Cue-Elicited Anxiety and Alcohol Craving as Indicators of the Validity of ALCO-VR Software: A Virtual Reality Study


 ,
, 
Abstract
:1. Introduction
2. Method
2.1. Participants
2.2. Measures
2.3. Instruments
2.3.1. Hardware
2.3.2. “ALCO-VR” Software
2.4. Procedure
2.5. Statistical Analysis
3. Results
Data of the Self-Reported Questionnaires
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Thursz, M.; Kamath, P.S.; Mathurin, P.; Szabo, G.; Shah, V.H. Alcohol-related liver disease: Areas of consensus, unmet needs and opportunities for further study. J. Hepatol. 2019, 65, 2271–2283. [Google Scholar] [CrossRef] [PubMed]
- Connor, J.P.; Haber, P.S.; Hall, W.D. Alcohol use disorders. Lancet 2016, 387, 988–998. [Google Scholar] [CrossRef] [Green Version]
- Rehm, J.; Anderson, P.; Barry, J.; Dimitrov, P.; Elekes, Z.; Feijão, F.; Frick, U.; Gual, A.; Gmel, G.; Kraus, L.; et al. Prevalence of and potential influencing factors for alcohol dependence in Europe. Eur. Addict. Res. 2015, 21, 6–18. [Google Scholar] [CrossRef] [PubMed]
- Shield, K.D.; Parry, C.; Rehm, J. Chronic diseases and conditions related to alcohol use. Alcohol. Res. Curr. Rev. 2014, 35, 155–173. [Google Scholar]
- Prince, M.A.; Read, J.P.; Colder, C.R. Trajectories of college alcohol involvement and their associations with later alcohol use disorder symptoms. Prev. Sci. 2019, 20, 741–752. [Google Scholar] [CrossRef] [PubMed]
- King, A.C.; Hasin, D.; O’Connor, S.J.; McNamara, P.J.; Cao, D. A prospective 5-year re-examination of alcohol response in heavy drinkers progressing in alcohol use disorder. Biol. Psychiatry 2016, 79, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Schulte, M.T.; Ramo, D.; Brown, S.A. Gender differences in factors influencing alcohol use and drinking progression among adolescents. Clin. Psychol. Rev. 2009, 296, 535–547. [Google Scholar] [CrossRef]
- Dawson, D.A.; Goldstein, R.B.; Chou, S.P.; June-Ruan, W.; Grant, B.F. Age at first drink and the first incidence of adult-onset DSM-IV alcohol use disorders. Alcohol. Clin. Exp. Res. 2008, 32, 2149–2160. [Google Scholar] [CrossRef]
- Coriale, G.; Fiorentino, D.; Rosa, F.; Solombrino, S.; Scalese, B.; Ciccarelli, R.; Attilia, F.; Vitali, M.; Musetti, A.; Fiore, M.; et al. Treatment of alcohol use disorder from a psychological point of view. Riv. Psichiatr. 2018, 53, 141–148. [Google Scholar]
- Andersson, H.W.; Wenaas, M.; Nordfjærn, T. Relapse after inpatient substance use treatment: A prospective cohort study among users of illicit substances. Addict. Behav. 2019, 90, 222–228. [Google Scholar] [CrossRef]
- Sinha, R.; Fox, H.C.; Hong, K.; Hansen, J.; Tuit, K.; Kreek, M.J. Effects of adrenal sensitivity, stress- and cue-induced craving, and anxiety on subsequent alcohol relapse and treatment outcomes. Arch. Gen. Psychiatry 2011, 68, 942–952. [Google Scholar] [CrossRef]
- Blanco, C.; Flórez-Salamanca, L.; Secades-Villa, R.; Wang, S.; Hasin, D.S. Predictors of initiation of nicotine, alcohol, cannabis, and cocaine use: Results of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). Am. J. Addict. 2018, 27, 477–484. [Google Scholar] [CrossRef]
