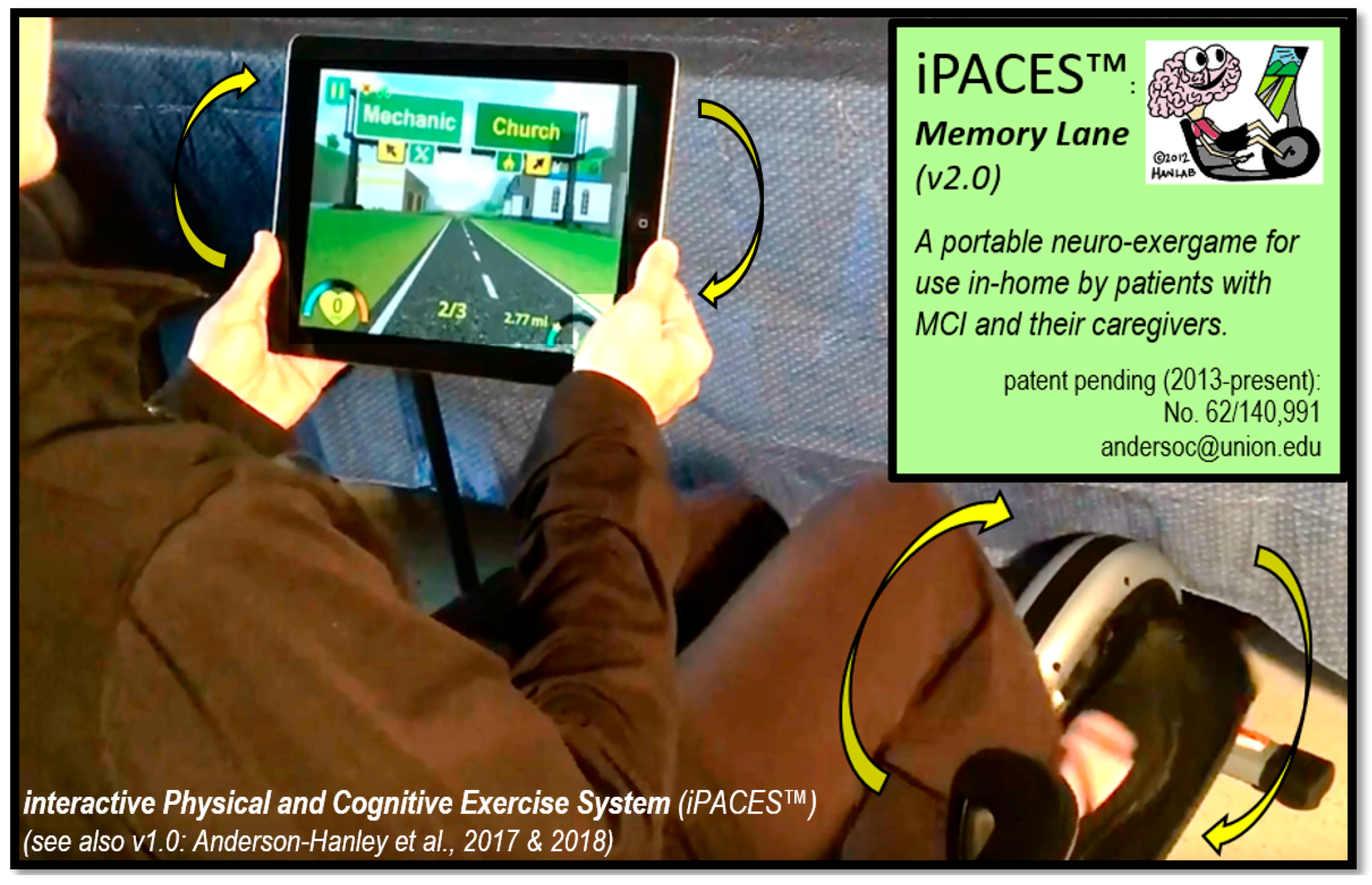
The Enhanced Interactive Physical and Cognitive Exercise System (iPACESTM v2.0): Pilot Clinical Trial of an In-Home iPad-Based Neuro-Exergame for Mild Cognitive Impairment (MCI)

 ,
, 
Abstract
:1. Introduction
1.1. Physical Exercise and Aging
1.2. Physical Exercise and Cognitive Decline (MCI)
1.3. Mental Exercise (Cognitive Training) and Cognitive Decline (MCI)
1.4. Combined Physical and Mental Exercise for MCI (e.g., Combined/Tandem or Interactive/Neuro-Exergaming)
1.5. Exercise, Cognition, and Biomarker Indicators
- cognitive improvement would be correlated with salivary biomarkers:
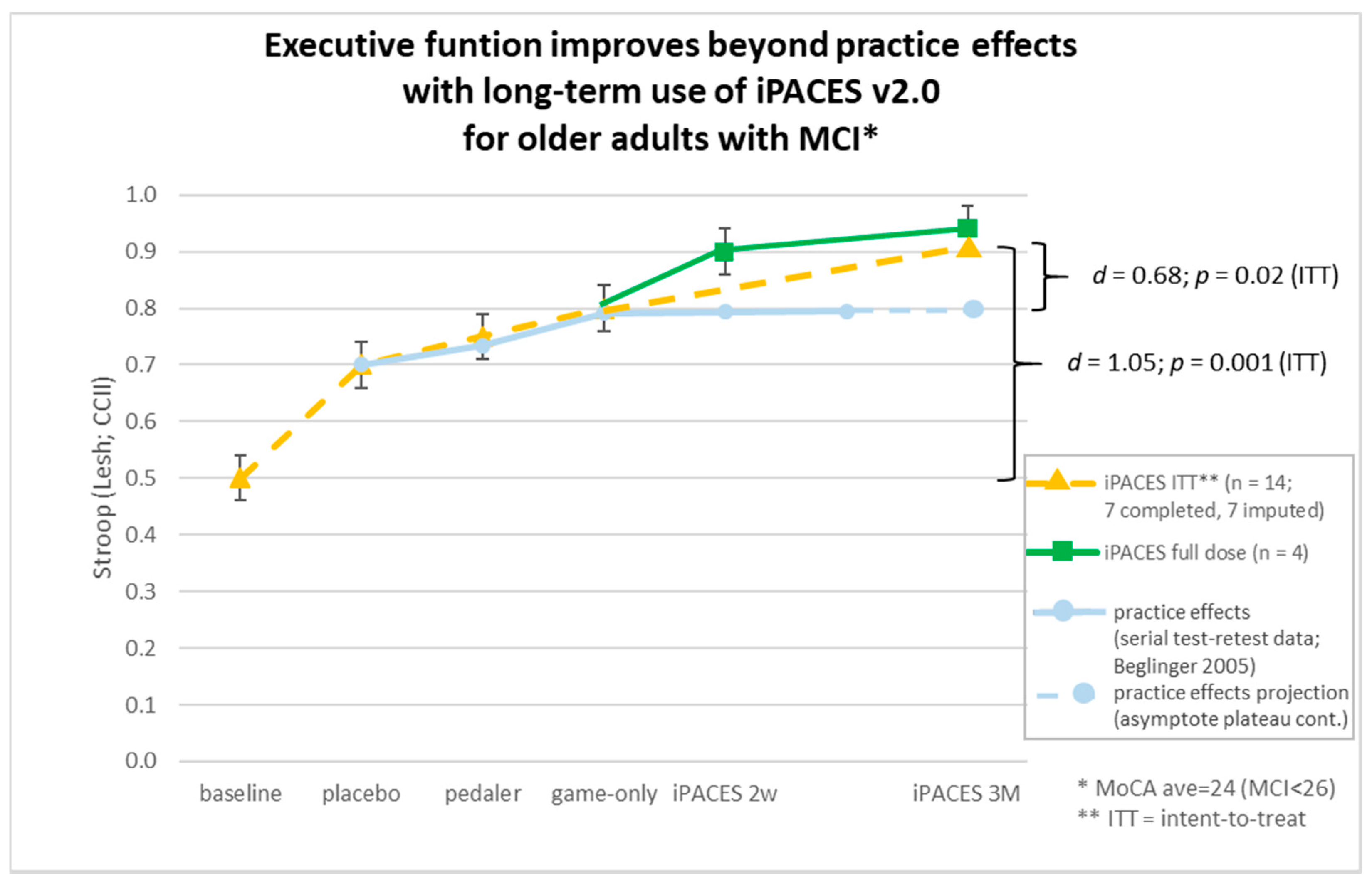
- a component familiarization period would not exceed standard practice effects [pedal-only and game-only practice periods were included to gradually train and prepare cognitively challenged participants for the more complex interactive neuro-exergaming experience (iPACES) and also these periods were anticipated to have a dual benefit of washing out any practice effects from serial cognitive testing such that the learning curve would be similar to that of published normative data] [101].
2. Experimental Section
2.1. Participants
2.2. Procedures
2.3. Measures
2.3.1. Neuropsychological Evaluation
2.3.2. Other Tests Administered
2.4. Materials
3. Results
3.1. Cognitive Results
3.2. Biomarker Results
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kirova, A.M.; Bays, R.B.; Lagalwar, S. Working memory and executive function decline across normal aging, mild cognitive impairment, and Alzheimer’s disease. Biol. Med. Res. Int. 2015, 2015. [Google Scholar] [CrossRef] [PubMed]
- Prince, M.; Wimo, A.; Guerchet, M.; Ali, G.; Wu, Y.; Prina, M. World Alzheimer Report 2015—The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends; Alzheimer’s Disease International: London, UK, 2015. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Publishing: Arlington, VA, USA, 2010; Volume 4. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Publishing: Arlington, VA, USA, 2013; Volume 5. [Google Scholar] [CrossRef]
- Plassman, B.L.; Langa, K.M.; Fisher, G.G.; Heeringa, S.G.; Weir, D.R.; Ofstedal, M.B.; Steffens, D.C. Prevalence of dementia in the United States: The aging, demographics, and memory study. Neuroepidemiology 2007, 29, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Alzheimer’s Association. Available online: https://www.alz.org/aaic/overview.asp (accessed on 26 July 2018).
- Alzheimer’s Disease International: World Alzheimer Report 2009. Available online: https://www.alz.co.uk/research/GlobalImpactDementia2013.pdf (accessed on 27 August 2018).
- Fichman, H.C.; Oliveira, R.M.; Fernandes, C.S. Neuropsychological and neurobiological markers of the preclinical stage of alzheimer’s disease. Psychol. Neurosci. 2011, 4, 245–253. [Google Scholar] [CrossRef]
- Kramer, A.F.; Colcombe, S. Fitness Effects on the Cognitive Function of Older Adults: A Meta-Analytic Study—Revisited. Perspect. Psychol. Sci. 2018, 13, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef] [PubMed]
- Anderson-Hanley, C.; Stark, J.; Wall, K.M.; Van Brakle, M.; Michel, M.; Maloney, M.; Barcelos, N.; Striegnitz, K.; Cohen, B.D.; Kramer, A.F. The interactive Physical and Cognitive Exercise System (iPACES™): Effects of a 3-month in-home pilot clinical trial for mild cognitive impairment and caregivers. Clin. Int. Aging 2018, in press. [Google Scholar]
