The Touch and Feel of the Past—Using Haptic and VR Artefacts to Enrich Reminiscence Therapy for People with Dementia

User Interface Design GmbH, Rankestr. 8, 10789 Berlin, Germany
*
Author to whom correspondence should be addressed.
Technologies 2018, 6(4), 104; https://doi.org/10.3390/technologies6040104
Submission received: 1 October 2018
/
Revised: 1 November 2018
/
Accepted: 8 November 2018
/
Published: 13 November 2018
(This article belongs to the Special Issue The PErvasive Technologies Related to Assistive Environments (PETRA))
Abstract
:New technology always needs validation in terms of stakeholder acceptance and usability. This challenge also applies in the case of technology for reminiscence therapy for people with dementia. We are looking at how to overcome this situation and identifying how technology can support reminiscence therapy. Therefore, we are conducting user research with people with dementia and their caregivers, prototyping multimedia approaches and testing for efficacy and acceptance of these approaches. Reminiscence therapy is an important aspect in the care for people with dementia as it improves their wellbeing. So far, mostly conventional, analog media is used for this purpose. Our qualitative research suggests that technology can enrich traditional reminiscence therapy, foster conversations, and support positive interactions between caregivers and people with dementia. As outcomes, we identify that special consideration should be directed toward the choice of personally relevant and engaging content, contextual factors of the therapy situations, and high usability of potential therapy artefacts. Suggestions for future research and further prototype iterations are provided.
1. Introduction
Recent estimates show that around 1.6 million people with dementia live in Germany [1]. By 2060, there will be approximately 2.5 million of them and they will represent 3.8% of the population [2]. Technology, designed with the needs of people with dementia in mind, can support the care and wellbeing of these people and help their caregivers and relatives [3]. Therefore, the focus of technology for dementia patients should always be their quality of life and wellbeing.
Section 2 gives an introduction to the current state of technology-supported reminiscence therapy. It continues to outline the research and ideation approaches in the project “Interactive Memories” in Section 3 and to deliver insight into the developed prototypes in Section 4 (Figure 1). Section 5 summarizes the findings and offers a conclusion.
2. Background
2.1. An Outline of Previous Technology Development for People with Dementia
2.2. Status Quo in Reminiscence Therapy
Today, reminiscence therapy is an important aspect of human-centered care for people with dementia, and it improves their wellbeing temporarily [7]. It requires skilled caregivers and a lot of empathy. In individual or group sessions, reminiscence therapy is usually supported by conventional media (mostly photography, poetry, and music).
2.3. Examples of Interactive Systems
Previous studies addressed the issue of dementia with digital photo frames which contain visual and auditive stimuli [6,8]. Independent usage of such digital photo frames by people with dementia was found to be feasible [8]. Research also suggests that the effects of stimuli, addressing the specific needs of people with dementia, are positive on their wellbeing and decrease workload for their caregivers [9].
Virtual reality worlds with a high level of interaction demands are often too hard to grasp for people with dementia in terms of cognitive elaboration and comprehension of the metaphors used. Nevertheless, there is indication that simulated locations and objects can have a positive impact for reminiscence therapy [10].
2.4. The Project “Interactive Memories”
In the project “Interactive Memories”, we are investigating how digital media, new technologies, and innovative ways of interaction can be used to support reminiscence therapy for people with dementia. The development of prototypes for this purpose is carried out in a human-centered design process. Through multimodal stimuli, technology was used to enhance positive aspects of reminiscence therapy and to be able to integrate it seamlessly into care processes in both nursing homes and in the homes of people with dementia. To achieve this goal, therapy artefacts with haptic and virtual reality (VR) features were created to help the user explore media of personal relevance and spark conversations with caregivers and family. Multimedia and multimodal stimuli were used to enhance memory recall and positive emotions during interaction and to improve the wellbeing of people with dementia. This particular study aimed to discover design requirements for such artefacts and to evaluate their general acceptance and overall usability in the user group.
3. Methodology
3.1. Contextual Inquiry and Scenario-Based Design
To gain initial insight, the partners of our project group conducted several focus groups with overall 18 caregivers and 17 relatives of people with dementia. From the findings of these sessions, we were able to define a scope for the project. In order to establish a human-centered approach and focus on the needs of people with dementia, the project group used a research method called contextual inquiry. This method is a combination of observational and conversational techniques, accompanied by visualization and clustering techniques which lead to the deduction of user requirements [11,12]. A contextual inquiry is conducted in the location where the observed target group usually accomplishes the tasks which are to be observed. The researchers interview people from the target group while they accomplish those tasks. Because of the hands-on and open-ended nature of this methodology, researchers are able to uncover aspects of the context or work that the target group might not even be able to articulate because they are not consciously aware of them.
