Fabrication of Oxygen Releasing Scaffold by Embedding H2O2-PLGA Microspheres into Alginate-Based Hydrogel Sponge and Its Application for Wound Healing


Abstract
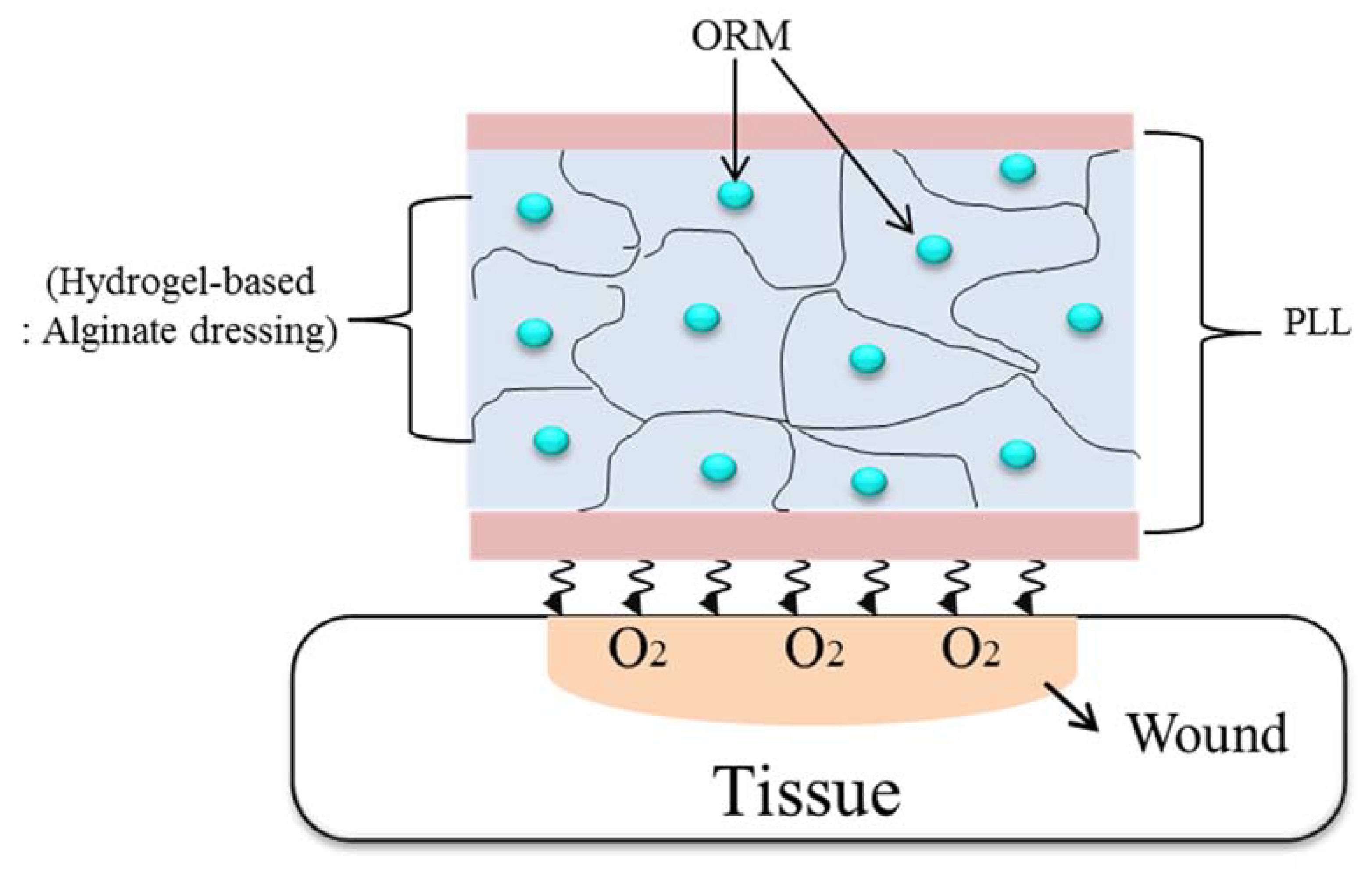
:1. Introduction
2. Materials and Methods
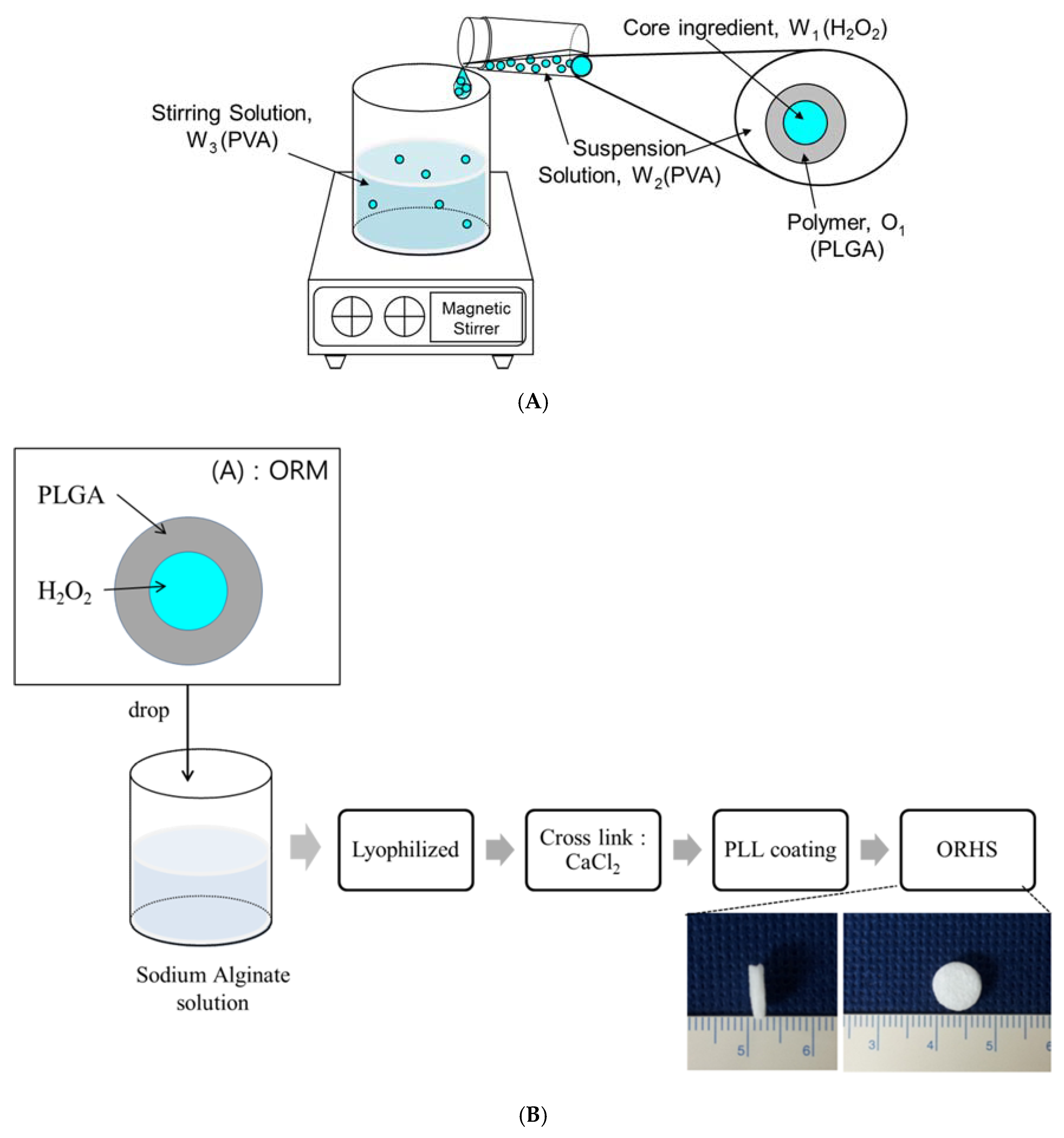
2.1. Preparation of the ORHS
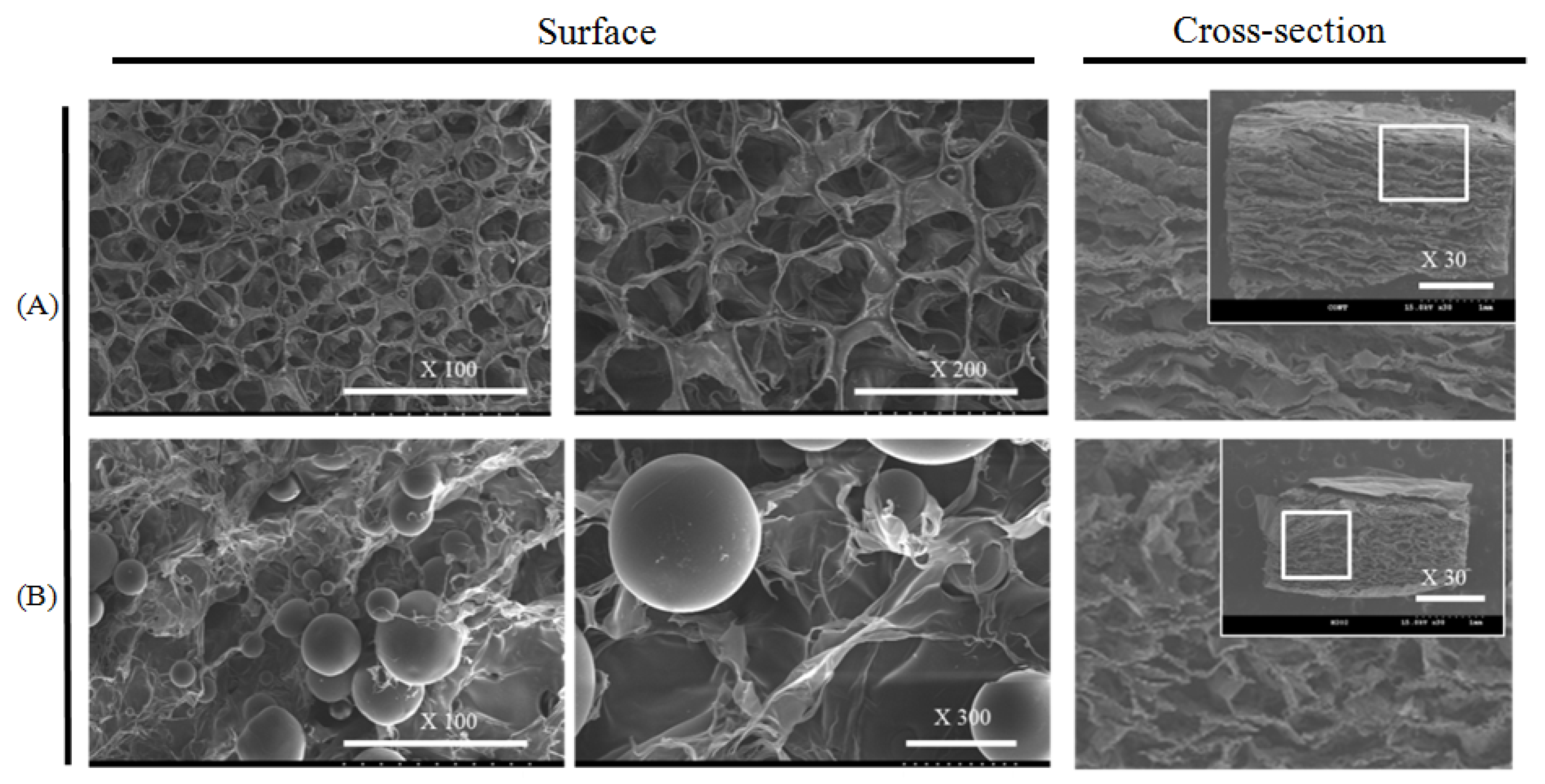
2.2. Morphological Analysis of the ORHS
2.3. Analysis of Oxygen Release from the ORHS
2.4. Analysis of the Release of H2O2 Contained in the ORHS
2.5. In Vitro Study
2.5.1. Biocompatibility of ORHS on Cell Survival Rate
2.5.2. Analysis of Cell Migration Using an In Vitro Wound Model
2.6. Evaluation of In Vivo Efficacy
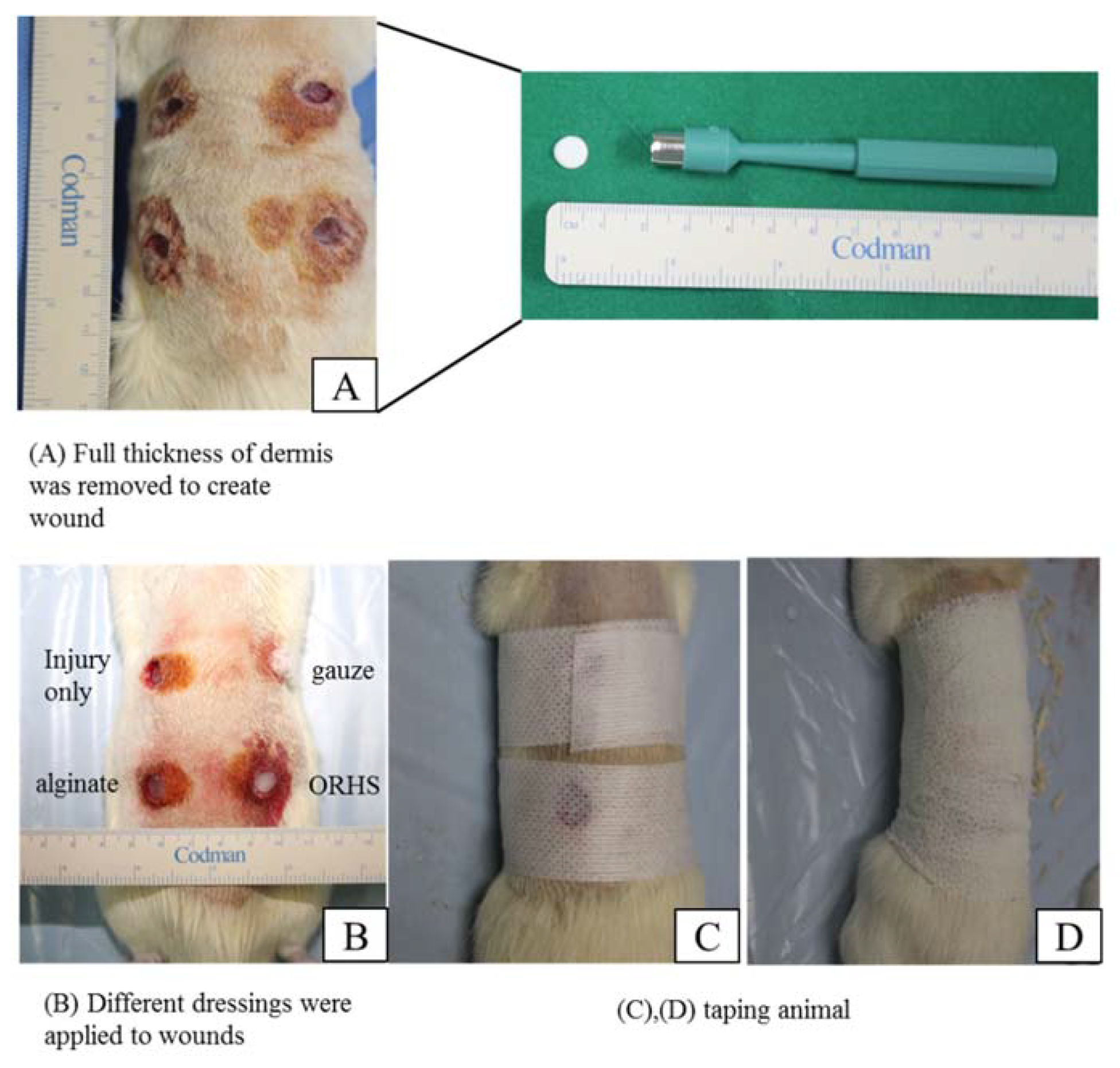
2.6.1. Animal In Vivo Model
2.6.2. Immunohistological Analysis
2.7. Statistical Analysis
3. Results
3.1. Morphological Analysis