- Colcombe, S.; Kramer, A. Fitness effects on the cognitive function of older adults: A meta-analytic study. Psychol. Sci. 2003, 14, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Rathore, A.; Lom, B. The effects of chronic and acute physical activity on working memory performance in healthy participants: A systematic review with meta-analysis of randomized controlled trials. Syst. Rev. 2017, 6, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Cui, M.Y.; Lin, Y.; Sheng, J.Y.; Zhang, X.; Cui, R.J. Exercise Intervention Associated with Cognitive Improvement in Alzheimer’s Disease. Neural Plast. 2018, 2018. [Google Scholar] [CrossRef] [PubMed]
- Mistridis, P.; Krumm, S.; Monsch, A.U.; Berres, M.; Taylor, K.I. The 12 years preceding mild cognitive impairment due to Alzheimer’s disease: The temporal emergence of cognitive decline. J. Alzheimer’s Dis. 2015, 48, 1095–1107. [Google Scholar] [CrossRef] [PubMed]
- Zheng, G.; Xia, R.; Zhou, W.; Tao, J.; Chen, L. Aerobic exercise ameliorates cognitive function in older adults with mild cognitive impairment: A systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 2016, 50, 1443–1450. [Google Scholar] [CrossRef] [PubMed]
- Song, D.; Yu, D.S.F.; Li, P.W.C.; Lei, Y. The effectiveness of physical exercise on cognitive and psychological outcomes in individuals with mild cognitive impairment: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2018, 79, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Hess, N.C.L.; Dieberg, G.; Mcfarlane, J.R.; Smart, N.A. The effect of exercise intervention on cognitive performance in persons at risk of, or with, dementia: A systematic review and meta-analysis. Health Aging Res. 2014, 3, 1–10. [Google Scholar] [CrossRef]
- Ludyga, S.; Gerber, M.; Brand, S.; Holsboer-Trachsler, E.; Pühse, U. Acute effects of moderate aerobic exercise on specific aspects of executive function in different age and fitness groups: A meta-analysis. Psychophysiology 2016, 53, 1611–1626. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.H.; Minzenberg, M.J.; Ursu, S.; Walter, R.; Wendelken, C.; Ragland, J.D.; Carter, C.S. Association of dorsolateral prefrontal cortex dysfunction with disrupted coordinated brain activity in schizophrenia: Relationship with impaired cognition, behavioral disorganization, and global function. Am. J. Psychiatry 2008, 165, 1006–1014. [Google Scholar] [CrossRef] [PubMed]
- Liang, J.-H.; Xu, Y.; Lin, L.; Jia, R.-X.; Zhang, H.-B.; Hang, L. Comparison of multiple interventions for older adults with Alzheimer disease or mild cognitive impairment: A PRISMA-compliant network meta-analysis. Medicine (Baltimore) 2018, 97, e10744. [Google Scholar] [CrossRef] [PubMed]
- Anderson-Hanley, C.; Arciero, P.J.; Brickman, A.M.; Nimon, J.P.; Okuma, N.; Westen, S.C.; Merz, M.E.; Pence, B.D.; Woods, J.A.; Kramer, A.F.; et al. Exergaming and older adult cognition: A cluster randomized clinical trial. Am. J. Prev. Med. 2012, 42, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Pope, Z.; Zeng, N.; Zhang, R.; Lee, H.Y.; Gao, Z. Effectiveness of Combined Smartwatch and Social Media Intervention on Breast Cancer Survivor Outcomes: Randomized Trial. Med. Sci. Sports Exer. 2018, 50, 137. [Google Scholar] [CrossRef]
- Van Praag, H.; Kempermann, G.; Gage, F.H. Neural consequences of environmental enrichment. Nat. Rev. Neurosci. 2000, 1, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Van Praag, H.; Shubert, T.; Zhao, C.; Gage, F. Exercise enhances learning and hippocampal neurogenesis in aged mice. J. Neurosci. 2005, 25, 8680–8685. [Google Scholar] [CrossRef] [PubMed]
- Van Praag, H. Neurogenesis and exercise: past and future directions. Neuromol. Med. 2008, 10, 128–140. [Google Scholar] [CrossRef] [PubMed]
- Suo, C.; Singh, M.F.; Gates, N.; Wen, W.; Sachdev, P.; Brodaty, H.; Baune, B.T. Therapeutically relevant structural and functional mechanisms triggered by physical and cognitive exercise. Mol. Psychiatry 2016, 21, 1633–1642. [Google Scholar] [CrossRef] [PubMed]