In March 2016, said contextual inquiries were conducted in two nursing homes with approximately 50 participants in their usual environment (care groups specifically for people with dementia). The method was adapted to fit the context of people with dementia. Because people with different stages of dementia may be confused and unable to communicate their needs and wishes [6], the observers joined the different care groups at different periods of the day for a whole week and watched what they would do and how they would interact with each other and with their caregivers [13]. Occasionally, the observers interacted with the participants directly and talked to caregivers; however, they mainly observed and took notes. The observers collected insight into the activities, schedules, habits, conversations, and feelings that people with dementia have in the context of a nursing home with special care groups. Each care group of about 12 people was observed by two researchers. After each day, the researchers gathered and collected all their findings on post-it notes, which were later digitized and arranged in an affinity diagram.
In the framework of the project, Ethical, Legal and Social Implications (ELSI) guidelines were followed during recruiting, research, and testing. All subjects or their legal guardians gave their informed consent for inclusion before they participated in the study. The protocol was approved by the Ethics Committee of Demenz Support Stuttgart. Before the contextual inquiry took place, an ethics workshop was conducted with all the observers.
3.2. Scenario-Based Design and Requirements
The results of the contextual inquiries were analyzed according to contextual design methods. All findings were gathered and arranged in an affinity diagram. They were clustered into different categories and physically put on a wall. The interpretation session of the contextual inquiry is depicted in Figure 2.
These aggregated insights were then turned into scenarios in a scenario-based design process [14]. Scenario-based design is a design process which describes the use of a future system or product in a narrative way. It features four different levels of narrative descriptions: Problem scenarios illustrate the current state and the problems people face at the moment, while activity scenarios show a desirable future on a high level, and information scenarios and interaction scenarios turn this vision of the future into a more and more detailed description.
Firstly, we uncovered problem scenarios and then created activity scenarios, information scenarios, and interaction scenarios. From the resulting scenarios, we derived requirements for different prototypes. Requirements found in this process were as follows: for the development of a prototype, it was essential to address the importance of a high haptic affordance of the object. At the same time, it had to be considered that the motor skills of people with dementia are reduced [15]. In order to support learned interaction behavior and to avoid reactance against the artefacts, technological metaphors had to be borrowed from concepts which were already well known in the middle of the 20th century. To trigger memories and foster conversations, the provided content had to consist of personally relevant stimuli. For this requirement, we analyzed the anonymous biographies of potential participants. We focused on the periods which included the adolescence and early adulthood of the participants. According to research on the life retrieval span, this is a time of increased ability of memory recollection also known as the reminiscence bump [16]. Mostly, the chosen topics concerned family, profession, local history or hometown, and local identity, as well as nature, outdoor activities, entertainment, and stars from different genres such as movies and TV shows. Elderly people also reacted mostly positively to music from the time of their adolescence and early adulthood. To support daily procedures in elder care, it was important to design for group situations, one-on-one care situations, and situations when direct care cannot be provided due to other tasks being carried out by the caregivers.
