
Effectiveness of Positive Deviance, an Asset-Based Behavior Change Approach, to Improve Knowledge, Attitudes, and Practices Regarding Dengue in Low-Income Communities (Slums) of Islamabad, Pakistan: A Mixed-Method Study


Abstract
:Simple Summary
Abstract
1. Introduction
Positive Deviance
2. Materials and Methods
2.1. Study Setting
2.2. Study Design and Sampling
| β | Beta error, where power = (1-Beta error): 0.8 |
| α | Alfa error rate: 0.05 |
| E | Effect size: 0.59 |
| N | Sample size: 92 |
2.3. Training of Data Collectors
2.4. Data Management and Analysis
2.5. Ethical Consideration
2.6. Positive Deviance Intervention
2.6.1. Phase 1. PD Process (One Week)
- Community sensitization meeting
- Situation analysis
- Positive deviance inquiry
- Community feedback session and action planning
2.6.2. Phase 2. Positive Deviance Intervention (2 Months)
- Training of volunteers and IEC materials development
- Interactive PD sessions
- PD Seminar
3. Results
3.1. Sociodemographics at the Baseline
3.2. Dengue Knowledge at Baseline
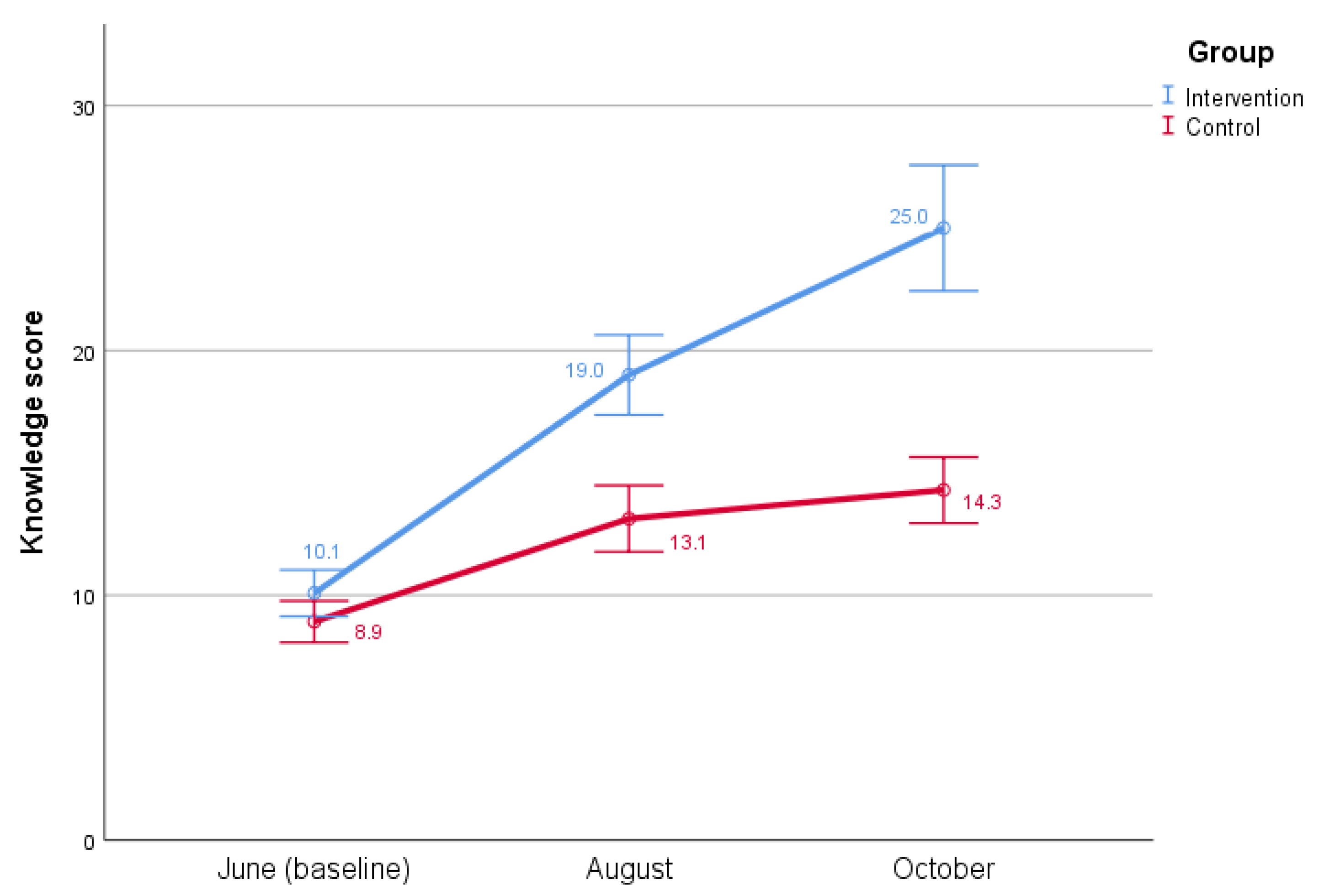
3.3. Knowledge about Dengue at the Baseline, Midline, and Endline
3.4. Knowledge Score Comparison between Intervention vs. Control Groups
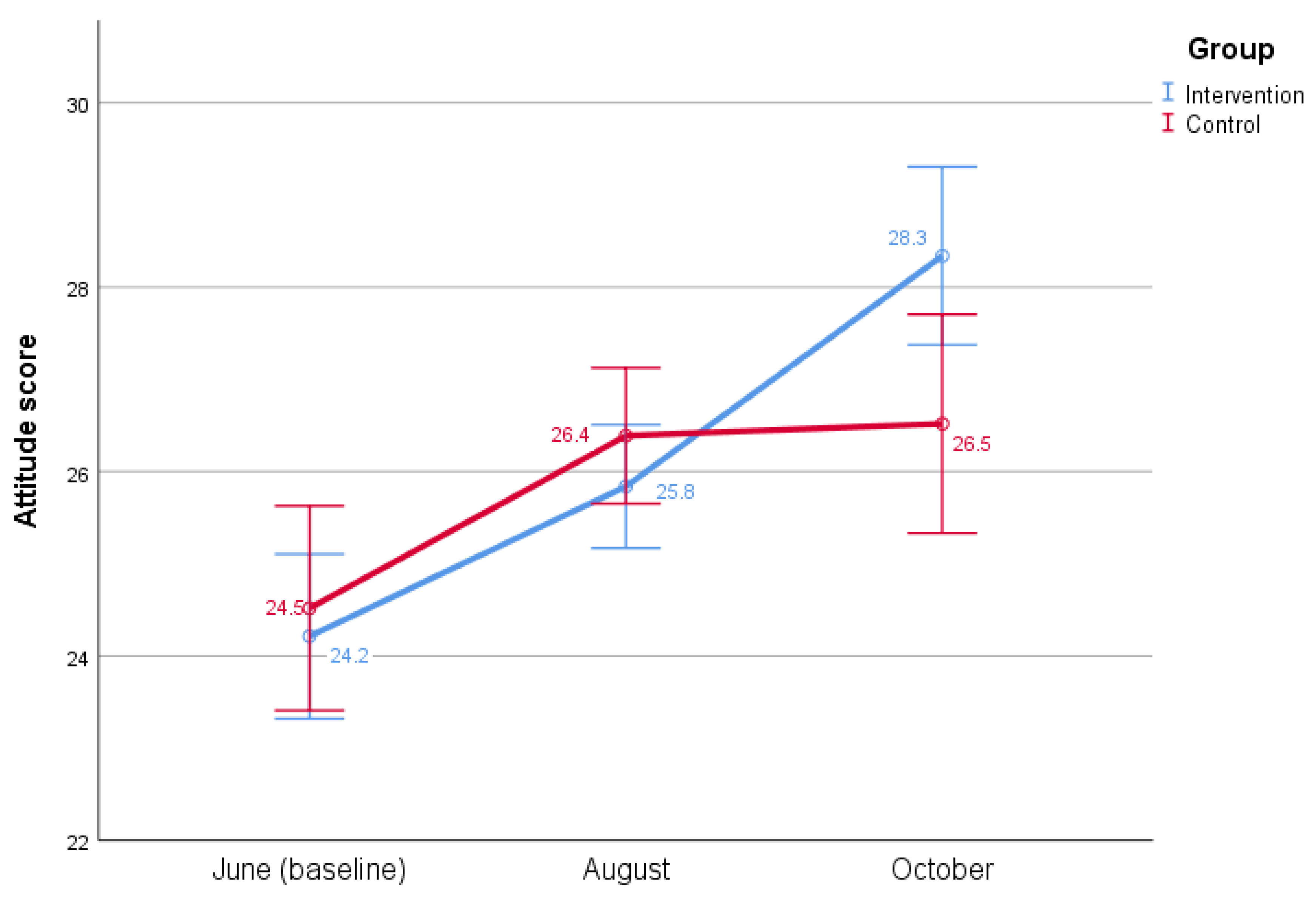
3.5. Attitude towards Dengue at Baseline, Midline, and Endline
3.6. Attitude Scores Comparison between Intervention and Control Groups
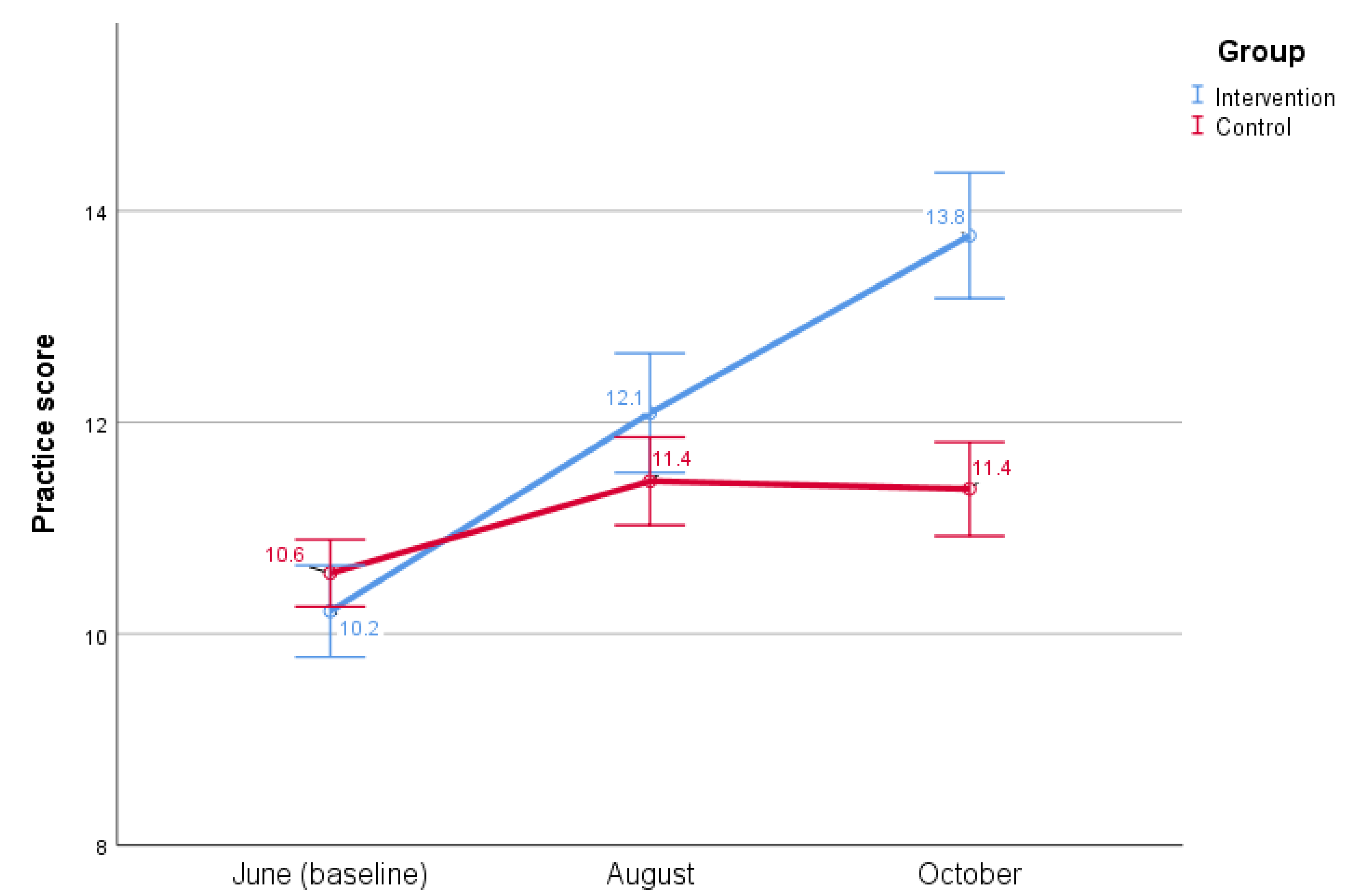
3.7. Dengue Prevention and Control Practices at Baseline, Midline and Endline
3.8. Practice Score Comparison between Intervention and Control Groups
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kraemer, M.U.G.; Sinka, M.E.; Duda, K.A.; Mylne, A.Q.N.; Shearer, F.M.; Barker, C.M.; Moore, C.G.; Carvalho, R.G.; Coelho, G.E.; Van Bortel, W.; et al. The global distribution of the arbovirus vectors Aedes aegypti and Ae. albopictus. eLife 2015, 4, e08347. [Google Scholar] [CrossRef]
- Brady, O.J.; Gething, P.W.; Bhatt, S.; Messina, J.P.; Brownstein, J.S.; Hoen, A.G.; Moyes, C.L.; Farlow, A.W.; Scott, T.W.; Hay, S.I. Refining the Global Spatial Limits of Dengue Virus Transmission by Evidence-Based Consensus. PLoS Negl. Trop. Dis. 2012, 6, e1760. [Google Scholar] [CrossRef]
- Mitra, A.K.; Mawson, A.R. Neglected Tropical Diseases: Epidemiology and Global Burden. Trop. Med. Infect. Dis. 2017, 2, 36. [Google Scholar] [CrossRef] [Green Version]
- Bhatt, S.; Gething, P.W.; Brady, O.J.; Messina, J.P.; Farlow, A.W.; Moyes, C.L.; Drake, J.M.; Brownstein, J.S.; Hoen, A.G.; Sankoh, O.; et al. The global distribution and burden of dengue. Nature 2013, 496, 504–507. [Google Scholar] [CrossRef]
- Guzman, M.G.; Gubler, D.J.; Izquierdo, A.; Martinez, E.; Halstead, S.B. Dengue infection. Nat. Rev. Dis. Primers 2016, 2, 16055. [Google Scholar] [CrossRef] [PubMed]
- Messina, J.P.; Brady, O.J.; Scott, T.W.; Zou, C.; Pigott, D.M.; Duda, K.A.; Bhatt, S.; Katzelnick, L.; Howes, R.E.; Battle, K.E.; et al. Global spread of dengue virus types: Mapping the 70 year history. Trends Microbiol. 2014, 22, 138–146. [Google Scholar] [CrossRef] [Green Version]
- Ebi, K.L.; Nealon, J. Dengue in a changing climate. Environ. Res. 2016, 151, 115–123. [Google Scholar] [CrossRef] [Green Version]
- Murray, N.E.A.; Quam, M.B.; Wilder-Smith, A. Epidemiology of dengue: Past, present and future prospects. Clin. Epidemiol. 2013, 5, 299–309. [Google Scholar]
- Khan, J.; Khan, I.; Ghaffar, A.; Khalid, B. Epidemiological trends and risk factors associated with dengue disease in Pakistan (1980–2014): A systematic literature search and analysis. BMC Public Health 2018, 18, 745. [Google Scholar] [CrossRef]
- Rasheed, S.B.; Butlin, R.K.; Boots, M. A review of dengue as an emerging disease in Pakistan. Public Health 2013, 127, 11–17. [Google Scholar] [CrossRef]