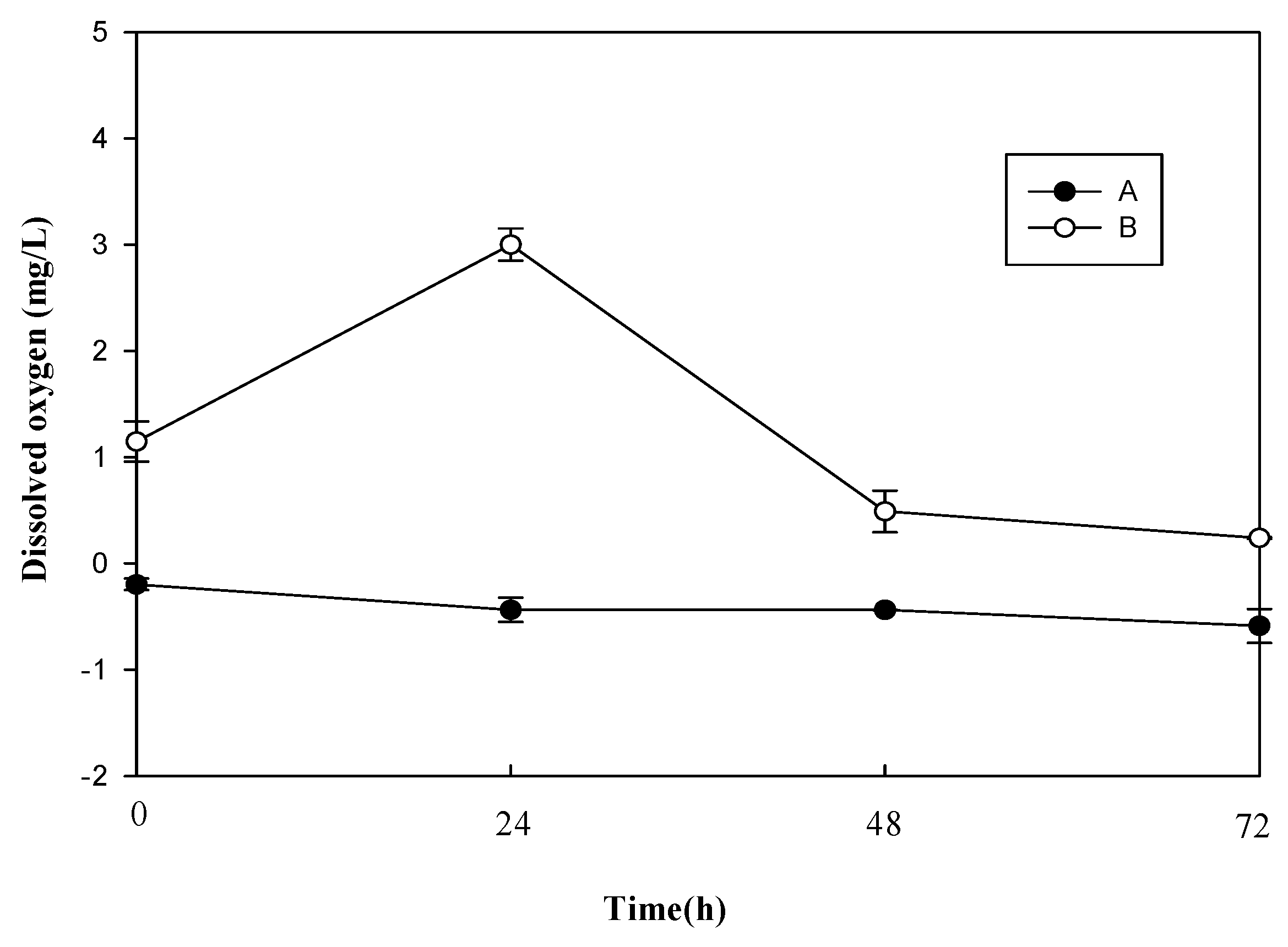
3.2. Release of Oxygen Contained in the ORHS
3.3. Release of H2O2 Contained in the ORHS
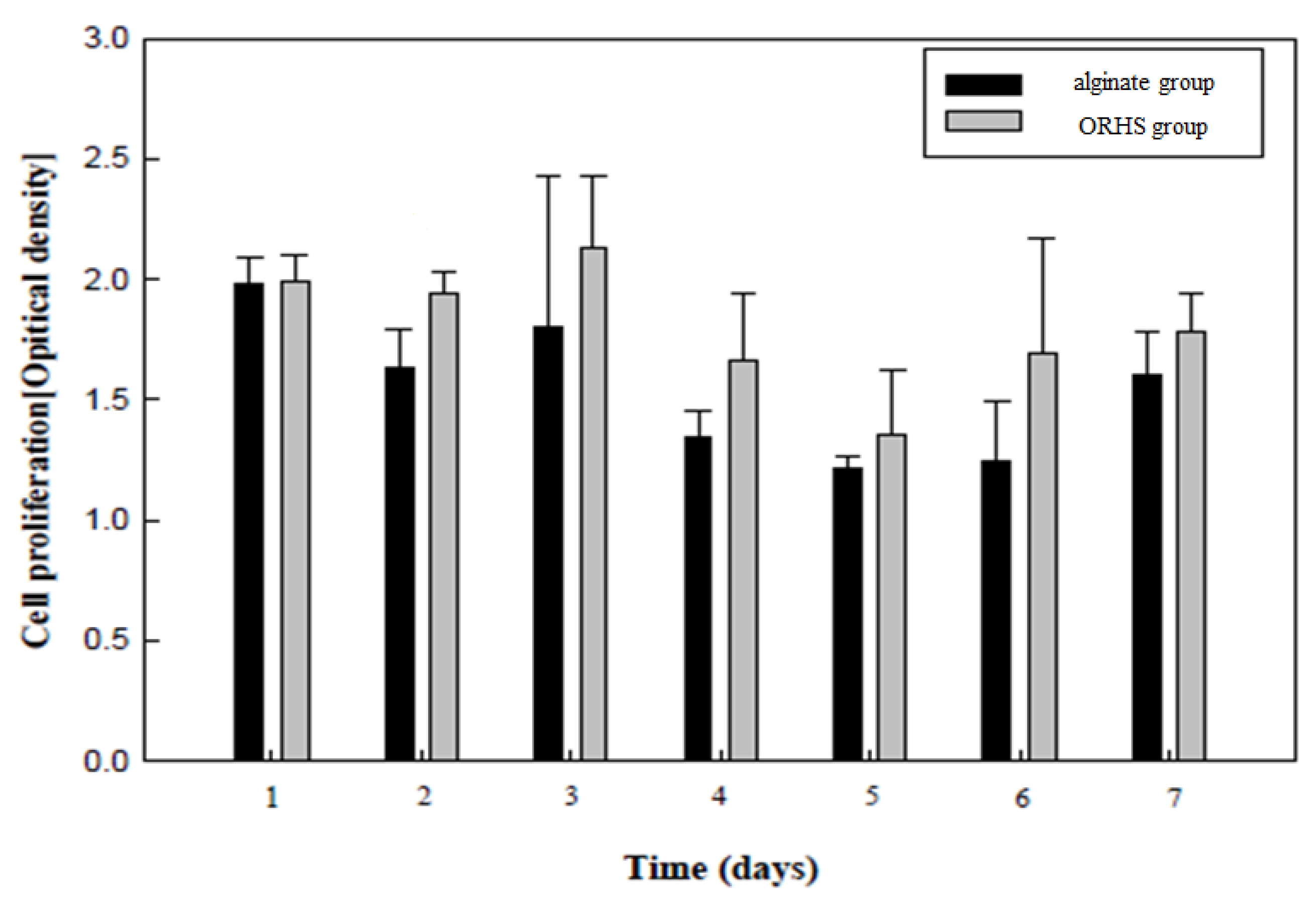
3.4. Biocompatibility of the ORHS
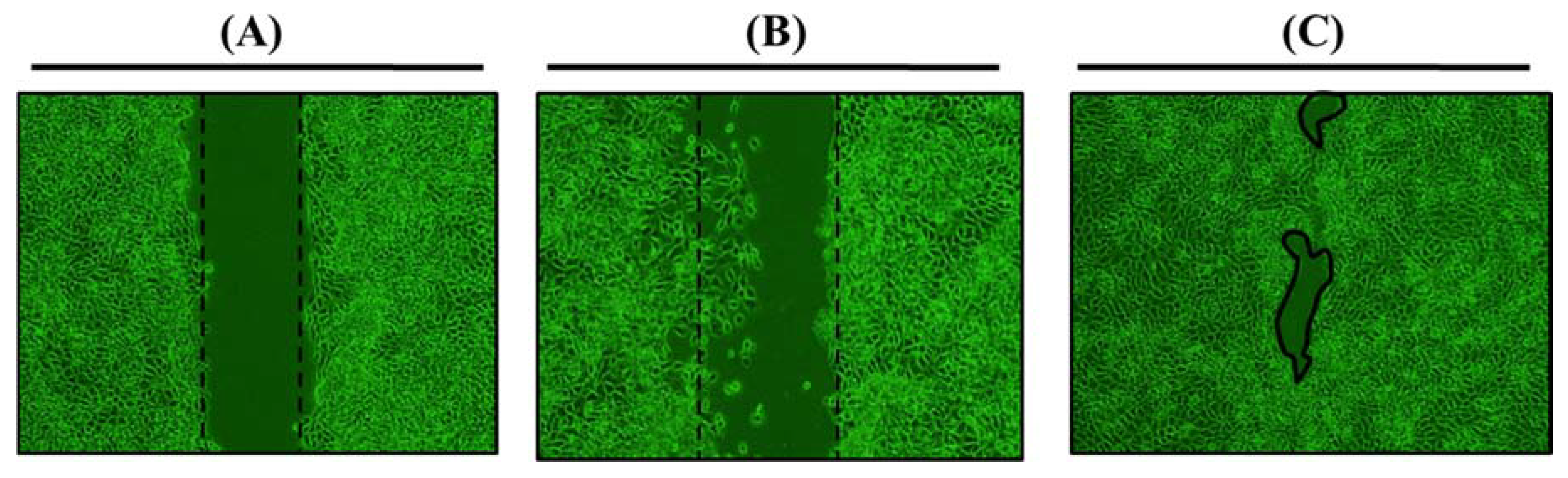
3.5. Evaluation of the Wound Healing Rate Using an in vitro Wound Model
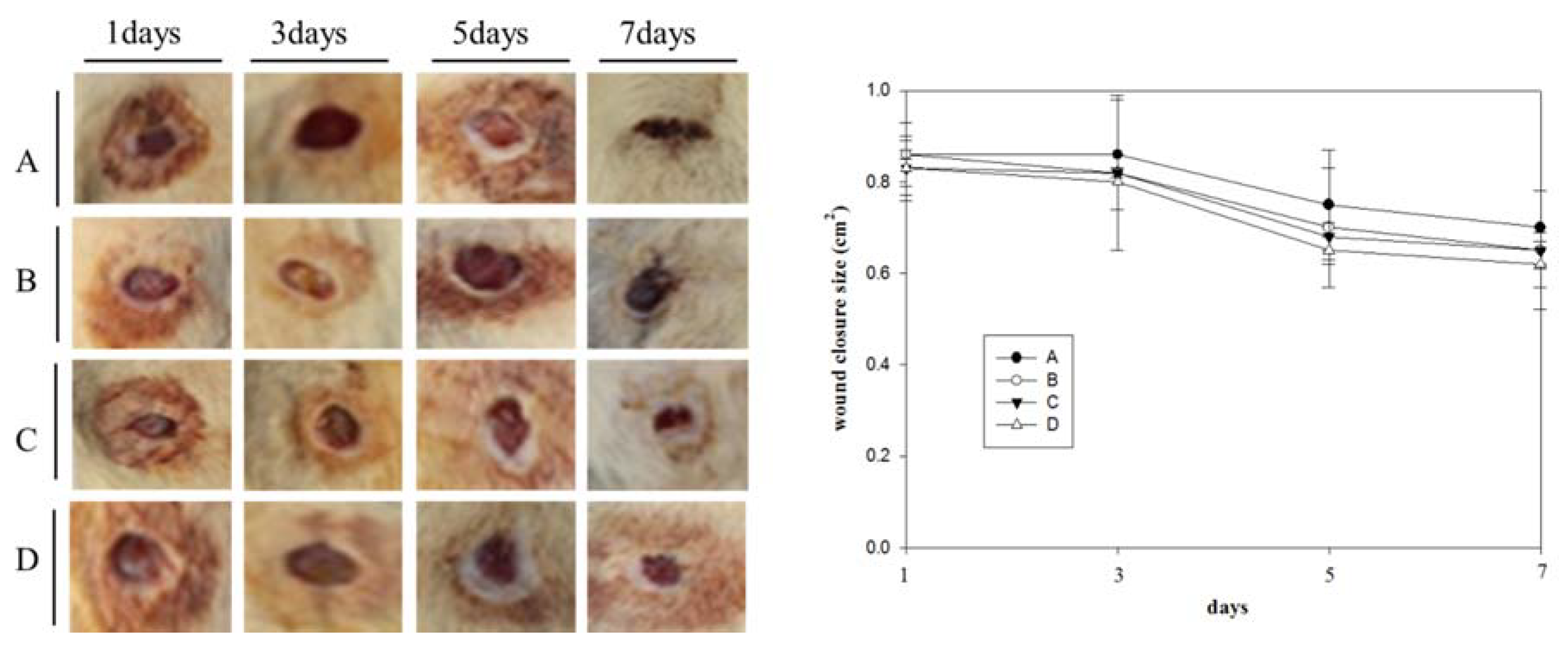
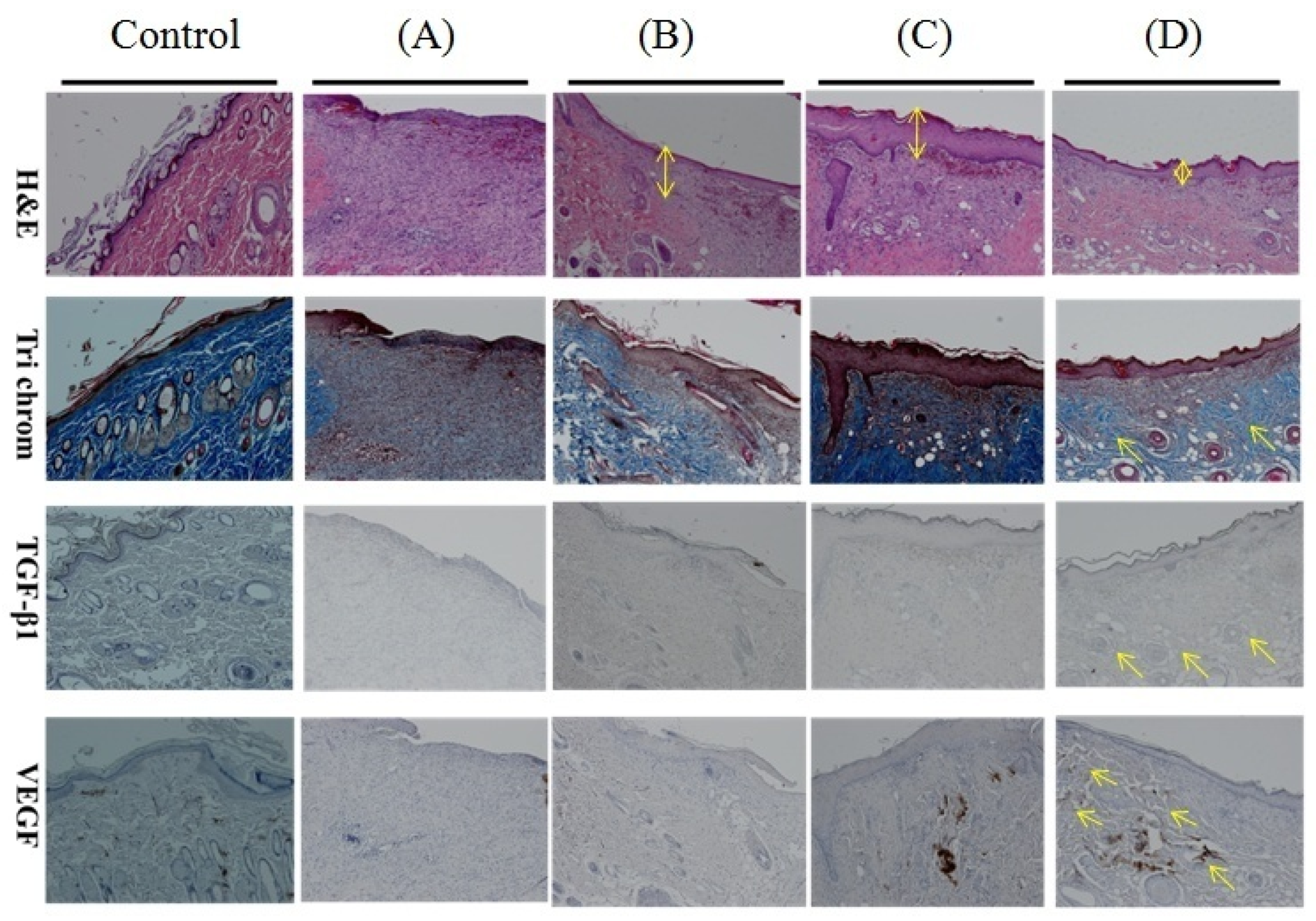
3.6. In Vivo Evaluation
4. Discussion
Author Contributions
Funding
Acknowledgements
Conflicts of Interest
References
- Schäfer, M.; Werner, S. Oxidative stress in normal and impaired wound repair. Pharmacol. Res. 2008, 58, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Cai, L.Y.; Xiong, X.; Kong, X.L.; Xie, J. The role of the lysyl oxidases in tissue repair and remodeling: A concise review. Tissue Eng. Regen. Med. 2017, 14, 15–30. [Google Scholar] [CrossRef]