3.3. Prototyping
We created three high-fidelity prototypes inspired by the findings from the research and the derived requirements. The “Jukebox” and the “Pyramid” were designed first, followed by the “Binoculars” (which were created later). The first two prototypes were built from scratch; for the “Binoculars”, we used available components and modified and put them together.
3.3.1. Jukebox
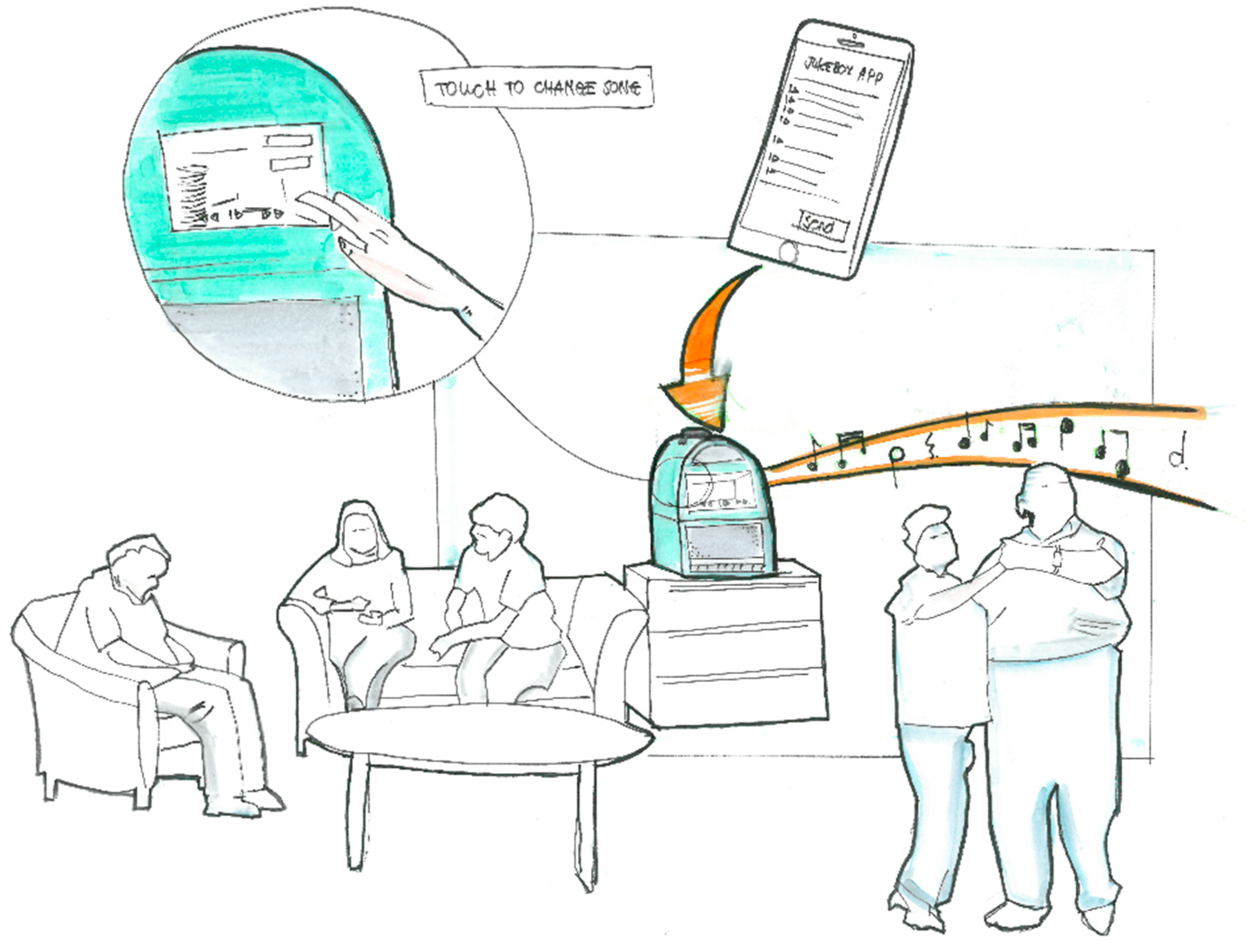
The “Jukebox” combines music from the past with relevant images to target different senses and stimulate memories. Since the prototype can be used just like an actual jukebox (through a limited number of radio buttons for choosing from predefined playlists), it also invites people to interact directly. At the same time, this direct interaction does not demand fine motor skills. All of this meets the described requirements for people with dementia. The general concept of an imagined setting for the “Jukebox” is displayed in Figure 3. The final prototype is shown in Figure 4.
3.3.2. Pyramid
The “Pyramid” combines image material from the most formative and influential spans of time from the lives of participants, with thematically relevant sounds (e.g., true-to-life farm animal sounds, if a farm is shown). Since the prototype can be manipulated by rotating (to change the picture within a topic) and turning the knob on top (to change the topic), this prototype also supports haptic interaction. Simultaneously, it does not demand fine motor skills, which is an important prerequisite for people with dementia. The general concept of an imagined setting for the “Pyramid” is displayed in Figure 5. Images of the actual prototype are depicted in Figure 6.
3.3.3. Binoculars
The “Binoculars” prototype was developed and tested half a year later than the afore-described “Jukebox” and “Pyramid”. Hence, the main findings from the respective tests could be used for the development of the “Binoculars”. These findings included the need for the following:
- Creating a tool for caregivers in one-on-one interventions;
- Reducing social interruptions;
- Decoupling visual experiences from auditive experiences;
- Incorporating information from the individuals’ “reminiscence bump” [16] in the form of a time-travel concept in an immersive and easy to control manner.
The “Binoculars” function as a window into the past. The interaction with the zooming wheel allows the user to move from more recent content (mostly material from the 1970s and 1960s) to more ancient content (mostly material from the 1950s and late 1940s) in a virtual-reality environment.
The flow of the images can also be started in auto-play mode by the caregivers in situations where the user is passive. The caregivers have the ability to do so via a linked computer, which displays the same image that the user of the “Binoculars” is viewing. In a parallel window on the computer screen, the caregiver has a list of suggested topics related to the shown image, which can be used to foster social exchange with the participant. The general concept of the “Binoculars” functionality is displayed in Figure 7. An image of the actual prototype is depicted in Figure 8.
To avoid privacy issues and overly complex content processing, the stimulus material was adjusted to locally relevant topics which were easy to recognize. These topics were enriched with talking points for the caregivers in order to foster conversations and reminiscence. The created content covered the following topics: time travel through Berlin from 1970 to 1949, movie stars of the 1960s and 1950s, popular television (TV) shows in the second half of the 20th century in Germany, time travel to Paris during the 20th century since this was a very popular travel destination, and a selection of images of handicraft.
