Seroepidemiology of Measles, Mumps and Rubella on Bonaire, St. Eustatius and Saba: The First Population-Based Serosurveillance Study in Caribbean Netherlands

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Study Population
2.2. Laboratory Analyses
2.3. Data Analyses
2.3.1. Seroprevalence and GMC
2.3.2. Waning Immunity after MMR Vaccination
2.3.3. Risk Factors for Seronegativity
3. Results
3.1. Study Characteristics
3.2. Age-Specific Seroprevalence and GMC
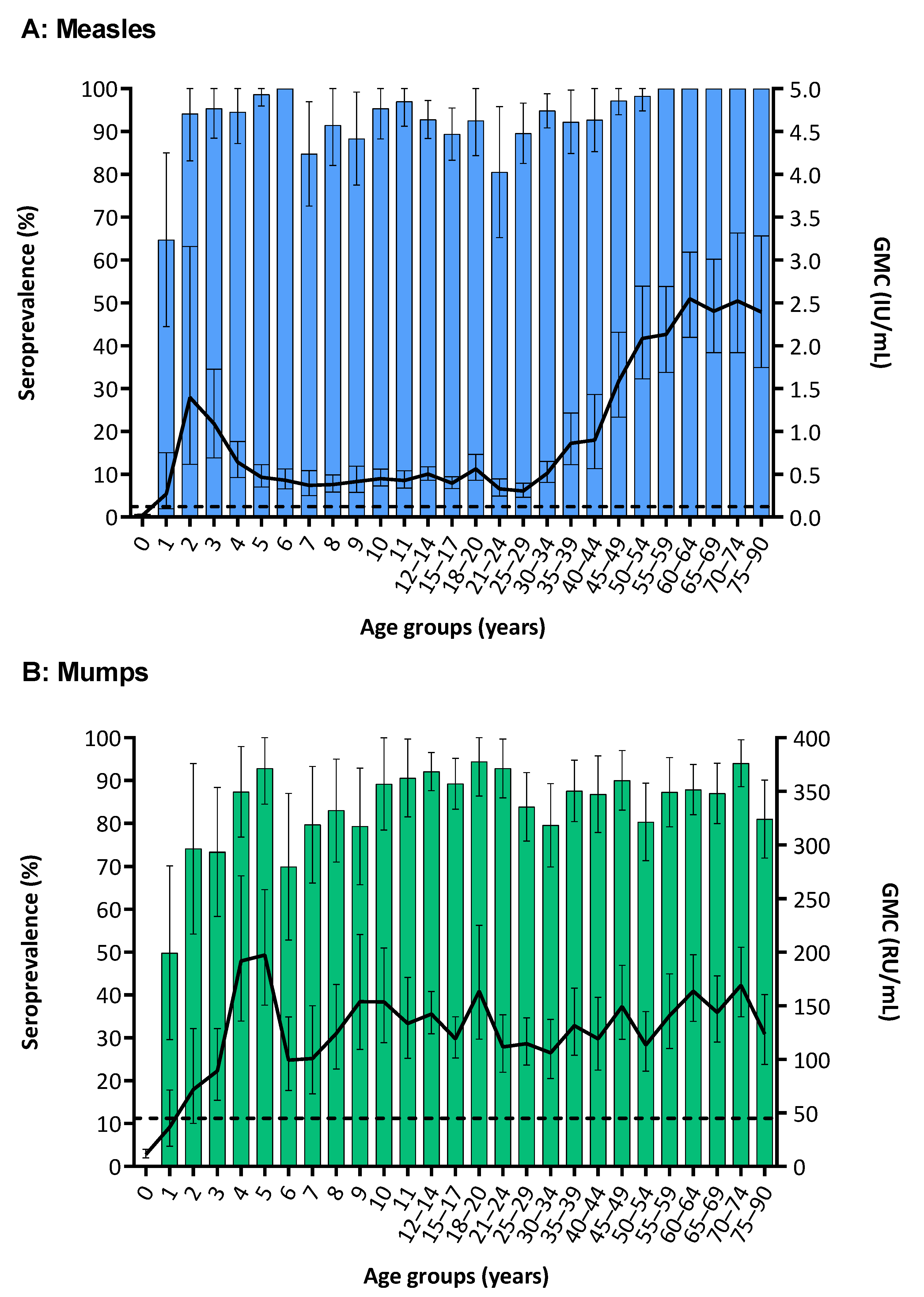
3.2.1. Measles
3.2.2. Mumps
3.2.3. Rubella
3.3. Waning Immunity after MMR Vaccination
3.4. Risk Factors for Seronegativity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- McLean, H.Q.; Fiebelkorn, A.P.; Temte, J.L.; Wallace, G.S. Prevention of measles, rubella, congenital rubella syndrome, and mumps, 2013: Summary recommendations of the Advisory Committee on Immunization Practices (ACIP). Mmwr. Recomm. Rep. Morb. Mortal. Wkly. Rep. Recomm. Rep. 2013, 62, 1–34. [Google Scholar]
- The Lancet. Measles eradication: A goal within reach, slipping away. Lancet 2019, 393, 1669. [Google Scholar] [CrossRef]
- Pan American Health Organization; World Health Organization. Epidemiological Update: Measles. 18 June 2019; PAHO/WHO: Washington, DC, USA, 2019. [Google Scholar]
- Paniz-Mondolfi, A.E.; Tami, A.; Grillet, M.E.; Marquez, M.; Hernandez-Villena, J.; Escalona-Rodriguez, M.A.; Blohm, G.M.; Mejias, I.; Urbina-Medina, H.; Risquez, A.; et al. Resurgence of Vaccine-Preventable Diseases in Venezuela as a Regional Public Health Threat in the Americas. Emerg. Infect. Dis. 2019, 25, 625. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Public Health and the Environment (RIVM). Vaccination Schedule Bonaire, Saba and St. Eustatius [in Dutch: Vaccinatieschema Bonaire, Saba en St. Eustatius]. Available online: https://rijksvaccinatieprogramma.nl/vaccinaties/vaccinatieschema (accessed on 5 June 2019).
