Risk of Incident Non-Valvular Atrial Fibrillation after Dialysis-Requiring Acute Kidney Injury

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
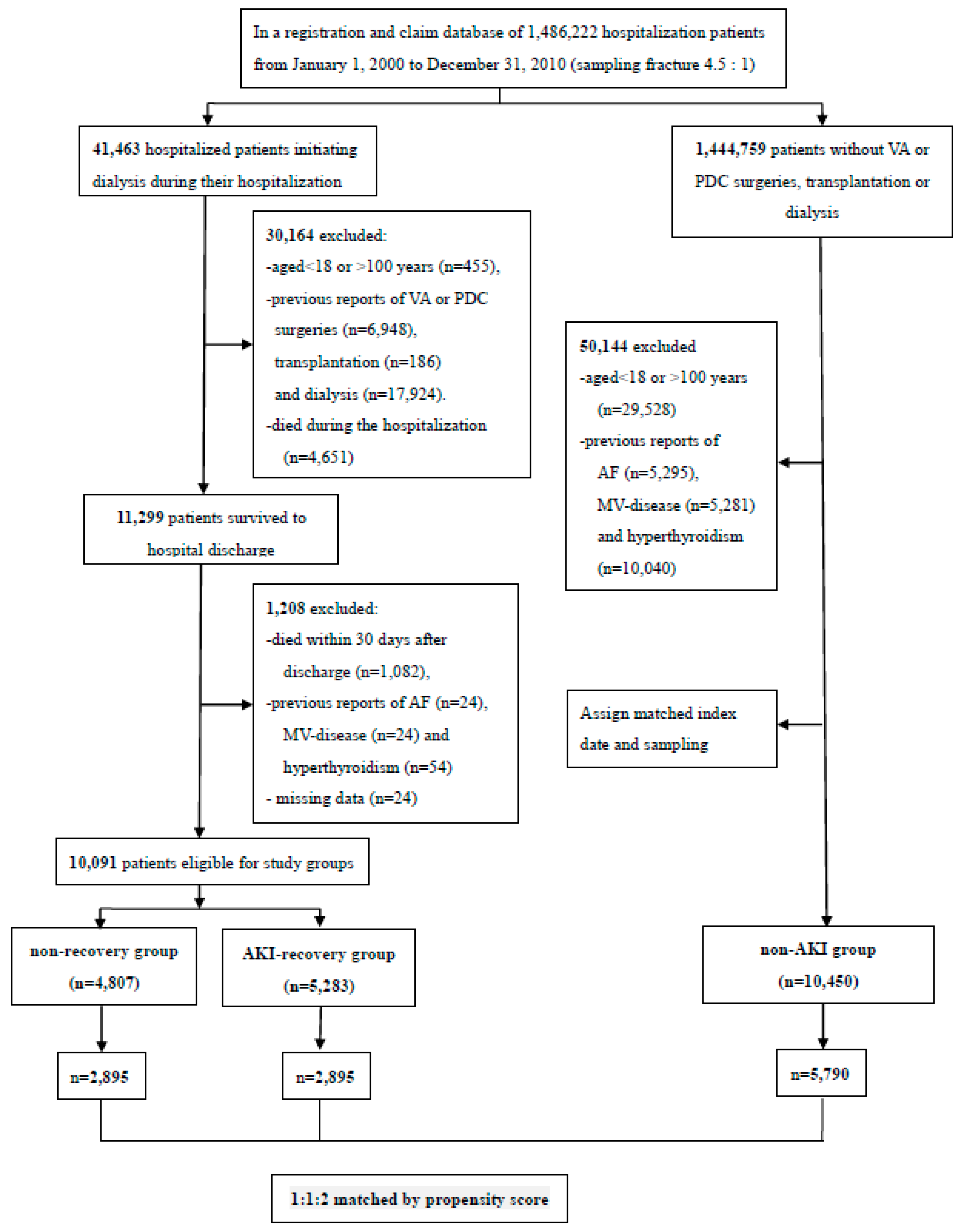
2.2. Study Cohort and Design
2.3. Research Variables
2.4. Outcome Variables
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Three Groups
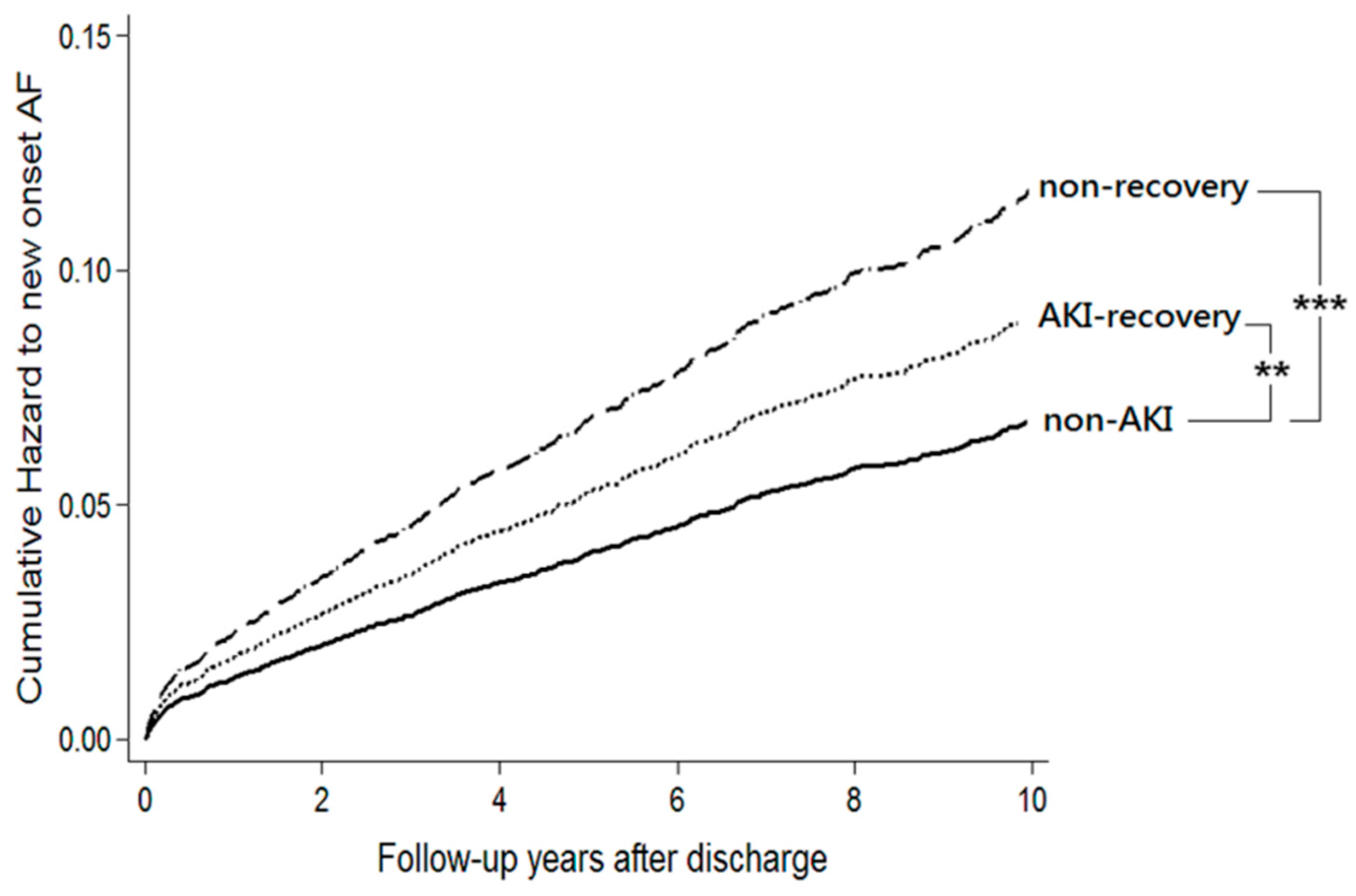
3.2. Risk of Incident Atrial Fibrillation
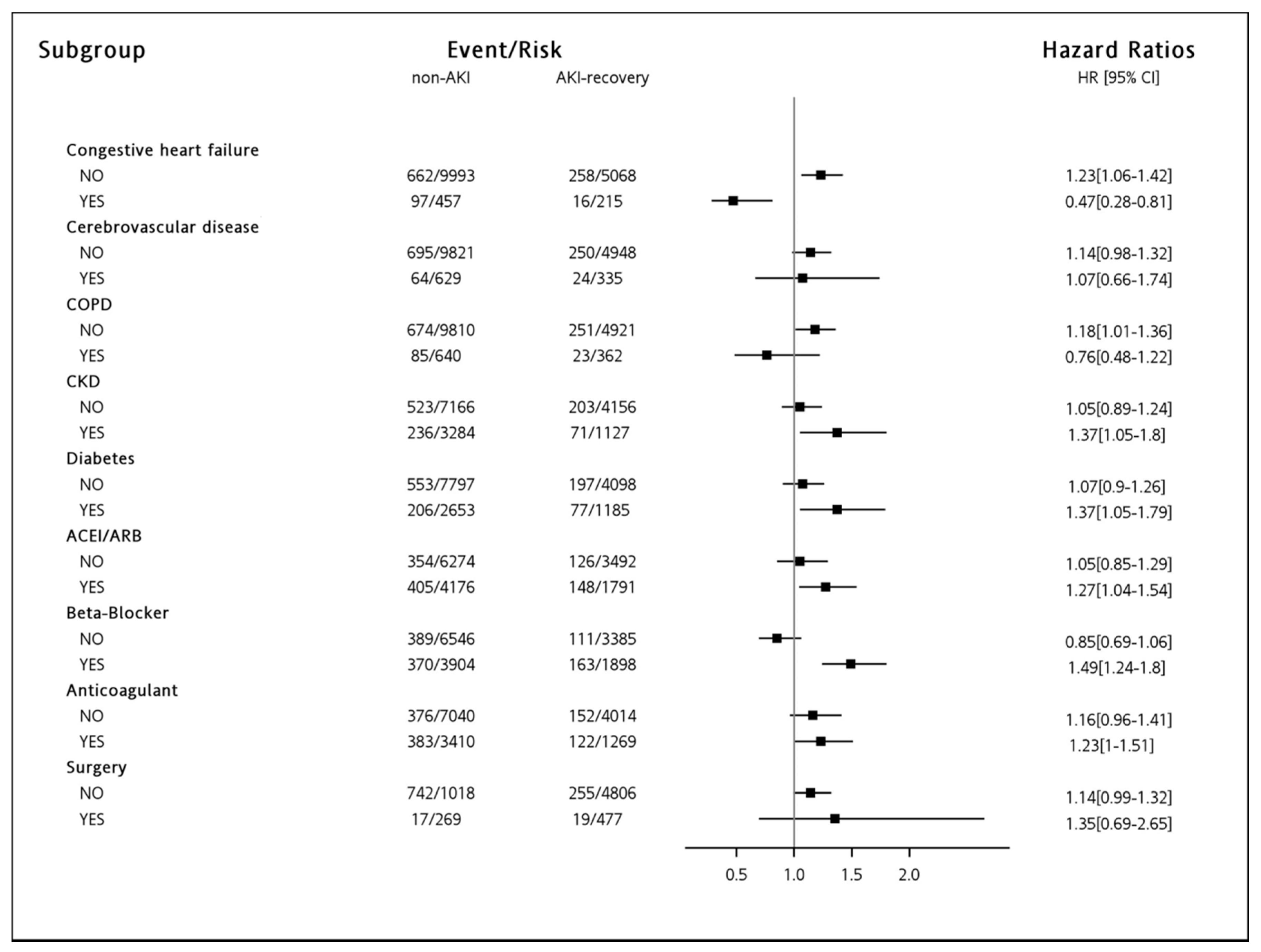
3.3. Risk of Incident Atrial Fibrillation in Subgroups
3.4. Risk of Major Adverse Events between Patients with and without Incident Atrial Fibrillation
4. Discussion
4.1. Acute Kidney Injury and Atrial Fibrillation
4.2. Major Adverse Events Associated with Atrial Fibrillation
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rahman, F.; Kwan, G.F.; Benjamin, E.J. Global epidemiology of atrial fibrillation. Nat. Rev. Cardiol. 2014, 11, 639–654. [Google Scholar] [CrossRef] [PubMed]
- Chan, L.; Mehta, S.; Chauhan, K.; Poojary, P.; Patel, S.; Pawar, S.; Patel, A.; Correa, A.; Patel, S.; Garimella, P.S.; et al. National trends and impact of acute kidney injury requiring hemodialysis in hospitalizations with atrial fibrillation. J. Am. Hear. Assoc. 2016, 5, e004509. [Google Scholar] [CrossRef] [PubMed]
- Wu, V.C.; Wu, C.H.; Huang, T.M.; Wang, C.Y.; Lai, C.F.; Shiao, C.C.; Chang, C.H.; Lin, S.L.; Chen, Y.Y.; Chen, Y.M.; et al. Long-term risk of coronary events after AKI. J. Am. Soc. Nephrol. 2014, 25, 595–605. [Google Scholar] [CrossRef] [PubMed]
- Wu, V.C.; Wu, P.C.; Wu, C.H.; Huang, T.M.; Chang, C.H.; Tsai, P.R.; Ko, W.J.; Chen, L.; Wang, C.Y.; Chu, T.S.; et al. The impact of acute kidney injury on the long-term risk of stroke. J. Am. Heart Assoc. 2014, 3, e000933. [Google Scholar] [CrossRef] [PubMed]
- Shiao, C.C.; Wu, P.C.; Huang, T.M.; Lai, T.S.; Yang, W.S.; Wu, C.H.; Lai, C.F.; Wu, V.C.; Chu, T.S.; Wu, K.D.; et al. Long-term remote organ consequences following acute kidney injury. Crit. Care 2015, 19, 438. [Google Scholar] [CrossRef] [PubMed]
- Diplaris, K.; Ampatzidou, F.; Karagounnis, L.; Drossos, G.; Vlahou, A. The role of blood transfusion in the development of atrial fibrillation after coronary artery bypass grafting. Thorac. Cardiovasc. Surg. 2016, 64, 688–692. [Google Scholar] [CrossRef] [PubMed]
- Ng, R.R.G.; Tan, G.H.J.; Liu, W.; Ti, L.K.; Chew, S.T.H. The association of acute kidney injury and atrial fibrillation after cardiac surgery in an asian prospective cohort study. Medicine 2016, 95, e3005. [Google Scholar] [CrossRef] [PubMed]
- Maesen, B.; Nijs, J.; Maessen, J.; Allessie, M.; Schotten, U. Post-operative atrial fibrillation: A maze of mechanisms. Europace 2011, 14, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Ommen, S.R.; Odell, J.A.; Stanton, M.S. Atrial arrhythmias after cardiothoracic surgery. New Engl. J. Med. 1997, 336, 1429–1434. [Google Scholar] [CrossRef] [PubMed]