3.4. Testing
3.4.1. Jukebox
The “Jukebox” was tested in special care groups for people with dementia in a nursing home in Freiburg, Germany in March 2017. The tests took place in six group sessions over the course of two days. In total, 24 participants were present in the six intervention groups. The participants were mostly female (n female = 19; n male = 5) with an average age of mean (M) = 82.63 years (standard error (SE) = 1.71). Every session was accompanied by two observers. The sessions were also video-recorded for subsequent analysis. Figure 9 shows one of the testing situations.
In the framework of the project, ELSI guidelines were followed during recruiting, research, and testing. All subjects or their legal guardians gave their informed consent for inclusion before they participated in the study. The protocol was approved by the Ethics Committee of Demenz Support Stuttgart.
3.4.2. Pyramid
The “Pyramid” was tested in special care groups for people with dementia in a nursing home in Freiburg, Germany in March 2017. The tests were conducted in four group sessions over the course of two days. In total, 25 participants were observed in four intervention sessions. The participants were predominantly female (n female = 20; n male = 5) with an average age of M = 82.32 years (SE = 1.27). Every session was accompanied by two observers. In addition, the sessions were also video-recorded for subsequent analysis. Figure 10 shows one of the testing situations.
In the framework of the project, ELSI guidelines were followed during recruiting, research, and testing. All subjects or their legal guardians gave their informed consent for inclusion before they participated in the study. The protocol was approved by the Ethics Committee of Demenz Support Stuttgart.
3.4.3. Binoculars
The “Binoculars” prototype was tested in November 2017 in a daycare center for geriatric diseases in Berlin, Germany. During the course of half a day, six participants were encouraged individually to use the “Binoculars”. They were all accompanied by one of their caregivers (always the same professional, experienced in reminiscence therapy). The participants were of heterogenous age (M = 74.67, SE = 5.71; range = 55–91). Female (n female = 3) and male (n male = 3) participants were represented equally. Four out of six participants were explicitly diagnosed with forms of dementia. The other two were not unequivocally diagnosed with a specific form of dementia, but showed similar cognitive impairment according to data of the daycare center. The sessions were held in a separate room and lasted from 12 to 20 minutes (M = 15.33, SE = 1.31). All sessions were observed by the same researcher. A second caregiver was present but passive. The setting for the tests is depicted in Figure 11.
In the framework of the project, ELSI guidelines were followed during recruiting, research, and testing. All subjects or their legal guardians gave their informed consent for inclusion before they participated in the study.
In addition to a qualitative behavioral protocol and a general usability assessment regarding the ISO 9241-110 criteria [17], we used a categorial system deriving from the concepts of personal detractors and personal enhancers in the logic of dementia care mapping established by Tom Kitwood in the 1990s [18]. The psychological concept behind this terminology is the ability to either support or undermine the so-called “personhood” of a person with dementia [19]. “Supportive” behavior of people interacting with people with dementia, such as helping them to reach a personally relevant goal or to support their subjective perception of the reality, can have positively stimulating effects. In contrast, behavior of people interacting with people with dementia, such as outpacing them in a decision or imposing a decision onto them, can hurt the personal integrity of the affected person severely [19]. We rated an adapted and reduced version of these forms of “destructive” and “supportive” behavior in the intervention situations. These criteria were chosen to be better able to assess the quality of social interaction fostered by the use of the “Binoculars” prototype. Since there was just one rater, we could not test for inter-rater reliability. Furthermore, the data of the tests were based on only a few participants and should, therefore, not be interpreted causally, but rather descriptively only. The two present caregivers were subsequently interviewed in a semi-structured manner, with a focus on personal recommendations and an assessment of feasibility of the approach in day-to-day procedures in a daycare for people with dementia.
4. Results and Discussion
4.1. Results of the Test Sessions
4.3.1. Jukebox
The auditive stimuli in the “Jukebox” (songs from different music genres) encouraged participants to sing along and clap their hands. This also fostered social exchange about the content and context of the heard stimuli. Validation and success experiences were achieved in a number of participants due to their ability to reminisce lyrics and melodies. Other participants were rather passively picked up in the process and seemed to feel included by the social situation. Few participants were outpaced by the situation. For most participants, it was hard to connect the thematically played music and pictures being displayed. Participants tended to either react to auditive stimuli (singing along, clapping, etc.) or to visual stimuli (gazing, commenting on images) exclusively. Through the reflection and assessment of the caregivers, it was revealed that the concept of the “Jukebox” addressed their needs and requirements insufficiently, since it did not engage the participants directly enough.
4.3.2. Pyramid
The “Pyramid” triggered exclusively positive reactions in participants and caregivers. The image material stimulated memories and fostered conversations in the majority of participants. Even for participants with severe symptoms, the interaction facilitated the success of reminiscence triggering and resulted in externally shown positive emotions.