- Van Lier, E.A.; Geraedts, J.L.E.; Oomen, P.J.; Giesbers, H.; van Vliet, J.A.; Drijfhout, I.H.; Zonnenberg-Hoff, I.F.; de Melker, H.E. Vaccination Coverage and Annual Report National Immunisation Programme Netherlands 2017 [in Dutch: Vaccinatiegraad en Jaarverslag Rijksvaccinatieprogramma Nederland 2017]; RIVM: Bilthoven, The Netherlands, 2018. [Google Scholar]
- Schurink-van’t Klooster, T.M.; de Melker, H.E. The National Immunisation Programma in the Netherlands—Surveillance and Developments in 2017–2018; RIVM: Bilthoven, The Netherlands, 2018. [Google Scholar]
- Cutts, F.T.; Hanson, M. Seroepidemiology: An underused tool for designing and monitoring vaccination programmes in low- and middle-income countries. Trop. Med. Int. Health TM IH 2016, 21, 1086–1098. [Google Scholar] [CrossRef]
- Verberk, J.D.M.; Vos, R.A.; Mollema, L.; van Vliet, J.; van Weert, J.W.M.; de Melker, H.E.; van der Klis, F.R.M. Third national biobank for population-based seroprevalence studies in the Netherlands, including the Caribbean Netherlands. BMC Infect. Dis. 2019, 19, 470. [Google Scholar] [CrossRef]
- Smits, G.P.; van Gageldonk, P.G.; Schouls, L.M.; van der Klis, F.R.; Berbers, G.A. Development of a bead-based multiplex immunoassay for simultaneous quantitative detection of IgG serum antibodies against measles, mumps, rubella, and varicella-zoster virus. Clin. Vaccine Immunol. CVI 2012, 19, 396–400. [Google Scholar] [CrossRef]
- Mei, J.V.; Alexander, J.R.; Adam, B.W.; Hannon, W.H. Use of filter paper for the collection and analysis of human whole blood specimens. J. Nutr. 2001, 131, 1631s–1636s. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute (CLSI). Blood Collection on Filter Paper for Newborn Screening Programs. In Approved Standard, 6th ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2013. [Google Scholar]
- World Health Organization (WHO). The Immunological Basis for Immunization Series: Module 7: Measles—Update 2009; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- Skendzel, L.P. Rubella immunity. Defining the level of protective antibody. Am. J. Clin. Pathol. 1996, 106, 170–174. [Google Scholar] [CrossRef]
- Andrews, N.; Pebody, R.G.; Berbers, G.; Blondeau, C.; Crovari, P.; Davidkin, I.; Farrington, P.; Fievet-Groyne, F.; Gabutti, G.; Gerike, E.; et al. The European Sero-Epidemiology Network: Standardizing the enzyme immunoassay results for measles, mumps and rubella. Epidemiol. Infect. 2000, 125, 127–141. [Google Scholar] [CrossRef]
- Bickel, P.; Doksum, K. Basic heuristics of estimation. In Mathematical Statistics: Basic Ideas and Selected Topics; Bickel, P., Doksum, K., Eds.; Prentice-Hall: London, UK, 2001; p. 101. [Google Scholar]
- Brinkman, I.D.; de Wit, J.; Smits, G.P.; Ten Hulscher, H.I.; Jongerius, M.C.; Abreu, T.C.; van der Klis, F.R.M.; Hahne, S.J.M.; Koopmans, M.P.G.; Rots, N.Y.; et al. Early measles vaccination during an outbreak in The Netherlands: Reduced short and long-term antibody responses in children vaccinated before 12 months of age. J. Infect. Dis. 2019. [Google Scholar] [CrossRef]
- Statistics Netherlands (CBS). Population Caribbean Netherlands, 1 January 2017. Available online: https://www.cbs.nl/en-gb/custom/2018/04/population-caribbean-netherlands-1-januari-2017 (accessed on 7 June 2019).
- Statistics Netherlands (CBS). Statline: Caribisch Nederland; Bevolking Hoogstbehaald Onderwijsniveau. Available online: http://statline.cbs.nl/ (accessed on 7 June 2019).
