Breastfeeding and Active Bonding Protects against Children’s Internalizing Behavior Problems


Abstract
:1. Introduction
2. Experimental Section
2.1. Participants and Sample Design
2.2. Measures
2.2.1. Internalizing Behavior Problems
2.2.2. Breastfeeding
2.2.3. Maternal Interaction
2.2.4. Social Adversity
2.3. Statistical Methods
3. Results
3.1. Single Effect of Breastfeeding or Active Bonding
3.2. Combined Effect of Breastfeeding and Active Bonding
3.3. Potential Confounds
3.4. Effect Moderator
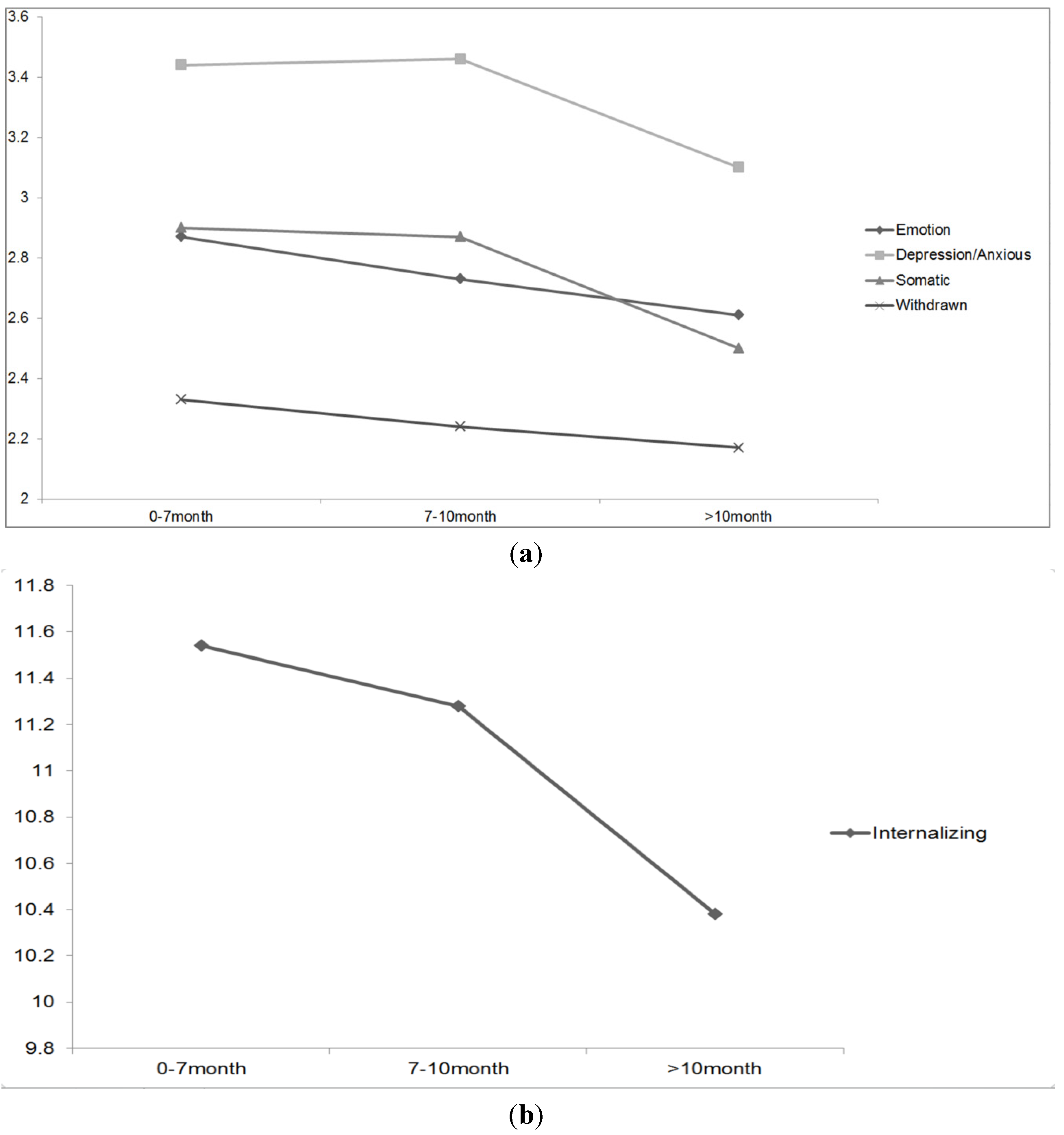
3.5. Dose Response Relationship
4. Discussion

{kind=link}
| Breastfeeding type | Active bonding | |||||||
|---|---|---|---|---|---|---|---|---|
| Variables | Exclusive 77% | Non-exclusive 23% | Effect Size (Cohen’s d) | P | Always 43.4% | Never/Sometimes 56.6% | Effect Size (Cohen’s d) | P |
| Emotionally Reactive | 2.63 (2.39) | 2.85 (2.38) | −0.092 | 0.168 | 2.52 (2.30) | 2.82 (2.43) | −0.126 | 0.031 |
| Anxious/Depressed | 3.22 (2.28) | 3.43 (2.30) | −0.091 | 0.175 | 3.13 (2.17) | 3.44 (2.36) | −0.136 | 0.02 |
| Somatic Complaints | 2.64 (2.47) | 3.01 (2.34) | −0.153 | 0.025 | 2.60 (2.33) | 2.86 (2.54) | −0.106 | 0.076 |
| Withdrawn | 2.18 (2.34) | 2.43 (2.40) | −0.105 | 0.11 | 1.89 (2.19) | 2.52 (2.44) | −0.271 | <0.001 |
| Total Internalizing | 10.66 (7.64) | 11.7 (7.53) | −0.137 | 0.04 | 10.14 (7.05) | 11.63 (7.94) | −0.198 | 0.001 |
| Boy % | 53.3 | 60.4 | \ | 0.031 | 57.3 | 53.1 | \ | 0.141 |
| Social Adversity | 3.53 (2.03) | 3.48 (2.11) | 0.0241 | 0.701 | 3.17 (1.83) | 3.77 (2.15) | −0.104 | <0.001 |
| Group 1 | Group 2 | Group 3 | Group 4 | |||
|---|---|---|---|---|---|---|
| Variables | Exclusive Breastfeeding with Active Bonding 34.8% | Exclusive Breastfeeding without Active Bonding 43.5% | Non-exclusive Breastfeeding with Active Bonding 9% | Non-exclusive Breastfeeding without Active Bonding 12.7% | Effect Size (omega squared w2) | P |
| Emotionally Reactive | 2.48 (2.30) | 2.73 (2.45) | 2.62 (2.22) | 3.07 (2.50) | 0.003 | 0.068 |
| Anxious/Depressed | 3.11 (2.17) | 3.30 (2.34) | 3.15 (2.15) | 3.71 (2.41) | 0.004 | 0.04 |
| Somatic Complaints | 2.56 (2.39) | 2.70 (2.53) | 2.72 (2.14) | 3.27 (2.50) | 0.005 | 0.023 |
| Withdrawn | 1.87 (2.20) | 2.40 (2.41) | 2.13 (2.22) | 2.73 (2.53) | 0.013 | <0.001 |
| Total Internalizing | 10.01 (7.21) | 11.12 (7.90) | 10.61 (6.66) | 12.79 (8.14) | 0.01 | 0.001 |
| Dependent Variables | Type III Sum of Squares | df | Mean square | F | Significance |
|---|---|---|---|---|---|
| Emotionally Reactive | 34.4 | 3, 1255 | 11 | 2.045 | 0.106 |
| Anxious/Depressed | 38.12 | 3, 1257 | 12.71 | 2.471 | 0.06 |
| Somatic Complaints | 54.6 | 3, 1258 | 18.2 | 3.108 | 0.026 |
| Withdrawn | 90.07 | 3, 1258 | 32.36 | 6.016 | <0.001 |
| Total Internalizing | 774.39 | 3, 1258 | 258.13 | 4.573 | 0.003 |

