External Beam Radiotherapy of Recurrent Glioma: Radiation Tolerance of the Human Brain

Abstract
:1. Introduction
2. Results

{kind=link}
{kind=link}
{kind=link}
 |
 |
 |
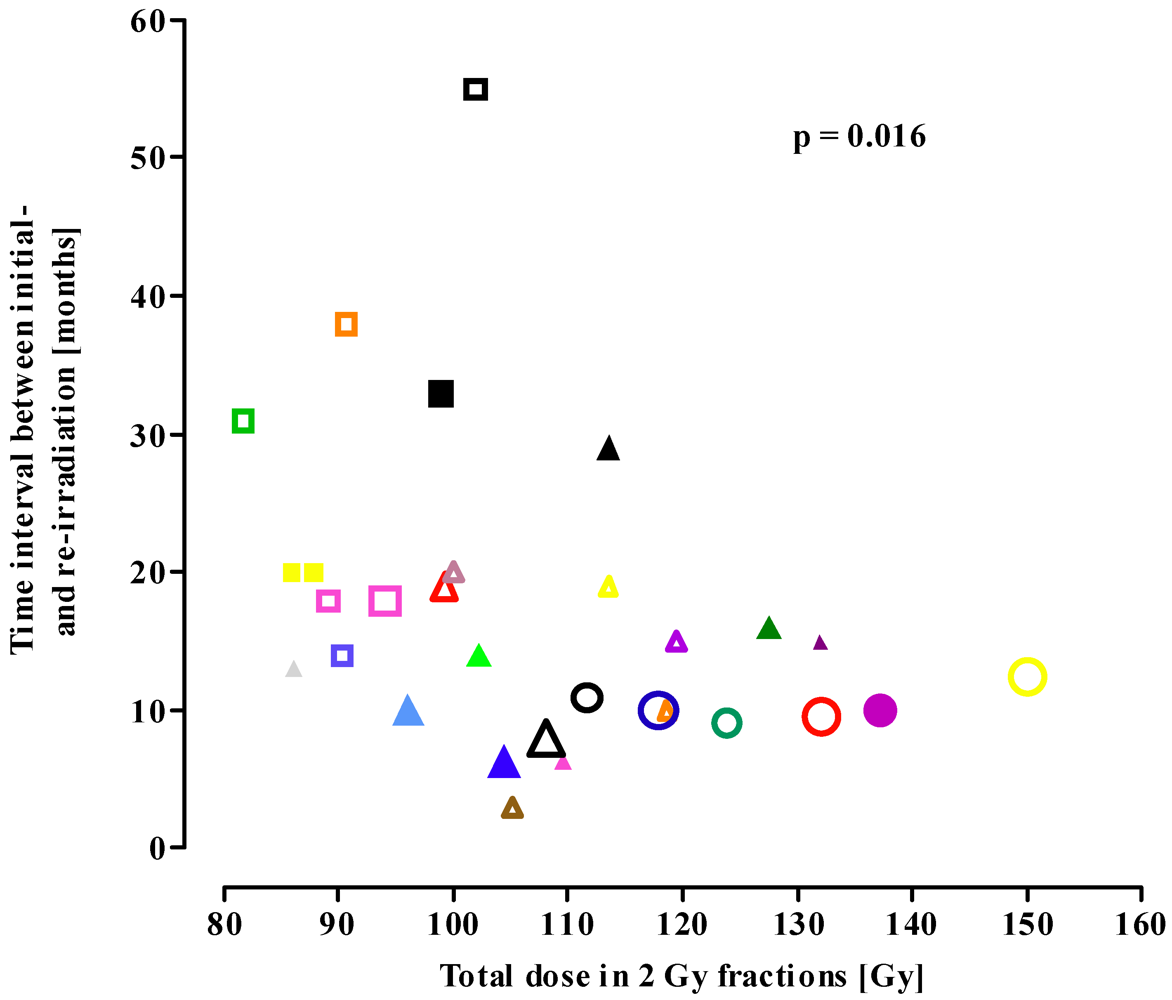

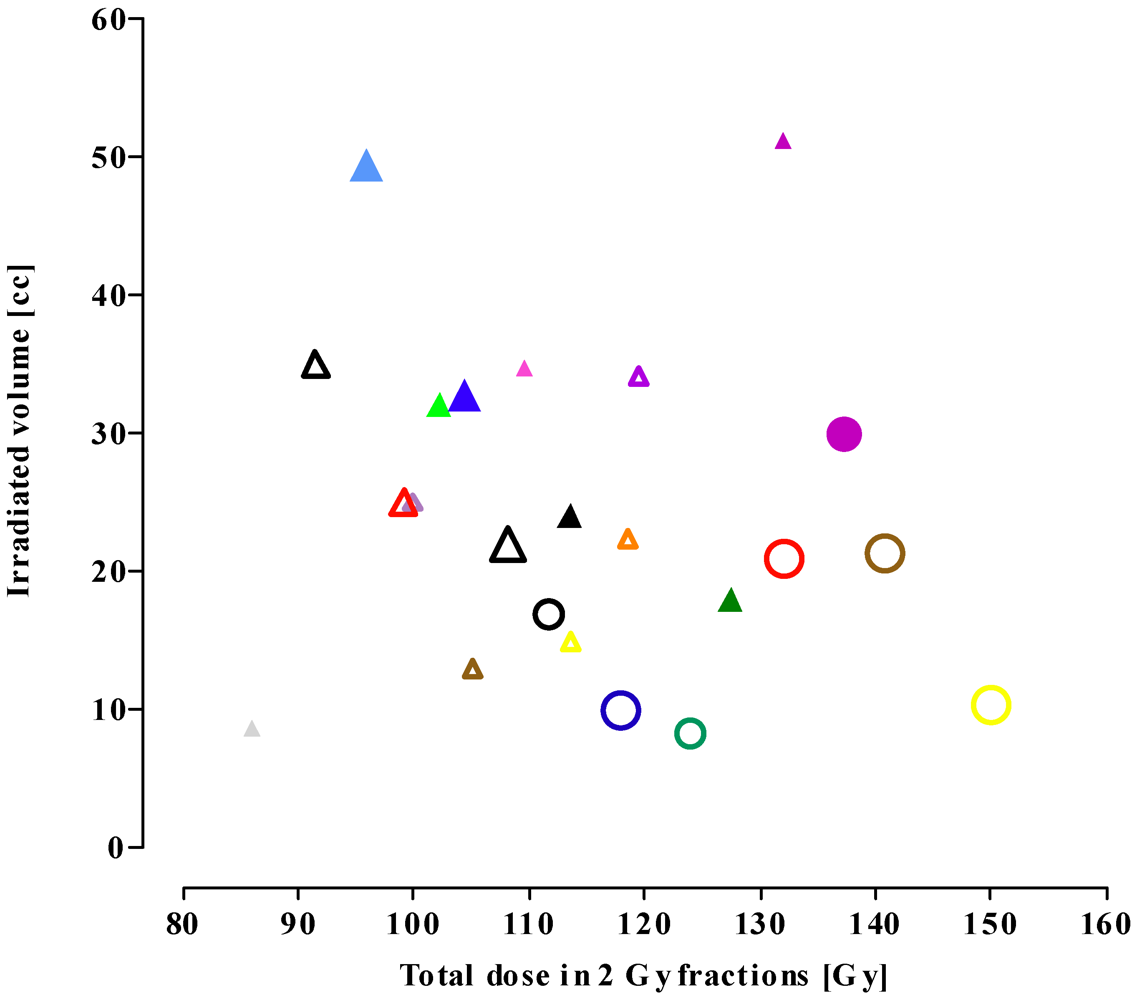
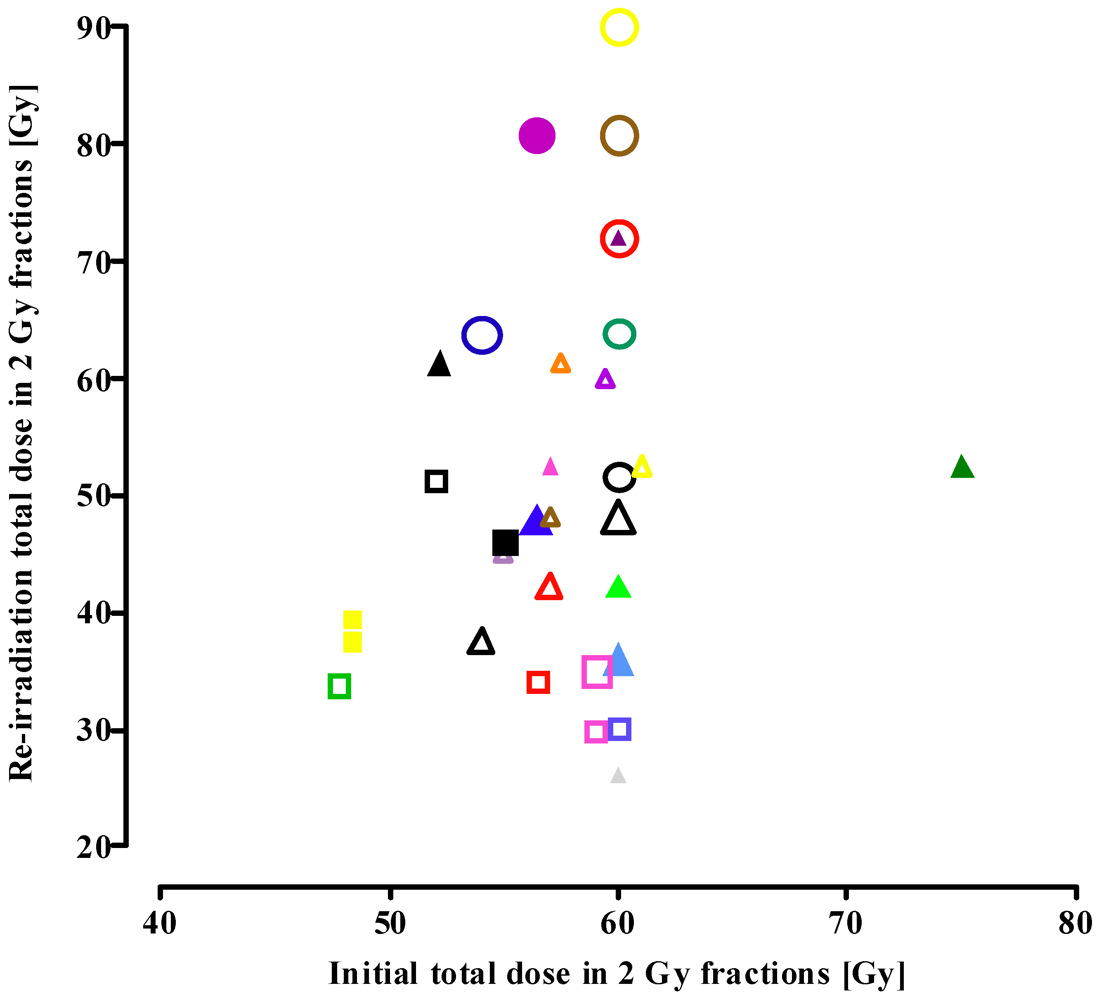
| Re-irradiation procedure | EQD2cumulative [Gy] | Time interval between initial radiotherapy and re-irradiation [months] | Mean treatment volume [cc] |
|---|---|---|---|
| Conventional radiotherapy | 92.6 ± 6.8 (81.6–102.8) | 29.9 ± 14.1 (14–55) | No data |
| Fractionated stereotactic radiotherapy | 109.9 ± 13.8 (86.1–133.9) | 16.7 ± 11.1 (3–48) | 27.6 ± 11.9 (8.7–51.1) |
| Stereotactic radiosurgery | 130.5 ± 13.5 (111.6 to ~150) | 10.4 ± 1.2 (9.1–12.5) | 16.9 ± 7.9 (8.4–30) |
3. Discussion
3.1. Re-Irradiation Tolerance of the CNS
3.1.1. Total Cumulative Dose
3.1.2. Time Interval between Initial Exposure and Retreatment
3.1.3. Size of the Initial Dose
3.1.4. Treatment Volume
3.2. Possible Role of Particle Therapy
3.3. Neurocognitive Function after Re-Irradiation
3.4. Survival Data Including Data with Additional Chemotherapy
3.4.1. Patients Re-Irradiated with Conventional Radiotherapy
3.4.2. Patients Re-Irradiated with Fractionated Stereotactic Radiotherapy
3.4.3. Patients Re-Irradiated with Stereotactic Radiosurgery
4. Experimental Section
5. Conclusions
Conflicts of interest
References
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar]
- Stupp, R.; Hegi, M.E.; Mason, W.P.; van den Bent, M.J.; Taphoorn, M.J.; Janzer, R.C.; Ludwin, S.K.; Allgeier, A.; Fisher, B.; Belanger, K.; et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-Year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009, 10, 459–466. [Google Scholar]
- Jansen, E.P.; Dewit, L.G.; van Herk, M.; Bartelink, H. Target volumes in radiotherapy for high grade malignant glioma of the brain. Radiother. Oncol. 2000, 56, 151–156. [Google Scholar]
- Emami, B.; Lyman, J.; Brown, A.; Coia, L.; Goitein, M.; Munzenrider, J.E.; Shank, B.; Solin, L.J.; Wesson, M. Tolerance of normal tissue to therapeutic irradiation. Int. J. Radiat. Oncol. Biol. Phys. 1991, 21, 109–122. [Google Scholar]
