
Embolization of Perforated Coronary Artery with a Fragment of Balloon Catheter (Cut Balloon Technique)—Multicenter Study

 ,
,  , , and
, , and 
Abstract
:1. Introduction
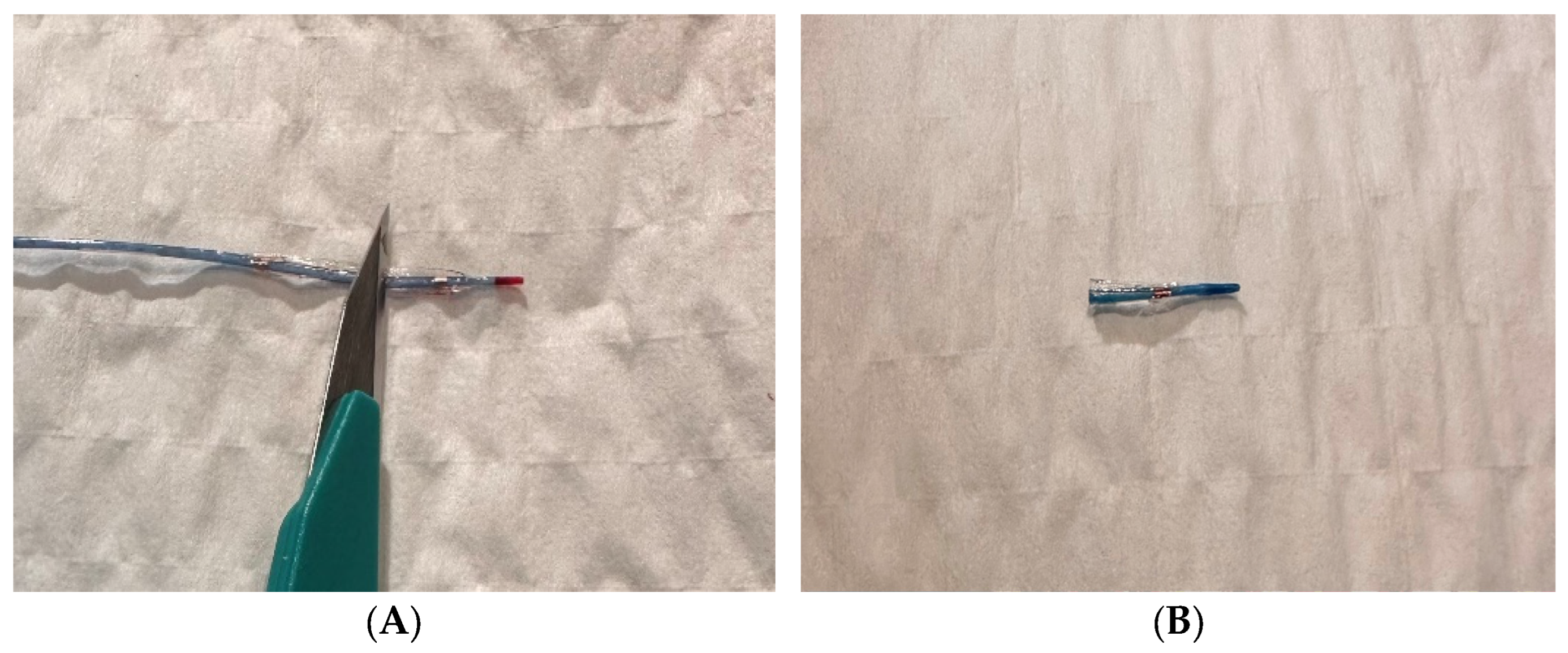
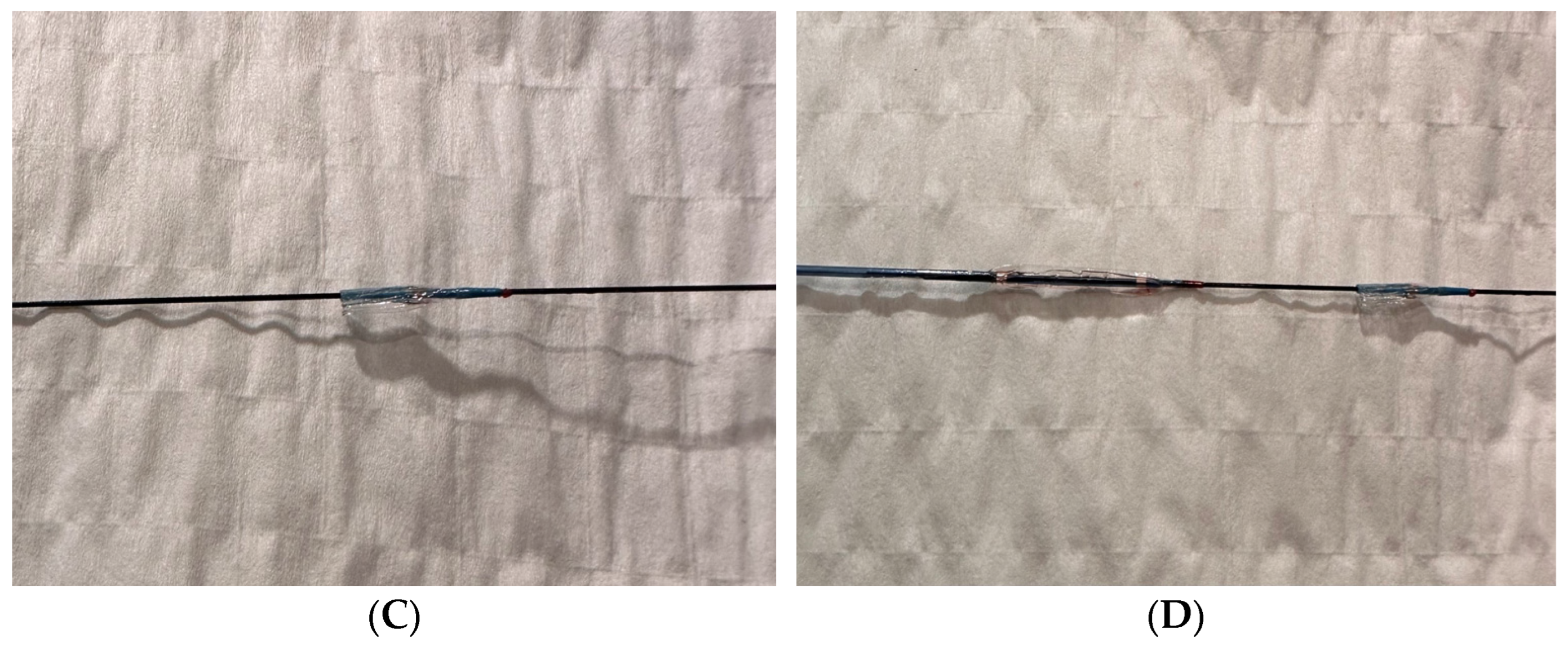
2. Methods
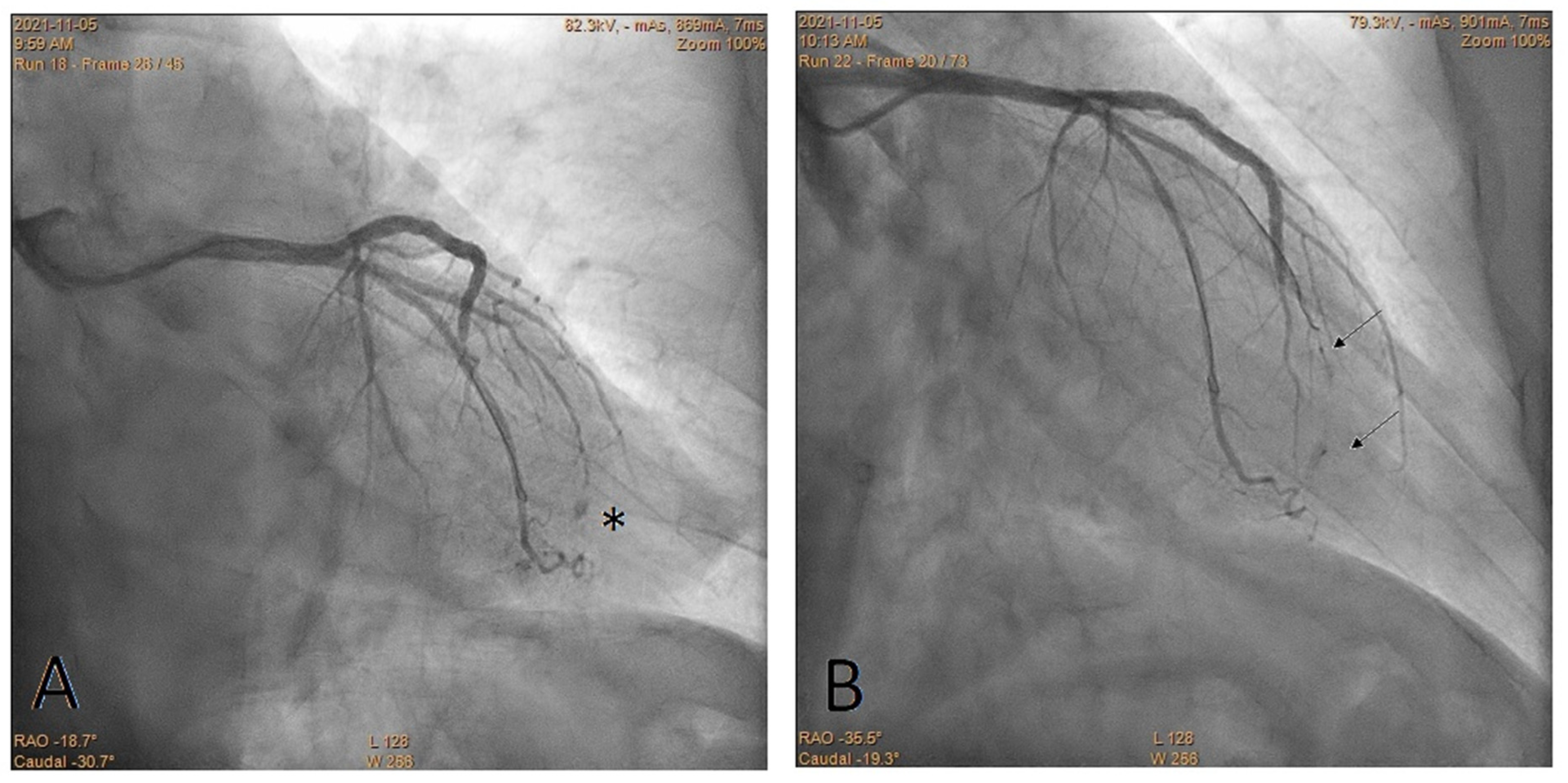
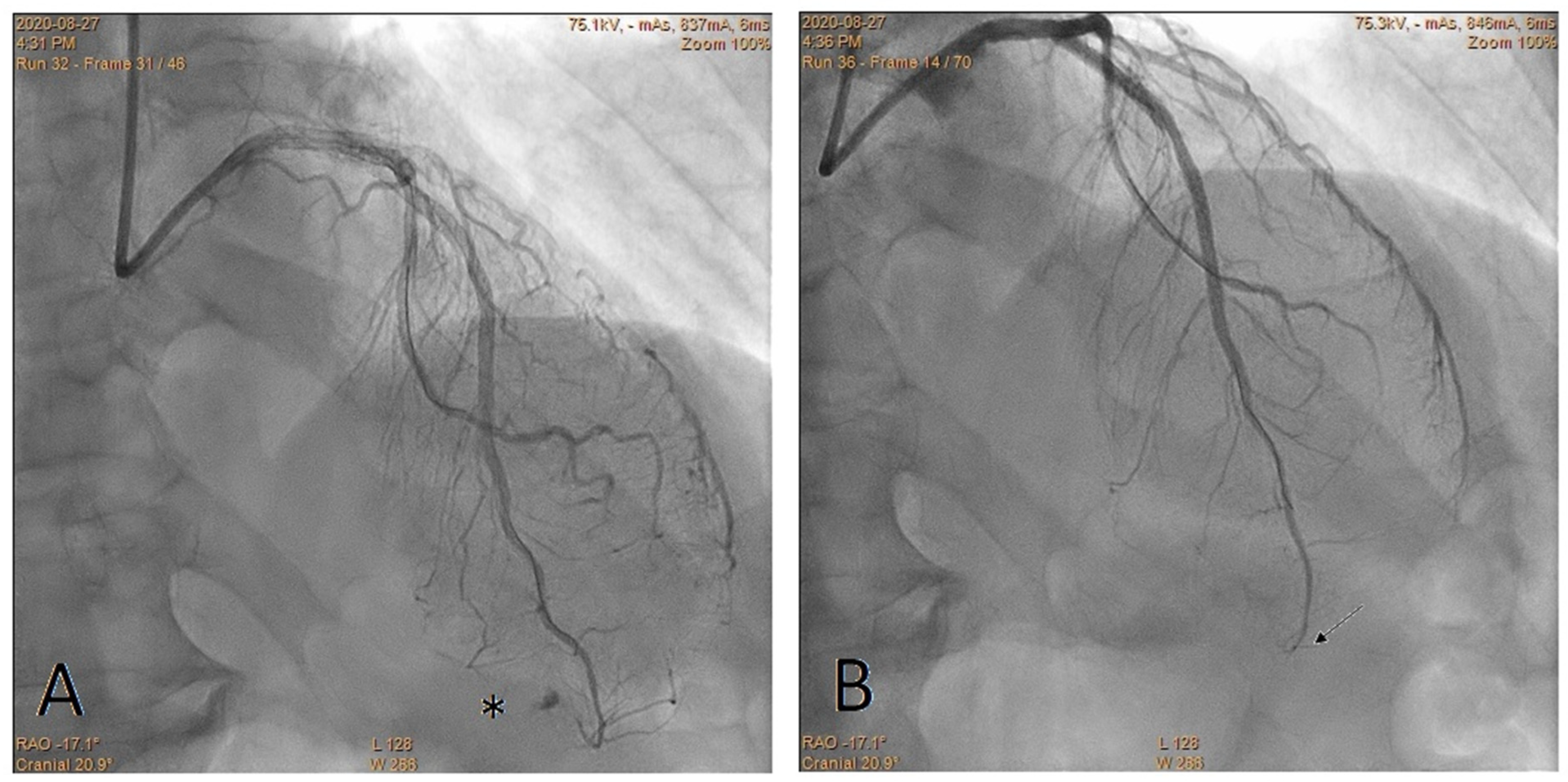
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brilakis, E. Manual of Coronary Chronic Total Occlusion Interventions: A Step-by-Step Approach, 2nd ed.; Elsevier: Cambridge, MA, USA, 2017. [Google Scholar]
- Ellis, S.G.; Ajluni, S.; Arnold, A.Z.; Popma, J.J.; Bittl, J.A.; Eigler, N.L.; Cowley, M.J.; Raymond, R.E.; Safian, R.D.; Whitlow, P.L. Increased coronary perforation in the new device era. Incidence, classification, management, and outcome. Circulation 1994, 90, 2725–2730. [Google Scholar] [CrossRef] [PubMed]
- Teis, A.; Fernández-Nofrerías, E.; Rodríguez-Leor, O.; Tizón, H.; Salvatella, N.; Valle, V.; Mauri, J. Coronary artery perforation by intracoronary guide wires: Risk factors and clinical outcomes. Rev. Esp. Cardiol. 2010, 63, 730–734, Erratum in Rev. Esp. Cardiol. 2010, 63, 1516. Teis-Soley, Albert [corrected to Teis, Albert]. [Google Scholar] [CrossRef] [PubMed]