- Auer, J.; Lamm, G.; Weber, T.; Berent, R.; Ng, C.-K.; Porodko, M.; Eber, B. Renal function is associated with risk of atrial fibrillation after cardiac surgery. Can. J. Cardiol. 2007, 23, 859–863. [Google Scholar] [CrossRef]
- Lin, L.-J.; Cheng, M.-H.; Lee, C.-H.; Wung, D.-C.; Cheng, C.-L.; Kao Yang, Y.-H. Compliance with antithrombotic prescribing guidelines for patients with atrial fibrillation—A nationwide descriptive study in taiwan. Clin. Ther. 2008, 30, 1726–1736. [Google Scholar] [CrossRef] [PubMed]
- Chao, T.-F.; Huang, Y.-C.; Liu, C.-J.; Chen, S.-J.; Wang, K.-L.; Lin, Y.-J.; Chang, S.-L.; Lo, L.-W.; Hu, Y.-F.; Tuan, T.-C.; et al. Acute myocardial infarction in patients with atrial fibrillation with a cha2ds2-vasc score of 0 or 1: A nationwide cohort study. Hear. Rhythm. 2014, 11, 1941–1947. [Google Scholar] [CrossRef] [PubMed]
- Jensen, P.N.; Johnson, K.; Floyd, J.; Heckbert, S.R.; Carnahan, R.; Dublin, S. A systematic review of validated methods for identifying atrial fibrillation using administrative data. Pharmacoepidemiol. Drug Saf. 2012, 21, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.J.; Chao, C.T.; Huang, Y.C.; Wang, C.Y.; Chang, C.H.; Huang, T.M.; Lai, C.F.; Huang, H.Y.; Shiao, C.C.; Chu, T.S.; et al. The impact of acute kidney injury with temporary dialysis on the risk of fracture. J. Bone Miner. Res. 2013, 29, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Chao, T.-F.; Liu, C.-J.; Tuan, T.-C.; Chen, T.-J.; Hsieh, M.-H.; Lip, G.Y.H.; Chen, S.-A. Lifetime Risks, Projected Numbers, and Adverse Outcomes in Asian Patients With Atrial Fibrillation: A Report From the Taiwan Nationwide AF Cohort Study. Chest 2018, 153, 453–466. [Google Scholar] [CrossRef] [PubMed]
- Chien, K.-L.; Su, T.-C.; Hsu, H.-C.; Chang, W.-T.; Chen, P.-C.; Chen, M.-F.; Lee, Y.-T. Atrial fibrillation prevalence, incidence and risk of stroke and all-cause death among Chinese. Int. J. Cardiol. 2010, 139, 173–180. [Google Scholar] [CrossRef] [PubMed]
- January, C.T.; Wann, L.S.; Alpert, J.S.; Calkins, H.; Cigarroa, J.E.; Cleveland, J.C., Jr.; Conti, J.B.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 2014, 64, e1–e76. [Google Scholar] [CrossRef] [PubMed]
- Ologunde, R.; Zhao, H.; Lu, K.; Ma, D. Organ cross talk and remote organ damage following acute kidney injury. Int. Urol. Nephrol. 2014, 46, 2337–2345. [Google Scholar] [CrossRef] [PubMed]
- Grams, M.E.; Rabb, H. The distant organ effects of acute kidney injury. Kidney Int. 2012, 81, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Kelly, K.J. Distant effects of experimental renal ischemia/reperfusion injury. J. Am. Soc. Nephrol. 2003, 14, 1549–1558. [Google Scholar] [CrossRef] [PubMed]