- Kimmel, H.M.; Grant, A.; Ditata, J. The Presence of oxygen in wound healing. Wounds 2016, 28, 264–270. [Google Scholar] [PubMed]
- Sen, C.K. Wound healing essentials: Let there be oxygen. Wound Repair. Regen. 2009, 17, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khattak, S.F.; Chin, K.S.; Bhatia, S.R.; Roberts, S.C. Enhancing oxygen tension and cellular function in alginate cell encapsulation devices through the use of perfluorocarbons. Biotechnol. Bioeng. 2007, 96, 156–166. [Google Scholar] [CrossRef] [PubMed]
- Selçuk, C.T.; Kuvat, S.V.; Bozkurt, M. The effect of hyperbaric oxygen therapy on the survival of random pattern skin flaps in nicotine treated rats. J. Plast. Reconstr. Aesthet. Surg. 2012, 65, 489–493. [Google Scholar] [CrossRef] [PubMed]
- Harrison, B.S.; Eberli, D.; Lee, S.J.; Atala, A.; Yoo, J.J. Oxygen producing biomaterials for tissue regeneration. Biomaterials 2007, 28, 4628–4634. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.H.; Ward, C.L.; Atala, A.; Yoo, J.J.; Harrison, B.S. Oxygen generating scaffolds for enhancing engineered tissue survival. Biomaterials 2009, 30, 757–762. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.M.; Choi, J.Y.; Han, H.S.; Huh, J.S.; Lim, J.O. Novel microencapsulation of potential drugs with low molecular weight and high hydrophilicity: Hydrogen peroxide as a candidate compound. Int. J. Pharm. 2010, 384, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Abdi, S.I.H.; Ng, S.M.; Lim, J.O. An enzyme-modulated oxygen-producing micro-system for regenerative therapeutics. Int. J. Pharm. 2011, 409, 203–205. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, P.B.; McGinity, J.W. Preparation of microspheres by the solvent evaporation technique. Adv. Drug Deliv. Rev. 1997, 28, 25–42. [Google Scholar] [CrossRef]