Most participants were able to change the images on the “Pyramid” easily and playfully after initial instruction of their caregivers. Some of the participants did so fully independently, but the majority needed repeated invitation. Few needed constant explanation and animation. The experience of haptic control seemed to cause increased self-efficacy in most participants. The overall ability to interact with the “Pyramid” far exceeded the caregivers’ expectations.
Despite the rather small screen size (10 inches) the “Pyramid” proved itself valid for group sessions. Participants recognized the content of the images even over relatively far distances. However, user behavior (holding and body positioning) repeatedly showed that hardly more than three people (one active interactor and two adjacently seated) were able to follow the visual stimuli at a time. Caregivers expressed the preference to use artefacts like the “Pyramid” in individual or small group sessions in the future.
4.3.3. Conclusions from the Initial Tests
The following observations were obtained in the test sessions with the “Jukebox” and the “Pyramid”:
- Content material for technology-aided reminiscence therapy needs to contain personally or individually relevant stimuli.
- Memory and emotional effects were much more viable if participants had a personal connection to the material.
- General content from a personally formative era or locally relevant content can be effective, if it triggers connections to personally relevant topics from the past.
- Haptic experience should be offered. At the same time, fine motor skills should not be required, although no severe restrains were observed in the tests.
- Guidance or assistance is mostly needed for interaction with technological aid for reminiscence therapy.
- Intense supportive social interaction between participants and caregivers facilitated the positive effects (memory and conversation) through the usage of the prototypes in the sessions.
The observations of the test sessions with the “Jukebox” and the “Pyramid” led to the following conclusions and, therefore, to the for the additional design of the “Binoculars” prototype:
- Because of the two previous findings (necessity of social guidance and high value of intense social interaction), future prototypes should be especially designed as tools for caregivers.
- The intervention must be feasible in elder care and should not require much preparation or technical knowledge.
- Personally relevant material should be used as stimuli.
- The content should be presented in a more immersive fashion.
- Participants need to stay in control of the situation. There must be an easy way of interrupting or ceasing immersion, as well as a way of re-entering it independently.
4.3.4. Binoculars
In all six observations, the use of the “Binoculars” for reminiscence therapy fostered conversations between the participants and the caregiver. The overall emotional reaction toward the interaction and the content was positive. Some participants figuratively lit up, laughed, and recited lyrics or sang melodies related to the context of the content. Independent use of the “Binoculars” was often possible, but instruction and external motivation was necessary in three out of six cases. Reminiscence seemed to be supported by the content or the questions of the caregiver or both. Images with reportedly higher personal relevance caused more intense exchange between patient and caregiver. Excluding one participant, the participants’ immersion was usually suspended for conversing with the caregiver. This behavior supported the natural conversational situation that the “Binoculars” were intended to facilitate. Sheer passive consumption of the content was not observed. The participants’ attention span was usually not exceeded. Only one participant quit the intervention without completing the time travel she started.
Although all participants assessed the necessary interactions with the “Binoculars” as easily manageable, many of them had trouble reaching for the control wheel. This was partly caused by the very high position of the wheel which made interaction especially hard for participants with small hands or with tremor symptoms. About half of the participants showed either high cautiousness or motoric difficulties turning the control wheel which resulted in slow progress and sometimes in temporary confusion or frustration.
Unintended interactions, such as “zooming” too far, were easy to correct. All participants understood the bidirectional navigation through the content with the wheel. Five out of six participants understood the time-travel metaphor immediately, but some initially struggled with the concept of “zooming” into the past which was supported visually (images where enlarged gradually).
Concerning the categories for “supportive” and “destructive” behavior related to dementia care mapping, we found a clear imbalance in favor of “supportive” interactions (fsup = 92) over “destructive” interactions (fdes = 10). Table 1 shows frequencies of the respective sorts of interactions throughout the six sessions.
Predominantly “supportive” interactions included validation of the participants by the caregiver (fvalidation = 34), especially concerning reported memories or opinions in relation to the shown context; facilitation (ffacilitation = 23) of the interaction with the ”Binoculars”, especially in the moments after temporary confusion or motoric issues; recognition (frecognition = 19) in reaction to success in terms of recognizing content or coping with the task of “time travel”, and as a reply to self-presentation tendencies; and celebration (fcelebration = 15) in reaction to success in terms of recognizing content or coping with the task of “time travel”, and as a reply to the humorous comments of the participants. Table 2 shows frequencies of the specific “supportive” interaction types throughout the six sessions.
Rather “destructive” interactions were only sporadically observed in the form of outpacing (foutpacing = 5) the participants, when they were not yet done with a memory report or were still trying to recall a memory; and imposition (fimposition = 4), when the participants chose not to interact with the “Binoculars”, but were told to do so in a directive manner. Table 3 shows frequencies of the specific “destructive” interaction types throughout the six sessions.