- Lawrence, Y.R.; Li, X.A.; El Naqa, I.; Hahn, C.A.; Marks, L.B.; Merchant, T.E.; Dicker, A.P. Radiation dose-volume effects in the brain. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, S20–S27. [Google Scholar] [CrossRef]
- Barendsen, G.W. Dose fractionation, dose rate and iso-effect relationships for normal tissue responses. Int. J. Radiat. Oncol. Biol. Phys. 1982, 8, 1981–1997. [Google Scholar]
- Joiner, M.C.; Bentzen, S.M. Fractionation: The linear-quadratic approach. In Basic Clinical Radiobiology; Joiner, M.C., van der Kogel, A.J., Eds.; Hodder Arnold: London, UK, 2009; pp. 102–119. [Google Scholar]
- Shrieve, D.C. Radiation dose, fractionation and normal tissue injury. In Human Radiation Injury; Shrieve, D.C., Loeffler, J.S., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2011; pp. 32–42. [Google Scholar]
- Kim, H.K.; Thornton, A.F.; Greenberg, H.S.; Page, M.A.; Junck, L.; Sandler, H.M. Results of re-irradiation of primary intracranial neoplasms with three-dimensional conformal therapy. Am. J. Clin. Oncol. 1997, 20, 358–363. [Google Scholar]
- Hayat, K.; Jones, B.; Bisbrown, G.; Baria, K.; Pigott, T. Retreatment of patients with intracranial gliomas by external beam radiotherapy and cytotoxic chemotherapy. Clin. Oncol. 1997, 9, 158–163. [Google Scholar]
- Arcicasa, M.; Roncadin, M.; Bidoli, E.; Dedkov, A.; Gigante, M.; Trovò, M.G. Reirradiation and lomustine in patients with relapsed high-grade gliomas. Int. J. Radiat. Oncol. Biol. Phys. 1999, 43, 789–793. [Google Scholar] [CrossRef]
- Nieder, C.; Nestle, U.; Niewald, M.; Walter, K.; Schnabel, K. Hyperfractionated reirradiation for malignant gliomas. Front. Radiat. Ther. Oncol. 1999, 33, 150–157. [Google Scholar]
- Veninga, T.; Langendijk, H.A.; Slotman, B.J.; Rutten, E.H.; van der Kogel, A.J.; Prick, M.J.; Keyser, A.; van der Maazen, R.W. Reirradiation of primary brain tumours: Survival, clinical response and prognostic factors. Radiother. Oncol. 2001, 59, 127–137. [Google Scholar]