5. Conclusions
Acknowledgements
Conflicts of Interest
References
- Ip, S.; Chung, M.; Raman, G.; Chew, P.; Magula, N.; Devine, D.; Trikalinos, T.; Lau, J. Breastfeeding and maternal and infant health outcomes in developed countries. Evid. Rep. Technol. Assess. 2007, 153, 1–186. [Google Scholar]
- Uauy, R.; de Andraca, I. Human milk and breast feeding for optimal mental development. J. Nutr. 1995, 125, 2278S–2280S. [Google Scholar]
- Quinn, P.J.; O’Callaghan, M.; Williams, G.M.; Najman, J.M.; Andersen, M.J.; Bor, W. The effect of breastfeeding on child development at 5 years: A cohort study. J. Paediatr. Child Health 2001, 37, 465–469. [Google Scholar] [CrossRef]
- Whitehouse, A.J.; Robinson, M.; Li, J.; Oddy, W.H. Duration of breastfeeding and language ability in middle childhood. Paediatr. Perinat. Epidemiol. 2011, 25, 44–52. [Google Scholar] [CrossRef]
- Feldman, R.; Eidelman, A.I. Direct and indirect effects of breast milk on the neurobehavioral and cognitive development of premature infants. Dev. Psychobiol. 2003, 43, 109–119. [Google Scholar] [CrossRef]
- Zetterstrom, R. Breastfeeding and infant-mother interaction. Acta Paediatr. Suppl. 1999, 88, 1–6. [Google Scholar] [CrossRef]
- Fergusson, D.M.; Woodward, L.J. Breast feeding and later psychosocial adjustment. Paediatr. Perinat. Epidemiol. 1999, 13, 144–157. [Google Scholar] [CrossRef]
- DeWitt, S.J.; Sparks, J.W.; Swank, P.B.; Smith, K.; Denson, S.E.; Landry, S.H. Physical growth of low birthweight infants in the first year of life: Impact of maternal behaviors. Early Hum. Dev. 1997, 47, 19–34. [Google Scholar] [CrossRef]
- Costello, E.J.; Mustillo, S.; Erkanli, A.; Keeler, G.; Angold, A. Prevalence and development of psychiatric disorders in childhood and adolescence. Arch. Gen. Psychiatry 2003, 60, 837–844. [Google Scholar] [CrossRef]
- Kovacs, M.; Devlin, B. Internalizing disorders in childhood. J. Child Psychol. Psychiatry 1998, 39, 47–63. [Google Scholar] [CrossRef]
- Kramer, M.S.; Fombonne, E.; Igumnov, S.; Vanilovich, I.; Matush, L.; Mironova, E.; Bogdanovich, N.; Tremblay, R.E.; Chalmers, B.; Zhang, X.; et al. Effects of prolonged and exclusive breastfeeding on child behavior and maternal adjustment: Evidence from a large, randomized trial. Pediatrics 2008, 121, e435–e440. [Google Scholar] [CrossRef]
- Papp, L.M. Longitudinal associations between breastfeeding and observed mother-child interaction qualities in early childhood. Child Care Health Dev. 2013. [Google Scholar] [CrossRef]
- Kwok, M.K.; Leung, G.M.; Schooling, C.M. Breast feeding and early adolescent behaviour, self-esteem and depression: Hong Kong’s “Children of 1997” birth cohort. Arch. Dis. Child. 2013, 98, 887–894. [Google Scholar] [CrossRef]
