implantation: The International Multicenter Prospective HAWKEYE Study. JACC Cardiovasc. Interv. 2019, 12, 2079–2088. [Google Scholar] [CrossRef]
- Terentes-Printzios, D.; Gkini, K.P.; Oikonomou, D.; Gardikioti, V.; Aznaouridis, K.; Dima, I.; Tsioufis, K.; Vlachopoulos, C. Prognostic Value of Post-PCI Angiography-Derived Fractional Flow Reserve: A Systematic Review and Meta-Analysis of Cohort Studies. J. Pers. Med. 2023, 13, 1251. [Google Scholar] [CrossRef]
- Cheng, H.; Hong, L.; Xi, G.; Wang, H.; Hu, J.; Liu, Q.; Yang, L. Prognostic value of quantitative flow ratio in patients with coronary heart disease after percutaneous coronary intervention therapy: A meta-analysis. Front. Cardiovasc. Med. 2023, 10, 1164290. [Google Scholar] [CrossRef]
- Mizukami, T.; Sonck, J.; Sakai, K.; Ko, B.; Maeng, M.; Otake, H.; Koo, B.; Nagumo, S.; Nørgaard, B.L.; Leipsic, J.; et al. Procedural Outcomes after Percutaneous Coronary Interventions in Focal and Diffuse Coronary Artery Disease. J. Am. Heart Assoc. 2022, 11, e026960. [Google Scholar] [CrossRef]
- Biscaglia, S.; Verardi, F.M.; Tebaldi, M.; Guiducci, V.; Caglioni, S.; Campana, R.; Scala, A.; Marrone, A.; Pompei, G.; Marchini, F.; et al. QFR-Based Virtual PCI or Conventional Angiography to Guide PCI: The AQVA Trial. Cardiovasc. Interv. 2023, 16, 783–794. [Google Scholar]
- Rubimbura, V.; Guillon, B.; Fournier, S.; Amabile, N.; Pan, C.C.; Combaret, N.; Eeckhout, E.; Kibler, M.; Silvain, J.; Wijns, W.; et al. Quantitative flow ratio virtual stenting and post stenting correlations to post stenting fractional flow reserve measurements from the DOCTORS (does optical coherence tomography optimize results of stenting) study population. Catheter. Cardiovasc. Interv. 2020, 96, 1145–1153. [Google Scholar] [CrossRef] [PubMed]
- Van Diemen, P.A.; De Winter, R.W.; Schumacher, S.P.; Bom, M.J.; Driessen, R.S.; Everaars, H.; Jukema, R.A.; Somsen, Y.B.; Popelkova, L.; van de Ven, P.M.; et al. Residual Quantitative Flow Ratio to Estimate Post-Percutaneous Coronary Intervention Fractional Flow Reserve. J. Interv. Cardiol. 2021, 2021, 4339451. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.Y.; Hwang, B.H.; Kim, M.J.; Choo, E.H.; Choi, I.J.; Kim, C.J.; Lee, S.W.; Lee, J.M.; Kim, M.J.; Jeon, D.S.; et al. Influence of lesion and disease subsets on the diagnostic performance of the quantitative flow ratio in real-world patients. Sci. Rep. 2021, 11, 2995. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Baseline Characteristics | Global Study Population (N = 84) | |
|---|---|---|
| Age—years | 65.52 ± 10.87 | |
| Gender (female)—no. (%) | 14 (17) | |
| Hypertension—no. (%) | 59 (83) * | |
| Dyslipidemia—no. (%) | 55 (89) * | |
| Diabetes mellitus—no. (%) | 28 (78) * | |
| Smoking—no. (%) | 42 (50) | |
| Chronic kidney disease—no. (%) | 11 (29) * | |
| Creatinine (mg/dL) | 0.89 (0.76–1.12) | |
| Dyalisis—no. (%) | 1 (4) * | |
| Prior MI—no. (%) | 19 (50) * | |
| LVEF (%) | 57 (46–60) | |
| Peak Troponin (ui/mL) | 805 (135–4000) | |
| Prior PCI—no. (%) | 31 (65) * | |
| Peripheral artery disease—no. (%) | 4 (14) * | |
| Clinical presentation—no. (%) | ||
| Stable angina | 32 (38) | |
| Unstable angina | 11 (13) | |
| Non-ST-elevated MI | 33 (39) | |
| LVEF deterioration | 8 (10) | |
| Medications | ||
| Aspirin | 81 (96) * | |