- Henke, G.; Paulsen, F.; Steinbach, J.P.; Ganswindt, U.; Isijanov, H.; Kortmann, R.D.; Bamberg, M.; Belka, C. Hypofractionated reirradiation for recurrent malignant glioma. Strahlenther. Onkol. 2009, 185, 113–119. [Google Scholar] [CrossRef]
- Niyazi, M.; Ganswindt, U.; Schwarz, S.B.; Kreth, F.W.; Tonn, J.C.; Geisler, J.; la Fougère, C.; Ertl, L.; Linn, J.; Siefert, A.; et al. Irradiation and bevacizumab in high-grade glioma retreatment settings. Int. J. Radiat. Oncol. Biol. Phys. 2011, 98, 1–14. [Google Scholar]
- Shepherd, S.F.; Laing, R.W.; Cosgrove, V.P.; Warrington, A.P.; Hines, F.; Ashley, S.E.; Brada, M. Hypofractionated stereotactic radiotherapy in the management of recurrent glioma. Int. J. Radiat. Oncol. Biol. Phys. 1997, 37, 393–398. [Google Scholar]
- Cho, K.H.; Hall, W.A.; Gerbi, B.J.; Higgins, P.D.; McGuire, W.A.; Clark, H.B. Single dose versus fractionated stereotactic radiotherapy for recurrent high-grade gliomas. Int. J. Radiat. Oncol. Biol. Phys. 1999, 45, 1133–1141. [Google Scholar]
- Hudes, R.S.; Corn, B.W.; Werner-Wasik, M.; Andrews, D.; Rosenstock, J.; Thoron, L.; Downes, B.; Curran, W.J., Jr. A phase I dose escalation study of hypofractionated stereotactic radiotherapy as salvage therapy for persistent or recurrent malignant glioma. Int. J. Radiat. Oncol. Biol. Phys. 1999, 43, 293–298. [Google Scholar] [CrossRef]
- Lederman, G.; Wronski, M.; Arbit, E.; Odaimi, M.; Wertheim, S.; Lombardi, E.; Wrzolek, M. Treatment of recurrent glioblastoma multiforme using fractionated stereotactic radiosurgery and concurrent paclitaxel. Am. J. Clin. Oncol. 2000, 23, 155–159. [Google Scholar]
- Voynov, G.; Kaufman, S.; Hong, T.; Pinkerton, A.; Simon, R.; Dowsett, R. Treatment of recurrent malignant gliomas with stereotactic intensity modulated radiation therapy. Am. J. Clin. Oncol. 2002, 25, 606–611. [Google Scholar]
- Grosu, A.L.; Weber, W.A.; Franz, M.; Stärk, S.; Piert, M.; Thamm, R.; Gumprecht, H.; Schwaiger, M.; Molls, M.; Nieder, C. Reirradiation of recurrent high-grade gliomas using amino acid PET (SPECT)/CT/MRI image fusion to determine gross tumor volume for stereotactic fractionated radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2005, 63, 511–519. [Google Scholar]