- World Health Organization (WHO). Eliminating Measles and Rubella: Framework for the Verification Process in the WHO European Region; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Anderson, R.M.; May, R.M. Immunisation and herd immunity. Lancet (Lond. Engl.) 1990, 335, 641–645. [Google Scholar] [CrossRef]
- Vos, R.A.; Mollema, L.; Kerkhof, J.; van den Kerkhof, J.; Gerstenbluth, I.; Janga-Jansen, A.V.A.; Stienstra, Y.; de Melker, H.E.; van der Klis, F.R.M. Risk of Measles and Diphtheria Introduction and Transmission on Bonaire, Caribbean Netherlands, 2018. Am. J. Trop. Med. Hyg. 2019. [Google Scholar] [CrossRef] [PubMed]
- Dimech, W.; Mulders, M.N. A 16-year review of seroprevalence studies on measles and rubella. Vaccine 2016, 34, 4110–4118. [Google Scholar] [CrossRef] [PubMed]
- Lebo, E.J.; Kruszon-Moran, D.M.; Marin, M.; Bellini, W.J.; Schmid, S.; Bialek, S.R.; Wallace, G.S.; McLean, H.Q. Seroprevalence of measles, mumps, rubella and varicella antibodies in the United States population, 2009–2010. Open Forum Infect. Dis. 2015, 2, ofv006. [Google Scholar] [CrossRef] [PubMed]
- Smits, G.; Mollema, L.; Hahne, S.; de Melker, H.; Tcherniaeva, I.; Waaijenborg, S.; van Binnendijk, R.; van der Klis, F.; Berbers, G. Seroprevalence of mumps in The Netherlands: Dynamics over a decade with high vaccination coverage and recent outbreaks. PLoS ONE 2013, 8, e58234. [Google Scholar] [CrossRef]
- Fischinger, S.; Boudreau, C.M.; Butler, A.L.; Streeck, H.; Alter, G. Sex differences in vaccine-induced humoral immunity. Semin. Immunopathol. 2019, 41, 239–249. [Google Scholar] [CrossRef]
- Cook, I.F. Sexual dimorphism of humoral immunity with human vaccines. Vaccine 2008, 26, 3551–3555. [Google Scholar] [CrossRef]
- Plotkin, S.A. Correlates of protection induced by vaccination. Clin. Vaccine Immunol. CVI 2010, 17, 1055–1065. [Google Scholar] [CrossRef]
- Mollema, L.; Smits, G.P.; Berbers, G.A.; Van Der Klis, F.R.; Van Binnendijk, R.S.; De Melker, H.E.; Hahne, S.J. High risk of a large measles outbreak despite 30 years of measles vaccination in The Netherlands. Epidemiol. Infect. 2014, 142, 1100–1108. [Google Scholar] [CrossRef]
- Smits, G.; Mollema, L.; Hahne, S.; de Melker, H.; Tcherniaeva, I.; van der Klis, F.; Berbers, G. Seroprevalence of rubella antibodies in The Netherlands after 32 years of high vaccination coverage. Vaccine 2014, 32, 1890–1895. [Google Scholar] [CrossRef]
- Guerra, F.M.; Bolotin, S.; Lim, G.; Heffernan, J.; Deeks, S.L.; Li, Y.; Crowcroft, N.S. The basic reproduction number (R0) of measles: A systematic review. Lancet Infect. Dis. 2017, 17, e420–e428. [Google Scholar] [CrossRef]
- Edmunds, W.J.; Gay, N.J.; Kretzschmar, M.; Pebody, R.G.; Wachmann, H. The pre-vaccination epidemiology of measles, mumps and rubella in Europe: Implications for modelling studies. Epidemiol. Infect. 2000, 125, 635–650. [Google Scholar] [CrossRef] [PubMed]
- Seagle, E.E.; Bednarczyk, R.A.; Hill, T.; Fiebelkorn, A.P.; Hickman, C.J.; Icenogle, J.P.; Belongia, E.A.; McLean, H.Q. Measles, mumps, and rubella antibody patterns of persistence and rate of decline following the second dose of the MMR vaccine. Vaccine 2018, 36, 818–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaaijk, P.; Wijmenga-Monsuur, A.J.; van Houten, M.A.; Veldhuijzen, I.K.; Ten Hulscher, H.I.; Kerkhof, J.; van der Klis, F.R.; van Binnendijk, R.S. A Third Dose of Measles-Mumps-Rubella Vaccine to Improve Immunity Against Mumps in Young Adults. J. Infect. Dis. 2019. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, J.; Davidkin, I.; Kafatos, G.; Andrews, N.; Barbara, C.; Cohen, D.; Duks, A.; Griskevicius, A.; Johansen, K.; Bartha, K.; et al. Seroepidemiology of mumps in Europe (1996–2008): Why do outbreaks occur in highly vaccinated populations? Epidemiol. Infect. 2013, 141, 651–666. [Google Scholar] [CrossRef]