- Chan, Y.C.; Salahuddin, N.; Khan, J.; Tan, H.C.; Seah, C.L.K.; Li, J.; Chow, V.T.K. Dengue haemorrhagic fever outbreak in Karachi, Pakistan, 1994. Trans. R. Soc. Trop. Med. Hyg. 1995, 89, 619–620. [Google Scholar] [CrossRef]
- Zahir, A.; Ullah, A.; Shah, M.; Mussawar, A. Community Participation, Dengue Fever Prevention and Control Practices in Swat, Pakistan. Int. J. MCH AIDS 2016, 5, 39–45. [Google Scholar] [CrossRef]
- Abdullah, S.A.; Salman, M.; Din, M.; Khan, K.; Ahmad, M.; Khan, F.H.; Arif, M. Dengue Outbreaks in Khyber Pakhtunkhwa (KPK), Pakistan in 2017: An Integrated Disease Surveillance and Response System (IDSRS)-Based Report. Pol. J. Microbiol. 2019, 68, 115–119. [Google Scholar] [CrossRef] [Green Version]
- Baloch, M.; Baig, A.M.; Ochani, R.K. Is Dengue the new rising global health problem? The outbreak of 2019 in Pakistan. Minerva Med. 2020. [Google Scholar] [CrossRef]
- Capeding, M.R.; Tran, N.H.; Hadinegoro, S.R.; Ismail, H.I.; Chotpitayasunondh, T.; Chua, M.N.; Luong, C.Q.; Rusmil, K.; Wirawan, D.N.; Nallusamy, R.; et al. Clinical efficacy and safety of a novel tetravalent dengue vaccine in healthy children in Asia: A phase 3, randomised, observer-masked, placebo-controlled trial. Lancet 2014, 384, 1358–1365. [Google Scholar] [CrossRef]
- Vannice, K.S.; Roehrig, J.T.; Hombach, J. Next generation dengue vaccines: A review of the preclinical development pipeline. Vaccine 2015, 33, 7091–7099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Echaubard, P.; Thy, C.; Sokha, S.; Srun, S.; Nieto-Sanchez, C.; Grietens, K.P.; Juban, N.R.; Mier-Alpano, J.; Deacosta, S.; Sami, M.; et al. Fostering social innovation and building adaptive capacity for dengue control in Cambodia: A case study. Infect. Dis. Poverty 2020, 9, 126. [Google Scholar] [CrossRef]
- Al-Muhandis, N.; Hunter, P.R. The Value of Educational Messages Embedded in a Community-Based Approach to Combat Dengue Fever: A Systematic Review and Meta Regression Analysis. PLoS Negl. Trop. Dis. 2011, 5, e1278. [Google Scholar] [CrossRef] [PubMed]
- Nguyen-Tien, T.; Probandari, A.; Ahmad, R.A.; Thang, N.T. Barriers to Engaging Communities in a Dengue Vector Control Program: An Implementation Research in an Urban Area in Hanoi City, Vietnam. Am. J. Trop. Med. Hyg. 2019, 100, 964–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zakus, J.D.; Lysack, C.L. Revisiting community participation. Health Policy Plan 1998, 13, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Wai, K.T.; Htun, P.T.; Oo, T.; Myint, H.; Lin, Z.; Kroeger, A.; Sommerfeld, J.; Petzold, M. Community-centred eco-bio-social approach to control dengue vectors: An intervention study from Myanmar. Pathog. Glob. Health 2012, 106, 461–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toledo, M.; Vanlerberghe, V.; Baly, A.; Ceballos, E.; Valdes, L.; Searret, M.; Boelaert, M.; Van Der Stuyft, P. Towards active community participation in dengue vector control: Results from action research in Santiago de Cuba, Cuba. Trans. R. Soc. Trop. Med. Hyg. 2007, 101, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Vanlerberghe, V.; Toledo, M.E.; Rodríguez, M.; Gomez, D.; Baly, A.; Benitez, J.R.; Van der Stuyft, P. Community involvement in dengue vector control: Cluster randomised trial. BMJ 2009, 338, b1959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shafique, M.; Lopes, S.; Doum, D.; Keo, V.; Sokha, L.; Sam, B.; Vibol, C.; Alexander, N.; Bradley, J.; Liverani, M.; et al. Implementation of guppy fish (Poecilia reticulata), and a novel larvicide (Pyriproxyfen) product (Sumilarv 2MR) for dengue control in Cambodia: A qualitative study of acceptability, sustainability and community engagement. PLoS Negl. Trop. Dis. 2019, 13, e0007907. [Google Scholar] [CrossRef] [PubMed]