- Shaukat, A.; Tajti, P.; Sandoval, Y.; Stanberry, L.; Garberich, R.; Nicholas Burke, M.; Gössl, M.; Henry, T.; Mooney, M.; Sorajja, P.; et al. Incidence, predictors, management and outcomes of coronary perforations. Catheter. Cardiovasc. Interv. 2019, 93, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Abdalwahab, A.; Farag, M.; Brilakis, E.S.; Galassi, A.R.; Egred, M. Management of Coronary Artery Perforation. Cardiovasc. Revasc. Med. 2021, 26, 55–60. [Google Scholar] [CrossRef] [PubMed]
- He, L.Y.; Han, J.L.; Guo, L.J.; Zhang, F.C.; Cui, M.; Gao, W. Effect of transcatheter embolization by autologous fat particles in the treatment of coronary artery perforation during percutaneous coronary intervention. Chin. Med. J. 2015, 128, 745–749. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S.; Nishigaki, K.; Ojio, S.; Yasuda, S.; Okubo, M.; Yamaki, T.; Kubota, T.; Takasugi, N.; Ishihara, Y.; Kawasaki, M.; et al. Transcatheter embolization by autologous blood clot is useful management for small side branch perforation due to percutaneous coronary intervention guide wire. J. Cardiol. 2008, 52, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Hachinohe, D.; Kashima, Y.; Okada, Y.; Kanno, D.; Kobayashi, K.; Kaneko, U.; Sugie, T.; Tadano, Y.; Watanabe, T.; Shitan, H.; et al. Coil Embolization for Coronary Artery Perforation: A Retrospective Analysis of 110 Patients. J. Interv. Cardiol. 2021, 2021, 9022326. [Google Scholar] [CrossRef] [PubMed]
- Sobieszek, G.; Zięba, B. Balloon Fragment Technique Used to Close Distal Coronary Vessel Perforation. J. Invasive Cardiol. 2020, 32, E370–E372. [Google Scholar] [PubMed]