- Bhalodia, Y.S.; Sheth, N.R.; Vaghasiya, J.D.; Jivani, N.P. Homocysteine-dependent endothelial dysfunction induced by renal ischemia/reperfusion injury. J. Nephrol. 2011, 24, 631–635. [Google Scholar] [CrossRef] [PubMed]
- Kelly, K.J.; Meehan, S.M.; Colvin, R.B.; Williams, W.W.; Bonventre, J.V. Protection from toxicant-mediated renal injury in the rat with anti-cd54 antibody. Kidney Int. 1999, 56, 922–931. [Google Scholar] [CrossRef] [PubMed]
- Leaf, D.E.; Christov, M.; Jüppner, H.; Siew, E.; Ikizler, T.A.; Bian, A.; Chen, G.; Sabbisetti, V.S.; Bonventre, J.V.; Cai, X.; et al. Fibroblast growth factor 23 levels are elevated and associated with severe acute kidney injury and death following cardiac surgery. Kidney Int. 2016, 89, 939–948. [Google Scholar] [CrossRef] [PubMed]
- Mathew, J.S.; Sachs, M.C.; Katz, R.; Patton, K.K.; Heckbert, S.R.; Hoofnagle, A.N.; Alonso, A.; Chonchol, M.; Deo, R.; Ix, J.H.; et al. Fibroblast growth factor-23 and incident atrial fibrillation: the multi-ethnic study of atherosclerosis (mesa) and the cardiovascular health study (chs). Circulation 2014, 130, 298–307. [Google Scholar] [CrossRef] [PubMed]
- Sciacqua, A.; Perticone, M.; Tripepi, G.; Miceli, S.; Tassone, E.J.; Grillo, N.; Carullo, G.; Sesti, G.; Perticone, F. Renal disease and left atrial remodeling predict atrial fibrillation in patients with cardiovascular risk factors. Int. J. Cardiol. 2014, 175, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Cao, W.; Li, A.; Li, J.; Wu, C.; Cui, S.; Zhou, Z.; Liu, Y.; Wilcox, C.S.; Hou, F.F. Reno-cerebral reflex activates the renin-angiotensin system, promoting oxidative stress and renal damage after ischemia-reperfusion injury. Antioxid. Redox Signal 2017, 27, 415–432. [Google Scholar] [CrossRef] [PubMed]
- Lane, K.; Dixon, J.J.; MacPhee, I.A.M.; Philips, B.J. Renohepatic crosstalk: Does acute kidney injury cause liver dysfunction? Nephrol. Dial. Transplant. 2013, 28, 1634–1647. [Google Scholar] [CrossRef] [PubMed]
- Roldan, V.; Marin, F.; Fernandez, H.; Manzano-Fernandez, S.; Gallego, P.; Valdes, M.; Vicente, V.; Lip, G.Y. Renal impairment in a “real-life” cohort of anticoagulated patients with atrial fibrillation (implications for thromboembolism and bleeding). Am. J. Cardiol. 2013, 111, 1159–1164. [Google Scholar] [CrossRef] [PubMed]
- Peng, X.S.; Meng, G.W.; Zhang, J.; Wang, X.F.; Zhao, L.X.; Wang, Y.W.; Zhang, L.D. Electrochemical fabrication of ordered Ag2S nanowire arrays. Mater. Res. Bull. 2002, 37, 1369–1375. [Google Scholar] [CrossRef]
- Violi, F.; Pastori, D.; Perticone, F.; Hiatt, W.R.; Sciacqua, A.; Basili, S.; Proietti, M.; Corazza, G.R.; Lip, G.Y.H.; Pignatelli, P. Relationship between low ankle-brachial index and rapid renal function decline in patients with atrial fibrillation: A prospective multicentre cohort study. BMJ Open 2015, 5, e008026. [Google Scholar] [CrossRef] [PubMed]