- Pappa, K.; Walsh, S.; Snyder, P. Immediate and delayed effects of cognitive interventions in healthy elderly: A review of current literature and future directions. Alzheimer’s Dement. 2009, 5, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Anguera, J.A.; Boccanfuso, J.; Rintoul, J.L.; Al-Hashimi, O.; Faraji, F.; Janowich, J.; Kong, E.; Larraburo, Y.; Rolle, C.; Johnston, E.; et al. Video game training enhances cognitive control in older adults. Nature 2013, 501, 97–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, K.Z.H.; Lindenberger, U.; Freund, A.M.; Baltes, P.B. WALKING WHILE MEMORIZING: Age-Related Differences in Compensatory Behavior. Psychol. Sci. 2001, 12, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Toril, P.; Reales, J.M.; Ballesteros, S. Video game training enhances cognition of older adults: A meta-analytic study. Psychol. Aging 2014, 29, 706. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Yu, J.; Wang, H.; Tan, C.; Meng, X.; Tan, L. Non-pharmacological interventions for patients with mild cognitive impairment: A meta-analysis of randomized controlled trials of cognition-based and exercise interventions. J. Alzheimer’s Dis. 2014, 42, 663–678. [Google Scholar] [CrossRef] [PubMed]
- Ballesteros, S.; Prieto, A.; Mayas, J.; Toril, P.; Pita, C.; Ponce de León, L.; Reales, J.M.; Waterworth, J. Brain training with non-action video games enhances aspects of cognition in older adults: A randomized controlled trial. Front. Aging Neurosci. 2014, 6, 277. [Google Scholar] [CrossRef] [PubMed]
- Corbett, A.; Owen, A.; Hampshire, A.; Grahn, J.; Stenton, R.; Dajani, S.; Burns, A.; Howard, R.; Williams, N.; Williams, G.; et al. The Effect of an Online Cognitive Training Package in Healthy Older Adults: An Online Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2015, 16, 990–997. [Google Scholar] [CrossRef] [PubMed]
- Mowszowski, L.; Lampit, A.; Walton, C.; Naismith, S. Strategy-Based Cognitive Training for Improving Executive Functions in Older Adults: A Systematic Review. Neuropsychol. Rev. 2016, 26, 252–270. [Google Scholar] [CrossRef] [PubMed]
- Bahar-Fuchs, A.; Clare, L.; Woods, B. Cognitive training and cognitive rehabilitation for persons with mild to moderate dementia of the Alzheimer’s or vascular type: A review. Alzheimer’s Res. Ther. 2013, 5, 35. [Google Scholar] [CrossRef] [PubMed]
- Karr, J.E.; Areshenkoff, C.N.; Rast, P.; Garcia-Barrera, M.A. An empirical comparison of the therapeutic benefits of physical exercise and cognitive training on the executive functions of older adults: A meta-analysis of controlled trials. Neuropsychology 2014, 28, 829. [Google Scholar] [CrossRef] [PubMed]
- Martin, M.; Clare, L.; Altgassen, A.M.; Cameron, M.H.; Zehnder, F. Cognition-based interventions for healthy older people and people with mild cognitive impairment. Cochrane Libr. 2011. [Google Scholar] [CrossRef] [PubMed]
- Simons, D.J.; Boot, W.R.; Charness, N.; Gathercole, S.E.; Chabris, C.F.; Hambrick, D.Z.; Stine-Morrow, E.A. Do “Brain Training” Programs Work? Psychol. Sci. Public Interest Suppl. 2016, 17, 103–186. [Google Scholar] [CrossRef] [PubMed]
- Reijnders, J.; van Heugten, C.; van Boxtel, M. Cognitive interventions in healthy older adults and people with mild cognitive impairment: A systematic review. Ageing Res. Rew. 2013, 12, 263–275. [Google Scholar] [CrossRef] [PubMed]
- Zokaei, N.; MacKellar, C.; Čepukaitytė, G.; Patai, E.Z.; Nobre, A.C. Cognitive training in the elderly: Bottlenecks and new avenues. J. Cogn. Neurosci. 2017, 29, 1473–1482. [Google Scholar] [CrossRef] [PubMed]
- AAN Summary of Practice Guidelines for Clinicians, Practice Guideline Update: Mild Cognitive Impairment. Available online: https://www.aan.com/Guidelines/Home/GetGuidelineContent/882 (accessed on 1 July 2018).