- Oddy, W.H.; Kendall, G.E.; Li, J.; Jacoby, P.; Robinson, M.; de Klerk, N.H.; Silburn, S.R.; Zubrick, S.R.; Landau, L.I.; Stanley, F.J. The long-term effects of breastfeeding on child and adolescent mental health: A pregnancy cohort study followed for 14 years. J. Pediatr. 2010, 156, 568–574. [Google Scholar] [CrossRef]
- Liu, J.; McCauley, L.A.; Zhao, Y.; Zhang, H.; Pinto-Martin, J. Cohort profile: The China Jintan child cohort study. Int. J. Epidemiol. 2010, 39, 668–674. [Google Scholar] [CrossRef]
- Liu, J.; McCauley, L.; Leung, P.; Wang, B.; Needleman, H.; Pinto-Martin, J. Community-based participatory research (CBPR) approach to study children’s health in China: Experiences and reflections. Int. J. Nurs. Stud. 2011, 48, 904–913. [Google Scholar] [CrossRef]
- Liu, J.; Cheng, H.; Leung, P.W. The application of the preschool child behavior checklist and the caregiver-teacher report form to mainland Chinese children: Syndrome structure, gender differences, country effects, and inter-informant agreement. J. Abnorm. Child Psychol. 2011, 39, 251–264. [Google Scholar] [CrossRef]
- Achenbach, T.; Rescorla, L. Manual for the ASEBA Preschool Forms & Profiles; University of Vermont Research Center for Children, Youth & Families: Burlington, VT, USA, 2000. [Google Scholar]
- Achenbach, T.M. Manual for the Child Behavior Checklist/4–18 and 1991 Profile; University of Vermont, Department of Psychiatry: Burlington, VT, USA, 1991. [Google Scholar]
- Rutter, M. Family, Area and School Influences in the Genesis of Conduct Disorders: Aggression and Anti-Social Behaviour in Child-Hood and Adolescence; Hersov, L.A., Berger, M., Shaffer, D., Eds.; Pergamon: Oxford, UK, 1978; pp. 95–113. [Google Scholar]
- Moffit, T.E. Juvenile delinquency and attention deficit disorder: Boys’ developmental trajectories from age 3 to age 15. Child Dev. 1990, 61, 893–910. [Google Scholar] [CrossRef]
- Liu, J.; Portnoy, J.; Raine, A. Association between a marker for prenatal testosterone exposure and externalizing behavior problems in children. Dev. Psychopathol. 2012, 24, 771–782. [Google Scholar] [CrossRef]
- Rautava, S.; Walker, W.A. Academy of breastfeeding medicine founder’s lecture 2008: Breastfeeding—An extrauterine link between mother and child. Breastfeed Med. 2009, 4, 3–10. [Google Scholar] [CrossRef]
- McNamara, R.K.; Jandacek, R.; Rider, T.; Tso, P.; Dwivedi, Y.; Pandey, G.N. Selective deficits in erythrocyte docosahexaenoic acid composition in adult patients with bipolar disorder and major depressive disorder. J. Affect. Disord. 2010, 126, 303–311. [Google Scholar] [CrossRef]
- Colangelo, L.A.; He, K.; Whooley, M.A.; Daviglus, ML.; Liu, K. Higher dietary intake of long-chain omega-3 polyunsaturated fatty acids are inversely associated with depressive symptoms in women. Nutrition 2009, 25, 1011–1019. [Google Scholar] [CrossRef]