- Brodsky, S.V.; Hebert, L.A. Anticoagulant-Related Nephropathy: Is an AKI Elephant Hiding in Plain View? J. Am. Coll. Cardiol. 2016, 68, 2284–2286. [Google Scholar] [CrossRef] [PubMed]
- Bohm, M.; Ezekowitz, M.D.; Connolly, S.J.; Eikelboom, J.W.; Hohnloser, S.H.; Reilly, P.A.; Schumacher, H.; Brueckmann, M.; Schirmer, S.H.; Kratz, M.T.; et al. Changes in renal function in patients with Atrial Fibrillation: An analysis from the RE-LY Trial. J. Am. Coll. Cardiol. 2015, 65, 2481–2493. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.H.; Yeh, Y.H.; See, L.C.; Wang, C.L.; Chang, S.H.; Lee, H.F.; Wu, L.S.; Tu, H.T.; Kuo, C.T. Acute kidney injury in Asians with atrial fibrillation treated with dabigatran or warfarin. J. Am. Coll. Cardiol. 2016, 68, 2272–2283. [Google Scholar] [CrossRef] [PubMed]
- Soliman, E.Z.; Safford, M.M.; Muntner, P.; Khodneva, Y.; Dawood, F.Z.; Zakai, N.A.; Thacker, E.L.; Judd, S.; Howard, V.J.; Howard, G.; et al. Atrial fibrillation and the risk of myocardial infarction. JAMA Intern. Med. 2014, 174, 107–114. [Google Scholar] [CrossRef] [PubMed]
- O’Neal, W.T.; Sangal, K.; Zhang, Z.-M.; Soliman, E.Z. Atrial fibrillation and incident myocardial infarction in the elderly. Clin. Cardiol. 2014, 37, 750–755. [Google Scholar] [CrossRef] [PubMed]
- Ruddox, V.; Sandven, I.; Munkhaugen, J.; Skattebu, J.; Edvardsen, T.; Otterstad, J.E. Atrial fibrillation and the risk for myocardial infarction, all-cause mortality and heart failure: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2017, 24, 1555–1566. [Google Scholar] [CrossRef] [PubMed]
- Emdin, C.A.; Wong, C.X.; Hsiao, A.J.; Altman, D.G.; Peters, S.A.; Woodward, M.; Odutayo, A.A. Atrial fibrillation as risk factor for cardiovascular disease and death in women compared with men: Systematic review and meta-analysis of cohort studies. BMJ 2016, 352, h7013. [Google Scholar] [CrossRef] [PubMed]
- Pastori, D.; Pignatelli, P.; Angelico, F.; Farcomeni, A.; Del Ben, M.; Vicario, T.; Bucci, T.; Raparelli, V.; Cangemi, R.; Tanzilli, G.; Lip, G.Y.H.; Violi, F. Incidence of myocardial infarction and vascular death in elderly patients with atrial fibrillation taking anticoagulants. Chest 2015, 147, 1644–1650. [Google Scholar] [CrossRef] [PubMed]
- Tornyos, A.; Kehl, D.; D’Ascenzo, F.; Komócsi, A. Risk of myocardial infarction in patients with long-term non-vitamin k antagonist oral anticoagulant treatment. Prog. Cardiovasc. Dis. 2016, 58, 483–494. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.J.; Gerds, T.A.; Carlson, N.; Bonde, A.N.; Gislason, G.H.; Lamberts, M.; Olesen, J.B.; Pallisgaard, J.L.; Hansen, M.L.; Torp-Pedersen, C. Risk of myocardial infarction in anticoagulated patients with atrial fibrillation. J. Am. Coll. Cardiol. 2018, 72, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Li, P.K.T.; Burdmann, E.A.; Mehta, R.L. World kidney day 2013: Acute kidney injury—global health alert. Am. J. Kidney Dis. 2013, 61, 359–363. [Google Scholar] [CrossRef] [PubMed]