Reasons for this desirable ratio between “supportive” and “destructive” interactions can be manifold. One influential factor may be the technology-aided aspect which made the reminiscence therapy session playful. Another aspect that might be relevant is the rare situation of a one-on-one session as opposed to more dynamic group sessions with less attention paid to one person and more detracting interferences from other people with dementia. Furthermore, the caregiver in the test sessions was experienced and professional and, finally, we must consider a possible observer effect.
The caregivers stated the following evaluations in a semi-structured interview after the tests:
- According to their assessment, usage of the prototypes needed to happen more fluently; long transitions between images and the “zooming” metaphor were to be eliminated, as they confused some of the participants.
- A smaller angle of rotation to switch from image to image should be selected for the control wheel.
- It was perceived as vital to establish some form of handling facilitation for users with tremors, weakness, or decreased motor skills.
- At the same time, the assumption was supported that headbands (as used in VR headsets) should not be used for the “Binoculars”, as they would force the immersion onto potentially confused users and would inhibit the observed immersion pause (lowering the “Binoculars”) for conversation with the caregiver, which was a common behavior in almost every user. With the approach that we chose, the user always stayed in control.
- In general, a solid efficacy of technology-aided reminiscence therapy was confirmed by the caregivers.
- It was stressed that participants of the sessions should always be accompanied by a caregiver or a relative to effectively trigger a positive user experience, since the participants explicitly enjoyed the social exchange and would likely only consume the content otherwise. This confirms our assumptions and corroborates our concept of providing a tool for caregivers.
Nevertheless, the caregivers saw only little chance to establish the “Binoculars” approach in daily care as it is currently organized in Germany, since reminiscence therapy is usually conducted in group sessions due to lack of workforce for one-on-one sessions. However, this objection is only valid in the context of ambulant daycare. In stationary nursing homes, individual reminiscence sessions are common, which provides outstanding opportunities to establish the use of the “Binoculars”. Additionally, the caregivers saw a valuable field of application of this prototype in hospice clinics. In this setting, a very intensive one-on-one care with a focus on wellbeing is common.
5. Summary and Conclusions
5.1. Summary of the Test Results
In the project “Interactive Memories”, we derived requirements for the design of technological reminiscence therapy objects from a contextual inquiry and through scenario-based design. Requirements for technology-aided reminiscence therapy found with these methods were as follows:
- Using highly personally relevant content;
- Addressing several sensory modalities including haptic affordance;
- Adaption to motor abilities and mental models of people with dementia (i.e., applicable metaphors for prototypes);
- Fostering conversation through technology and solutions applicable for group situations and one-on-one interventions (i.e., caregiver tools).
Initial tests with the “Jukebox” and the “Pyramid” showed proof of concept regarding effects on recognition and social exchange. Necessary adaptions concerned the following:
- Scope of intervention situations (next iteration as a one-on-one caregiver tool);
- Higher levels of immersion with robust levels of user control to be able to leave unpleasant situations;
- Contextual information for the caregiver to foster conversation;
- Decoupling different sources of sensory stimulation.
Tests of the next prototype generation (“Binoculars”) showed the following:
- Proof of concept regarding effects for recognition and social exchange was acquired;
- The concept of time traveling was mostly understood well and perceived as favorable;
- The intervention with the “Binoculars” seemed to be explicitly beneficial for “supportive” interactions between caregivers and people with dementia;
- Insight into usability and ergonomics were gathered for future design iterations.
5.2. Conclusions
This paper covered the general acceptance of technology-aided reminiscence therapy and the acceptance, as well as efficacy, of the tested prototypes. Our findings strengthen our assumptions of the incremental value of technology in this field. In order to objectively determine the benefit of technology in comparison to traditional reminiscence therapy, it appears to be advisable to conduct comparative research not only in terms of acceptance and efficacy, but also of efficiency and satisfaction. Is technology-aided reminiscence therapy just as successful or potentially even more promising than traditional forms?
As we decided to build our third prototype as a tool for caregivers in one-on-one sessions, we shifted the focus of analysis away from group situations with the “Binoculars”. It appears to be advisable to conduct comparative research concerning acceptance and efficacy of this approach. This is especially the case in terms of the protection of “personhood” during sessions, as it seems like a more individually stimulating and gentle intervention. This impression needs to be verified.
The research in this paper was mainly of a qualitative nature. To strengthen the observations and conclusions which derive from this project, it seems advisable to establish an assuring metric to provide a measure for operationalization of intervention success. A first step toward this issue is the implementation of basic categories related to dementia care mapping, which can be extended. A further necessary effort to validate the observations and conclusions in this paper is to invest in inter-rater reliability analysis, especially since only one rater applied the categorial system in the examination of the “Binoculars”.