- Ahrari, M.; Houser, R.F.; Yassin, S.; Mogheez, M.; Hussaini, Y.; Crump, P.; Darmstadt, G.L.; Marsh, D.; Levinson, F.J. A Positive Deviance-based Antenatal Nutrition Project Improves Birth-weight in Upper Egypt. J. Health Popul. Nutr. 2006, 24, 498–507. [Google Scholar] [PubMed]
- Fowles, E.R.; Hendricks, J.A.; Walker, L.O. Identifying Healthy Eating Strategies in Low-Income Pregnant Women: Applying a Positive Deviance Model. Health Care Women Int. 2005, 26, 807–820. [Google Scholar] [CrossRef]
- Kanani, S.; Popat, K. Growing Normally in an Urban Environment: Positive Deviance among Slum Children of Vadodara, India. Indian J. Pediatr. 2012, 79, 606–611. [Google Scholar] [CrossRef]
- Ndiaye, M.; Siekmans, K.; Haddad, S.; Receveur, O. Impact of a Positive Deviance Approach to Improve the Effectiveness of an Iron-Supplementation Program to Control Nutritional Anemia among Rural Senegalese Pregnant Women. Food Nutr. Bull. 2009, 30, 128–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabbay, R.A.; Friedberg, M.W.; Miller-Day, M.; Cronholm, P.F.; Adelman, A.; Schneider, E.C. A Positive Deviance Approach to Understanding Key Features to Improving Diabetes Care in the Medical Home. Ann. Fam. Med. 2013, 11, S99–S107. [Google Scholar] [CrossRef] [Green Version]
- Shafique, M.; Edwards, H.M.; De Beyl, C.Z.; Thavrin, B.K.; Min, M.; Roca-Feltrer, A. Positive deviance as a novel tool in malaria control and elimination: Methodology, qualitative assessment and future potential. Malar. J. 2016, 15, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marsh, D.R.; Sternin, M.; Khadduri, R.; Ihsan, T.; Nazir, R.; Bari, A.; Lapping, K. Identification of Model Newborn Care Practices through a Positive Deviance Inquiry to Guide Behavior-Change Interventions in Haripur, Pakistan. Food Nutr.Bull. 2002, 23, 107–116. [Google Scholar] [CrossRef] [Green Version]
- Lapping, K.; Marsh, D.R.; Rosenbaum, J.; Swedberg, E.; Sternin, J.; Sternin, M.; Schroeder, D.G. The positive deviance approach: Challenges and opportunities for the future. Food Nutr. Bull. 2002, 23, 130–137. [Google Scholar] [CrossRef]
- Marsh, D.R.; Schroeder, D.G.; A Dearden, K.; Sternin, J.; Sternin, M. The power of positive deviance. BMJ 2004, 329, 1177–1179. [Google Scholar] [CrossRef] [Green Version]
- Mackintosh, U.A.T.; Marsh, D.R.; Schroeder, D.G. Sustained positive deviant child care practices and their effects on child growth in Viet Nam. Food Nutr. Bull. 2002, 23, 18–27. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanklang, S.; Ratanasiripong, P.; Sivasan, S. Effectiveness of the intervention program for dengue hemorrhagic fever prevention among rural communities in Thailand. J. Health Res. 2018, 32, 352–363. [Google Scholar] [CrossRef] [Green Version]
- Kumaran, E.; Doum, D.; Keo, V.; Sokha, L.; Sam, B.; Chan, V.; Alexander, N.; Bradley, J.; Liverani, M.; Prasetyo, D.B.; et al. Dengue knowledge, attitudes and practices and their impact on community-based vector control in rural Cambodia. PLoS Negl. Trop. Dis. 2018, 12, e0006268. [Google Scholar] [CrossRef] [Green Version]
- Hustedt, J.C.; Doum, D.; Keo, V.; Ly, S.; Sam, B.; Chan, V.; Alexander, N.; Bradley, J.; Liverani, M.; Prasetyo, D.B.; et al. Field Efficacy of Larvivorous Fish and Pyriproxyfen Combined with Community Engagement on Dengue Vectors in Cambodia: A Randomized Controlled Trial. Am. J. Trop. Med. Hyg. 2021, 105, 1265–1276. [Google Scholar] [CrossRef]
- Parks, W.; Lloyd, L. Planning Social Mobilization and Communication for Dengue Fever Prevention and Control: A Step-by-Step Guide; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Gubler, D.J.; Clark, G.G. Community-Based Integrated Control of Aedes Aegypti: A Brief Overview of Current Programs. Am. J. Trop. Med. Hyg. 1994, 50, 50–60. [Google Scholar] [CrossRef]