- Liangos, O.; Wald, R.; O’Bell, J.W.; Price, L.; Pereira, B.J.; Jaber, B.L. Epidemiology and outcomes of acute renal failure in hospitalized patients: A national survey. Clin. J. Am. Soc. Nephrol. 2006, 1, 43–51. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Before Matching n = 20,540 | After Matching n = 11,680 | |||||||
|---|---|---|---|---|---|---|---|---|
| Variables | Non-Recovery n = 4807 | AKI-Recovery n = 5283 | Non-AKI n = 10,450 | p | Non-Recovery n = 2895 | AKI-Recovery n = 2895 | Non-AKI n = 5790 | p |
| Age, years | 59.7 ± 15.2 | 60.3 ± 17.7 | 59.8 ± 16.1 | <0.001 | 59.6 ± 15.7 | 60.2 ± 17.2 | 60.6 ± 15.7 | 0.01 |
| Gender, men | 2390 (49.7%) | 3172 (60.0%) | 5540 (53.0%) | <0.001 | 1542 (53.3%) | 1535 (53.0%) | 3178 (54.9%) | 0.68 |
| Monthly income, NTD | <0.001 | 0.21 | ||||||
| <19,100 | 1700 (35.4%) | 2103 (39.8%) | 3649 (34.9%) | 1064 (36.8%) | 1099 (38.0%) | 2203 (38.1%) | ||
| 19,100–41,999 | 2449 (51.0%) | 2434 (46.1%) | 5285 (50.6%) | 1443 (49.8%) | 1378 (47.6%) | 2925 (50.5%) | ||
| ≥42,000 | 658 (13.7%) | 746 (14.1%) | 1516 (14.5%) | 388 (13.4%) | 418 (14.4%) | 762 (13.2%) | ||
| Hospital level * | <0.001 | <0.001 | ||||||
| Level 1 | 1916 (39.9%) | 2648 (50.1%) | 4046 (38.7%) | 1218 (42.1%) | 1184 (40.9%) | 2641 (45.6%) | ||
| Level 2 | 2092 (43.5%) | 2158 (40.84%) | 3972 (38.0%) | 1249 (43.1%) | 1340 (46.3%) | 2282 (39.4%) | ||
| Levels 3 + 4 | 799 (16.6%) | 477 (9.0%) | 2,432 (23.3%) | 428 (14.8%) | 371 (12.8%) | 967 (16.7%) | ||
| Baseline Comorbidities | ||||||||
| CCI | 2.8 ± 1.6 | 2.1 ± 1.5 | 2.4 ± 1.6 | <0.001 | 2.4 ± 1.6 | 2.4 ± 1.6 | 2.4 ± 1.6 | 0.29 |
| Myocardial infarction | 22 (0.5%) | 27 (0.5%) | 37 (0.4%) | 0.31 | 12 (0.4%) | 10 (0.4%) | 22 (0.4%) | 0.91 |
| Congestive heart failure | 287 (6.0%) | 215 (4.1%) | 457 (4.4%) | <0.001 | 131 (4.5%) | 136 (4.7%) | 279 (4.8%) | 0.91 |
| Peripheral vascular disease | 26 (0.5%) | 34 (0.6%) | 54 (0.5%) | 0.59 | 13 (0.5%) | 17 (0.6%) | 39 (0.7%) | 0.47 |
| Cerebrovascular disease | 284 (5.9%) | 335 (6.3%) | 629 (6.0%) | 0.62 | 175 (6.0%) | 173 (6.0%) | 345 (6.0%) | 0.94 |
| Dementia | 24 (0.5%) | 74 (1.4%) | 68 (0.7%) | <0.001 | 20 (0.7%) | 19 (0.7%) | 35 (0.6%) | 0.85 |
| COPD | 333 (6.9%) | 362 (6.9%) | 640 (6.1%) | 0.08 | 179 (6.2%) | 209 (7.2%) | 414 (7.2%) | 0.23 |
| Rheumatologic disease | 47 (1.0%) | 61 (1.2%) | 103 (1.0%) | 0.57 | 30 (1.0%) | 28 (1.0%) | 69 (1.2%) | 0.66 |