- Vordermark, D.; Kolbl, O.; Ruprecht, K.; Vince, G.H.; Bratengeier, K.; Flentje, M. Hypofractionated stereotactic re-irradiation: Treatment option in recurrent malignant glioma. BMC Cancer 2005, 5, 55. [Google Scholar]
- Ernst-Stecken, A.; Ganslandt, O.; Lambrecht, U.; Sauer, R.; Grabenbauer, G. Survival and quality of life after hypofractionated stereotactic radiotherapy for recurrent malignant glioma. J. Neurooncol. 2007, 81, 287–294. [Google Scholar]
- Kohshi, K.; Yamamoto, H.; Nakahara, A.; Katoh, T.; Takagi, M. Fractionated stereotactic radiotherapy using gamma unit after hyperbaric oxygenation on recurrent high-grade gliomas. J. Neurooncol. 2007, 82, 297–303. [Google Scholar]
- Laing, R.W.; Warrington, A.P.; Graham, J.; Britton, J.; Hines, F.; Brada, M. Efficacy and toxicity of fractionated stereotactic radiotherapy in the treatment of recurrent gliomas (phase I/II study). Radiother. Oncol. 1993, 27, 22–29. [Google Scholar]
- Combs, S.E.; Thilmann, C.; Edler, L.; Debus, J.; Schulz-Ertner, D. Efficacy of fractionated stereotactic reirradiation in recurrent gliomas: Long-term results in 172 patients in a single insitution. J. Clin. Oncol. 2005, 23, 8863–8869. [Google Scholar] [CrossRef]
- Fokas, E.; Wacker, U.; Gross, M.W.; Henzel, M.; Encheva, E.; Engenhart-Cabillic, R. Hypofractionated stereotactic reirradiation of recurrent glioblastomas : A beneficial treatment option after high-dose radiotherapy? Strahlenther. Onkol. 2009, 185, 235–240. [Google Scholar] [CrossRef]
- Gutin, P.H.; Iwamoto, F.M.; Beal, K.; Mohile, N.A.; Karimi, S.; Hou, B.L.; Lymberis, S.; Yamada, Y.; Chang, J.; Abrey, L.E. Safety and efficacy of bevacizumab with hypofractionated stereotactic irradiation for recurrent malignant gliomas. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 156–163. [Google Scholar]
- Fogh, S.E.; Andrews, D.W.; Glass, J.; Curran, W.; Glass, C.; Champ, C.; Evans, J.J.; Hyslop, T.; Pequignot, E.; Downes, B.; et al. Hypofractionated stereotactic radiation therapy: An effective therapy for recurrent high-grade gliomas. J. Clin. Oncol. 2010, 28, 3048–3053. [Google Scholar]