- Gilpin, N.W.; Herman, M.A.; Roberto, M. The central amygdala as an integrative hub for anxiety and alcohol use disorders. Biol. Psychiatry 2015, 77, 859–869. [Google Scholar] [CrossRef]
- Anker, J.J.; Kummerfeld, E.; Rix, A.; Burwell, S.J.; Kushner, M.G. Causal Network Modeling of the determinants of drinking behavior in comorbid alcohol use and anxiety disorder. Alcohol. Clin. Exp. Res. 2018, 43, 91–97. [Google Scholar] [CrossRef]
- Miloyan, B.; Van Doorn, G. Longitudinal association between social anxiety disorder and incident alcohol use disorder: Results from two national samples of US adults. Soc. Psychiatry Psychiatr. Epidemiol. 2019, 54, 469–475. [Google Scholar] [CrossRef]
- Wolitzky-Taylor, K.; Niles, A.N.; Ries, R.; Krull, J.L.; Rawson, R.; Roy-Byrne, P.; Craske, M. Who needs more than standard care? Treatment moderators in a randomized clinical trial comparing addiction treatment alone to addiction treatment plus anxiety disorder treatment for comorbid anxiety and substance use disorders. Behav. Res. Ther. 2018, 107, 1–9. [Google Scholar] [CrossRef]
- Drummond, D.C. Theories of drugs craving, ancient and modern. Addiction 2001, 96, 33–46. [Google Scholar] [CrossRef]
- Van Lier, H.G.; Pieterse, M.E.; Schraagen, J.M.C.; Postel, M.G.; Vollenbroek-Hutten, M.M.R.; de Haan, H.A.; Noordzij, M.L. Identifying viable theoretical frameworks with essential parameters for real-time and real world alcohol craving research: A systematic review of craving models. Addict. Res. Theory 2018, 26, 35–51. [Google Scholar] [CrossRef]
- Pavlov, I.P. Conditioned reflexes: An investigation of the physiological activity of the cerebral cortex. Ann. Neurosci. 1927, 17, 136–141. [Google Scholar] [CrossRef]
- Pina, M.M.; Williams, R.A. Alcohol cues, craving, and relapse: Insights from animal models. In Recent Advances in Drug Addiction Research and Clinical Applications; IntechOpen: London, UK, 2016; pp. 47–79. [Google Scholar]
- Wrase, J.; Schlagenhauf, F.; Kienast, T.; Wustenberg, T.; Bermpohl, F.; Kahnt, T.; Beck, A.; Strohle, A.; Juckel, G.; Knutson, B.; et al. Dysfunction of reward processing correlates with alcohol craving in detoxified alcoholics. Neuroimage 2007, 35, 787–794. [Google Scholar] [CrossRef]
- Kim, D.J.; Jeong, J.; Kim, K.S.; Chae, J.H.; Jin, S.H.; Ahn, K.J.; Myrick, H.; Yoon, S.J.; Kim, H.R.; Kim, S.Y. Complexity changes of the EEG induced by alcohol cue exposure in alcoholics and social drinkers. Alcohol. Clin. Exp. Res. 2003, 27, 1955–1961. [Google Scholar] [CrossRef]
- Witteman, J.; Post, H.; Tarvainen, M.; De Bruijn, A.; De Elizabeth, S.F.P.; Ramaekers, J.G.; Wiers, R.W. Cue reactivity and its relation to craving and relapse in alcohol dependence: A combined laboratory and field study. Psychopharmacology 2015, 232, 3685–3696. [Google Scholar] [CrossRef]