- Hone, T.; Macinko, J.; Millett, C. Revisiting Alma-Ata: What is the role of primary health care in achieving the Sustainable Development Goals? Lancet 2018, 392, 1461–1472. [Google Scholar] [CrossRef]
- Rifkin, S.B. Paradigms lost: Toward a new understanding of community participation in health programmes. Acta Trop. 1996, 61, 79–92. [Google Scholar] [CrossRef]
- Figueroa, M.E.; Kincaid, D.L.; Rani, M.; Lewis, G. Communication for Social Change: An Integrated Model for Measuring the Process and Its Outcomes; The Rockefeller Foundation: New York, NY, USA, 2002. [Google Scholar]
- Castro, M.; Sánchez, L.; Pérez, D.; Carbonell, N.; Lefèvre, P.; Vanlerberghe, V.; Van der Stuyft, P. A community empowerment strategy embedded in a routine dengue vector control programme: A cluster randomised controlled trial. Trans. R. Soc. Trop. Med. Hyg. 2012, 106, 315–321. [Google Scholar] [CrossRef]
- Caprara, A.; Lima, J.W.D.O.; Peixoto, A.C.R.; Motta, C.M.V.; Nobre, J.M.S.; Sommerfeld, J.; Kroeger, A. Entomological impact and social participation in dengue control: A cluster randomized trial in Fortaleza, Brazil. Trans. R. Soc. Trop. Med. Hyg. 2015, 109, 99–105. [Google Scholar] [CrossRef] [Green Version]
- Tyagi, B.K.; Samuel, M.; Krishnamoorthi, R.; Manavalan, R.; Tewari, S.C.; Ashokkumar, V.; Kroeger, A.; Sommerfeld, J.; Petzold, M. Community-based control of Aedes aegypti by adoption of eco-health methods in Chennai City, India. Pathog. Glob. Health 2012, 106, 488–496. [Google Scholar]
- Lloyd, L.S.; Winch, P.; Ortega-Canto, J.; Kendall, C. The Design of a Community-Based Health Education Intervention for the Control of Aedes aegypti. Am. J. Trop. Med. Hyg. 1994, 50, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, J.-A.; Vallely, A.; Fitzgerald, L.; Whittaker, M.; Tanner, M. The architecture and effect of participation: A systematic review of community participation for communicable disease control and elimination. Implications for malaria elimination. Implications for malaria elimination. Malar. J. 2011, 10, 225. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Desired Behaviors | Positive Deviance Behaviors |
|---|---|
| Knowledge | Correct knowledge of the dengue vector and mosquito biting time |
| Knowledge of dengue mosquito’s breeding places inside and outside the house | |
| Avoid water storage | A housewife does not store water. She uses it immediately so that the dengue mosquitoes do not breed in the clean water |
| Change the water in plants | A housewife changes the water in her plants every day to ensure no mosquitoes breed inside the plants |
| Cover the water containers | A housewife covers all the water tanks and water containers to avoid mosquito breeding |
| Clean the water tank | A male community member covers his water tank and cleans it on regular basis to avoid any mosquito breeding |
| A female community member cleans her water tank with a brush and soap twice a week to avoid mosquito breeding | |
| Bury the old bottles and tins | A housewife collects the old bottles and tins and buries them outside the house to avoid mosquitoes breeding in them |
| Clean the tray under refrigerator | A female community member cleans the tray which lies under the refrigerators to avoid the breeding of mosquitoes in it |
| Change the water in the water cooler fan | A female community member changes the water in her watercooler fan on daily basis to avoid mosquito growth inside it |
| Healthcare seeking | A female community member knows the signs and symptoms of dengue fever and seeks treatment as soon as she suspects dengue |
| Personal protection | A mother ensures that her children wear full-sleeved clothes during the day to avoid mosquito bites |
| A mother keeps her children sleeping under bed net during the day to avoid mosquito bites | |