- Brilakis, E.S.; Karmpaliotis, D.; Patel, V.; Banerjee, S. Complications of Chronic Total Occlusion Angioplasty. Interv. Cardiol. Clin. 2012, 1, 373–389. [Google Scholar] [CrossRef] [PubMed]
- Kearns, M.J.; Walley, K.R. Tamponade: Hemodynamic and Echocardiographic Diagnosis. Chest 2018, 153, 1266–1275. [Google Scholar] [CrossRef] [PubMed]
- Theuerle, J.; Yudi, M.B.; Farouque, O.; Andrianopoulos, N.; Scott, P.; Ajani, A.E.; Brennan, A.; Duffy, S.J.; Reid, C.M.; Clark, D.J.; et al. Utility of the ACC/AHA lesion classification as a predictor of procedural, 30-day and 12-month outcomes in the contemporary percutaneous coronary intervention era. Catheter. Cardiovasc. Interv. 2018, 92, E227–E234. [Google Scholar] [CrossRef] [PubMed]
- Qin, Q.; Chang, S.; Xu, R.; Fu, M.; Chen, L.; Ge, L.; Qian, J.; Ma, J.; Ge, J. Short and long-term outcomes of coronary perforation managed by coil embolization: A single-center experience. Int. J. Cardiol. 2020, 298, 18–21. [Google Scholar] [CrossRef] [PubMed]
- Cerrato, E.; Pavani, M.; Barbero, U.; Colombo, F.; Mangieri, A.; Ryan, N.; Quadri, G.; Tomassini, F.; Presutti, D.G.; Calcagno, S.; et al. Incidence, Management, Immediate and Long-Term Outcome of Guidewire and Device Related Grade III Coronary Perforations (from G3CAP-Cardiogroup VI Registry). Am. J. Cardiol. 2021, 143, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Öcal, L.; Yılmaz, C.; Uysal, S.; Cerşit, S.; Zehir, R. Successful management of distal coronary artery perforation with the modified cut balloon technique during percutaneous coronary intervention. Anatol. J. Cardiol. 2022, 26, 66–68. [Google Scholar] [CrossRef] [PubMed]