- Eshkoor, S.A.; Hamid, T.A.; Mun, C.Y.; Ng, C.K. Mild cognitive impairment and its management in older people. Clin. Int. Aging 2015, 10, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Nagamatsu, L.S.; Flicker, L.; Kramer, A.F.; Voss, M.W.; Erickson, K.I.; Hsu, C.L.; Liu-Ambrose, T. Exercise is medicine, for the body and the brain. Br. J. Sports Med. 2014, 943–944. [Google Scholar] [CrossRef] [PubMed]
- Studenski, S.; Carlson, M.C.; Fillit, H.; Greenough, W.T.; Kramer, A.; Rebok, G.W. From bedside to bench: does mental and physical activity promote cognitive vitality in late life? Sci. SAGE KE 2006, 2006, pe21. [Google Scholar] [CrossRef] [PubMed]
- Foster, P.P.; Rosenblatt, K.P.; Kuljiš, R.O. Exercise-induced cognitive plasticity, implications for mild cognitive impairment and Alzheimer’s disease. Front. Neurol. 2011, 2, 28. [Google Scholar] [CrossRef] [PubMed]
- Gheysen, F.; Poppe, L.; DeSmet, A.; Swinnen, S.; Cardon, G.; De Bourdeaudhuij, I.; Chastin, S.; Fias, W. Physical activity to improve cognition in older adults: Can physical activity programs enriched with cognitive challenges enhance the effects? A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 63. [Google Scholar] [CrossRef] [PubMed]
- Constans, A.; Pin-barre, C.; Temprado, J.J.; Decherchi, P.; Laurin, J. Influence of aerobic training and combinations of interventions on cognition and neuroplasticity after stroke. Front. Aging Neurosci. 2016, 8, 164. [Google Scholar] [CrossRef] [PubMed]
- Diamond, A. Effects of Physical Exercise on Executive Functions: Going beyond Simply Moving to Moving with Thought. Ann. Sport Med. Res. 2015, 2, 1011. [Google Scholar]
- Zhu, X.; Yin, S.; Lang, M.; He, R.; Li, J. The more the better? A meta-analysis on effects of combined cognitive and physical intervention on cognition in healthy older adults. Ageing Res. Rev. 2016, 31, 67–79. [Google Scholar] [CrossRef] [PubMed]
- Geda, Y.E.; Silber, T.C.; Roberts, R.O.; Knopman, D.S.; Christianson, T.J.; Pankratz, V.S.; Boeve, B.F.; Tangalos, E.G.; Petersen, R.C. Computer activities, physical exercise, aging, and mild cognitive impairment: A population-based study. Mayo Clin. Proc. 2012, 87, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Shah, T.; Verdile, G.; Sohrabi, H.; Campbell, A.; Putland, E.; Cheetham, C.; Dhaliwal, S.; Weinborn, M.; Maruff, P.; Darby, D.; et al. A combination of physical activity and computerized brain training improves verbal memory and increases cerebral glucose metabolism in the elderly. Transl. Psychiatry 2014, 4, e487. [Google Scholar] [CrossRef] [PubMed]
- Karssemeijer, E.E.; Aaronson, J.J.; Bossers, W.W.; Smits, T.T.; Rikkert, M.M.; Kessels, R.R. Positive effects of combined cognitive and physical exercise training on cognitive function in older adults with mild cognitive impairment or dementia: A meta-analysis. Ageing Res. Rev. 2017. [Google Scholar] [CrossRef] [PubMed]
- Styliadis, C.; Kartsidis, P.; Paraskevopoulos, E.; Ioannides, A.A.; Bamidis, P.D. Neuroplastic effects of combined computerized physical and cognitive training in elderly individuals at risk for dementia: An eLORETA controlled study on resting states. Neural Plast. 2015, 2015. [Google Scholar] [CrossRef] [PubMed]
- Edwards, M.K.; Loprinzi, P.D. Experimental Effects of Acute Exercise and Meditation on Parameters of Cognitive Function. J. Clin. Med. 2018, 7, 125. [Google Scholar] [CrossRef] [PubMed]
- Anderson-Hanley, C.; Barcelos, N.M.; Zimmerman, E.A.; Gillen, R.W.; Dunnam, M.; Cohen, B.D.; Yerokhin, V.; Miller, K.E.; Hayes, D.J.; Arciero, P.J.; et al. The Aerobic and Cognitive Exercise Study (ACES) for community-dwelling older adults with or at-risk for mild cognitive impairment (MCI): Neuropsychological, neurobiological and neuroimaging outcomes of a randomized clinical trial. Front. Aging Neurosci. 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Anderson-Hanley, C.; Maloney, M.; Barcelos, N.; Striegnitz, K.; Kramer, A. Neuropsychological Benefits of Neuro-Exergaming for Older Adults: A Pilot Study of an Interactive Physical and Cognitive Exercise System (iPACES). J. Aging Phys. Act. 2017, 25, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Bamidis, P.D.; Vivas, A.B.; Styliadis, C.; Frantzidis, C.; Klados, M.; Schlee, W.; Siountasa, A.; Papageorgioud, S.G. A review of physical and cognitive interventions in aging. Neurosci. Biobehav. Rev. 2014, 44, 206–220. [Google Scholar] [CrossRef] [PubMed]
- Van Het Reve, E.; De Bruin, E.D. Strength-balance supplemented with computerized cognitive training to improve dual task gait and divided attention in older adults: A multicenter randomized-controlled trial. BMC Geriatr. 2014, 14, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, S.; Schumacher, V. The interplay between cognitive and motor functioning in healthy older adults: Findings from dual-task studies and suggestions for intervention. Gerontology 2011, 57, 239–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Law, L.L.; Barnett, F.; Yau, M.K.; Gray, M.A. Effects of combined cognitive and exercise interventions on cognition in older adults with and without cognitive impairment: A systematic review. Ageing Res. Rev. 2014, 15, 61–75. [Google Scholar] [CrossRef] [PubMed]
- Lauenroth, A.; Ioannidis, A.; Teichmann, B. Influence of combined physical and cognitive training on cognition: A systematic review. BMC Geriatr. 2016, 16, 141. [Google Scholar] [CrossRef] [PubMed]