- Minniti, G.; Armosini, V.; Salvati, M.; Lanzetta, G.; Caporello, P.; Mei, M.; Osti, M.F.; Maurizi, R.E. Fractionated stereotactic reirradiation and concurrent temozolomide in patients with recurrent glioblastoma. J. Neurooncol. 2011, 103, 683–691. [Google Scholar]
- Patel, M.; Siddiqui, F.; Jin, J.Y.; Mikkelsen, T.; Rosenblum, M.; Movsas, B.; Ryu, S. Salvage reirradiation for recurrent glioblastoma with radiosurgery: Radiographic response and improved survival. J. Neurooncol. 2009, 92, 185–191. [Google Scholar]
- Chamberlain, M.C.; Barba, D.; Kormanik, P.; Shea, W.M. Stereotactic radiosurgery for recurrent gliomas. Cancer 1994, 74, 1342–1347. [Google Scholar]
- van Kampen, M.; Engenhart-Cabillic, R.; Debus, J.; Fuss, M.; Rhein, B.; Wannenmacher, M. The radiosurgery of glioblastoma multiforme in cases of recurrence. The Heidelberg experiences compared to the literature. Strahlenther. Onkol. 1998, 174, 19–24. [Google Scholar] [CrossRef]
- Combs, S.E.; Widmer, V.; Thilmann, C.; Hof, H.; Debus, J.; Schulz-Ertner, D. Stereotactic radiosurgery (SRS): Treatment option for recurrent glioblastoma multiforme (GBM). Cancer 2005, 104, 2168–2173. [Google Scholar]
- Biswas, T.; Okunieff, P.; Schell, M.C.; Smudzin, T.; Pilcher, W.H.; Bakos, R.S.; Vates, G.E.; Walter, K.A.; Wensel, A.; Korones, D.N.; et al. Stereotactic radiosurgery for glioblastoma: Retrospective analysis. Radiat. Oncol. 2009, 4, 11. [Google Scholar] [CrossRef]
- Pouratian, N.; Crowley, R.W.; Sherman, J.H.; Jagannathan, J.; Sheehan, J.P. Gamma knife radiosurgery after radiation therapy as an adjunctive treatment for glioblastoma. J. Neurooncol. 2009, 94, 409–418. [Google Scholar]
- Brenner, D.J. The linear-quadratic model is an appropriate methodology for determining isoeffective doses at large doses per fraction. Semin. Radiat. Oncol. 2008, 18, 234–239. [Google Scholar]
- Kirkpatrick, J.P.; Meyer, J.J.; Marks, L.B. The linear-quadratic model is inappropriate to model high dose per fraction effects in radiosurgery. Semin. Radiat. Oncol. 2008, 18, 240–243. [Google Scholar]