- Makrides, M.; Gibson, R.A.; McPhee, A.J.; Yelland, L.; Quinlivan, J.; Ryan, P. Effect of DHA supplementation during pregnancy on maternal depression and neurodevelopment of young children: A randomized controlled trial. JAMA 2010, 304, 1675–1683. [Google Scholar] [CrossRef]
- Murakami, K.; Miyake, Y.; Sasaki, S.; Tanaka, K.; Arakawa, M. Fish and n-3 polyunsaturated fatty acid intake and depressive symptoms: Ryukyus child health study. Pediatrics 2010, 126, e623–e630. [Google Scholar] [CrossRef]
- Kennedy, D.O.; Jackson, P.A.; Elliot, J.M.; Scholey, A.B.; Robertson, B.C.; Greer, J.; Tiplady, B.; Buchanan, T.; Haskell, C.F. Cognitive and mood effects of 8 weeks’ supplementation with 400 mg or 1000 mg of the omega-3 essential fatty acid docosahexaenoic aicid (DHA) in healthy children aged 10–12 years. Nutr. Neurosci. 2009, 12, 48–56. [Google Scholar] [CrossRef]
- Kramer, M.S.; Aboud, F.; Mironova, E.; Vanilovich, I.; Platt, R.W.; Matush, L.; Igumnov, S.; Fombonne, E.; Bogdanovich, N.; Ducruet, T.; et al. Breastfeeding and child cognitive development: A new evidence from a large randomized trial. Arch. Gen. Psychiatry 2008, 65, 578–584. [Google Scholar] [CrossRef]
- Hayatbakhsh, M.R.; O’Callaghan, M.J.; Bor, W.; Williams, G.M.; Najman, J.M. Association of breastfeeding and adolescents’ psychopathology: A large prospective study. Breastfeed Med. 2012, 7, 480–486. [Google Scholar]
- Rutter, M.; Rutter, M. Developing Minds: Challenge and Continuity Across the Life Span; Basic Books: New York, NY, USA, 1993. [Google Scholar]
- Gribble, K.D. Mental health, attachment and breastfeeding: Implications for adopted children and their mothers. Int. Breastfeed J. 2006, 1, 5. [Google Scholar] [CrossRef]
- Britton, J.R.; Britton, H.L.; Gronwaldt, V. Breastfeeding, sensitivity, and attachment. Pediatrics 2006, 118, e1436–e1443. [Google Scholar] [CrossRef]
- Field, T.; Diego, M.; Hernandez-Reif, M.; Figueirdo, B.; Ezell, S.; Siblalingappa, V. Depressed mothers and infants are more relaxed during breastfeeding versus bottlefeeding interactions: Brief report. Infant Behav. Dev. 2010, 33, 241–244. [Google Scholar] [CrossRef] [Green Version]
- Groër, M.W. Differences between exclusive breastfeeders, formula-feeders, and controls: A study of stress, mood, and endocrine variables. Biol. Res. Nurs. 2005, 7, 106–117. [Google Scholar] [CrossRef]
- Rahman, A.; Harrington, R.; Bunn, J. Can maternal depression increase infant risk of illness and growth impairment in developing countries? Child Care Health Dev. 2002, 28, 51–56. [Google Scholar] [CrossRef]
- Hay, D.F.; Pawlby, S.; Waters, C.S.; Sharp, D. Antepartum and postpartum exposure to maternal depression: Different effects on different adolescent outcomes. J. Child Psychol. Psychiatry 2008, 49, 1079–1088. [Google Scholar] [CrossRef]