In our research, the level of experience, the set of professional skills, and the degree of social skills of the caregivers differed. Since this might have an influence on the handling of the artefacts for reminiscence therapy and overall interaction of the caregivers with the people with dementia during intervention sessions, it might be useful to further investigate the influence of the caregiver in charge.
The conducted research covered the initial acceptance of technology-aided reminiscence therapy and the acceptance, as well as efficacy, of the tested prototypes. To determine possible positive long-term effects of this approach, it might be desirable to gather longitudinal data.
Longitudinal data, in the form of log data and eye-tracking data collection in order to enable machine learning, could also foster iterative and ongoing re-design of future prototypes and products. Of course, these methods would be highly invasive and research would need to be carried out under strict ethical standards and caution. A goal for technology-aided reminiscence therapy might be the ability of artefacts to adaptively change behavior and content dependent on the changes in the behavior and reactions of interacting people with dementia on a day-to-day basis. If people with dementia respond to different stimuli on different days, then tools for caregivers with implemented machine learning might be able to help the present professionals react accordingly with different foci in image presentation and conversation. Personally relevant material and allowed degrees of immersion could possibly be adapted in different sessions.
Author Contributions
H.W. wrote the paper and was responsible for testing one of the prototypes. M.U. took part in the user research, prototype development, and testing. P.K. is the overall project manager and was responsible for reviewing the paper.
Funding
This research was funded by the German Federal Ministry of Education and Research, grant number 16SV7325.
Acknowledgments
In the project “Interactive Memories”, we investigated how digital media, new technologies, and innovative ways of interaction can be used to support reminiscence therapy for people with dementia. We would like to gratefully mention the constructive collaboration with our partners Demenz Support Stuttgart gGmbH, Julius-Maximilians-Universität Würzburg, Hochschule Furtwangen, Vertigo Systems GmbH, Marienhaus St. Johann e.V., Fürstlich-Fürstenbergisches Altenpflegeheim Hüfingen, and Caritasverband Erzdiözese Freiburg e.V. On a special note, we would like to thank the Evangelisches Geriatriezentrum Berlin for their cooperation. Finally, we would like to thank the Bundesministerium für Bildung und Forschung and VDI/VDE Innovation + Technik GmbH for funding. More information about the project “InterMem” can be found at http://www.intermem.org.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Policy in Practice—Country Comparisons—2013: The Prevalence of Dementia in Europe—Germany. 2014. Available online: http://www.alzheimer-europe.org/Policy-in-Practice2/Country-comparisons/2013-The-prevalence-of-dementia-in-Europe/Germany (accessed on 5 December 2017).
- Rothgang, H.; Iwansky, S.; Muller, R.; Sauer, S.; Unger, R. Barmer GEK-Pflegereport; Asgard-Verlag: St. Augustin, Germany, 2010. [Google Scholar]
- Topo, P. Technology studies to meet the needs of people with dementia and their caregivers. J. Appl. Gerontol. 2008, 28, 5–37. [Google Scholar] [CrossRef]
- Robinson, L.; Brittain, K.; Lindsay, S.; Jackson, D.; Olivier, P. Keeping in Touch Everyday (KITE) project: Developing assistive technologies with people with dementia and their carers to promote independence. Int. Psychogeriatr. 2009, 21, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Orpwood, R.; Chadd, J.; Howcroft, D.; Sixsmith, A.; Torrington, J.; Gibson, G.; Chalfont, G. User-led design of technology to improve quality of life for people with dementia. In Designing Inclusive Futures; Langdon, P., Clarkson, J., Robinson, P., Eds.; Springer: London, UK, 2008; pp. 185–195. [Google Scholar] [CrossRef]
- Sixsmith, A.; Gibson, G.; Orpwood, R.; Torrington, J. Developing a technology ‘wish-list’ to enhance the quality of life of people with dementia. Gerontechnology 2007, 6, 2–19. [Google Scholar] [CrossRef]
- Woods, B.; Spector, A.E.; Jones, C.A.; Orrell, M.; Davies, S.P. Reminiscence therapy for dementia. Cochrane Database Syst. Rev. 2005. [Google Scholar] [CrossRef] [PubMed]
- Gowans, G.; Campbell, J.; Alm, N.; Dye, R.; Astell, A.; Ellis, M. Designing a multimedia conversation aid for reminiscence therapy in dementia care environments. In CHI’04 Extended Abstracts on Human Factors in Computing Systems; ACM: New York, NY, USA, 2004; pp. 825–836. [Google Scholar]