- Waaijenborg, S.; Hahne, S.J.; Mollema, L.; Smits, G.P.; Berbers, G.A.; van der Klis, F.R.; de Melker, H.E.; Wallinga, J. Waning of maternal antibodies against measles, mumps, rubella, and varicella in communities with contrasting vaccination coverage. J. Infect. Dis. 2013, 208, 10–16. [Google Scholar] [CrossRef]
- Nic Lochlainn, L.M.; de Gier, B.; van der Maas, N.A.; Strebel, P.M.; Goodman, T.; van Binnendijk, R.S.; de Melker, H.E.; Hahne, S.J.M. Immunogenicity, effectiveness and safety of measles vaccination below nine months of age: A systematic review and meta-analysis. Lancet Infect. Dis. 2019, in press. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sociodemographic Characteristics and Vaccination History | Bonairen n (%) n = 1129 (61.7) | St. Eustatiusn n (%) n = 477 (26.1) | Saban n (%) n = 223 (12.2) | Totaln n (%) n = 1829 | |
|---|---|---|---|---|---|
| Sex | |||||
| Men | 506 (44.8) | 221 (46.3) | 97 (43.5) | 824 (45.1) | |
| Women | 623 (55.2) | 256 (53.7) | 126 (56.5) | 1005 (54.9) | |
| Age, mean (sd) | 34.6 (25.0) | 30.8 (23.7) | 37.5 (25.3) | 34.0 (24.8) | |
| Age groups, years | |||||
| 0–11 | 271 (24.0) | 128 (26.8) | 50 (22.4) | 449 (24.6) | |
| 12–17 | 181 (16.0) | 86 (18.0) | 24 (10.8) | 291 (15.9) | |
| 18–34 | 160 (14.2) | 83 (17.4) | 32 (14.3) | 275 (15.0) | |
| 35–59 | 242 (21.4) | 99 (20.8) | 60 (26.9) | 401 (21.9) | |
| 60–90 | 275 (23.4) | 81 (17.0) | 57 (25.6) | 413 (22.6) | |
| Ethnicity a | |||||
| Dutch overseas territories and Suriname | 803 (71.2) | 383 (82.0) | 126 (57.0) | 1312 (72.2) | |
| Indigenous Dutch and other Western countries | 143 (12.7) | 30 (6.4) | 50 (22.6) | 223 (12.3) | |
| Latin America and other non-Western countries | 182 (16.1) | 54 (11.6) | 45 (20.4) | 281 (15.5) | |
| (Maternal) educational level b | |||||
| High | 172 (15.2) | 68 (14.3) | 87 (39.0) | 327 (17.9) | |
| Middle | 298 (26.4) | 125 (26.2) | 45 (20.2) | 468 (25.6) | |
| Low | 571 (50.6) | 232 (48.6) | 80 (35.9) | 883 (48.3) | |
| Unknown | 88 (7.8) | 52 (10.9) | 11 (4.9) | 151 (8.2) | |
| Monthly gross income | |||||
| High (≥$3001) | 197 (17.4) | 91 (19.1) | 60 (26.9) | 348 (19.0) | |
| Middle ($1501–3000) | 328 (29.1) | 88 (18.5) | 60 (26.9) | 476 (26.0) | |
| Low (<$1500) | 329 (29.1) | 133 (27.8) | 56 (25.1) | 518 (28.3) | |
| Does not want to answer | 106 (9.4) | 73 (15.3) | 23 (10.3) | 202 (11.1) | |
| Unknown | 169 (15.0) | 92 (19.3) | 24 (10.8) | 285 (15.6) | |
| Vaccination history among National Immunization Program (NIP) eligible participants c | |||||
| Measles, total | 672 (59.5) | 302 (63.3) | 107 (48.0) | 1081 (59.1) | |
| 2 or more doses | 215 (32.0) | 106 (35.1) | 29 (27.1) | 350 (32.4) | |
| 1 dose | 248 (36.9) | 118 (39.1) | 51 (47.7) | 417 (38.6) | |
| (Partly) participated in the NIP (self-reported) | 148 (22.0) | 47 (15.5) | 20 (18.7) | 215 (19.9) | |
| Not vaccinated | 61 (9.1) | 31 (10.3) | 7 (6.5) | 99 (9.1) | |
| Mumps, total | 624 (55.3) | 263 (55.1) | 106 (47.5) | 993 (54.3) | |
| 2 or more doses | 213 (34.1) | 99 (37.6) | 29 (27.4) | 341 (34.3) | |
| 1 dose | 245 (39.3) | 113 (43.0) | 51 (48.1) | 409 (41.2) | |
| (Partly) participated in the NIP (self-reported) | 115 (18.4) | 30 (11.4) | 19 (17.9) | 164 (16.5) | |
| Not vaccinated | 51 (8.2) | 21 (8.0) | 7 (6.6) | 79 (8.0) | |
| Rubella, total | 736 (65.2) | 263 (55.1) | 106 (47.5) | 1105 (60.4) | |
| 2 or more doses | 216 (29.3) | 100 (38.0) | 29 (27.4) | 345 (31.2) | |
| 1 dose | 249 (33.8) | 112 (42.6) | 51 (48.1) | 412 (37.3) | |
| (Partly) participated in the NIP (self-reported) | 197 (26.8) | 30 (11.4) | 19 (17.9) | 246 (22.3) | |
| Not vaccinated | 74 (10.0) | 21 (8.0) | 7 (6.6) | 102 (9.2) | |