- Niegel, S.; Ystrom, E.; Hagtvet, K.A.; Vollrath, M.E. Difficult temperament, breastfeeding, and their mutual prospective effects: The Norwegian Mother and Child Cohort Study. JDBP 2008, 29, 458–462. [Google Scholar]
- Nishitani, S.; Miyamura, T.; Tagawa, M.; Sumi, M.; Takase, R.; Doi, H.; Moriuchi, H.; Shinohara, K. The calming effect of a maternal breast milk odor on the human newborn infant. Neurosci. Res. 2009, 63, 66–71. [Google Scholar] [CrossRef]
- Gray, L.; Watt, L.; Blass, E.M. Skin-to-skin contact is analgesic in healthy newborns. Pediatrics 2000, 105, e14. [Google Scholar] [CrossRef]
- Liu, J. Early health risk factors for violence: Conceptualization, review of the evidence, and implications. Aggress. Violent Behav. 2011, 16, 63–73. [Google Scholar] [CrossRef]
- Vaughn, B.E.; El-Sheikh, M.; Shin, N.; Elmore-Staton, L.; Krzysik, L.; Monteiro, L. Attachment representations, sleep quality and adaptive functioning in preschool age children. Attach. Hum. Dev. 2011, 13, 525–540. [Google Scholar] [CrossRef]
- Liu, J.; Zhou, G.; Wang, J.; Ai, Y.; Pinto-Martin, J.; Liu, X. Sleep problems, fatigue, and cognitive performance in Chinese kindergarten children. J. Pediatr. 2012, 161, 520–525.e2. [Google Scholar] [CrossRef]
- Liu, J.; Tuvblad, C.; Raine, A.; Baker, L. Genetic and environmental influences on nutrient intake. Genes Nutr. 2013, 8, 241–252. [Google Scholar] [CrossRef]
- Robinson, M.; Oddy, W.; Li, J.; Kendall, G.E.; de Klerk, N.H.; Silburn, S.R.; Zubrick, S.R.; Newnham, J.P.; Stanley, F.J.; Mattes, E. Pre- and postnatal influences on preschool mental health: A large-scale cohort study. J. Child Psychol. Psychiatry 2008, 49, 1118–1128. [Google Scholar] [CrossRef]
- Promislow, J.; Gladen, B.; Sandler, D. Maternal recall of breastfeeding duration by elderly women. Am. J. Epidemiol. 2005, 161, 289–296. [Google Scholar] [CrossRef]
- Liu, J.; Shi, Z.; Spatz, D.; Loh, R.; Sun, G.; Grisso, J. Social and demographic determinants for breastfeeding in a rural, suburban and city area of South East China. Contemp. Nurse 2013, 45, 234–243. [Google Scholar] [CrossRef]
- Liu, J.; Chen, X.; Lewis, G. Childhood internalizing behavior: Analysis and implications. J. Psychiatr. Ment. Health Nurs. 2011, 18, 884–894. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Liu, J.; Leung, P.; Yang, A. Breastfeeding and Active Bonding Protects against Children’s Internalizing Behavior Problems. Nutrients 2014, 6, 76-89. https://doi.org/10.3390/nu6010076
Liu J, Leung P, Yang A. Breastfeeding and Active Bonding Protects against Children’s Internalizing Behavior Problems. Nutrients. 2014; 6(1):76-89. https://doi.org/10.3390/nu6010076
Chicago/Turabian StyleLiu, Jianghong, Patrick Leung, and Amy Yang. 2014. "Breastfeeding and Active Bonding Protects against Children’s Internalizing Behavior Problems" Nutrients 6, no. 1: 76-89. https://doi.org/10.3390/nu6010076