| Peptic ulcer disease | 403 (8.4%) | 350 (6.6%) | 691 (6.6%) | <0.001 | 205 (7.1%) | 207 (7.2%) | 450 (7.8%) | 0.55 |
| Hemiplegia or paraplegia | 10 (0.2%) | 20 (0.4%) | 25 (0.2%) | 0.18 | 8 (0.3%) | 9 (0.3%) | 13 (0.2%) | 0.71 |
| CKD | 2396 (49.8%) | 1063 (20.1%) | 3225 (30.9%) | <0.001 | 1005 (34.7%) | 932 (32.2%) | 1910 (33.0%) | 0.06 |
| Liver disease a | 178 (3.7%) | 204 (3.9%) | 355 (3.4%) | 0.30 | 96 (3.3%) | 99 (3.4%) | 192 (3.3%) | 0.93 |
| Tumor | 86 (1.8%) | 137 (2.6%) | 195 (1.9%) | 0.004 | 62 (2.1%) | 56 (1.9%) | 113 (2.0%) | 0.77 |
| Diabetes | 1254 (26.1%) | 1186 (22.5%) | 2653 (25.4%) | <0.001 | 687 (23.7%) | 708 (24.5%) | 1504 (26.0%) | 0.16 |
| CHA2DS2-VASc † | <0.001 | <0.001 | ||||||
| 0 | 211 (4.4%) | 706 (13.4%) | 1018 (9.7%) | 204 (7.1%) | 200 (6.9%) | 400 (6.9%) | ||
| 1 | 890 (18.5%) | 996 (18.9%) | 1979 (18.9%) | 636 (22.0%) | 631 (21.8%) | 1125 (19.4%) | ||
| 2 | 1268 (26.4%) | 976 (18.5%) | 1908 (18.3%) | 834 (28.8%) | 613 (21.2%) | 1144 (19.8%) | ||
| 3 | 885 (18.4%) | 858 (16.2%) | 1896 (18.1%) | 534 (18.5%) | 505 (17.4%) | 1124 (19.4%) | ||
| 4 | 706 (14.7%) | 683 (12.9%) | 1462 (14.0%) | 438 (15.1%) | 410 (14.2%) | 894 (15.4%) | ||
| 5 | 456 (9.5%) | 483 (9.1%) | 1123 (10.8%) | 279 (9.6%) | 307 (10.6%) | 691 (11.9%) | ||
| 6 | 245 (5.1%) | 350 (6.6%) | 660 (6.3%) | 194 (6.7%) | 158 (5.5%) | 306 (5.3%) | ||
| 7 | 120 (2.5%) | 174 (3.3%) | 296 (2.8%) | 98 (3.4%) | 91 (3.1%) | 155 (2.7%) | ||
| 8 | 24 (0.5%) | 50 (1.0%) | 99 (1.0%) | 23 (0.8%) | 27 (0.9%) | 45 (0.8%) | ||
| 9 | 2 (0.04%) | 7 (0.1%) | 9 (0.1%) | 2 (0.1%) | 3 (0.1%) | 6 (0.1%) | ||
| Before Matching n = 20,540 | After Matching n = 11,680 | |||||||
|---|---|---|---|---|---|---|---|---|
| Variables | Non-Recovery n = 4807 | AKI-Recovery n = 5283 | Non-AKI n = 10,450 | p | Non-Recovery n = 2895 | AKI-Recovery n = 2895 | Non-AKI n = 5790 | p |
| Outpatient visits, times ‡ | < 0.001 | 0.09 | ||||||
| 0–5 visits | 4596 (95.6%) | 4932 (93.3%) | 9297 (89.0%) | 2763 (95.4%) | 2747 (94.9%) | 5530 (95.5%) | ||
| 6–10 visits | 121 (2.5%) | 151 (2.9%) | 450 (4.3%) | 67 (2.3%) | 74 (2.6%) | 190 (3.3%) | ||
| 11–15 visits | 66 (1.4%) | 123 (2.3%) | 479 (4.6%) | 47 (1.6%) | 50 (1.7%) | 123 (2.1%) | ||
| >15 visits | 24 (0.5%) | 77 (1.5%) | 224 (2.1%) | 18 (0.6%) | 24 (0.8%) | 47 (0.8%) | ||
| Medication for hypertension ‡ | ||||||||
| Alpha-Blocker | 571 (11.9%) | 629 (11.9%) | 1000 (9.6%) | <0.001 | 358 (12.4%) | 341 (11.8%) | 698 (12.1%) | 0.74 |
| Beta-Blocker | 2000 (41.6%) | 1898 (35.9%) | 3904 (37.4%) | <0.001 | 1129 (39.0%) | 1143 (39.5%) | 2369 (40.9%) | 0.52 |
| Calcium-Channel Blocker | 3006 (62.5%) | 2610 (49.4%) | 4986 (47.7%) | <0.001 | 1614 (55.8%) | 1630 (56.3%) | 3360 (58.0%) | 0.49 |