- Oppikofer, S.; Breitschmid, H.; Schachtler, F.; Neysari, M.; Aeschlimann, C. Filme für Menschen mit Demenz im Heim. In Zürcher Schriften zur Gerontologie; Zentrum für Gerontologie: Zürich, Switzerland, 2012. (In German) [Google Scholar]
- Siriaraya, P.; Ang, C.S. Recreating living experiences from past memories through virtual worlds for people with dementia. In Proceedings of the 32nd Annual ACM Conference on Human Factors in Computing Systems—CHI 2014, Toronto, ON, Canada, 26 April–1 May 2014; Volume 14, pp. 3977–3986. [Google Scholar] [CrossRef]
- Beyer, H.; Holtzblatt, K. Contextual Design: Defining Customer-Centered Systems; Morgan Kaufmann: San Francisco, CA, USA, 2009. [Google Scholar]
- Holtzblatt, K.; Wendell, J.B.; Wood, S. Rapid Contextual Design: A How-To Guide to Key Techniques for User-Centered Design; Morgan Kaufmann: Amsterdam, The Netherlands, 2009. [Google Scholar]
- Huber, S.; Preßler, J.; Hurtienne, J. Anpassung von Contextual Design für den Kontext Demenz. In Mensch und Computer 2016-Tagungsband; Gesellschaft für Informatik: Aachen, Germany, 2016. (In German) [Google Scholar]
- Rosson, M.B.; Carroll, J.M. Usability Engineering: Scenario-Based Development of Human Computer Interaction; Morgan Kaufmann: San Francisco, CA, USA, 2009. [Google Scholar]
- Scherder, E.; Dekker, W.; Eggermont, L. Higher-level hand motor function in aging and (preclinical) dementia: Its relationship with (instrumental) activities of daily life—A mini-review. Gerontology 2008, 54, 333–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansari, A.; Parkin, A.J. Things that go bump in your life: Explaining the reminiscence bump in autobiographical memory. Psychol. Aging 1996, 11, 85–91. [Google Scholar] [CrossRef] [PubMed]
- ISO 9241-110: Ergonomics of Human-System Interaction—Pt. 110: Dialogue Principles; International Organization for Standardization: Geneva, Switzerland, 2006.
- Kitwood, T.M. Dementia Reconsidered: The Person Comes First; Open University Press: Berkshire, UK, 2007. [Google Scholar]
- Brooker, D.; Surr, C. Dementia Care Mapping: Principles and Practice; University of Bradford: Bradford, UK, 2005. [Google Scholar]
Figure 1.
The pictures show prototypes for reminiscence therapy with people with dementia being tested in a nursing home and a daycare facility. Left to right: the “Jukebox”, the “Pyramid”, and the “Binoculars”.
Figure 1.
The pictures show prototypes for reminiscence therapy with people with dementia being tested in a nursing home and a daycare facility. Left to right: the “Jukebox”, the “Pyramid”, and the “Binoculars”.

Figure 2.
Interpretation session after contextual inquiry.

Figure 3.
Functionality of the “Jukebox”.

Figure 4.
The “Jukebox” prototype.

Figure 5.
Functionality of the “Pyramid”.

Figure 6.
The “Pyramid” prototype.

Figure 7.
Time-travel concept in the “Binoculars”.

Figure 8.
The “Binoculars” prototype.

Figure 9.
The “Jukebox” in a nursing home setting.

Figure 10.
The “Pyramid” in a nursing home setting.

Figure 11.
The “Binoculars” in a daycare setting.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Frequencies of destructive and supportive interactions in comparison.
| Participants | Destructive | Supportive |
|---|---|---|
| Participant 1 | 0 | 12 |
| Participant 2 | 2 | 11 |
| Participant 3 | 3 | 18 |
| Participant 4 | 0 | 23 |
| Participant 5 | 2 | 12 |
| Participant 6 | 3 | 16 |
| Total | 10 | 92 |
Table 2.
Frequencies of supportive interactions.
| Supportive Interactions | Frequency |
|---|---|
| Recognition | 19 |
| Celebration | 15 |
| Relaxation | 1 |
| Validation | 34 |
| Facilitation | 23 |
| Total | 92 |
Table 3.
Frequencies of destructive interactions.
| Destructive Interactions | Frequency |
|---|---|
| Outpacing | 5 |
| Ignoring | 1 |
| Imposition | 4 |
| Total | 10 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Klein, P.; Uhlig, M.; Will, H. The Touch and Feel of the Past—Using Haptic and VR Artefacts to Enrich Reminiscence Therapy for People with Dementia. Technologies 2018, 6, 104. https://doi.org/10.3390/technologies6040104
AMA Style
Klein P, Uhlig M, Will H. The Touch and Feel of the Past—Using Haptic and VR Artefacts to Enrich Reminiscence Therapy for People with Dementia. Technologies. 2018; 6(4):104. https://doi.org/10.3390/technologies6040104
Chicago/Turabian StyleKlein, Peter, Martina Uhlig, and Hannes Will. 2018. "The Touch and Feel of the Past—Using Haptic and VR Artefacts to Enrich Reminiscence Therapy for People with Dementia" Technologies 6, no. 4: 104. https://doi.org/10.3390/technologies6040104
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.