- Sinha, R.; Fox, H.C.; Hong, K.A.; Bergquist, K.; Bhagwagar, Z.; Siedlarz, K.M. Enhanced negative emotion and alcohol craving, and altered physiological responses following stress and cue exposure in alcohol dependent individuals. Neuropsychopharmacology 2009, 34, 1198–1208. [Google Scholar] [CrossRef]
- Bottlender, M.; Soyka, M. Impact of craving on alcohol relapse during, and 12 months following, outpatient treatment. Alcohol Alcohol. 2004, 39, 357–361. [Google Scholar] [CrossRef]
- Valyear, M.D.; Villaruel, F.R.; Chaudhri, N. Alcohol-seeking and relapse: A focus on incentive salience and contextual conditioning. Behav. Process. 2017, 141, 26–32. [Google Scholar] [CrossRef]
- Olney, J.J.; Warlow, S.M.; Naffziger, E.E.; Berridge, K.C. Current perspectives on incentive salience and applications to clinical disorders. Curr. Opin. Behav. Sci. 2018, 22, 59–69. [Google Scholar] [CrossRef]
- Stasiewicz, P.R.; Brandon, T.H.; Bradizza, C.M. Effects of extinction context and retrieval cues on renewal of alcohol-cue reactivity among alcohol-dependent outpatients. Psychol. Addict. Behav. 2007, 21, 244–253. [Google Scholar] [CrossRef]
- Conklin, C.A.; Tiffany, S.T. Applying extinction research and theory to cue-exposure addiction treatments. Addiction 2002, 97, 155–167. [Google Scholar] [CrossRef] [Green Version]
- Ghiţă, A.; Gutiérrez-Maldonado, J. Applications of virtual reality in individuals with alcohol misuse: A systematic review. Addict. Behav. 2018, 81, 1–11. [Google Scholar] [CrossRef]
- Riva, G. Virtual reality: An experiential tool for clinical psychology. Br. J. Guid. Couns. 2009, 37, 335–343. [Google Scholar] [CrossRef]
- Ferrer-García, M.; García-Rodríguez, O.; Gutiérrez-Maldonado, J.; Pericot-Valverde, I.; Secades-Villa, R. Efficacy of Virtual Reality in triggering the craving to smoke: Its relation to level of presence and nicotine dependence. Annu. Rev. Cyberther. Telemed. 2010, 8, 99–106. [Google Scholar]
- Serre, F.; Fatseas, M.; Swendsen, J.; Auriacombe, M. Ecological momentary assessment in the investigation of craving and substance use in daily life: A systematic review. Drug Alcohol. Dep. 2015, 148, 1–20. [Google Scholar] [CrossRef]
- Shiffman, S.; Stone, A.A.; Hufford, M.R. Ecological momentary assessment. Annu. Rev. Clin. Psychol. 2008, 4, 1–32. [Google Scholar] [CrossRef]
- Bordnick, P.S.; Traylor, A.; Copp, H.L.; Graap, K.M.; Carter, B.; Ferrer, M.; Waton, A.P. Assessing reactivity to virtual reality alcohol based cues. Addict. Behav. 2008, 33, 743–756. [Google Scholar] [CrossRef]
- Cho, S.; Ku, J.; Park, J.; Han, K.; Lee, H.; Choi, Y.K.; Jung, Y.-C.; Namkoong, K.; Kim, J.-J.; Kim, I.Y.; et al. Development and Verification of an Alcohol Craving–Induction Tool Using Virtual Reality: Craving Characteristics in Social Pressure Situation. CyberPsychol. Behav. 2008, 11, 302–309. [Google Scholar] [CrossRef]
- Pericot-Valverde, I.; Secades-Villa, R.; Gutierrez-Maldonado, J.; Garcia-Rodriguez, O. Effects of systematic cue exposure through virtual reality on cigarette craving. Nicotine Tob. Res. 2014, 16, 1470–1477. [Google Scholar] [CrossRef]