- Bentzen, S.M.; Saunders, M.I.; Dische, S. Repair halftimes estimated from observations of treatment-related morbidity after CHART or conventional radiotherapy in head and neck cancer. Radiother. Oncol. 1999, 53, 219–226. [Google Scholar]
- Mayer, R.; Sminia, P. Reirradiation tolerance of the human brain. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 1350–1360. [Google Scholar]
- Sahgal, A.; Wong, C.; van der Kogel, A.J. Spinal cord. In Human Radiation Injury; Shrieve, D.C., Loeffler, J.S., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2011; pp. 225–235. [Google Scholar]
- Sminia, P.; Oldenburger, F.; Slotman, B.J.; Schneider, C.J.; Hulshof, M.C. Re-irradiation of the human spinal cord. Strahlenther. Onkol. 2002, 178, 453–456. [Google Scholar]
- Fokas, E.; Kraft, G.; An, H.; Engenhart-Cabillic, R. Ion beam radiobiology and cancer: Time to update ourselves. Biochim. Biophys. Acta 2009, 1796, 216–229. [Google Scholar]
- Suit, H.; Delaney, T.; Goldberg, S.; Paganetti, H.; Clasie, B.; Gerweck, L.; Niemierko, A.; Hall, E.; Flanz, J.; Hallman, J.; et al. Proton versus carbon ion beams in the definitive radiation treatment of cancer patients. Radiother. Oncol. 2010, 95, 3–22. [Google Scholar] [CrossRef]
- Schulz-Ertner, D.; Tsujii, H. Particle radiation therapy using proton and heavier ion beams. J. Clin. Oncol. 2007, 25, 953–964. [Google Scholar]
- Combs, S.; Burkholder, I.; Edler, L.; Rieken, S.; Habermehl, D.; Jäkel, O.; Haberer, T.; Haselmann, R.; Unterberg, A.; Wick, W.; et al. Randomised phase I/II study to evaluate carbon ion radiotherapy versus fractionated stereotactic radiotherapy in patients with recurrent or progressive gliomas: The CINDERELLA trial. BMC Cancer 2010, 10, 533. [Google Scholar]
- Laack, N.N.I.; Brown, P.D. Cognitive sequelae of brain radiation. In Human Radiation Injury; Shrieve, D.C., Loeffler, J.S., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2011; pp. 169–179. [Google Scholar]
- Chakravarti, A.; Erkkinen, M.G.; Nestler, U.; Stupp, R.; Mehta, M.; Aldape, K.; Gilbert, M.R.; Black, P.M.; Loeffler, J.S. Temozolomide-mediated radiation enhancement in glioblastoma: A report on underlying mechanisms. Clin. Cancer Res. 2006, 12, 4738–4746. [Google Scholar]