- Alavi, S.H.; Hassanzadeh, M.; Dehghani, P.; Mehdipour Namdar, Z.; Aslani, A. A Novel Technique for Managing Guidewire-Induced Distal Coronary Perforation Using Coronary Balloon Pieces. JACC Case Rep. 2022, 4, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Abdalwahab, A.; McQuillan, C.; Farag, M.; Egred, M. Novel economic treatment for coronary wire perforation: A case report. World J. Cardiol. 2021, 13, 177–182. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CBT n = 26 | |
|---|---|
| Age, years | 71 ± 10.6 |
| ≥80 | 7 (27%) |
| Male | 18 (69%) |
| Acute coronary syndrome | 15 (58%) |
| STEMI | 4 (16%) |
| NSTEMI/UA | 11 (42%) |
| Chronic coronary syndrome | 11 (42%) |
| Previous MI | 9 (35%) |
| Previous PCI | 9 (35%) |
| Previous CABG | 0 |
| Diabetes | 7 (27%) |
| CBT n = 26 | |
|---|---|
| PCI type | |
| CTO | 3 (11%) |
| Non-CTO | 23 (89%) |
| Target vessel for PCI | |
| Left main coronary artery | 2 (8%) |
| Left anterior descending artery | 11 (42%) |
| Circumflex artery | 7 (27%) |
| Right coronary artery | 6 (23%) |
| ACC/AHA lesion classification | |
| A | 7 (27%) |
| B1 | 8 (31%) |
| B2 | 8 (31%) |
| C | 3 (11%) |
| Perforated coronary artery | |
| Left anterior descending artery | 9 (34%) |
| Diagonal branch | 2 (8%) |
| Intermediate branch | 1 (4%) |