- Noack, H.; Lövdén, M.; Schmiedek, F. On the validity and generality of transfer effects in cognitive training research. Psychol. Res. 2014, 78, 773–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ratner, E.; Atkinson, D. Why cognitive training and brain games will not prevent or forestall dementia. J. Am. Geriatr. Soc. 2015, 63, 2612–2614. [Google Scholar] [CrossRef] [PubMed]
- Maffei, L.; Picano, E.; Andreassi, M.G.; Angelucci, A.; Baldacci, F.; Baroncelli, L.; Begenisic, T.; Bellinvia, P.F.; Berardi, N.; Biagi, L.; et al. Randomized trial on the effects of a combined physical/cognitive training in aged MCI subjects: The Train the Brain study. Sci. Rep. 2017, 7, 39471. [Google Scholar]
- Voss, M.W.; Weng, T.B.; Burzynska, A.Z.; Wong, C.N.; Cooke, G.E.; Clark, R.; Fanning, J.; Awick, E.; Gothe, N.P.; Olson, E.A.; et al. Fitness, but not physical activity, is related to functional integrity of brain networks associated with aging. Neuroimage 2016, 131, 113–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fabre, C.; Chamari, K.; Mucci, P. Improvement of Cognitive Function by Mental and / or Individualized Aerobic Training in Healthy Elderly Subjects. Int. J. Sports Med. 2002, 33, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Oswald, W.D.; Gunzelmann, T.; Rupprecht, R.; Hagen, B. Differential effects of single versus combined cognitive and physical training with older adults: The SimA study in a 5-year perspective. Eur. J. Ageing 2006, 3, 179–192. [Google Scholar] [CrossRef] [PubMed]
- Shatil, E. Does combined cognitive training and physical activity training enhance cognitive abilities more than either alone? A four-condition randomized controlled trial among healthy older adults. Front. Aging Neurosci. 2013, 5, 8. [Google Scholar] [CrossRef] [PubMed]
- Linde, K.; Alfermann, D. Single versus combined cognitive and physical activity effects on fluid cognitive abilities of healthy older adults: A 4-month randomized controlled trial with follow-up. J. Aging Phys. Act. 2014, 22, 302–313. [Google Scholar] [CrossRef] [PubMed]
- Rahe, J.; Petrelli, A.; Kaesberg, S.; Fink, G.R.; Kessler, J.; Kalbe, E. Effects of cognitive training with additional physical activity compared to pure cognitive training in healthy older adults. Clin. Int. Aging 2015, 10, 297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desjardins-Crépeau, L.; Berryman, N.; Fraser, S.A.; Vu, T.T.M.; Kergoat, M.J.; Li, K.Z.; Bosquet, L.; Bherer, L. Effects of combined physical and cognitive training on fitness and neuropsychological outcomes in healthy older adults. Clin. Interv. Aging 2016, 11, 1287–1299. [Google Scholar] [CrossRef] [PubMed]
- Rahe, J.; Becker, J.; Fink, G.R.; Kessler, J.; Kukolja, J.; Rahn, A.; Rosen, J.B.; Szabados, F.; Wirth, B.; Kalbe, E. Cognitive training with and without additional physical activity in healthy older adults: cognitive effects, neurobiological mechanisms, and prediction of training success. Front. Aging Neurosci. 2015, 7, 187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruderer-Hofstetter, M.; Rausch-Osthoff, A.K.; Meichtry, A.; Münzer, T.; Niedermann, K. Effective multicomponent interventions in comparison to active control and no interventions on physical capacity, cognitive function and instrumental activities of daily living in elderly people with and without mild impaired cognition: A systematic review and network meta-analysis. Ageing Res. Rev. 2018, 45, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Ballesteros, S.; Voelcker-Rehage, C.; Bherer, L. Editorial: Cognitive and Brain Plasticity Induced by Physical Exercise, Cognitive Training, Video Games, and Combined Interventions. Front. Hum. Neurosci. 2018, 12, 169. [Google Scholar] [CrossRef] [PubMed]
- Hiyamizu, M.; Morioka, S.; Shomoto, K.; Shimada, T. Effects of dual task balancetraining on dual task performance in elderly people: A randomized controlled trial. Clin. Rehabil. 2012, 26, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Theill, N.; Schumacher, V.; Adelsberger, R.; Martin, M.; Jäncke, L. Effects of simultaneously performed cognitive and physical training in older adults. BMC Neurosci. 2013, 14, 103. [Google Scholar] [CrossRef] [PubMed]
- Kayama, H.; Okamoto, K.; Nishiguchi, S.; Yamada, M.; Kuroda, T.; Aoyama, T. Effect of a Kinect-based exercise game on improving executive cognitive performance in community-dwelling elderly: Case control study. J. Med. Internet Res. 2014, 16, e61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barcelos, N.; Shah, N.; Cohen, K.; Hogan, M.J.; Mulkerrin, E.; Arciero, P.J.; Cohen, B.D.; Kramer, A.F.; Anderson-Hanley, C. Aerobic and cognitive exercise (ACE) pilot study for older adults: Executive function improves with cognitive challenge while exergaming. J. Int. Neuropsychol. Soc. 2015, 21, 768–779. [Google Scholar] [CrossRef] [PubMed]
- Nishiguchi, S.; Yamada, M.; Tanigawa, T.; Sekiyama, K.; Kawagoe, T.; Suzuki, M.; Yoshikawa, S.; Abe, N.; Otsuka, Y.; Nakai, R.; et al. A 12-Week Physical and Cognitive Exercise Program Can Improve Cognitive Function and Neural Efficiency in Community-Dwelling Older Adults: A Randomized Controlled Trial. J. Am. Geriatr. Soc. 2015, 63, 1355–1363. [Google Scholar] [CrossRef] [PubMed]