- Acker, J.; MacKillop, J. Behavioral economic analysis of cue-elicited craving for tobacco: A Virtual Reality study. Nicotine Tob. Res. 2013, 15, 1409–1416. [Google Scholar] [CrossRef]
- Bordnick, P.S.; Graap, K.M.; Copp, H.L.; Brooks, J.; Ferrer, M. Virtual Reality cue reactivity assessment in cigarette smokers. Cyberpsychol. Behav. 2005, 8, 487–492. [Google Scholar] [CrossRef]
- Culbertson, C.; Nicolas, S.; Zaharovits, I.; London, E.D.; Garza, R.; Brody, A.L.; Newton, T.F. Methamphetamine craving induced in an online virtual reality environment. Pharmacol. Biochem. Behav. 2010, 96, 454–460. [Google Scholar] [CrossRef] [Green Version]
- Saladin, M.E.; Brady, K.T.; Graap, K.; Rothbaum, B.O. A preliminary report on the use of virtual reality technology to elicit craving and cue reactivity in cocaine dependent individuals. Addict. Behav. 2006, 31, 1881–1894. [Google Scholar] [CrossRef]
- Pla-Sanjuanelo, J.; Ferrer-García, M.; Vilalta-Abella, F.; Riva, G.; Dakanalis, A.; Ribas-Sabaté, J.; Andreu-Gracia, A.; Fernandez-Aranda, F.; Sanchez-Diaz, I.; Escandón-Nagel, N.; et al. Testing virtual reality-based cue-exposure software: Which cue-elicited responses best discriminate between patients with eating disorders and healthy controls? Eat. Weight Disord. 2019, 24, 757–769. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Llopis Llácer, J.J.; Gual Solé, A.; Rodríguez-Martos Dauer, A. Registro del consumo de bebidas alcohólicas mediante la unidad de bebida estándar. Diferencias geográficas. Adicciones 2000, 12, 11–20. [Google Scholar] [CrossRef]
- Saunders, J.B.; Aasland, O.G.; Babor, T.F.; De La Fuente, J.R.; Grant, M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption-II. Addiction 1993, 88, 791–804. [Google Scholar] [CrossRef]
- Contel Guillamón, M.; Gual Solé, A.; Colom Farran, J. Test para la identificación de trastornos por uso de alcohol (AUDIT): Traducción y validación del AUDIT al catalán y castellano. Adicciones 1999, 11, 337–347. [Google Scholar] [CrossRef]
- Guardia Serecigni, J.; Segura García, L.; Gonzalvo Cirac, B.; Trujols Albet, J.; Tejero Pociello, A.; Suárez González, A.; Martí Gil, A. Estudio de validación de la Escala Multidimensional de Craving de Alcohol. Med. Clin. 2004, 123, 211–216. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Gonzalez-Reigosa, F.; Martinez-Urrutia, A.; Natalicio, L.F.S.; Natalicio, D.S. Development of the Spanish Edition of the State-Trait Anxiety Inventory. Interam. J. Psychol. 1971, 5, 145–158. [Google Scholar]
- Ghiţă, A.; Teixidor, L.; Monras, M.; Ortega, L.; Mondon, S.; Gual, A.; Paredes, S.M.; Villares-Urgell, L.; Porras-Garcia, B.; Ferrer-Garcia, M.; et al. Identifying triggers of alcohol craving to develop effective virtual environments for cue exposure therapy. Front. Psychol. 2019, 10, 74. [Google Scholar] [CrossRef]
- Lee, J.S.; Namkoong, K.; Ku, J.; Cho, S.; Park, J.Y.; Choi, Y.K.; Kim, J.J.; Kim, I.Y.; Kim, S.I.; Jung, Y.C. Social pressure-induced craving in patients with alcohol dependence: Application of virtual reality to coping skill training. Psychiatry Investig. 2008, 5, 239–243. [Google Scholar] [CrossRef]