- Bae, Y.J.; Cho, C.H.; Lee, W.J.; Huh, J.S.; Lim, J.O. Optimization of recombinant human platelet-derived growth factor-BB encapsulated in Poly(lactic-co-glycolic acid) microspheres for applications in wound healing. Tissue Eng. Regen. Med. 2016, 13, 13–20. [Google Scholar] [CrossRef]
- Park, J.H.; Kwon, D.Y.; Heo, J.Y.; Park, S.H.; Park, J.Y.; Lee, B.; Kim, J.H.; Kim, S.M. Effect of Drug Carrier Melting Points on Drug Release of Dexamethasone-Loaded Microspheres. Tissue Eng. Regen. Med. 2017, 14, 743–753. [Google Scholar] [CrossRef]
- Takeo, M.; Lee, W.; Ito, M. Wound Healing and Skin Regeneration. Cold Spring Harb. Perspect. Med. 2015, 5, a023267. [Google Scholar] [CrossRef] [PubMed]
- Ng, W.Y.; Migotto, A.; Ferreira, T.S.; Lopes, L.B. Monoolein-alginate beads as a platform to promote adenosine cutaneous localization and wound healing. Int. J. Biol. Macromol. 2017, 102, 1104–1111. [Google Scholar] [CrossRef] [PubMed]
- Faragò, S.; Lucconi, G.; Perteghella, S.; Vigani, B.; Giuseppe, T.; Sorrenti, M.; Catenacci, L.; Boschi, A.; Faustini, M.; Vigo, D.; et al. A dry powder formulation from silk fibroin microspheres as a topical auto-gelling device. Pharm. Dev. Technol. 2016, 21, 453–462. [Google Scholar] [CrossRef] [PubMed]
- Theodora, C.; Sara, P.; Silvio, F.; Alessandra, B.; Giuseppe, T.; Barbara, V.; Barbara, C.; Sabrina, R.; Silvia, D.; Stefania, P.; et al. Platelet lysate and adipose mesenchymal stromal cells on silk fibroin nonwoven mats for wound healing. J. Appl. Polym. Sci. 2016, 133, 42942. [Google Scholar] [CrossRef]
- Shapiro, L.; Smadar, C. Novel alginate sponges for cell culture and transplantation. Biomaterials 1997, 18, 583–590. [Google Scholar] [CrossRef]
- Lai, H.L.; Abu’Khalil, A.; Craig, D.Q.M. The preparation and characterisation of drug-loaded alginate and chitosan sponges. Int. J. Pharm. 2003, 251, 175–181. [Google Scholar] [CrossRef]
- Freitas, S.; Merkle, H.P.; Gander, B. Microencapsulation by solvent extraction/evaporation: reviewing the state of the art of microsphere preparation process technology. J. Control. Release 2005, 102, 313–332. [Google Scholar] [CrossRef] [PubMed]
- Schoof, H.; Apel, J.; Heschel, I.; Rau, G. Control of pore structure and size in freeze-dried collagen sponges. J. Biomed. Mater. Res. 2001, 58, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Hydrogen Peroxide Assays. Available online: https://www.cellbiolabs.com/hydrogen-peroxide-assay (accessed on 31 December 2018).