- Leon, J.; Urena, A.; Bolanos, M.J.; Bilbao, A.; Ona, A. A combination of physical and cognitive exercise improves reaction time in persons 61–84 years old. J. Aging Phys. Activ. 2015, 23, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, H.; Okazaki, K.; Imai, D.; Yamashina, Y.; Takeda, R.; Naghavi, N.; Ota, A.; Hirasawa, Y.; Miyagawa, T. The effect of cognitive-motor dual-task training on cognitive function and plasma amyloid β peptide 42/40 ratio in healthy elderly persons: a randomized controlled trial. BMC Geriatr. 2015, 15, 60. [Google Scholar] [CrossRef] [PubMed]
- Mura, G.; Carta, M.G.; Sancassiani, F.; Machado, S.; Prosperini, L. Active exergames to improve cognitive functioning in neurological disabilities: A systematic review and meta-analysis. Eur. J. Phys. Rehabil. Med. 2017. [Google Scholar] [CrossRef]
- Stanmore, E.S.; Brendon, V.D.; de Bruin, E.D.; Firth, J. The effect of active video games on cognitive functioning in clinical and non-clinical populations: A meta-analysis of randomized controlled trials. Neurosci. Biobehav. Rev. 2017, 78, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Timmerman, C.E. Effects of Supportive Feedback Messages on Exergame Experiences. Mass Commun. Soc. 2018, 30, 29–40. [Google Scholar] [CrossRef]
- Sonntag, W.E.; Ramsey, M.; Carter, C.S. Growth hormone and insulin-like growth factor-1 (IGF-1) and their influence on cognitive aging. Ageing Res. Rev. 2005, 4, 195–212. [Google Scholar] [CrossRef] [PubMed]
- Dik, M.G.; Pluijm, S.M.F.; Jonker, C.; Deeg, D.J.H.; Lomecky, M.Z.; Lips, P. Erratum: Insulin-like growth factor I (IGF-I) and cognitive decline in older persons Neurobiol. Aging 2004, 25, 271. [Google Scholar] [CrossRef]
- Al-Delaimy, W.K.; Von Muhlen, D.; Barrett-Connor, E. Insulinlike growth factor-1, insulinlike growth factor binding protein-1, and cognitive function in older men and women. J. Am. Geriatr. Soc. 2009, 57, 1441–1446. [Google Scholar] [CrossRef] [PubMed]
- Vega, S.R.; Knicker, A.; Hollmann, W.; Bloch, W.; Strüder, H.K. Effect of resistance exercise on serum levels of growth factors in humans. Horm. Metab. Res. 2010, 42, 982–986. [Google Scholar] [CrossRef] [PubMed]
- Bellar, D.; Glickman, E.L.; Juvancic-Heltzel, J.; Gunstad, J. Serum insulin like growth factor-1 is associated with working memory, executive function and selective attention in a sample of healthy, fit older adults. Neuroscience 2011, 178, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Voss, M.W.; Prakash, R.S.; Erickson, K.I.; Basak, C.; Chaddock, L.; Kim, J.S.; Alves, H.; Heo, S.; Szabo, A.N.; White, S.M.; et al. Plasticity of brain networks in a randomized intervention trial of exercise training in older adults. Front. Aging Neurosci. 2010, 2. [Google Scholar] [CrossRef] [PubMed]
- Ray, L.; Khemka, V.K.; Behera, P.; Bandyopadhyay, K.; Pal, S.; Pal, K.; Basu, D.; Chakrabarti, S. Serum homocysteine, dehydroepiandrosterone sulphate and lipoprotein (a) in Alzheimer’s disease and vascular dementia. Aging Dis. 2013, 4, 57. [Google Scholar] [PubMed]
- Maggio, M.; De Vita, F.; Fisichella, A.; Colizzi, E.; Provenzano, S.; Lauretani, F.; Valenti, G. DHEA and cognitive function in the elderly. J. Steriod. Biochem. Mol. Biol. 2015, 145, 281–292. [Google Scholar] [CrossRef] [PubMed]
- Davis, S.R.; Shah, S.M.; McKenzie, D.P.; Kulkarni, J.; Davison, S.L.; Bell, R.J. Dehydroepiandrosterone sulfate levels are associated with more favorable cognitive function in women. J. Clin. Endocrinol. Metab. 2008, 93, 801–808. [Google Scholar] [CrossRef] [PubMed]
- Lupien, S.; Nair, N.; Briére, S.; Maheu, F.; Tu, M.; Lemay, Μ.; Meaney, M. Increased cortisol levels and impaired cognition in human aging: Implication for depression and dementia in later life. Rev. Neurosci. 1999, 10, 117–140. [Google Scholar] [CrossRef] [PubMed]
- Lupien, S.J.; Leon, M.D.; Santi, S.D.; Convit, A.; Tarshish, C.; Nair, N.P.; Meaney, M.J. Cortisol, human aging, hippocampal atrophy, and memory deficits. Neuroscientist 1998, 4, 389–390. [Google Scholar]
- Csernansky, J.G.; Dong, H.; Fagan, A.M.; Wang, L.; Xiong, C.; Holtzman, D.M.; Morris, J.C. Plasma cortisol and progression of dementia in subjects with Alzheimer-type dementia. Am. J. Psychiatry 2006, 163, 2164–2169. [Google Scholar] [CrossRef] [PubMed]
- Lara, J.; Cooper, R.; Nissan, J.; Ginty, A.T.; Khaw, K.T.; Deary, I.J.; Lord, J.M.; Kuh, D.; Mathers, J.C. A proposed panel of biomarkers of healthy ageing. BMC Med. 2015, 13, 222. [Google Scholar] [CrossRef] [PubMed]
- Lara, V.P.; Caramelli, P.; Teixeira, A.L.; Barbosa, M.T.; Carmona, K.C.; Carvalho, M.G.; Fernandes, A.P.; Gomes, K.B. High cortisol levels are associated with cognitive impairment no-dementia (CIND) and dementia. Clin. Chim. Acta 2013, 423, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Tortosa-Martínez, J.; Clow, A.; Caus-Pertegaz, N.; González-Caballero, G.; Abellán-Miralles, I.; Saenz, M.J. Exercise increases the dynamics of diurnal cortisol secretion and executive function in people with amnestic mild cognitive impairment. J. Aging Phys. Act. 2015, 23, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Beglinger, L.J.; Gaydos, B.; Tangphao-Daniels, O.; Duff, K.; Kareken, D.A.; Crawford, J.; Fastenau, P.S.; Siemers, E.R. Practice effects and the use of alternate forms in serial neuropsychological testing. Arch. Clin. Neuropsychol. 2005, 20, 517–529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veterans Health Administration Handbook 2007. Available online: https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=2966 (accessed on 1 July 2018).