| Measles | Mumps | Rubella | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Seroprevalence ≥0.120 IU/mL | GMC | Seroprevalence ≥45 RU/mL | GMC | Seroprevalence ≥10.0 IU/mL | GMC | ||||||||
| % | (95% CI) | IU/mL | (95% CI) | % | (95% CI) | RU/mL | (95% CI) | % | (95% CI) | IU/mL | (95% CI) | ||
| Total Caribbean Netherlands population | |||||||||||||
| Overall | 93.8 | (92.3–95.2) | 0.93 | (0.86–1.01) | 85.0 | (83.0–87.0) | 125 | (133–188) | 84.5 | (82.4–86.6) | 31.2 | (28.5–34.2) | |
| Island | |||||||||||||
| Bonaire | 93.7 | (91.9–95.4) | 0.92 | (0.83–1.02) | 86.0 | (83.7–88.3) | 129 | (120–138) | 85.1 | (82.6–87.6) | 32.0 | (28.7–35.6) | |
| St. Eustatius | 93.9 | (91.2–96.5) | 0.97 | (0.83–1.14) | 81.0 | (76.2–85.8) | 104 | (92–118) | 82.3 | (77.8–86.8) | 24.8 | (20.3–30.2) | |
| Saba | 94.9 | (91.4–98.4) | 1.01 | (0.81–1.24) | 81.4 | (75.4–87.4) | 135 | (113–161) | 82.7 | (76.8–88.6) | 36.6 | (27.5–48.7) | |
| Sex | |||||||||||||
| Men | 93.1 | (90.8–95.3) | 0.87 | (0.76–0.99) | 84.9 | (81.8–87.9) | 120 | (110–131) | 86.0 | (82.8–89.1) | 33.6 | (29.2–38.6) | |
| Women | 94.5 | (92.8–96.2) | 1.00 | (0.90–1.12) | 85.1 | (82.5–87.7) | 131 | (121–142) | 83.0 | (80.2–85.8) | 28.8 | (25.6–32.5) | |
| Among NIP eligibles a | |||||||||||||
| Overall | 89.2 | (86.7–91.8) | 0.46 | (0.42–0.51) | 83.9 | (81.0–86.8) | 116 | (107–125) | 87.5 | (84.8–90.1) | 30.6 | (27.5–34.0) | |
| Among non-NIP eligible adults | |||||||||||||
| Overall | 98.6 | (97.6–99.7) | 1.96 | (1.77–2.18) | 85.6 | (83.0–88.7) | 133 | (123–145) | 80.6 | (77.1–84.1) | 32.1 | (27.3–37.7) | |
| Potential Risk Factor for Measles Seronegativity | n (%) n = 1075 | % Measles Seropositive (95% CI) | UnivariateCrude OR b (95% CI) | p Value c | MultivariateaOR b (95% CI) | p Value c | |
|---|---|---|---|---|---|---|---|
| Island | 0.04 | ||||||
| Bonaire | 671 (62.4) | 89.4 (87.1–97.7) | Ref. | ||||
| St. Eustatius | 297 (27.6) | 92.3 (89.2–95.3) | 0.62 (0.37–1.06) | ||||
| Saba | 107 (10.0) | 94.4 (90.0–98.8) | 0.38 (0.15–0.95) | ||||
| Sex | 0.01 | 0.003 | |||||
| Men | 492 (45.8) | 88.6 (85.8–91.4) | 1.78 (1.14–2.78) | 2.06 (1.29–3.30) | |||
| Women | 583 (54.2) | 92.5 (90.3–94.6) | Ref. | Ref. | |||
| Age group, years | <0.0001 | <0.0001 | |||||
| 0–1 | 49 (4.6) | 49.0 (35.0–63.0) | 17.94 (8.71–36.99) | 8.78 (3.80–20.27) | |||
| 2–10 | 356 (33.1) | 94.1 (91.6–96.6) | Ref. | Ref. | |||
| 11–17 | 335 (31.1) | 93.4 (90.8–96.1) | 1.13 (0.61–2.11) | 0.54 (0.26–1.15) | |||
| 18–29 | 172 (16.0) | 88.4 (83.6–93.2) | 2.29 (1.20–4.37) | 1.08 (0.50–2.32) | |||
| 30–41 | 163 (15.1) | 92.6 (88.6–96.7) | 1.78 (1.14–2.78) | 0.40 (0.16–1.00) | |||
| Ethnicity | |||||||
| Dutch overseas territories d and Suriname | 857 (79.7) | 91.9 (90.1–93.8) | Ref. | 0.0001 | |||
| Indigenous Dutch and other Western countries | 80 (7.4) | 92.5 (86.7–98.3) | 1.19 (0.47–3.00) | ||||
| Latin America and other non-Western countries | 138 (12.8) | 81.9 (75.4–88.3) | 3.38 (1.93–5.90) | ||||
| (Maternal) educational level e | 0.097 | ||||||
| High | 171 (15.9) | 90.6 (86.3–95.0) | Ref. | ||||
| Middle | 358 (33.3) | 92.5 (89.7–95.2) | 1.02 (0.50–2.10) | ||||
| Low | 479 (44.6) | 89.4 (86.6–92.1) | 1.89 (0.95–3.75) | ||||
| Unknown | 67 (6.2) | 91.0 (84.2–97.9) | 1.49 (0.52–4.29) | ||||
| Monthly gross income household | 0.74 | ||||||
| High (≥$3,001) | 187 (17.4) | 91.4 (87.4–95.5) | Ref. | ||||
| Middle ($1501–3000) | 272 (25.3) | 91.2 (87.8–94.6) | 1.16 (0.57–2.36) | ||||
| Low (≤$1500) | 219 (20.4) | 89.0 (84.9–93.2) | 1.37 (0.67–2.81) | ||||
| Does not want to answer | 144 (13.4) | 88.9 (83.7–94.0) | 1.70 (0.77–3.75) | ||||
| Unknown | 253 (23.5) | 92.1 (88.8–95.4) | 1.26 (0.56–2.85) | ||||
| Resident of Caribbean Netherlands since, years of age | <0.0001 | 0.005 | |||||
| 0–1 | 703 (65.4) | 91.8 (89.7–93.8) | Ref. | Ref. | |||