- Kirsner, R.S.; Eaglstein, W.H. The wound healing process. Dermatol. Clin. 1993, 11, 629–640. [Google Scholar] [CrossRef]
- Gurtner, G.C.; Werner, S.; Barrandon, Y.; Longaker, M.T. Wound repair and regeneration. Nature 2008, 453, 314–321. [Google Scholar] [CrossRef] [PubMed]
- MacNeil, S. Progress and opportunities for tissue-engineered skin. Nature 2007, 445, 874–880. [Google Scholar] [CrossRef] [PubMed]
- Werner, S.; Grose, R. Regulation of wound healing by growth factors and cytokines. Physiol. Rev. 2003, 83, 835–870. [Google Scholar] [CrossRef] [PubMed]
- Um, J.H.; Yu, J.Y.; Dubon, M.J.; Park, K.S. Substance P and thiorphansynergically enhance angiogenesis in wound healing. Tissue Eng. Regen. Med. 2016, 13, 149–154. [Google Scholar] [CrossRef]
- Liu, Z.H.; Li, S.; Cai, Y.C.; Wang, A.X.; He, Q.T.; Zheng, C.X.; Zhao, T.T.; Ding, X.Q.; Zhou, X.F. Manganese superoxide dismutase induces migration and invasion of tongue squamous cell carcinoma via H2O2-dependent Snail signaling. Free Radic. Biol. Med. 2012, 53, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Bretón-Romero, R.; Lamas, S. Hydrogen peroxide signaling in vascular endothelial cells. Redox Biol. 2014, 2, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Oshikawa, J.; Urao, N.; Kim, H.W.; Kaplan, N.; Razvi, M.; Mckinney, R.; Poole, L.B.; Fukai, T.; Ushio-Fukai, M. Extracellular SOD-derived H2O2 promotes VEGF signaling in caveolae/lipid rafts and post-ischemic angiogenesis in mice. PLoS ONE 2010, 5, e10189. [Google Scholar] [CrossRef] [PubMed]
- Marinho, H.S.; Real, C.; Cyrne, L.; Soares, H.; Autunes, F. Hydrogen peroxide sensing, signaling and regulation of transcription factors. Redox Biol. 2014, 2, 535–562. [Google Scholar] [CrossRef] [PubMed]
- Muschler, G.F.; Nakamoto, C.; Griffith, L.G. Engineering principles of clinical cell-based tissue engineering. J. Bone Jt. Surg. Am. 2004, 86, 1541–1558. [Google Scholar] [CrossRef]
- Lewis, D.; Goldztein, H.; Deschler, D. Use of hyperbaric oxygen to enhance auricular composite graft survival in the rabbit model. Arch. Facial Plast. Surg. 2006, 8, 310–313. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.O.; Huh, J.S.; Abdi, S.I.H.; Ng, S.M.; Yoo, J.J. Functionalized biomaterials-oxygen releasing scaffolds. J. Biotechnol. Biomater. 2015, 5, 2. [Google Scholar]
- Chua, L.S.; Kim, H.W.; Lee, J.H. Signaling of extracellular matrices for tissue regeneration and therapeutics. Tissue Eng. Regen. Med. 2016, 13, 1–12. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| H2O2 % of Control c (n = 5) | Weight | Total H2O2 μM/Loading Efficiency (%) b |
|---|---|---|
| ORHS a | 10.0 mg | 5.822/0.44 ± 0.0568 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, J.; Hong, G.; Kwon, T.; Lim, J.O. Fabrication of Oxygen Releasing Scaffold by Embedding H2O2-PLGA Microspheres into Alginate-Based Hydrogel Sponge and Its Application for Wound Healing. Appl. Sci. 2018, 8, 1492. https://doi.org/10.3390/app8091492
Choi J, Hong G, Kwon T, Lim JO. Fabrication of Oxygen Releasing Scaffold by Embedding H2O2-PLGA Microspheres into Alginate-Based Hydrogel Sponge and Its Application for Wound Healing. Applied Sciences. 2018; 8(9):1492. https://doi.org/10.3390/app8091492
Chicago/Turabian StyleChoi, Jeongyeon, Gyeongsik Hong, Taegyun Kwon, and Jeong Ok Lim. 2018. "Fabrication of Oxygen Releasing Scaffold by Embedding H2O2-PLGA Microspheres into Alginate-Based Hydrogel Sponge and Its Application for Wound Healing" Applied Sciences 8, no. 9: 1492. https://doi.org/10.3390/app8091492