| A father ensures that his children wear long-sleeved clothes to avoid mosquito bites during the day |
| Characteristics (N = 112) | Intervention Group | Control Group | |||
|---|---|---|---|---|---|
| n (%) | Median (Range) | n (%) | Median (Range) | p-Value * | |
| Sex | |||||
| Female | 47 (83.9) | - | 42 (75.0) | - | 1.000 |
| Male | 9 (16.1) | - | 14 (25.0) | - | |
| Age | 31.0 (18–58) | 30.0 (18–55) | |||
| <30 | 24 (42.9) | 24.0 (18–28) | 25 (44.6) | 21.0 (18–29) | 0.789 |
| ≥30 | 32 (57.1) | 35.5 (30–58) | 31 (55.4) | 37.0 (30–55) | |
| Marital status | |||||
| Single | 15 (26.8) | - | 13 (23.2) | - | 1.000 |
| Married | 41 (73.2) | - | 43 (76.8) | - | |
| Religion | |||||
| Christian | 56 (100) | - | 56 (100) | - | |
| Education | |||||
| Primary school (1–5) | 5 (8.9) | - | 7 (12.5) | - | 0.285 |
| Secondary school (5–9) | 6 (10.7) | - | 11 (19.6) | - | |
| High school (10) | 14 (25.0) | - | 19 (33.9) | - | |
| Intermediate-FA | 5 (8.9) | - | 3 (5.4) | - | |
| Bachelor-BA | 1 (1.8) | - | 1 (1.8) | - | |
| Masters-MA | 0 (0) | - | 2 (3.6) | - | |
| No formal education | 25 (44.6) | - | 13 (23.2) | - | |
| Occupation | |||||
| Unemployed | 15 (26.8) | - | 15 (26.8) | - | 0.114 |
| Government job | 3 (5.4) | - | 1 (1.8) | - | |
| Private job | 11 (19.6) | - | 14 (25.0) | - | |
| Street vendor | 1 (1.8) | - | 2 (3.6) | - | |
| Housewife | 24 (42.9) | - | 24 (42.9) | - | |
| Others | 2 (3.6) | - | 0 (0) | - | |
| Average monthly income (Rupees) | |||||
| <25,000 | 36 (64.3) | - | 31 (55.4) | - | 0.896 |
| 25,000–50,000 | 11 (19.6) | - | 16 (28.6) | - | |
| 50,000–75,000 | 4 (7.1) | - | 2 (3.6) | - | |
| >100,000 | 1 (1.8) | - | 0 (0) | - | |
| Don’t know | 4 (7.1) | - | 7 (12.5) | - | |
| n | % | n | % | ||
|---|---|---|---|---|---|
| Baseline | Intervention Group (n = 56) | Control Group (n = 56) | p-Value | ||
| Knowledge | |||||
| Dengue is mosquito-transmitted | 38 | 67.9 | 38 | 67.9 | 1.000 * |
| Knows 3 or more dengue symptoms | 30 | 53.6 | 11 | 19.6 | p < 0.001 * |
| Knows 1 or more mosquito breeding sites inside the house | 47 | 83.9 | 44 | 78.6 | 0.629 * |
| Knows 1 or more mosquito breeding sites outside the house | 45 | 80.4 | 44 | 78.6 | 1.000 * |
| Knows 1 or more mosquito breeding prevention methods | 48 | 85.7 | 50 | 89.3 | 0.776 * |
| Knows 1 or more dengue prevention methods | 52 | 92.9 | 52 | 92.9 | 1.000 * |
| Total knowledge score (0–48) | Mean | SD | Mean | SD | 0.062 ** |
| 10.09 | 3.549 | 8.91 | 3.053 | ||
| Attitude | |||||
| Total attitude score (0–32) | Mean | SD | Mean | SD | 0.627 ** |
| 24.21 | 3.329 | 24.55 | 4.004 | ||
| Practice | |||||
| Total practice score (0–24) | Mean | SD | Mean | SD | 0.156 ** |
| 10.21 | 1.615 | 10.63 | 1.169 | ||
| Knowledge | Baseline | Midline | Endline | |||
|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||||
| I Group | C Group | I Group | C Group | I Group | C Group | |
| How is dengue transmitted? | ||||||
| Mosquito | 38 (67.9) | 38 (67.9) | 56 (100) | 44 (81.5) | 56 (100) | 45 (83.3) |
| What type of mosquito causes dengue fever? | ||||||
| Aedes | 5 (8.9) | 6 (10.7) | 38 (67.9) | 20 (37) | 50 (89.3) | 31 (57.4) |
| When do dengue mosquitoes most often bite? | ||||||
| Bite during the day | 15 (26.8) | 10 (17.9) | 49 (87.5) | 19 (35.2) | 54 (96.4) | 35 (64.8) |
| Bite during the night time | 25 (44.6) | 34 (60.7) | 7 (12.5) | 29 (53.7) | 2 (3.6) | 19 (35.2) |
| Other | 2 (3.6) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Don’t know | 14 (25) | 12 (21.4) | 0 (0) | 6 (11.1) | 0 (0) | 0 (0) |
| Where do Aedes mosquitoes usually breed inside the house? | ||||||
| In the trays under the fridge | 3 (5.4) | 1 (1.8) | 6 (10.7) | 3 (5.6) | 8 (14.3) | 5 (9.3) |