| 2–10 | 144 (13.4) | 93.1 (88.9–97.2) | 1.45 (0.69–3.02) | 1.11 (0.52–12.25) | |||
| 11–17 | 47 (4.4) | 72.3 (59.5–85.1) | 9.17 (4.07–20.7) | 5.12 (2.13–12.30) | |||
| 18–41 | 128 (11.9) | 89.8 (84.6–95.1) | 1.89 (0.84–4.27) | 1.03 (0.45–2.37) | |||
| Unknown | 53 (4.9) | 88.7 (80.1–97.2) | 1.85 (0.70–4.90) | 1.46 (0.54–3.97) | |||
| Number of vaccinations against measles f | <0.0001 | <0.0001 | |||||
| 2 or more doses | 349 (32.5) | 95.1 (92.9–97.4) | Ref. | Ref. | |||
| 1 dose | 416 (38.7) | 94.7 (92.6–96.9) | 0.79 (0.38–1.61) | 0.74 (0.36–1.52) | |||
| (Partly) followed NIP (as a child) (self-reported) | 213 (19.8) | 85.9 (81.2–90.6) | 4.29 (2.13–8.63) | 3.24 (1.55–6.75) | |||
| Not vaccinated | 97 (9.0) | 68.0 (58.7–77.3) | 6.82 (3.21–14.49) | 5.67 (2.62–12.25) | |||
| (Parent/caregiver) influenced by beliefs about vaccination g | 0.83 | ||||||
| Yes | 118 (11.0) | 89.0 (83.3–94.6) | Ref. | ||||
| No | 820 (76.3) | 90.7 (88.7–92.7) | 0.83 (0.43–1.60) | ||||
| Unknown | 137 (12.7) | 92.0 (87.4–96.5) | 0.79 (0.32–1.92) | ||||
| Household size, persons | 0.97 | ||||||
| Single-person household | 48 (4.5) | 89.6 (80.9–98.2) | Ref. | ||||
| 2–5 | 868 (80.7) | 90.9 (89.0–92.8) | 0.86 (0.31–2.35) | ||||
| ≥6 | 150 (14.0) | 90.0 (85.2–94.8) | 0.98 (0.31–3.08) | ||||
| Unknown | 9 (0.8) | 88.9 (68.3–100.0) | |||||
| Contact yesterday, persons | 0.31 | ||||||
| 0–8 | 415 (38.6) | 89.6 (86.7–92.6) | Ref. | ||||
| ≥9 | 537 (50.0) | 92.2 (89.9–94.5) | 0.89 (0.55–1.44) | ||||
| Unknown | 123 (11.4) | 87.8 (82.0–93.6) | 1.49 (0.77–2.90) | ||||
| Potential Risk Factor for Mumps Seronegativity | n (%) n = 1816 | % Mumps Seropositive (95% CI) | Univariate Crude OR a (95% CI) | p Value b | Multivariate aOR a (95% CI) | p Value b | |
|---|---|---|---|---|---|---|---|
| Island | 0.29 | ||||||
| Bonaire | 1128 (62.1) | 85.2 (83.1–87.3) | Ref. | ||||
| St. Eustatius | 467 (25.7) | 84.2 (80.8–87.5) | 1.04 (0.77–1.42) | ||||
| Saba | 221 (12.2) | 80.5 (75.3–85.8) | 1.36 (0.93–1.99) | ||||
| Sex | 0.25 | 0.19 | |||||
| Men | 818 (45.0) | 83.5 (81.0–86.0) | 1.17 (0.90–1.52) | 1.20 (0.92–1.56) | |||
| Women | 998 (55.0) | 85.1 (82.9–87.3) | Ref. | Ref. | |||
| Age group, years | <0.0001 | <0.0001 | |||||
| 0–1 | 49 (2.7) | 36.7 (23.3–50.2) | 17.07 (8.57–34.00) | 10.15 (4.72–21.80) | |||
| 2–10 | 356 (19.6) | 83.1 (79.3–87.0) | 1.98 (1.25–3.15) | 1.87 (1.11–3.17) | |||
| 11–17 | 335 (18.5) | 90.7 (87.6–93.9) | Ref. | Ref. | |||
| 18–29 | 172 (9.5) | 84.3 (78.9–89.7) | 1.86 (1.07–3.24) | 1.81 (0.99–3.32) | |||
| 30–59 | 493 (27.1) | 83.2 (79.9–86.5) | 2.02 (1.30–3.14) | 2.02 (0.97–4.21) | |||
| 60–90 | 411 (22.6) | 87.3 (84.1–90.6) | 1.43 (0.89–2.29) | 1.44 (0.62–4.86) | |||
| Ethnicity | 0.13 | ||||||
| Dutch overseas territories c and Suriname | 1312 (72.2) | 83.5 (81.5–85.5) | Ref. | ||||
| Indigenous Dutch and other Western countries | 223 (12.3) | 83.4 (78.5–88.3) | 1.03 (0.69–1.53) | ||||
| Latin America and other non-Western countries | 281 (15.5) | 89.0 (85.3–92.6) | 0.66 (0.44–1.00) | ||||
| (Maternal) educational level d | 0.39 | ||||||
| High | 326 (18.0) | 81.9 (77.7–86.1) | Ref. | ||||
| Middle | 466 (25.7) | 85.6 (82.4–88.8) | 0.83 (0.55–1.24) | ||||
| Low | 877 (48.3) | 84.3 (81.9–86.7) | 1.10 (0.77–1.57) | ||||
| Unknown | 147 (8.1) | 86.4 (80.8–91.9) | 0.88 (0.50–1.54) | ||||
| Monthly gross income | 0.61 | ||||||
| High (≥$3001) | 346 (19.0) | 81.5 (77.4–85.6) | Ref. | ||||
| Middle ($1501–3000) | 475 (26.2) | 84.6 (81.4-87.9) | 0.81 (0.55-1.18) | ||||
| Low (≤$1500) | 513 (28.2) | 85.2 (82.1–88.3) | 0.84 (0.57–1.22) | ||||
| Does not want to answer | 199 (11.0) | 83.4 (78.2–88.6) | 1.08 (0.67–1.75) | ||||
| Unknown | 283 (15.6) | 86.6 (82.6–90.5) | 1.04 (0.62–1.73) | ||||
| Resident of Caribbean Netherlands since, years of age | 0.009 | 0.02 | |||||