| Diuretic | 1707 (35.5%) | 2485 (47.0%) | 4168 (39.9%) | <0.001 | 1193 (41.2%) | 1231 (42.5%) | 2522 (43.6%) | 0.35 |
| ACEI/ARB | 1725 (35.9%) | 1791 (33.9%) | 4176 (40.0%) | <0.001 | 1057 (36.5%) | 1073 (37.1%) | 2231 (38.5%) | 0.44 |
| Other Medication ‡ | ||||||||
| Anti-diabetic drugs | 1468 (30.5%) | 1595 (30.2%) | 3230 (30.9%) | 0.57 | 849 (29.3%) | 887 (30.6%) | 1846 (31.9%) | 0.16 |
| Aspirin | 411 (8.6%) | 396 (7.5%) | 1259 (12.1%) | <0.001 | 246 (8.5%) | 247 (8.5%) | 517 (8.9%) | 0.88 |
| Clopidogrel | 143 (3.0%) | 291 (5.5%) | 443 (4.2%) | <0.001 | 104 (3.6%) | 114 (3.9%) | 212 (3.7%) | 0.70 |
| Ticlopidine | 208 (4.33%) | 117 (2.2%) | 370 (3.5%) | <0.001 | 85 (2.9%) | 86 (3.0%) | 194 (3.4%) | 0.57 |
| Dipyridamole | 1059 (22.0%) | 792 (15.0%) | 2224 (21.3%) | <0.001 | 538 (18.6%) | 555 (19.2%) | 1147 (19.8%) | 0.61 |
| Nitrate | 868 (18.1%) | 1050 (19.9%) | 1262 (12.1%) | <0.001 | 501 (17.3%) | 524 (18.1%) | 1053 (18.2%) | 0.71 |
| Statin | 519 (10.8%) | 628 (11.9%) | 1524 (15.6%) | <0.001 | 334 (11.5%) | 355 (12.3%) | 743 (12.8%) | 0.35 |
| Proton pump inhibitor | 26 (0.5%) | 57 (1.1%) | 64 (0.6%) | 0.001 | 24 (0.8%) | 22 (0.8%) | 42 (0.7%) | 0.84 |
| NSAID | 3062 (63.7%) | 2832 (53.6%) | 7863 (75.2%) | <0.001 | 1811 (65.6%) | 1833 (63.3%) | 3707 (64.0%) | 0.84 |
| H2-blocker | 1173 (24.4%) | 1232 (23.3%) | 2718 (26.0%) | <0.001 | 692 (23.9%) | 739 (25.5%) | 1535 (26.5%) | 0.09 |
| Outcome ‡‡ | ||||||||
| Atrial fibrillation | 384 (8.0%) | 274 (5.2%) | 759 (7.3%) | <0.001 | 214 (7.4%) | 149 (5.2%) | 383 (6.6%) | 0.002 |
| MACE | 830 (17.3%) | 617 (11.7%) | 1449 (13.9%) | <0.001 | 467 (16.1%) | 333 (11.5%) | 772 (13.3%) | <0.001 |
| Ischemia Stroke | 1226 (25.5%) | 824 (15.6%) | 4195 (40.1%) | <0.001 | 696 (24.0%) | 481 (16.6%) | 2286 (39.5%) | <0.001 |
| Hemorrhage Stroke | 367 (7.6%) | 229 (4.3%) | 1176 (11.3%) | <0.001 | 222 (7.7%) | 140 (4.8%) | 719 (13.7%) | <0.001 |
| All stroke | 1399 (29.1%) | 944 (17.9%) | 4748 (45.4%) | <0.001 | 802 (27.7%) | 555 (19.2%) | 2617 (45.2%) | <0.001 |
| Advanced CKD | 988 (20.6%) | 723 (13.7%) | 702 (6.8%) | <0.001 | 822 (28.4%) | 482 (16.6%) | 423 (7.3%) | <0.001 |
| Mortality | 2486 (51.7%) | 2204 (41.7%) | 3025 (29.0%) | <0.001 | 1482 (51.2%) | 1188 (41.0 %) | 1890 (32.6%) | <0.001 |
| Atrial Fibrillation | Crude Risk | Adjusted Risk ‡ | Adjusted Risk ‡‡ | |||
|---|---|---|---|---|---|---|
| Events | Person-Years | Incidence Rate § | HR (95% CI) | aHR (95% CI) | aHR (95% CI) | |
| Before propensity score-matching | ||||||
| non-AKI | 759 | 81,186.67 | 0.94 | ref | ref | ref |
| AKI-recovery | 274 | 24,007.06 | 1.14 | 1.08 (0.94–1.24) | 1.16 (1.00–1.33) | 1.15 (1.10–1.32) |
| non-recovery | 384 | 28,726.82 | 1.34 | 1.36 *** (1.20–1.54) | 1.62 *** (1.43–1.83) | 1.58 *** (1.39–1.80) |
| After propensity score-matching | ||||||