- Gamito, P.; Oliveira, J.; Baptista, A.; Morais, D.; Lopes, P.; Rosa, P.; Santos, N.; Brito, R. Eliciting nicotine craving with virtual smoking cues. Cyberpsychol. Behav. Soc. Netw. 2014, 17, 556–561. [Google Scholar] [CrossRef]
- Shin, Y.B.; Kim, J.J.; Kim, M.K.; Kyeong, S.; Jung, Y.H.; Eom, H.; Kim, E. Development of an effective virtual environment in eliciting craving in adolescents and young adults with internet gaming disorder. PLoS ONE 2018, 13, e0195677. [Google Scholar] [CrossRef]
- Bouchard, S.; Robillard, G.; Giroux, I.; Jacques, C.; Loranger, C.; St-Pierre, M.; Chrétien, M.; Goulet, A. Using virtual reality in the treatment of gambling disorder: The development of a new tool for cognitive behavior therapy. Front. Psychiatry 2017, 8, 27. [Google Scholar] [CrossRef] [PubMed]
- Ryan, J.J.; Kreiner, D.S.; Chapman, M.D.; Stark-Wroblewski, K. Virtual reality cues for binge drinking in college students. CyberPsychol. Behav. 2010, 13, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Ferrer-García, M.; Pla-Sanjuanelo, J.; Dakanalis, A.; Vilalta-Abella, F.; Riva, G.; Fernandez-Aranda, F.; Forcano, L.; Riesco, N.; Sánchez, I.; Clerici, M.; et al. A randomized trial of Virtual Reality-based cue exposure second-level therapy and cognitive-behavior second-level therapy for bulimia nervosa and binge-eating disorder: Outcome at six-month follow-up. Cyberpsychol. Behav. Soc. Netw. 2018, 22, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Ghiţă, A.; Ferrer-Garcia, M.; Gutiérrez-Maldonado, J. Behavioral, craving, and anxiety responses among light and heavy drinking college students in alcohol-related virtual environments. Annu. Rev. Cyberther. Telemed. 2017, 15, 135–140. [Google Scholar]
- Bordnick, P.S.; Carter, B.L.; Traylor, A.C. What virtual reality research in addictions can tell us about the future of obesity assessment and treatment. J. Diabetes Sci. Technol. 2011, 5, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Pla-Sanjuanelo, J.; Ferrer-García, M.; Gutiérrez-Maldonado, J.; Riva, G.; Andreu-Gracia, A.; Dakanalis, A.; Fernandez-Aranda, F.; Forcano, L.; Ribas-Sabaté, J.; Riesco, N.; et al. Identifying specific cues and contexts related to bingeing behavior for the development of effective virtual environments. Appetite 2015, 87, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Ferrer-García, M.; Gutiérrez-Maldonado, J.; Pla-Sanjuanelo, J.; Vilalta-Abella, F.; Riva, G.; Clerici, M.; Ribas-Sabate, J.; Andreu-Garcia, A.; Fernandez-Aranda, F.; Forcano, L.; et al. A randomised controlled comparison of second-level treatment approaches for treatment-resistant adults with bulimia nervosa and binge eating disorder: Assessing the benefits of virtual reality cue exposure therapy. Eur. Eat. Disord. Rev. 2017, 25, 479–490. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scales | Alcohol Use Disorder (AUD) Patients M (SD) | Social Drinkers M (SD) |