| 0–1 | 1034 (56.9) | 83.7 (81.4–85.9) | Ref. | Ref. | |||
| 2–10 | 161 (8.9) | 82.0 (76.0–87.9) | 1.54 (0.98–2.43) | 1.47 (0.92–2.34) | |||
| 11–17 | 54 (3.0) | 78.9 (64.5–87.3) | 2.85 (1.42–5.71) | 2.12 (1.02–4.41) | |||
| 18–39 | 294 (16.2) | 86.7 (82.9–90.6) | 0.73 (0.48–1.11) | 0.63 (0.41–0.97) | |||
| 40–59 | 163 (9.0) | 89.0 (84.1–93.8) | 0.63 (0.36–1.09) | 0.61 (0.35–1.06) | |||
| ≥60 | 28 (1.5) | 89.3 (77.8–100.0) | 0.70 (0.20–2.44) | 0.68 (0.20–2.35) | |||
| Unknown | 82 (4.5) | 84.1 (76.2–92.1) | 1.00 (0.53–1.89) | 0.95 (0.50–1.81) | |||
| Number of vaccinations against mumps e | <0.0001 | <0.0001 | |||||
| 2 or more doses | 349 (19.1) | 94.3 (91.8–96.7) | Ref. | Ref. | |||
| 1 dose | 421 (23.0) | 81.0 (77.2–84.7) | 2.81 (1.63–4.86) | 2.82 (1.63–4.86) | |||
| (Partly) followed NIP (as a child) (self-reported) | 163 (8.9) | 78.5 (72.2–84.8) | 3.93 (2.08–7.42) | 3.75 (1.96–7.15) | |||
| Not vaccinated | 79 (4.3) | 58.2 (47.3–69.1) | 7.17 (3.56–14.44) | 7.00 (3.45–14.18) | |||
| Not eligible for NIP | 817 (44.7) | 85.7 (83.3–88.1) | 3.06 (1.39–6.76) | 2.93 (1.32–6.49) | |||
| Influenced by beliefs about vaccination f | 0.35 | ||||||
| Yes | 195 (10.7) | 84.1 (79.0–89.2) | Ref. | ||||
| No | 1369 (75.4) | 84.7 (82.8–86.6) | 1.00 (0.66–1.54) | ||||
| Unknown | 252 (13.9) | 82.5 (77.8–87.2) | 1.31 (0.78–2.21) | ||||
| Household size, persons | 0.96 | ||||||
| Single-person household | 218 (12.0) | 85.5 (80.9–90.2) | Ref. | ||||
| 2–5 | 1382 (76.1) | 84.2 (82.3–86.2) | 1.01 (0.66–1.54) | ||||
| ≥6 | 204 (11.2) | 84.8 (79.9–89.7) | 0.95 (0.54–1.68) | ||||
| Unknown | 12 (0.7) | 75.0 (50.5–99.5) | 1.40 (0.33–5.92) | ||||
| Contact yesterday, persons | 0.52 | ||||||
| 0–8 | 810 (44.6) | 84.4 (81.9–86.9) | Ref. | ||||
| ≥9 | 794 (43.7) | 84.8 (82.3–87.3) | 0.99 (0.75–1.32) | ||||
| Unknown | 212 (11.7) | 82.5 (77.4–87.7) | 1.25 (0.82–1.89) | ||||
| Mumps symptoms in preceding year g | 0.43 | ||||||
| Yes | 27 (1.5) | 81.5 (66.8–96.1) | Ref. | ||||
| No | 1622 (89.3) | 84.6 (82.9–86.4) | 0.68 (0.25–1.82) | ||||
| Unknown | 167 (9.2) | 82.0 (76.2–87.9) | 0.85 (0.30–2.47) | ||||
| Potential Risk Factor for Rubella Seronegativity | n (%) n = 1816 | % Rubella Seropositive (95% CI) | Univariate Crude OR a(95% CI) | p Value b | Multivariate aOR a (95% CI) | p Value b | |
|---|---|---|---|---|---|---|---|
| Island | 0.48 | ||||||
| Bonaire | 1128 (62.1) | 86.1 (84.1–88.1) | Ref. | ||||
| St. Eustatius | 467 (25.7) | 85.9 (82.7–89.0) | 1.07 (0.77–1.48) | ||||
| Saba | 221 (12.2) | 81.9 (76.8–87.0) | 1.28 (0.86–1.90) | ||||
| Sex | 0.23 | 0.34 | |||||
| Men | 818 (45.0) | 87.0 (84.7–89.3) | Ref. | 0.87 (0.65–1.16) | |||
| Women | 998 (55.0) | 84.3 (82.0–86.5) | 1.18 (0.90–1.56) | Ref. | |||
| Age group, years | <0.0001 | <0.0001 | |||||
| 0–1 | 49 (2.7) | 44.9 (31.0–58.8) | 24.28 (11.53–51.14) | 14.60 (6.50–32.81) | |||
| 2–10 | 356 (19.6) | 95.2 (93.0–97.4) | Ref. | Ref. | |||
| 11–17 | 335 (18.4) | 93.7 (91.1–96.3) | 1.33 (0.69–2.57) | 1.12 (0.54–2.31) | |||
| 18–39 | 337 (18.6) | 85.5 (81.7–89.2) | 3.30 (1.86–5.87) | 2.61 (1.33–5.10) | |||
| 40–59 | 328 (18.1) | 79.6 (75.2–83.9) | 5.04 (2.89–8.79) | 3.34 (1.52–7.35) | |||
| 60–90 | 411 (22.6) | 80.0 (76.2–83.9) | 4.93 (2.86–8.50) | 2.89 (1.25–6.64) | |||
| Ethnicity | 0.0002 | ||||||
| Dutch overseas territories c and Suriname | 1312 (72.2) | 84.8 (82.8–86.7) | 3.16 (1.83–5.43) | ||||
| Indigenous Dutch and other Western countries | 223 (12.3) | 92.8 (89.4–96.2) | Ref. | ||||
| Latin America and other non-Western countries | 281 (15.5) | 83.3 (78.9–87.6) | 2.94 (1.60–5.39) | ||||
| (Maternal) educational level d | 0.053 | ||||||
| High | 326 (18.0) | 86.2 (82.4–89.9) | Ref. | ||||
| Middle | 466 (25.7) | 87.8 (84.8–90.7) | 1.18 (0.76–1.84) | ||||