| In the flower pot trays | 2 (3.6) | 1 (1.8) | 7 (12.5) | 2 (3.7) | 9 (16.1) | 2 (3.7) |
| In the water containers | 35 (62.5) | 22 (39.3) | 30 (53.6) | 35 (64.8) | 31 (55.4) | 18 (33.3) |
| In the open water tanks | 8 (14.3) | 22 (39.3) | 30 (53.6) | 16 (29.6) | 34 (60.7) | 34 (63) |
| Dirty environment | 2 (3.6) | 1 (1.8) | 1 (1.8) | 0 (0) | 0 (0) | 0 (0) |
| Don’t know | 6 (10.7) | 11 (19.6) | 0 (0) | 7 (13) | 0 (0) | 3 (5.6) |
| Knows 1 or more breeding sites inside the house | 47 (83.9) | 44 (78.6) | 54 (96.4) | 47 (87) | 55 (98.2) | 51 (94.4) |
| Where do Aedes mosquitoes usually breed outside the house? | ||||||
| In the flower leaves | 9 (16.1) | 15 (26.8) | 14 (25) | 12 (22.2) | 19 (33.9) | 8 (14.8) |
| In the old tires | 6 (10.7) | 1 (1.8) | 13 (23.2) | 4 (7.4) | 20 (35.7) | 1 (1.9) |
| In the roof gutter | 12 (21.4) | 5 (8.9) | 17 (30.4) | 10 (18.5) | 11 (19.6) | 3 (5.6) |
| In the empty cans, shells | 22 (39.3) | 27 (48.2) | 38 (67.9) | 23 (42.6) | 51 (91.1) | 43 (79.6) |
| Dirty water | 2 (3.6) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Don’t know | 9 (16.1) | 11 (19.6) | 1 (1.8) | 14 (25.9) | 0 (0) | 3 (5.6) |
| Knows 1 or more breeding sites outside the house | 45 (80.4) | 44 (78.6) | 54 (96.4) | 40 (74.1) | 56 (100) | 51 (94.4) |
| How can you prevent mosquitoes from breeding? | ||||||
| Using insecticide in water | 9 (16.1) | 12 (21.4) | 31 (55.4) | 14 (25.9) | 35 (62.5) | 16 (29.6) |
| Changing stored water frequently | 7 (12.5) | 11 (19.6) | 24 (42.9) | 15 (27.8) | 28 (50) | 13 (24.1) |
| Turning containers upside down | 10 (17.9) | 21 (37.5) | 31 (55.4) | 20 (37) | 40 (71.4) | 17 (31.5) |
| Putting covers on water jars | 27 (48.2) | 20 (35.7) | 45 (80.4) | 28 (51.9) | 34 (60.7) | 22 (40.7) |
| Burning or burying empty cans, shells | 3 (5.4) | 3 (5.4) | 14 (25) | 7 (13) | 23 (41.1) | 10 (18.5) |
| Spraying insecticide | 14 (25) | 11 (19.6) | 15 (26.8) | 10 (18.5) | 33 (58.9) | 20 (37) |
| Clean the household | 7 (12.5) | 3 (5.4) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Don’t know | 3 (5.4) | 2 (3.6) | 2 (3.6) | 3 (5.6) | 0 (0) | 0 (0) |
| Knows 1 or more mosquito breeding prevention methods | 48 (85.7) | 50 (89.3) | 55 (98.2) | 51 (94.4) | 56 (100) | 54 (100) |
| How can you prevent dengue? | ||||||
| Use mosquito net during the day | 5 (8.9) | 9 (16.1) | 15 (26.8) | 14 (25.9) | 22 (39.3) | 9 (16.7) |
| Wear long sleeves/long pants | 23 (41.1) | 22 (39.3) | 48 (85.7) | 37 (68.5) | 52 (92.9) | 42 (77.8) |
| Use mosquito repellent | 15 (26.8) | 22 (39.3) | 22 (39.3) | 26 (48.1) | 33 (58.9) | 22 (40.7) |
| Use insecticide spray | 34 (60.7) | 36 (64.3) | 27 (48.2) | 31 (57.4) | 41 (73.2) | 32 (59.3) |
| Cut down bushes near the house | 1 (1.8) | 1 (1.8) | 6 (10.7) | 2 (3.7) | 14 (25) | 6 (11.1) |
| Have children play far from mosquito breeding area | 3 (5.4) | 0 (0) | 3 (5.4) | 0 (0) | 14 (25) | 1 (1.9) |
| Use mosquito coils during the day | 4 (7.1) | 3 (5.4) | 9 (16.1) | 2 (3.7) | 21 (37.5) | 3 (5.6) |
| Keep household environment clean | 4 (7.1) | 0 (0) | 4 (7.1) | 4 (7.4) | 26 (46.4) | 12 (22.2) |
| Install screens on windows/doors | 1 (1.8) | 0 (0) | 1 (1.8) | 0 (0) | 16 (28.6) | 1 (1.9) |
| Keep clothes tidy | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 18 (32.1) | 2 (3.7) |
| Use fan | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 2 (3.6) | 1 (1.9) |
| Don’t know | 4 (7.1) | 2 (3.6) | 1 (1.8) | 2 (3.7) | 0 (0) | 1 (1.9) |
| Knows 1 or more dengue prevention methods | 52 (92.9) | 52 (92.9) | 55 (98.2) | 52 (96.3) | 56 (100) | 53 (98.1) |
| What are the symptoms of dengue? | ||||||
| High fever | 40 (70.1) | 37 (66.1) | 52 (92.9) | 42 (77.8) | 55 (98.2) | 45 (83.3) |
| Headache | 16 (28.6) | 12 (21.4) | 34 (60.7) | 26 (48.1) | 45 (80.4) | 29 (53.7) |
| Chills | 5 (8.9) | 0 (0) | 24 (42.9) | 14 (25.9) | 35 (62.5) | 17 (31.5) |