| Obtuse marginal branch | 7 (27%) |
| Right posterolateral artery | 4 (15%) |
| Right posterior descending artery | 2 (8%) |
| Septal collateral | 1 (4%) |
| Device responsible for distal/septal collateral perforation | |
| Non-hydrophilic guidewire | 23 (88%) |
| Hydrophilic guidewire | 2 (8%) |
| Microcatheter | 1 (4%) |
| Number of guidewires used during procedure | |
| 1 | 10 (39%) |
| 2 | 12 (46%) |
| ≥3 | 4 (15%) |
| Clinical management | |
| Pericardiocentesis | 4 (16%) |
| Protamine | 0 |
| Prolonged balloon inflation | 25 (100%) |
| Number of balloons used to close the perforation | |
| 1 | 12 (46%) |
| 2 | 6 (23%) |
| 3 | 5 (19%) |
| 4 | 1 (4%) |
| 5 | 2 (8%) |
| In-hospital prognosis | |
| Cardiac tamponade | 4 (16%) |
| Emergency surgery | 0 |
| Death | 0 |
| Embolization Techniques | Advantages | Disadvantages |
|---|---|---|
| Coils | reliable treatment effect | high cost, need for special (delivery and release) equipment, limited operator experience |
| CBT | high availability, low cost, simplicity, no need for special (delivery) equipment, potentially repeatable if unsuccessful | constrained deliverability |
| Thrombin | low cost | limited operator experience, need for special (delivery) equipment, limited availability |
| Fat | high availability, cost-free | limited operator experience, need for special (delivery) equipment, uncertain effects, limited data in the literature |