- van Nifterik, K.A.; van den Berg, J.; Stalpers, L.J.; Lafleur, M.V.; Leenstra, S.; Slotman, B.J.; Hulsebos, T.J.; Sminia, P. Differential radiosensitizing potential of temozolomide in MGMT promoter methylated glioblastoma multiforme cell lines. Int. J. Radiat. Oncol. Biol. Phys. 2007, 69, 1246–1253. [Google Scholar]
- Chalmers, A.J.; Ruff, E.M.; Martindale, C.; Lovegrove, N.; Short, S.C. Cytotoxic effects of temozolomide and radiation are additive- and schedule-dependent. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 1511–1519. [Google Scholar]
- PubMed Homepage. Available online: http://www.ncbi.nlm.nih.gov/pubmed/ (accessed on 2 March 2012).
- Flickinger, J.C.; Kondziolka, D.; Lunsford, L.D.; Kassam, A.; Phuong, L.K.; Liscak, R.; Pollock, B. Development of a model to predict permanent symptomatic postradiosurgery injury for arteriovenous malformation patients. Int. J. Radiat. Oncol. Biol. Phys. 2000, 46, 1143–1148. [Google Scholar]
- Barani, I.J.; Sneed, P.K. Cerebral radionecrosis. In Human Radiation Injury; Shrieve, D.C., Loeffler, J.S., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2011; pp. 254–267. [Google Scholar]
- Siepmann, D.B.; Siegel, A.; Lewis, P.J. Tl-201 SPECT and F-18 FDG PET for assessment of glioma recurrence versus radiation necrosis. Clin. Nucl. Med. 2005, 30, 199–200. [Google Scholar]
- Wigg, R.W. Applied Radiobiology and Bioeffect Planning; Medical Physics Publishing Madison: Madison, WI, USA, 2001; p. 253. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Sminia, P.; Mayer, R. External Beam Radiotherapy of Recurrent Glioma: Radiation Tolerance of the Human Brain. Cancers 2012, 4, 379-399. https://doi.org/10.3390/cancers4020379
Sminia P, Mayer R. External Beam Radiotherapy of Recurrent Glioma: Radiation Tolerance of the Human Brain. Cancers. 2012; 4(2):379-399. https://doi.org/10.3390/cancers4020379
Chicago/Turabian StyleSminia, Peter, and Ramona Mayer. 2012. "External Beam Radiotherapy of Recurrent Glioma: Radiation Tolerance of the Human Brain" Cancers 4, no. 2: 379-399. https://doi.org/10.3390/cancers4020379