| Low | 877 (48.3) | 83.8 (81.4–86.2) | 1.59 (1.08–2.35) | ||||
| Unknown | 147 (8.1) | 87.1 (81.6–92.5) | 1.04 (0.57–1.89) | ||||
| Monthly gross income | 0.22 | ||||||
| High (≥$3001) | 346 (19.0) | 87.6 (84.1–91.1) | Ref. | ||||
| Middle ($1501–3000) | 475 (26.2) | 85.5 (82.3–88.6) | 1.28 (0.84–1.96) | ||||
| Low (≤$1,501) | 513 (28.2) | 80.9 (77.5–84.3) | 1.61 (1.07–2.41) | ||||
| Does not want to answer | 199 (11.0) | 85.9 (81.1–90.8) | 1.55 (0.90–2.65) | ||||
| Missing | 283 (15.6) | 91.2 (87.9–94.5) | 1.27 (0.69–2.33) | ||||
| Resident of Caribbean Netherlands since, years of age | <0.0001 | <0.0001 | |||||
| 0–1 | 1034 (56.9) | 84.0 (81.8–86.3) | 3.44 (1.96–6.05) | 3.58 (2.03–6.29) | |||
| 2–10 | 161 (8.9) | 87.0 (81.7–92.2) | 5.68 (2.68–12.03) | 5.48 (2.57–11.69) | |||
| 11–17 | 54 (3.0) | 79.6 (68.9–90.4) | 8.70 (3.46–21.91) | 6.83 (2.66–17.52) | |||
| 18–39 | 294 (16.2) | 86.1 (82.1–90.0) | 1.88 (1.00–3.51) | 1.72 (0.91–3.23) | |||
| 40–59 | 163 (9.0) | 90.2 (85.6–94.8) | Ref. | Ref. | |||
| ≥60 | 28 (1.5) | 96.4 (89.5–100.0) | 0.36 (0.05–2.83) | 0.37 (0.05–2.91) | |||
| Unknown | 82 (4.5) | 90.2 (83.8–96.7) | 1.76 (0.70–4.43) | 1.63 (0.64–4.11) | |||
| Number of vaccinations against rubella e | <0.0001 | <0.0001 | |||||
| 2 or more doses | 349 (19.2) | 95.1 (92.9–97.4) | Ref. | Ref. | |||
| 1 dose | 425 (23.4) | 92.7 (90.2–95.2) | 1.27 (0.65–2.48) | 1.30 (0.67–2.53) | |||
| (Partly) followed NIP (as a child) (self-reported) | 245 (13.5) | 84.9 (80.4–89.4) | 2.37 (1.21–4.65) | 2.45 (1.24–4.84) | |||
| Not vaccinated | 101 (5.6) | 66.3 (57.1–75.6) | 4.76 (2.32–9.75) | 5.15 (2.50–10.62) | |||
| Not eligible for NIP | 696 (38.3) | 79.3 (76.3–82.3) | 3.68 (1.74–7.79) | 3.75 (1.77–7.96) | |||
| Influenced by beliefs about vaccination f | 0.99 | ||||||
| Yes | 195 (10.7) | 85.1 (80.1–90.1) | Ref. | ||||
| No | 1369 (75.4) | 85.5 (83.7–87.4) | 1.02 (0.65–1.58) | ||||
| Unknown | 252 (13.9) | 85.7 (81.4–90.0) | 1.04 (0.60–1.81) | ||||
| Household size, persons | 0.52 | ||||||
| Single-person household | 218 (12.0) | 78.4 (73.0–83.9) | Ref. | ||||
| 2–5 | 1382 (76.1) | 86.5 (84.7–88.3) | 0.78 (0.53–1.13) | ||||
| ≥6 | 204 (11.2) | 86.3 (81.5–91.0) | 0.88 (0.51–1.52) | ||||
| Unknown | 12 (0.7) | 91.7(76.0–100.0) | 0.40 (0.04–3.74) | ||||
| Contact yesterday, persons | 0.003 | ||||||
| 0–8 | 810 (44.6) | 84.3 (81.8–86.8) | Ref. | ||||
| ≥9 | 794 (43.7) | 88.4 (86.2–90.6) | 0.85 (0.63–1.15) | ||||
| Unknown | 212 (11.7) | 79.2 (73.8–84.7) | 1.76 (1.17–2.63) | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vos, R.A.; Mollema, L.; van Binnendijk, R.; Veldhuijzen, I.K.; Smits, G.; Janga-Jansen, A.V.A.; Baboe-Kalpoe, S.; Hulshof, K.; van der Klis, F.R.M.; de Melker, H.E. Seroepidemiology of Measles, Mumps and Rubella on Bonaire, St. Eustatius and Saba: The First Population-Based Serosurveillance Study in Caribbean Netherlands. Vaccines 2019, 7, 137. https://doi.org/10.3390/vaccines7040137
Vos RA, Mollema L, van Binnendijk R, Veldhuijzen IK, Smits G, Janga-Jansen AVA, Baboe-Kalpoe S, Hulshof K, van der Klis FRM, de Melker HE. Seroepidemiology of Measles, Mumps and Rubella on Bonaire, St. Eustatius and Saba: The First Population-Based Serosurveillance Study in Caribbean Netherlands. Vaccines. 2019; 7(4):137. https://doi.org/10.3390/vaccines7040137
Chicago/Turabian StyleVos, Regnerus A., Liesbeth Mollema, Rob van Binnendijk, Irene K. Veldhuijzen, Gaby Smits, Alcira V.A. Janga-Jansen, Sharda Baboe-Kalpoe, Koen Hulshof, Fiona R.M. van der Klis, and Hester E. de Melker. 2019. "Seroepidemiology of Measles, Mumps and Rubella on Bonaire, St. Eustatius and Saba: The First Population-Based Serosurveillance Study in Caribbean Netherlands" Vaccines 7, no. 4: 137. https://doi.org/10.3390/vaccines7040137