| non-AKI | 383 | 45,562.79 | 0.84 | ref | ref | ref |
| AKI-recovery | 149 | 13,462.42 | 1.11 | 1.18 (0.98–1.43) | 1.33 ** (1.10–1.61) | 1.30 ** (1.07–1.58) |
| non-recovery | 214 | 17,088.48 | 1.25 | 1.42 *** (1.20–1.68) | 1.72 *** (1.45–2.03) | 1.62 *** (1.36–1.94) |
| AF | Non-AF | Crude Risk | Adjusted Risk ‡ | |||||
|---|---|---|---|---|---|---|---|---|
| Event | Person-Year | Incidence Rate § | Event | Person-Year | Incidence Rate § | HR (95% CI) | HR (95% CI) | |
| Before propensity score-matching | ||||||||
| MACE | 987 | 9230.59 | 10.69 | 2466 | 117,959.62 | 2.09 | 2.25 ** (2.03–2.49) | 1.88 ** (1.70–2.09) |
| Hemorrhagic stroke | 161 | 10,381.48 | 1.55 | 1611 | 121,543.88 | 1.33 | 1.20 * (1.02–1.41) | 1.24 * (1.05–1.46) |
| Ischemic stroke | 667 | 7077.34 | 9.42 | 5578 | 96,917.20 | 5.76 | 1.62 ** (1.49–1.75) | 1.31 ** (1.21–1.42) |
| Total stroke | 714 | 6867.78 | 10.40 | 6377 | 93,540.77 | 6.82 | 1.50 ** (1.39–1.62) | 1.26 ** (1.17–1.36) |
| After propensity score-matching | ||||||||
| MACE | 511 | 4729.33 | 10.80 | 1337 | 67,595.80 | 1.98 | 2.49 ** (2.17–2.86) | 2.11 ** (1.83–2.43) |
| Hemorrhagic stroke | 89 | 5321.74 | 1.67 | 992 | 68,827.18 | 1.44 | 1.20 (0.97–1.49) | 1.23 (0.99–1.53) |
| Ischemic stroke | 333 | 3766.11 | 8.84 | 3130 | 55,361.13 | 5.65 | 1.57 ** (1.40–1.75) | 1.33 ** (1.19–1.49) |
| All Stroke | 362 | 3654.72 | 9.90 | 3612 | 53,357.19 | 6.77 | 1.46 ** (1.31–1.63) | 1.28 ** (1.15–1.43) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shiao, C.-C.; Kan, W.-C.; Wang, J.-J.; Lin, Y.-F.; Chen, L.; Chueh, E.; Huang, Y.-T.; Chiang, W.-P.; Tseng, L.-J.; Wang, C.-H.; et al. Risk of Incident Non-Valvular Atrial Fibrillation after Dialysis-Requiring Acute Kidney Injury. J. Clin. Med. 2018, 7, 248. https://doi.org/10.3390/jcm7090248
Shiao C-C, Kan W-C, Wang J-J, Lin Y-F, Chen L, Chueh E, Huang Y-T, Chiang W-P, Tseng L-J, Wang C-H, et al. Risk of Incident Non-Valvular Atrial Fibrillation after Dialysis-Requiring Acute Kidney Injury. Journal of Clinical Medicine. 2018; 7(9):248. https://doi.org/10.3390/jcm7090248
Chicago/Turabian StyleShiao, Chih-Chung, Wei-Chih Kan, Jian-Jhong Wang, Yu-Feng Lin, Likwang Chen, Eric Chueh, Ya-Ting Huang, Wen-Po Chiang, Li-Jung Tseng, Chih-Hsien Wang, and et al. 2018. "Risk of Incident Non-Valvular Atrial Fibrillation after Dialysis-Requiring Acute Kidney Injury" Journal of Clinical Medicine 7, no. 9: 248. https://doi.org/10.3390/jcm7090248
APA StyleShiao, C.-C., Kan, W.-C., Wang, J.-J., Lin, Y.-F., Chen, L., Chueh, E., Huang, Y.-T., Chiang, W.-P., Tseng, L.-J., Wang, C.-H., & Wu, V.-C. (2018). Risk of Incident Non-Valvular Atrial Fibrillation after Dialysis-Requiring Acute Kidney Injury. Journal of Clinical Medicine, 7(9), 248. https://doi.org/10.3390/jcm7090248