- Eggenberger, P.; Wolf, M.; Schumann, M.; de Bruin, E. Exergame and Balance Training Modulate Prefrontal Brain Activity during Walking and Enhance Executive Function in Older Adults. Front. Aging Neurosci. 2016, 8, 66. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, E.; You, T.; Leveille, S. Potential benefits of exergaming for cognition and dual-task function in older adults: A systematic review. J. Aging Phys. Act. 2016, 24, 332–336. [Google Scholar] [CrossRef] [PubMed]
- Strauss, E.; Sherman, E.M.; Spreen, O. A compendium of Neuropsychological Tests: Administration, Norms, and Commentary; Oxford University Press: New York, NY, USA, 2006. [Google Scholar]
- Lee, K.; Baniqued, P.; Cosman, J.; Mullen, S.; McAuley, E.; Severson, J.; Kramer, A.F. Examining cognitive function across the lifespan using a mobile application. Comput. Hum. Behav. 2012, 28, 1934–1946. [Google Scholar] [CrossRef]
- Lesh, T.A.; Westphal, A.J.; Niendam, T.A.; Yoon, J.H.; Minzenberg, M.J.; Ragland, J.D.; Carter, C.S. Proactive and reactive cognitive control and dorsolateral prefrontal cortex dysfunction in first episode schizophrenia. NeuroImage Clin. 2013, 2, 590–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Elst, W.; Van Boxtel, M.; Van Breukelen, G.; Jolles, J. The Stroop color-word test: influence of age, sex, and education; and normative data for a large sample across the adult age range. Assessment 2006, 13, 62–79. [Google Scholar] [CrossRef] [PubMed]
- Scarpina, F.; Tagini, S. The stroop color and word test. Front. Psychol. 2017, 8, 557. [Google Scholar] [CrossRef] [PubMed]
- Wecker, N.S.; Kramer, J.H.; Wisniewski, A.; Delis, D.C.; Kaplan, E. Age effects on executive ability. Neuropsychology 2000, 14, 409. [Google Scholar] [CrossRef] [PubMed]
- D’Elia, L.G.; Satz, P.; Uchiyama, C.L.; White, T. Color Trails Test (CTT); Psychological Assessment Resources: Odessa, FL, USA, 1996. [Google Scholar]
- Harrison, J. Measuring cognitive change in Alzheimer’s disease clinical drug trials. J. Nutr. Health Aging 2007, 11, 327–329. [Google Scholar] [PubMed]
- Podhorna, J.; Krahnke, T.; Shear, M.; Harrison, J.E. Alzheimer’s Disease Assessment Scale-Cognitive subscale variants in mild cognitive impairment and mild Alzheimer’s disease: Change over time and the effect of enrichment strategies. Alzheimer’s Res. Ther. 2016, 8, 8. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Schillaci, A. Neuropsychological Effects of the Interactive Physical and Cognitive Exercise System (iPACES™) for Older Adults: Executive Function and Mood. Bachelor’s Thesis, Union College, Schenectady, NY, USA, June 2017. [Google Scholar]
- Gray, W.D. Plateaus and asymptotes: Spurious and real limits in human performance. Curr. Dir. Psychol. Sci. 2017, 26, 59–67. [Google Scholar] [CrossRef]
- Guazzo, E.P.; Kirkpatrick, P.J.; Goodyer, I.M.; Shiers, H.M.; Herbert, J. Cortisol, dehydroepiandrosterone (DHEA), and DHEA sulfate in the cerebrospinal fluid of man: relation to blood levels and the effects of age. J. Clin. Endocrinol. Metabol. 1996, 81, 3951–3960. [Google Scholar] [CrossRef]
- Mura, G.; Cossu, G.; Migliaccio, G.M.; Atzori, C.; Nardi, A.E.; Machado, S.; Carta, M.G. Quality of life, cortisol blood levels and exercise in older adults: Results of a randomized controlled trial. Clin. Pract. Epidemiol. Ment. Health 2014, 10, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Chew, J.; Chong, M.S.; Fong, Y.L.; Tay, L. Outcomes of a multimodal cognitive and physical rehabilitation program for persons with mild dementia and their caregivers: A goal-oriented approach. Clin. Int. Aging 2015, 10, 1687. [Google Scholar] [CrossRef] [PubMed]
- Chuang, L.Y.; Hung, H.Y.; Huang, C.J.; Chang, Y.K.; Hung, T.M. A 3-month intervention of Dance Dance Revolution improves interference control in elderly females: A preliminary investigation. Exp. Brain Res. 2015, 233, 1181–1188. [Google Scholar] [CrossRef] [PubMed]
- Dunkin, J.; Anderson-Hanley, C. Dementia caregiver burden: A review of the literature and guidelines for assessment and intervention. Neurology 1998, 51, S53–S60. [Google Scholar] [CrossRef] [PubMed]
- Loprinzi, P.D.; Frith, E. The Role of Sex in Memory Function: Considerations and Recommendations in the Context of Exercise. J. Clin. Med. 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- Barha, C.; Davis, J.; Falck, R.; Nagamatsu, L.; Liu-Ambrose, T. Sex differences in exercise efficacy to improve cognition: A systematic review and meta-analysis of randomized controlled trials in older humans. Front. Neuroendocr. 2017, 46, 71–85. [Google Scholar] [CrossRef] [PubMed]
- Osho, O.; Owoeye, O.; Armijo-Olivo, S. Adherence and Attrition in Fall Prevention Exercise Programs for Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis. J. Aging Phys. Act. 2018, 26, 304–326. [Google Scholar] [CrossRef] [PubMed]
- Köbe, T.; Witte, A.V.; Schnelle, A.; Lesemann, A.; Fabian, S.; Tesky, V.A.; Pantel, J.; Flöel, A. Combined omega-3 fatty acids, aerobic exercise and cognitive stimulation prevents decline in gray matter volume of the frontal, parietal and cingulate cortex in patients with mild cognitive impairment. Neuroimage 2016, 131, 226–238. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Soobiah, C.; Berliner, S.; Ho, J.M.; Ng, C.H.; Ashoor, H.M.; Chen, M.H.; Hemmelgarn, B.; Straus, S.E. Efficacy and safety of cognitive enhancers for patients with mild cognitive impairment: A systematic review and meta-analysis. Can. Med. Assoc. J. 2013, 185, 1393–1401. [Google Scholar] [CrossRef] [PubMed]