| Nausea/Vomiting | 12 (21.4) | 4 (7.1) | 31 (55.4) | 17 (31.5) | 36 (64.3) | 19 (35.2) |
| Rash | 13 (23.2) | 3 (5.4) | 24 (42.9) | 9 (16.7) | 22 (39.3) | 7 (13) |
| Muscle and joint pain | 11 (19.6) | 11 (19.6) | 26 (46.4) | 16 (29.6) | 37 (66.1) | 15 (27.8) |
| Bleeding | 6 (10.7) | 2 (3.6) | 25 (44.6) | 7 (13) | 35 (62.5) | 12 (22.2) |
| Diarrhea | 0 (0) | 0 (0) | 5 (8.9) | 1 (1.9) | 1 (1.8) | 0 (0) |
| Eye pain | 3 (5.4) | 0 (0) | 12 (21.4) | 2 (3.7) | 25 (44.6) | 1 (1.9) |
| Don’t know | 12 (21.4) | 18 (32.1) | 3 (5.4) | 9 (16.7) | 0 (0) | 7 (13) |
| Attitude | Agree | Don’t Know | Disagree | |||
|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||||
| I Group | C Group | I Group | C Group | I Group | C Group | |
| Dengue is a serious illness? | ||||||
| Baseline | 56 (100) | 53 (94.6) | 0 (0) | 0 (0) | 0 (0) | 3 (5.4) |
| Midline | 55 (98.2) | 54 (100) | 0 (0) | 0 (0) | 1 (1.8) | 0 (0) |
| Endline | 56 (100) | 51 (94.4) | 0 (0) | 1 (1.9) | 0 (0) | 2 (3.7) |
| Dengue is a transmissible disease? | ||||||
| Baseline | 47 (83.9) | 39 (69.6) | 0 (0) | 2 (3.6) | 9 (16.1) | 15 (26.8) |
| Midline | 50 (89.3) | 46 (85.2) | 0((0) | 1 (1.9) | 6 (10.7) | 7 (13) |
| Endline | 51 (91.1) | 44 (81.5) | 0 (0) | 0 (0) | 5 (8.9) | 10 (18.5) |
| You are at risk of getting dengue? | ||||||
| Baseline | 37 (66.1) | 40 (71.4) | 7 (12.5) | 6 (10.7) | 12 (21.4) | 10 (17.9) |
| Midline | 49 (87.5) | 37 (68.5) | 2 (3.6) | 3 (5.6) | 5 (8.9) | 14 (25.9) |
| Endline | 46 (82.1) | 38 (70.4) | 4 (7.1) | 5 (9.3) | 6 (10.7) | 11 (20.4) |
| Dengue fever can be prevented easily? | ||||||
| Baseline | 34 (60.7) | 39 (69.6) | 1 (1.8) | 0 (0) | 21 (37.5) | 17 (30.4) |
| Midline | 44 (78.6) | 40 (74.1) | 0 (0) | 2 (3.7) | 12 (21.4) | 12 (22.2) |
| Endline | 47 (83.9) | 34 (63) | 0 (0) | 0 (0) | 9 (16.1) | 20 (37) |
| Can removing empty containers protect you from dengue infection? | ||||||
| Baseline | 49 (87.5) | 48 (85.7) | 0 (0) | 1 (1.8) | 7 (12.5) | 7 (12.5) |
| Midline | 56 (100) | 54 (100) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Endline | 55 (98.2) | 52 (96.3) | 0 (0) | 0 (0) | 1 (1.8) | 2 (3.7) |
| Using bed nets, repellents, and long sleeves can protect from mosquito bites? | ||||||
| Baseline | 55 (98.2) | 54 (96.4) | 0 (0) | 0 (0) | 1 (1.8) | 2 (3.6) |
| Midline | 56 (100) | 53 (98.1) | 0 (0) | 0 (0) | 0 (0) | 1 (1.9) |
| Endline | 56 (100) | 52 (96.3) | 0 (0) | 0 (0) | 0 (0) | 2 (3.7) |
| Practice | Baseline | Midline | Endline | |||
|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||||
| I Group | C Group | I Group | C Group | I Group | C Group | |
| What do you do to prevent dengue? | ||||||
| Nothing | 2 (3.6) | 7 (12.5) | 3 (5.4) | 2 (3.7) | 4 (7.1) | 0 (0) |
| Sleep under bed net during the day | 9 (16.1) | 16 (28.6) | 15 (26.8) | 22 (40.7) | 29 (51.8) | 18 (33.3) |
| Use fan to prevent mosquito bites | 9 (16.1) | 17 (30.4) | 10 (17.9) | 22 (40.7) | 17 (30.4) | 10 (18.5) |
| Use insecticide spray | 40 (71.4) | 41 (73.2) | 47 (83.9) | 41 (75.9) | 53 (94.6) | 49 (90.7) |
| Use repellent | 30 (53.6) | 26 (46.4) | 47 (83.9) | 38 (70.4) | 51 (91.1) | 32 (59.3) |
| Use mosquito coil | 25 (44.6) | 22 (39.3) | 42 (75) | 28 (51.9) | 51 (91.1) | 30 (55.6) |
| Use smoke to drive away mosquitoes | 5 (8.9) | 1 (1.8) | 8 (14.3) | 5 (9.3) | 13 (23.2) | 2 (3.7) |
| Cover all water containers | 6 (10.7) | 3 (5.4) | 21 (37.5) | 6 (11.1) | 30 (53.6) | 15 (27.8) |
| Change water in trays under the fridge | 0 (0) | 0 (0) | 7 (12.5) | 0 (0) | 11 (19.6) | 2 (3.7) |
| Destroy or burn unused containers | 1 (1.8) | 0 (0) | 3 (5.4) | 0 (0) | 18 (32.1) | 2 (3.7) |
| Do you keep covers on the water containers in the home? | ||||||
| Yes | 55 (98.2) | 54 (96.4) | 56 (100) | 53 (98.1) | 56 (100) | 54 (100) |