|---|---|---|
| Alcohol Use Disorder Identification Test (AUDIT) | 23.77 (13) | 4.5 (2.2) |
| State-Trait Anxiety Inventory (STAI) (trait part) | 34.85 (12) | 19 (13) |
| Multidimensional Alcohol Craving Scale (MACS) | 29.23 (9.3) | 20 (4.1) |
| STAI (state part) | 18.77 (12.4) | 15.64 (14.41) |
| MACS-VR | 36 (12.17) | 26.64 (10.9) |
| AUD Patients (N = 13) | Social Drinkers (N = 14) | ||||||
|---|---|---|---|---|---|---|---|
| Mean (SD) | Median | IQR a | Mean (SD) | Median | IQR | Z b | |
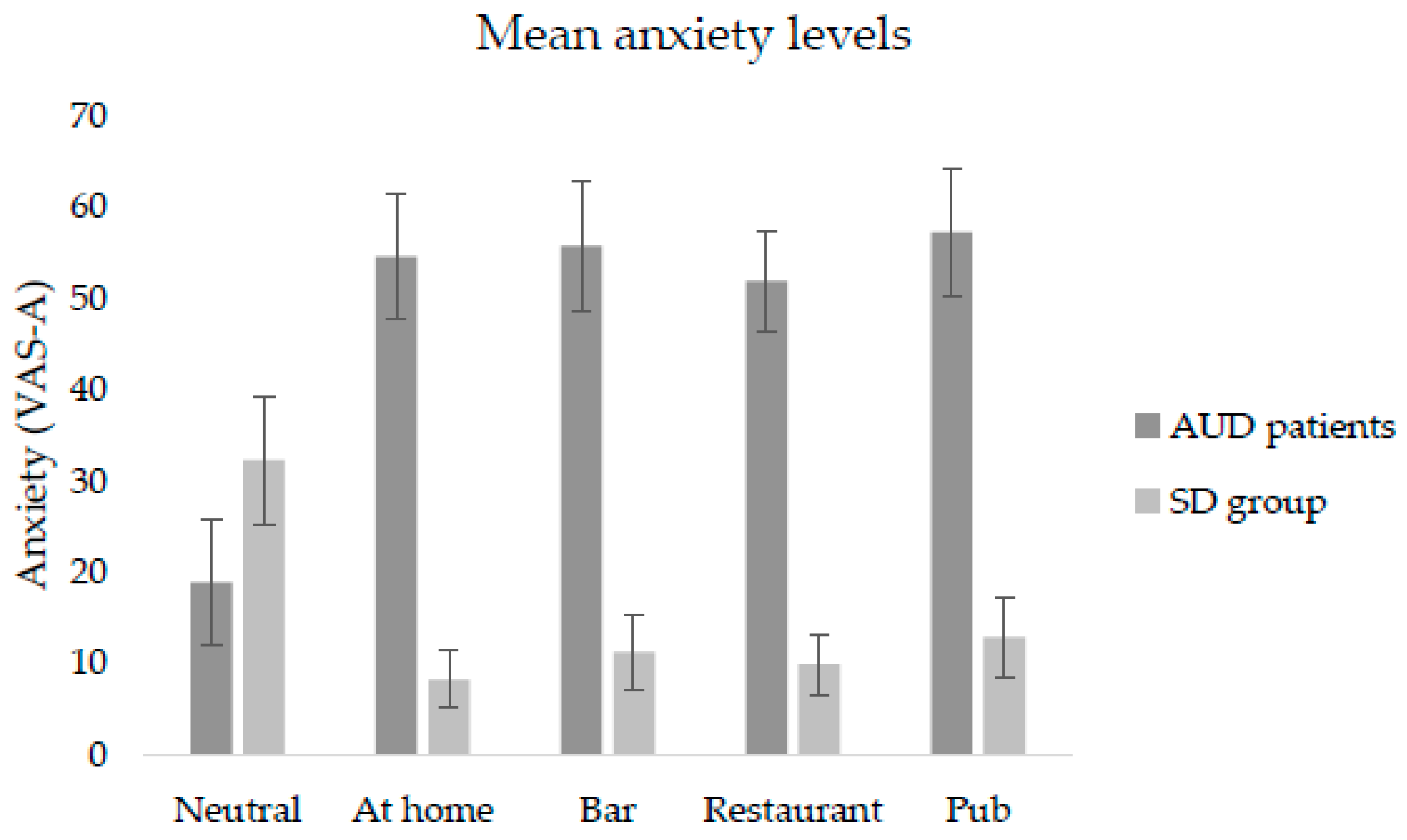
| Neutral env c | |||||||
| Anxiety | 18.85 (24.54) | 5.00 | 40 | 32.21 (26.45) | 34.00 | 50 | −1.347 |
| Craving | 7.69 (16.05) | 0.00 | 7 | 21.64 (26.38) | 11.00 | 32 | −1.726 |
| At home | |||||||
| Anxiety | 54.54 (24.97) | 54.00 | 36 | 8.21 (11.82) | .50 | 15 | −4.064 *** |
| Craving | 54.77 (22.86) | 62.00 | 33 | 24.93 (18.71) | 19.00 | 33 | −3.180 *** |
| Bar | |||||||
| Anxiety | 55.69 (25.70) | 52.00 | 43 | 11.21 (15.55) | 2.50 | 22 | −3.980 *** |
| Craving | 58.62 (23.11) | 61.00 | 44 | 31.64 (21.57) | 32.00 | 42 | −2.719 * |
| Restaurant | |||||||
| Anxiety | 51.77 (20.17) | 53.00 | 41 | 9.93 (12.17) | 5.50 | 17 | −4.162 *** |
| Craving | 57.54 (22.74) | 59.00 | 44 | 30.93 (20.58) | 34.50 | 39 | −2.671 * |
| Pub | |||||||
| Anxiety | 57.15 (25.32) | 54.00 | 46 | 12.86 (16.61) | 5.00 | 27 | −3.896 *** |
| Craving | 61.85 (24.46) | 64.00 | 50 | 35.64 (24.48) | 39.00 | 46 | −2.258 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghiţă, A.; Hernández-Serrano, O.; Fernández-Ruiz, Y.; Monras, M.; Ortega, L.; Mondon, S.; Teixidor, L.; Gual, A.; Porras-García, B.; Ferrer-García, M.; et al. Cue-Elicited Anxiety and Alcohol Craving as Indicators of the Validity of ALCO-VR Software: A Virtual Reality Study. J. Clin. Med. 2019, 8, 1153. https://doi.org/10.3390/jcm8081153
Ghiţă A, Hernández-Serrano O, Fernández-Ruiz Y, Monras M, Ortega L, Mondon S, Teixidor L, Gual A, Porras-García B, Ferrer-García M, et al. Cue-Elicited Anxiety and Alcohol Craving as Indicators of the Validity of ALCO-VR Software: A Virtual Reality Study. Journal of Clinical Medicine. 2019; 8(8):1153. https://doi.org/10.3390/jcm8081153
Chicago/Turabian StyleGhiţă, Alexandra, Olga Hernández-Serrano, Yolanda Fernández-Ruiz, Miquel Monras, Lluisa Ortega, Silvia Mondon, Lidia Teixidor, Antoni Gual, Bruno Porras-García, Marta Ferrer-García, and et al. 2019. "Cue-Elicited Anxiety and Alcohol Craving as Indicators of the Validity of ALCO-VR Software: A Virtual Reality Study" Journal of Clinical Medicine 8, no. 8: 1153. https://doi.org/10.3390/jcm8081153
APA StyleGhiţă, A., Hernández-Serrano, O., Fernández-Ruiz, Y., Monras, M., Ortega, L., Mondon, S., Teixidor, L., Gual, A., Porras-García, B., Ferrer-García, M., & Gutiérrez-Maldonado, J. (2019). Cue-Elicited Anxiety and Alcohol Craving as Indicators of the Validity of ALCO-VR Software: A Virtual Reality Study. Journal of Clinical Medicine, 8(8), 1153. https://doi.org/10.3390/jcm8081153