- Kosmat, H.; Vranic, A. The efficacy of a dance intervention as cognitive training for the old-old. J. Aging Phys. Act. 2017, 25, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Merom, D.; Grunseit, A.; Eramudugolla, R.; Jefferis, B.; Mcneill, J.; Anstey, K.J. Cognitive benefits of social dancing and walking in old age: The dancing mind randomized controlled trial. Front. Aging Neurosci. 2016, 8, 26. [Google Scholar] [CrossRef] [PubMed]
- Burzynska, A.Z.; Jiao, Y.; Knecht, A.M.; Fanning, J.; Awick, E.A.; Chen, T.; Gothe, N.; Voss, M.W.; McAuley, E.; Kramer, A.F. White matter integrity declined over 6-months, but dance intervention improved integrity of the fornix of older adults. Front. Aging Neurosci. 2017, 9, 59. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.; Rudolph, E.; Anderson-Hanley, C. Aerobic and cognitive exercise over time: Virtual versus outdoor cycling. Presented at the annual meeting of the Society of Behavioral Medicine, Philadelphia, PA. Ann. Behav. Med. 2013, 47, S282. [Google Scholar]
- Nelson, L.; Tabet, N. Slowing the progression of Alzheimer’s disease; what works? Ageing Res. Rev. 2015, 23, 193–209. [Google Scholar] [CrossRef] [PubMed]
- Wayne, P.M.; Walsh, J.N.; Taylor-Piliae, R.E.; Wells, R.E.; Papp, K.V.; Donovan, N.J.; Yeh, G.Y. Effect of Tai Chi on cognitive performance in older adults: Systematic review and meta-Analysis. J. Am. Geriatr. Soc. 2014, 62, 25–39. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Shimada, H.; Makizako, H.; Doi, T.; Yoshida, D.; Ito, K.; Shimokata, H.; Washimi, Y.; Endo, H.; Kato, T. A randomized controlled trial of multicomponent exercise in older adults with mild cognitive impairment. PLoS One 2013, 8, e61483. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.E. Healthy cognitive aging and dementia prevention. Am. Psychol. 2016, 71, 268. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, J. Adam Gazzaley, MD, PhD: Developing Prescribable Video Games. JAMA 2018, 320, 16–18. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 0 | 2w | 4w | 6w | 8w | 3M | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| baseline (n = 14) | placebo (n = 12) | pedaler (n = 11) | game (n = 11) | iPACES (n = 11, 7) | |||||||||
| ave | SD | ave | SD | ave | SD | ave | SD | ave | SD | ave | SD | ||
| Stroop | Incongruent % correct | 0.61 | 0.31 | 0.77 | 0.33 | 0.78 | 0.28 | 0.86 | 0.13 | 0.79 | 0.24 | 0.93 | 0.05 |
| Congruent % correct | 0.88 | 0.13 | 0.94 | 0.10 | 0.97 | 0.06 | 0.94 | 0.07 | 0.96 | 0.05 | 0.98 | 0.03 | |
| Incongruent ave time (s) | 1.45 | 0.22 | 1.38 | 0.17 | 1.42 | 0.22 | 1.41 | 0.21 | 1.35 | 0.16 | 1.33 | 0.16 | |
| Congruent ave time (s) | 1.37 | 0.18 | 1.22 | 0.25 | 1.13 | 0.14 | 1.22 | 0.17 | 1.23 | 0.19 | 1.10 | 0.07 | |
| Total duration (s) | 269.0 | 104.3 | 186.8 | 63.7 | 149.9 | 68.3 | 107.3 | 54.9 | 100.6 | 44.6 | 70.7 | 5.7 | |
| CCII | 0.48 | 0.41 | 0.71 | 0.39 | 0.75 | 0.33 | 0.80 | 0.16 | 0.75 | 0.28 | 0.91 | 0.07 | |
| Trails | restarts | 4.77 | 6.56 | 2.00 | 1.95 | 1.64 | 2.25 | 1.36 | 1.12 | 0.73 | 1.19 | 1.43 | 1.90 |
| A % error | 0.42 | 0.58 | 0.20 | 0.24 | 0.15 | 0.23 | 0.11 | 0.09 | 0.06 | 0.09 | 0.13 | 0.16 | |
| B % error | 0.29 | 0.27 | 0.18 | 0.17 | 0.16 | 0.16 | 0.10 | 0.10 | 0.10 | 0.09 | 0.28 | 0.15 | |
| B duration (s) | 212.6 | 175.5 | 160.9 | 151.6 | 145.8 | 81.1 | 124.5 | 69.2 | 125.0 | 81.0 | 163.1 | 55.4 | |
| CCII | 0.28 | 0.73 | 0.64 | 0.31 | 0.69 | 0.30 | 0.79 | 0.16 | 0.84 | 0.15 | 0.59 | 0.28 | |
| Flanker | Incongruent % correct | 0.81 | 0.25 | 0.91 | 0.14 | 0.90 | 0.17 | 0.93 | 0.07 | 0.92 | 0.12 | 0.76 | 0.36 |
| Congruent % correct | 0.91 | 0.10 | 0.89 | 0.14 | 0.97 | 0.03 | 0.95 | 0.08 | 0.95 | 0.08 | 0.98 | 0.02 | |
| Incongruent ave time (s) | 0.78 | 0.21 | 0.65 | 0.08 | 0.71 | 0.12 | 0.66 | 0.12 | 0.64 | 0.06 | 0.77 | 0.22 | |
| Congruent ave time (s) | 0.74 | 0.25 | 0.63 | 0.08 | 0.64 | 0.07 | 0.61 | 0.12 | 0.61 | 0.07 | 0.67 | 0.12 | |
| Total duration (s) | 244.9 | 47.7 | 207.9 | 94.2 | 152.7 | 63.4 | 97.8 | 64.5 | 97.4 | 57.9 | 71.9 | 16.7 | |
| CCII | 0.72 | 0.28 | 0.79 | 0.27 | 0.87 | 0.19 | 0.87 | 0.13 | 0.87 | 0.20 | 0.74 | 0.36 | |
| ADAS | Word List (sum trials correct) | 18.64 | 4.58 | 19.29 | 5.68 | 20.33 | 4.33 | 19.92 | 3.96 | 21.00 | 4.63 | 21.13 | 4.67 |
| Word List (delay correct) | 5.08 | 2.66 | 5.85 | 2.44 | 5.58 | 2.23 | 6.42 | 2.02 | 5.75 | 2.83 | 5.63 | 2.13 | |
| Biomarkers | cortisol | 3.55 | 3.36 | 5.08 | 5.37 | 5.52 | 5.23 | 2.58 | 3.38 | 3.06 | 4.00 | 17.61 | 7.17 |
| DHEA-S | 8733 | 5923 | 7729 | 8620 | 7301 | 9153 | 6508 | 6085 | 4999 | 3547 | 6072 | 6503 | |
| IGF-1 | 3.16 | 2.73 | 3.43 | 3.66 | 1.82 | 1.01 | 2.64 | 1.91 | 1.83 | 1.37 | 2.56 | 2.46 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wall, K.; Stark, J.; Schillaci, A.; Saulnier, E.T.; McLaren, E.; Striegnitz, K.; Cohen, B.D.; Arciero, P.J.; Kramer, A.F.; Anderson-Hanley, C. The Enhanced Interactive Physical and Cognitive Exercise System (iPACESTM v2.0): Pilot Clinical Trial of an In-Home iPad-Based Neuro-Exergame for Mild Cognitive Impairment (MCI). J. Clin. Med. 2018, 7, 249. https://doi.org/10.3390/jcm7090249
Wall K, Stark J, Schillaci A, Saulnier ET, McLaren E, Striegnitz K, Cohen BD, Arciero PJ, Kramer AF, Anderson-Hanley C. The Enhanced Interactive Physical and Cognitive Exercise System (iPACESTM v2.0): Pilot Clinical Trial of an In-Home iPad-Based Neuro-Exergame for Mild Cognitive Impairment (MCI). Journal of Clinical Medicine. 2018; 7(9):249. https://doi.org/10.3390/jcm7090249
Chicago/Turabian StyleWall, Kathryn, Jessica Stark, Alexa Schillaci, Emilie T. Saulnier, Elizabeth McLaren, Kristina Striegnitz, Brian D. Cohen, Paul J. Arciero, Arthur F. Kramer, and Cay Anderson-Hanley. 2018. "The Enhanced Interactive Physical and Cognitive Exercise System (iPACESTM v2.0): Pilot Clinical Trial of an In-Home iPad-Based Neuro-Exergame for Mild Cognitive Impairment (MCI)" Journal of Clinical Medicine 7, no. 9: 249. https://doi.org/10.3390/jcm7090249