| Clot | high availability, cost-free | limited operator experience, need for special (delivery) equipment, uncertain effects, limited data in the literature |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sobieszek, G.; Zięba, B.; Dworzański, W.; Celiński, R.; Barbero, U.; Opolski, M.P. Embolization of Perforated Coronary Artery with a Fragment of Balloon Catheter (Cut Balloon Technique)—Multicenter Study. J. Cardiovasc. Dev. Dis. 2023, 10, 496. https://doi.org/10.3390/jcdd10120496
Sobieszek G, Zięba B, Dworzański W, Celiński R, Barbero U, Opolski MP. Embolization of Perforated Coronary Artery with a Fragment of Balloon Catheter (Cut Balloon Technique)—Multicenter Study. Journal of Cardiovascular Development and Disease. 2023; 10(12):496. https://doi.org/10.3390/jcdd10120496
Chicago/Turabian StyleSobieszek, Grzegorz, Bartosz Zięba, Wojciech Dworzański, Rafał Celiński, Umberto Barbero, and Maksymilian P. Opolski. 2023. "Embolization of Perforated Coronary Artery with a Fragment of Balloon Catheter (Cut Balloon Technique)—Multicenter Study" Journal of Cardiovascular Development and Disease 10, no. 12: 496. https://doi.org/10.3390/jcdd10120496
APA StyleSobieszek, G., Zięba, B., Dworzański, W., Celiński, R., Barbero, U., & Opolski, M. P. (2023). Embolization of Perforated Coronary Artery with a Fragment of Balloon Catheter (Cut Balloon Technique)—Multicenter Study. Journal of Cardiovascular Development and Disease, 10(12), 496. https://doi.org/10.3390/jcdd10120496