| Ticagrelor | 28 (33) * | |
| Clopidogrel | 47 (56) * | |
| Prasugrel | 7 (8) * | |
| Direct oral anticoag. | 7 (8) * | |
| Warfarine | 1 (1) * | |
| Killip Kimball | ||
| I–II | 46 (92) * | |
| III–IV | 4 (8) *^ | |
| CCS class | ||
| I | 9 (36) * | |
| II | 14 (56) * | |
| III | 2 (8) * | |
| Baseline Characteristics | Global Study Population (N = 84) | |
|---|---|---|
| Vascular access | ||
| Radial | 78 (92) | |
| Femoral | 5 (5) | |
| Cubital | 1 (1) | |
| Procedural duration (min) | 69 (52–86) | |
| Contrast dose | 239.5 (178–280) | |
| Fluoroscopy dose | 98 (55–1383) | |
| Fluoroscopy time | 17.43 (12–26) | |
| Target lesion ^ | ||
| Left anterior descending | 48 (69) * | |
| Circumflex | 11 (16) * | |
| Right coronary artery | 11 (16) * | |
| Left main | 3 (4) * | |
| Diameter reference | 2.82 ± 0.41 | |
| Lesion characteristics | ||
| Stenosis diameter (%) | 60 (52–70) | |
| Length (mm) | 20 (14–31) | |
| Number of lesions | ||
| 1 | 45 (59) * | |
| 2 | 25 (33) * | |
| 3 | 4 (5) * | |
| Type of lesion ° | ||
| Calcified | 8 (9) | |
| Sequential | 7 (8) | |
| Bifurcation | 55 (59) | |
| NHPR indexes used | ||
| RFR | 36 (46.8) | |
| DPR | 16 (20.8) | |
| iFR | 25 (32.5) | |
| Number of implanted stents | 1.17 ± 0.46 | |
| 0 | 1 (1) | |
| 1 | 72 (78) | |
| 2 | 12 (13) | |
| 3 | 2 (2) | |
| Stent diameter (mm) | 2.93 ± 0.45 | |
| Stent length (mm) | 27 (19–35) | |
| Baseline | Post-PCI | |
|---|---|---|
| QFR | 0.69 ± 0.12 | 0.95 ± 0.05 |
| Residual QFR | 0.95 ± 0.07 | / |
| Hyperaemic index | ||
| FFR | 0.73 ± 0.08 | 0.87 ± 0.05 |
| Non-hyperaemic indexes | ||
| NHPR | 0.82 ± 0.11 | 0.92 ± 0.05 |
| Lin’s CCC | Pearson ρ | p-Value | ||
|---|---|---|---|---|
| Residual QFR | QFR post | 0.050 (−0.150, 0.246) | 0.058 (−0.175, 0.284) | 0.627 |
| FFR post | 0.090 (−0.044, 0.221) | 0.163 (−0.078, 0.386) | 0.185 | |
| NHPR post | −0.035 (−0.255, 0.187) | −0.044 (−0.313, 0.232) | 0.757 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amat-Santos, I.J.; Marengo, G.; Sánchez-Luna, J.P.; Cortés Villar, C.; Rivero Crespo, F.; Jiménez Díaz, V.A.; de la Torre Hernández, J.M.; Pérez de Prado, A.; Sabaté, M.; López-Palop, R.; et al. Validation of Quantitative Flow Ratio-Derived Virtual Angioplasty with Post-Angioplasty Fractional Flow Reserve—The QIMERA-I Study. J. Cardiovasc. Dev. Dis. 2024, 11, 14. https://doi.org/10.3390/jcdd11010014
Amat-Santos IJ, Marengo G, Sánchez-Luna JP, Cortés Villar C, Rivero Crespo F, Jiménez Díaz VA, de la Torre Hernández JM, Pérez de Prado A, Sabaté M, López-Palop R, et al. Validation of Quantitative Flow Ratio-Derived Virtual Angioplasty with Post-Angioplasty Fractional Flow Reserve—The QIMERA-I Study. Journal of Cardiovascular Development and Disease. 2024; 11(1):14. https://doi.org/10.3390/jcdd11010014
Chicago/Turabian StyleAmat-Santos, Ignacio J., Giorgio Marengo, Juan Pablo Sánchez-Luna, Carlos Cortés Villar, Fernando Rivero Crespo, Víctor Alfonso Jiménez Díaz, José María de la Torre Hernández, Armando Pérez de Prado, Manel Sabaté, Ramón López-Palop, and et al. 2024. "Validation of Quantitative Flow Ratio-Derived Virtual Angioplasty with Post-Angioplasty Fractional Flow Reserve—The QIMERA-I Study" Journal of Cardiovascular Development and Disease 11, no. 1: 14. https://doi.org/10.3390/jcdd11010014