| Please can I observe some of the containers? | ||||||
| Covers observed on all containers | 45 (80.4) | 44 (78.6) | 51 (91.1) | 48 (88.9) | 53 (94.6) | 53 (98.1) |
| Covers observed on some containers | 10 (17.9) | 9 (16.1) | 5 (8.9) | 5 (9.3) | 3 (5.4) | 1 (1.9) |
| No covers observed | 1 (1.8) | 3 (5.4) | 0 (0) | 1 (1.9) | 0 (0) | 0 (0) |
| How often do you change the storage water? | ||||||
| Once a week | 14 (25) | 18 (32.1) | 21 (37.5) | 20 (37) | 31 (55.4) | 30 (55.6) |
| More than once a week | 34 (60.7) | 37 (66.1) | 31 (55.4) | 34 (63) | 24 (42.9) | 22 (40.7) |
| Twice per month | 2 (3.6) | 0 (0) | 2 (3.6) | 0 (0) | 0 (0) | 0 (0) |
| Once a month | 0 (0) | 1 (1.8) | 2 (3.6) | 0 (0) | 1 (1.8) | 2 (3.7) |
| Never | 4 (7.1) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Don’t know | 2 (3.6) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| How often do you clean the water containers? | ||||||
| Every day | 43 (76.8) | 44 (78.6) | 45 (80.4) | 43 (79.6) | 35 (62.5) | 36 (66.7) |
| Once a week | 8 (14.3) | 9 (16.1) | 10 (17.9) | 11 (20.4) | 20 (35.7) | 10 (18.5) |
| Once a month | 4 (7.1) | 2 (3.6) | 0 (0) | 0 (0) | 0 (0) | 8 (14.8) |
| Occasionally | 1 (1.8) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Never | 0 (0) | 1 (1.8) | 0 (0) | 0 (0) | 1 (1.8) | 0 (0) |
| Don’t know | 0 (0) | 0 (0) | 1 (1.8) | 0 (0) | 0 (0) | 0 (0) |
| Observe water containers | ||||||
| Containers look very clean | 50 (89.3) | 48 (85.7) | 56 (100) | 51 (94.4) | 56 (100) | 52 (96.3) |
| Containers do not look very clean | 6 (10.7) | 8 (14.3) | 0 (0) | 3 (5.6) | 0 (0) | 2 (3.7) |
| What do you do with containers you are not currently using? | ||||||
| Leave them empty as they are | 4 (7.1) | 3 (5.4) | 3 (5.4) | 6 (11.1) | 2 (3.6) | 0 (0) |
| Turn them upside down | 13 (23.2) | 13 (23.2) | 29 (51.8) | 21 (38.9) | 33 (58.9) | 26 (48.1) |
| Move them inside | 12 (21.4) | 23 (41.1) | 17 (30.4) | 12 (22.2) | 15 (26.8) | 12 (22.2) |
| Move them outside | 26 (46.4) | 18 (32.1) | 12 (21.4) | 20 (37) | 10 (17.9) | 16 (29.6) |
| Don’t have extra containers/Sell | 2 (3.6) | 1 (1.8) | 0 (0) | 1 (1.9) | 0 (0) | 0 (0) |
| What do you do with waste such as old shells, cans, tires, plastic bottles, and other small containers? | ||||||
| Bury them | 1 (1.8) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Turn them upside down | 2 (3.6) | 0 (0) | 1 (1.8) | 2 (3.7) | 3 (5.4) | 1 (1.9) |
| Burn them | 0 (0) | 0 (0) | 1 (1.8) | 0 (0) | 2 (3.6) | 1 (1.9) |
| Move them outside | 52 (92.9) | 54 (96.4) | 55 (98.2) | 52 (96.3) | 52 (92.9) | 52 (96.3) |
| Sell/Recycle | 6 (10.7) | 3 (5.4) | 0 (0) | 0 (0) | 1 (1.8) | 0 (0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shafique, M.; Mukhtar, M.; Areesantichai, C.; Perngparn, U. Effectiveness of Positive Deviance, an Asset-Based Behavior Change Approach, to Improve Knowledge, Attitudes, and Practices Regarding Dengue in Low-Income Communities (Slums) of Islamabad, Pakistan: A Mixed-Method Study. Insects 2022, 13, 71. https://doi.org/10.3390/insects13010071
Shafique M, Mukhtar M, Areesantichai C, Perngparn U. Effectiveness of Positive Deviance, an Asset-Based Behavior Change Approach, to Improve Knowledge, Attitudes, and Practices Regarding Dengue in Low-Income Communities (Slums) of Islamabad, Pakistan: A Mixed-Method Study. Insects. 2022; 13(1):71. https://doi.org/10.3390/insects13010071
Chicago/Turabian StyleShafique, Muhammad, Muhammad Mukhtar, Chitlada Areesantichai, and Usaneya Perngparn. 2022. "Effectiveness of Positive Deviance, an Asset-Based Behavior Change Approach, to Improve Knowledge, Attitudes, and Practices Regarding Dengue in Low-Income Communities (Slums) of Islamabad, Pakistan: A Mixed-Method Study" Insects 13, no. 1: 71. https://doi.org/10.3390/insects13010071